Gender Inequities, Intersectionality, and Implicit Bias
1/36
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
37 Terms
Gender:
refers to the socially defined roles and responsibilities of men, women, boys, and girls
gender roles are learned from families and communities and vary by culture and generation
Sex:
a biological construct premised upon biological characteristics enabling sexual reproduction
Gender equality:
absence of discrimination, based on a person’s sex, in opportunities, in the allocation of resources or benefits or in access to services
Gender equity:
fairness and justice in the distribution of benefits and responsibilities between women and men and often requires women-specific projects and programs to end existing inequities
Sex as a Biological Variable (SABV):
NIH policy (2016) requiring biological sex be considered in preclinical research, since sex differences affect disease, drug metabolism, and treatment
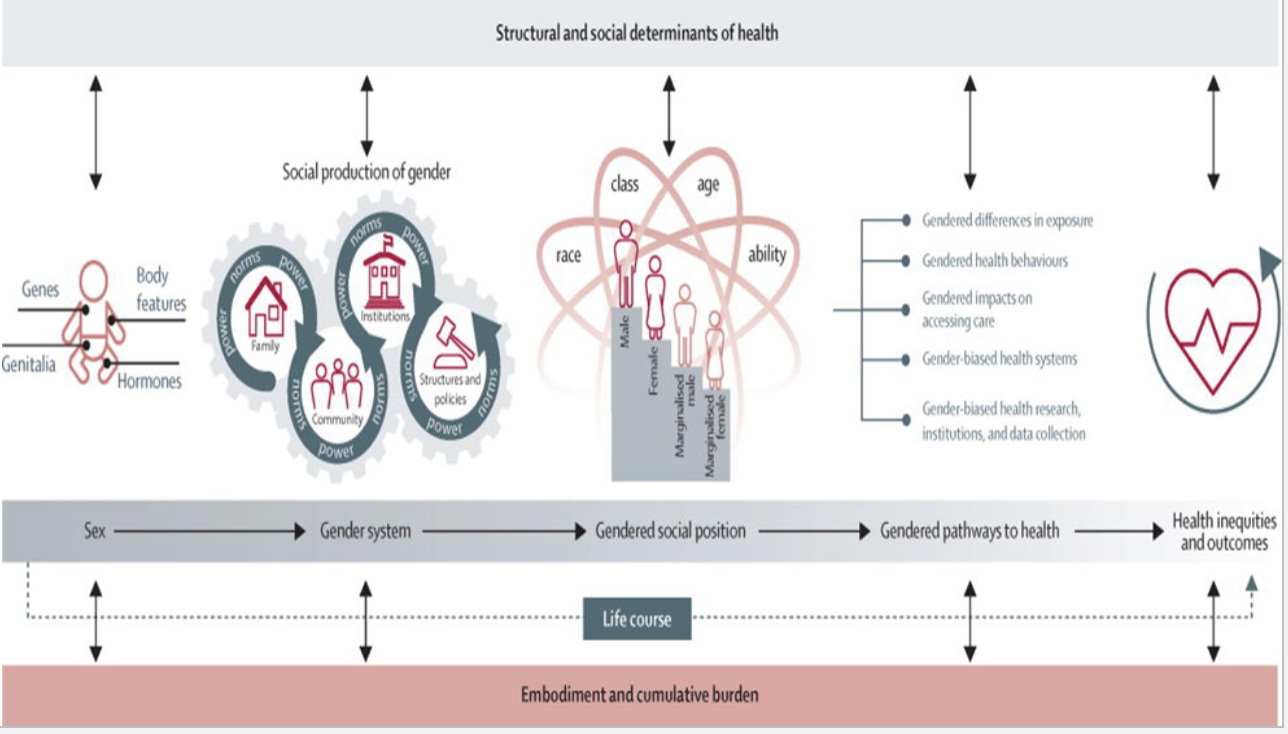
Social determinants affecting Women’s Health:
health status of women in the United States has two key factors (race/ethnicity and socioeconomic status) where they are quite complex, relating to neonatal care, birth outcomes, and increased prevalence of certain diseases
quality and accessibility of care to women varies drastically from one social setting to another, with hardship experienced by women in low-income areas and incarcerated women
Less research on women overall
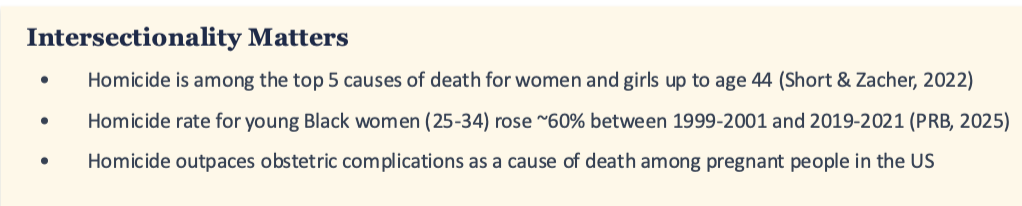
Intersectionality plays a role
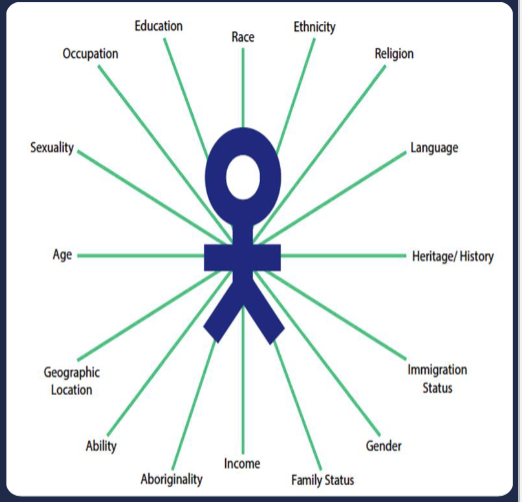
Intersectionality:
a theoretical framework for understanding how aspects of one's social and political identities (gender, race, class, sexuality, ability, height etc.) create unique experiences of privilege or oppression
aims to broaden the agenda of the first waves of feminism, which largely focused on the experiences of white, middle-class women
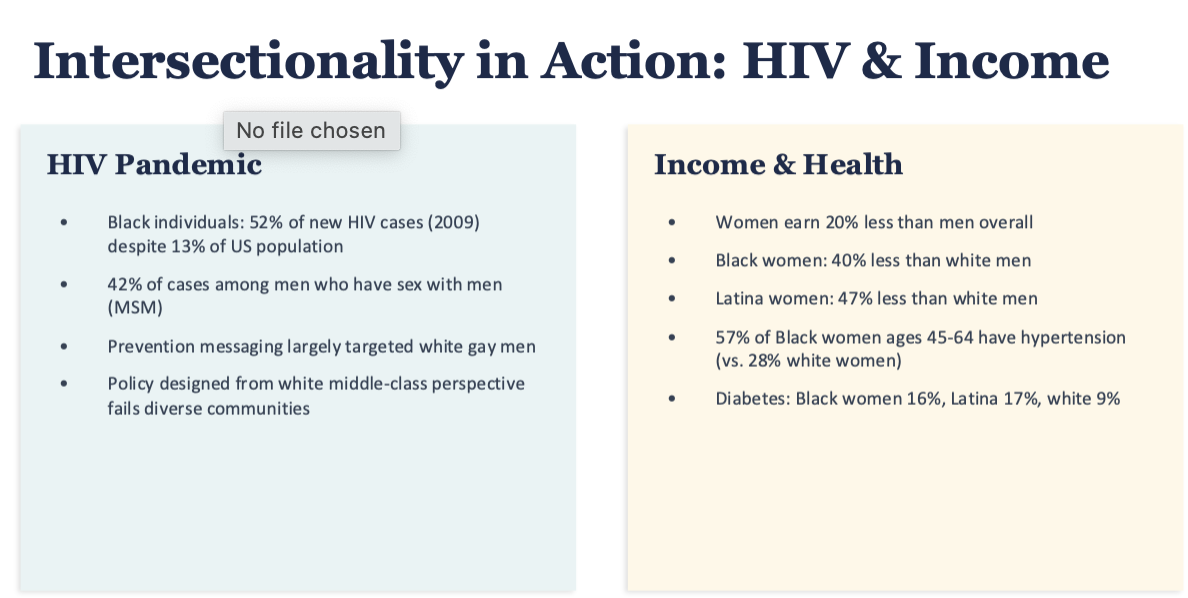
In public health, intersectionality reveals what?
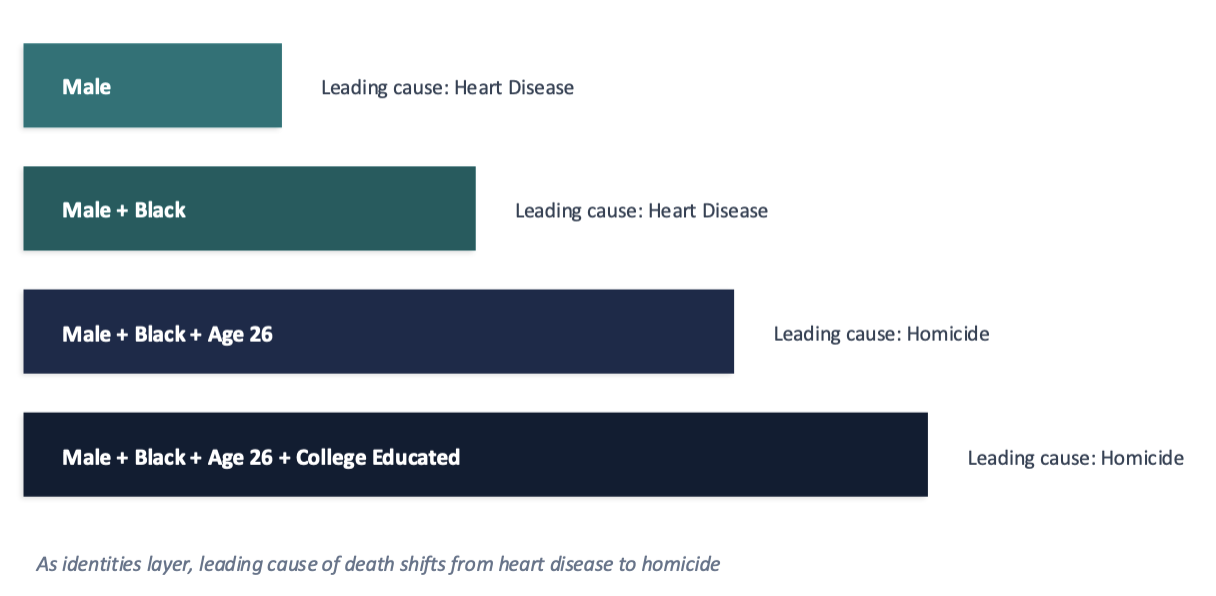
reveals how multiple marginalized identities compound health risks in ways a single-axis analysis misses
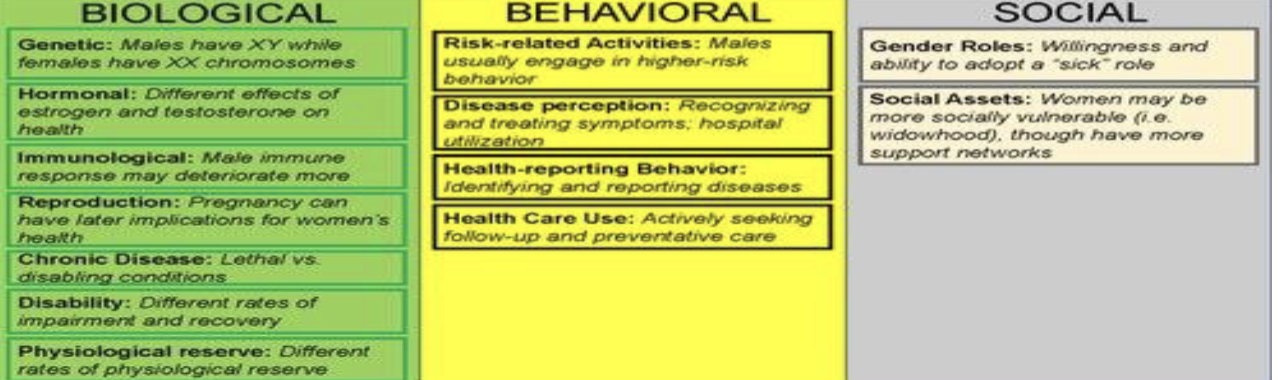
Biological determinants of Women’s Health Disparities:
Heart disease symptoms present differently in women, but male presentation was considered the default until 1999 (AHA)
Iron deficiency anemia related to menstruation
Complications of pregnancy: hemorrhage, hypertensive disorders
Increased susceptibility to certain STIs due to anatomy
Health conditions biologically specific to women (e.g., ovarian cancer)
Sex-based differences in drug metabolism and adverse effects
How is there stigma about female bodies?
stigma discourages women from reporting symptoms and clinicians from taking them seriously where Menstrual health, menopause, and pelvic pain are chronically under-researched
at least 1 in 4 women need medical intervention for menstrual pain, yet it is routinely dismissed
Endometriosis takes an average of 7-10 years to diagnose
Conditions like PCOS, fibroids, and vulvodynia receive a fraction of the funding that conditions of comparable prevalence in men receive
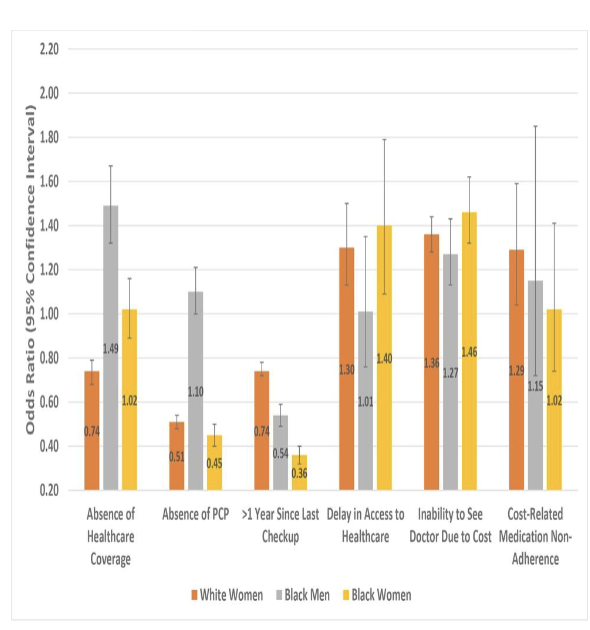
Women and access to healthcare:
lack of coverage for reproductive and mental health services where distrust of providers grows when women feel dismissed or unheard
One-quarter of US women have been diagnosed with depression or anxiety, with little variation across racial/ethnic groups
51% of adults reporting delayed healthcare were female (2007 data)
Looming physician shortage → projected 139,000+ by 2030, further limiting timely care
Median doctor visit: 15.7 minutes covering 6 topics (inadequate for complex needs)
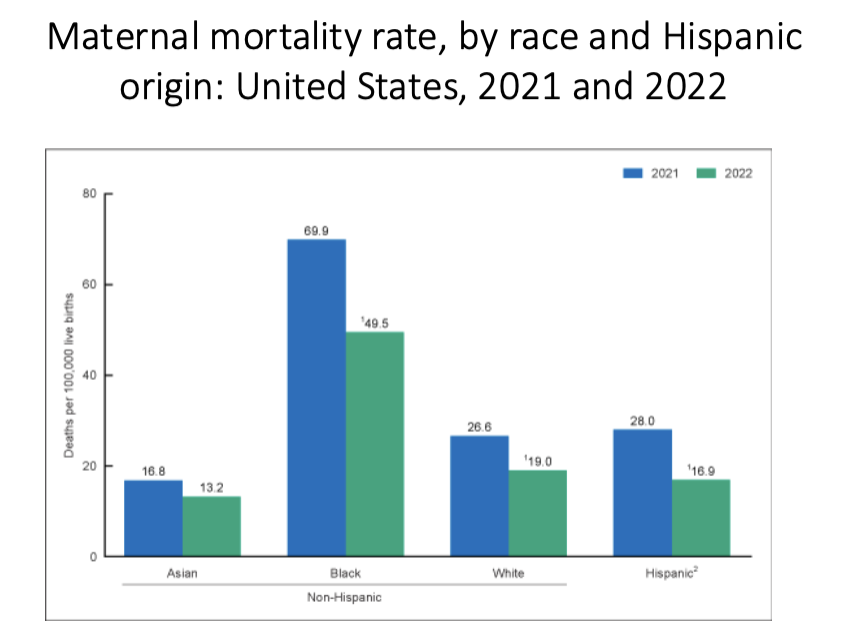
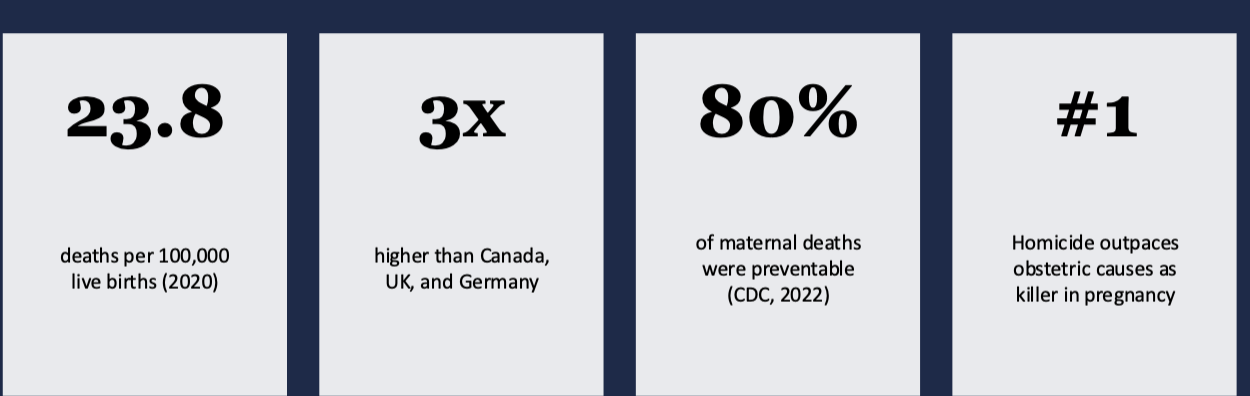
Maternal Mortality:
Black women are 2-3x more likely to die from pregnancy-related causes than white women
Higher education and income do not mitigate this risk
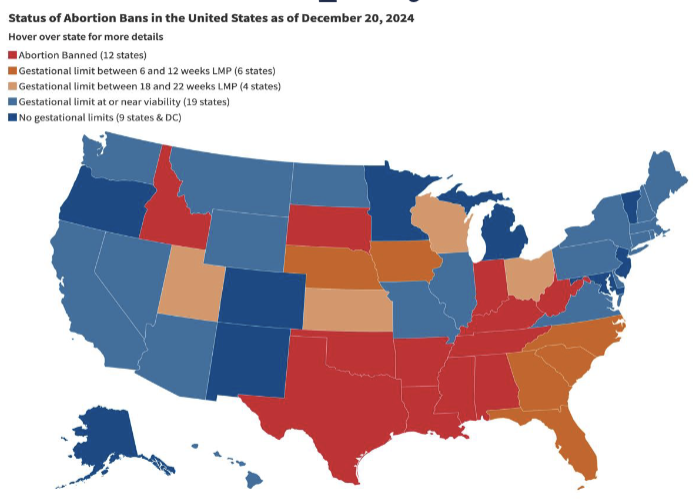
Dobbs v. Jackson (2022):
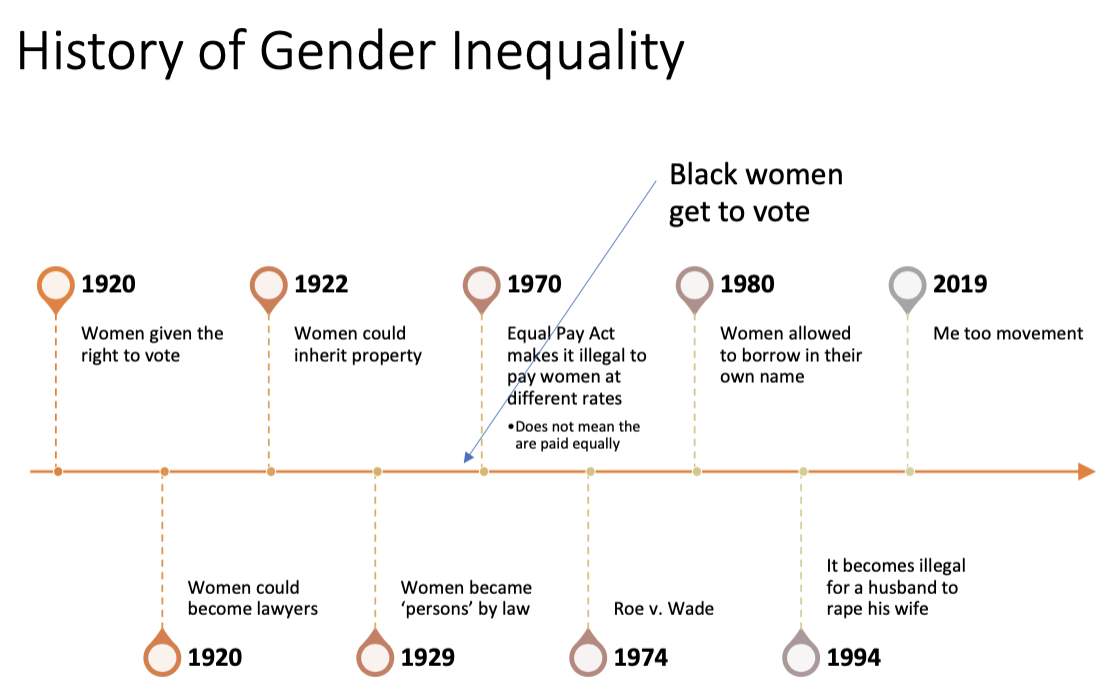
overturned Roe v. Wade, creating a patchwork of state-level bans
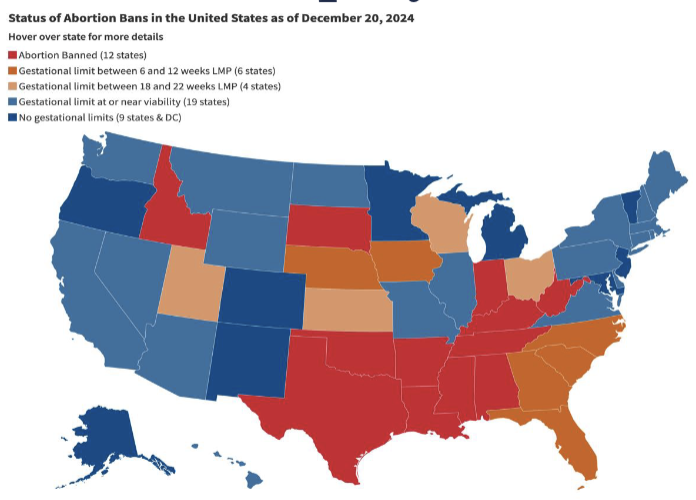
Abortion Access:
Abortion restrictions are a mortality and morbidity issue, not only a rights issue and is not equal as income, geography, and race determine who can obtain care
US is the only high-income nation without federally mandated paid parental leave
Restriction of reproductive autonomy has cascading effects on economic stability, mental health, and family wellbeing

Women in Medical Research:
Women with metal hip replacements: 29% more likely to experience implant failure than men
AHA did not publish a Guide to Preventive Cardiology for Women until 1999, despite heart disease being the leading killer of both sexes
NIH tends to overfund diseases disproportionately affecting men while underfunding those primarily affecting women
Funding for transgender and nonbinary health research also lags significantly
What are mortality patterns among women?
Leading causes of death for both sexes is cardiovascular disease (226/100k) and cancers (185/100k)
Coronary heart disease (CHD) is the single most important specific cause → 185/100k
Male mortality rates are higher overall, but not for heart disease
Black women have significantly higher rates of hypertension than other groups, with earlier onset
Critical factors may include racism and chronic stress (weathering hypothesis)
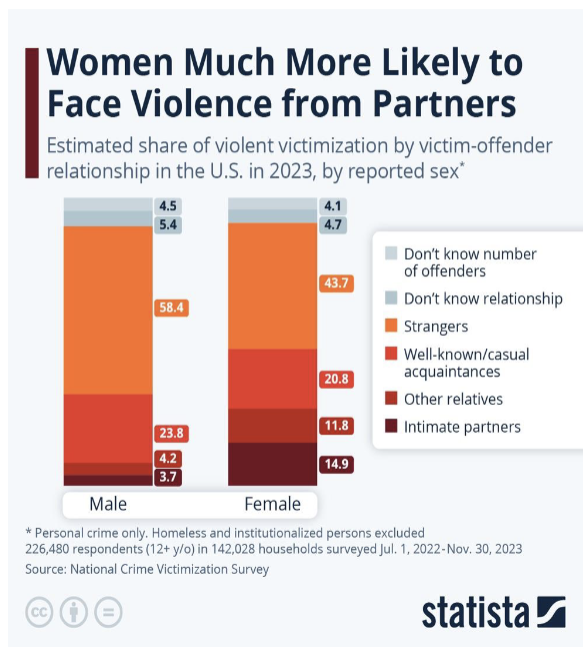
How do we see intersectionality in Violence and Sexual Abuse?
violence can occur at any age, with any gender, in many situations and Intimate partner violence is more common in women but an equal problem in men, which can lead to injuries, unwanted pregnancy, STIs, depression, disability, and death
Risk factors → low SES, young age of male partner, gender inequality, substance use
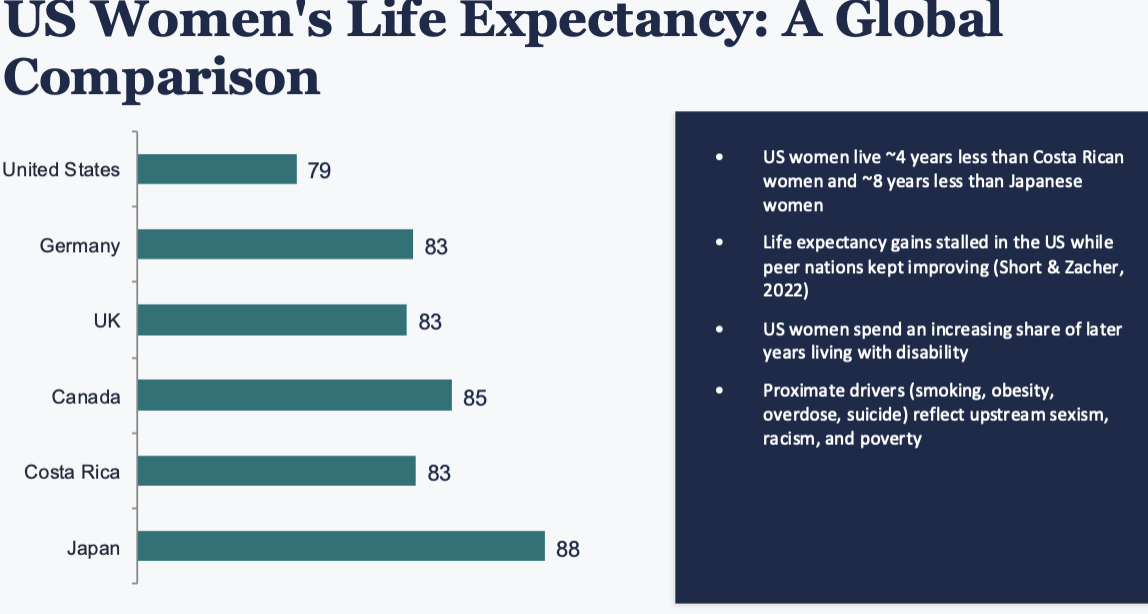
Women’s Health Paradox:
women generally live longer than men but experience higher rates of chronic illness, disability, and lower self-reported health
women notice symptoms earlier and seek treatment more
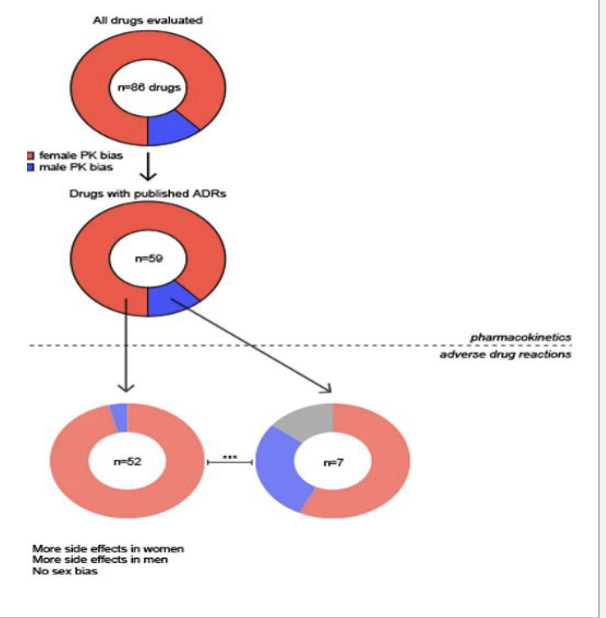
Medication Safety Gap:
AHA did not recognize that women experience different heart attack symptoms until publishing a Guide to Preventive Cardiology for Women in 1999 and Pregnant people are even more commonly excluded from clinical trials, leaving critical gaps in medication safety data during pregnancy
Women experience adverse drug effects at twice the rate of men
Women with metal hip replacements were 29% more likely to experience implant failure (2013 study), possibly due to anatomical differences and inadequate testing
not abstract policy problems, they are clinical harms with real consequences for patients
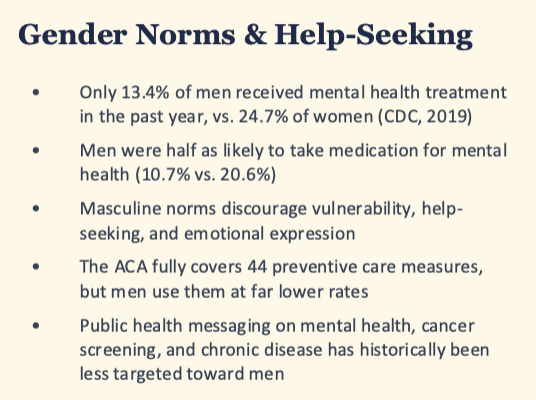
What does we see in male mortality and life expectancy?
in 2024, men's life expectancy was 76.5 years vs. 81.4 for women, a gap of nearly 5 years where, in 13 of the 14 leading causes of death common to both sexes, males have a higher age-adjusted mortality rate
Alzheimer's is the sole exception
American Indian and Black men had the highest age-adjusted death rates in 2024, at roughly 1,200 per 100,000
Heart disease and cancer each kill more than 600,000 people annually → both disproportionately affect men
Drug overdose deaths spiked during the pandemic but fell 26% in 2024 → men remain more affected

What do we see in suicide and deaths of despair of men’s health?
male suicide rate: ~23 per 100,000 vs. ~6 for women (4x disparity), the largest demographic gap in suicide where ~40,000 men die by suicide each year, nearly equal to annual female breast cancer deaths
Highest rates → AI/AN men (41.3/100k), non-Hispanic white men (35.7/100k)
Men over 75 face 7x higher suicide risk than women of the same age
Intersectionality → Black and Hispanic men accounted for 85% of the increase in young adult suicides between 2014-2024
What are some solutions in closing the health gap?
Establish economic parity between men and women
Ensure access to optimal care for low-income communities
Improve educational systems in under-resourced communities
Eliminate racism and discrimination, specifically as directed toward emerging majority women
Care for women before pregnancy and throughout the lifespan, not only during pregnancy
Educate healthcare providers about culture, history, and SES to improve birth outcomes
Provide culturally competent care that recognizes diverse histories, languages, and traditions
What are some solution in changing the system?
Recognize health literacy as critical to improving women's and family health outcomes
Recruit and place more healthcare providers of color in underserved communities
Address the US poverty crisis and unemployment as structural determinants of women's health
End mass incarceration to enable rebuilding of families and communities of color
Fund a dedicated Women's Health Research Institute at NIH
Require equitable representation in clinical trials by sex, race, and gender identity
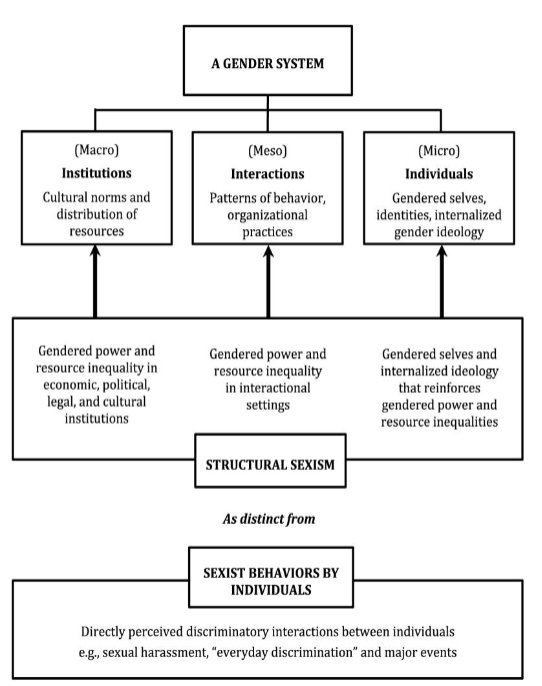
Implicit Bias:
unconscious mental processes that produce automatic associations and reactions (including favorable or unfavorable evaluations) toward groups of people
unaware of them, yet they shape our decisions
Explicit Bias:
preferences, beliefs, and attitudes that people are consciously aware of, personally endorse, and can identify and communicate
Hidden curriculum:
lessons learners absorb through socialization (faculty role-modeling, institutional signals, informal culture) rather than through formal instruction
What makes a bias “implicit”?
it is the residue of a lifetime of exposure to media, language, institutions, and patterns of who does what and who is seen as whom
two people with identical conscious values can carry very different implicit associations, shaped by very different environments
Four features → automatic, unintentional, unaware, consequential
Implicit Association Test (IAT):
measures the speed of automatic associations between concepts (e.g., racial group + “good” / “bad”) with faster pairing = stronger unconscious association and reveals associations people often do not know they hold, and sometimes reject when shown
low test-retest reliability at individual level
single scores do not predict one person’s action
raises awareness and prompt reflection → not diagnosing
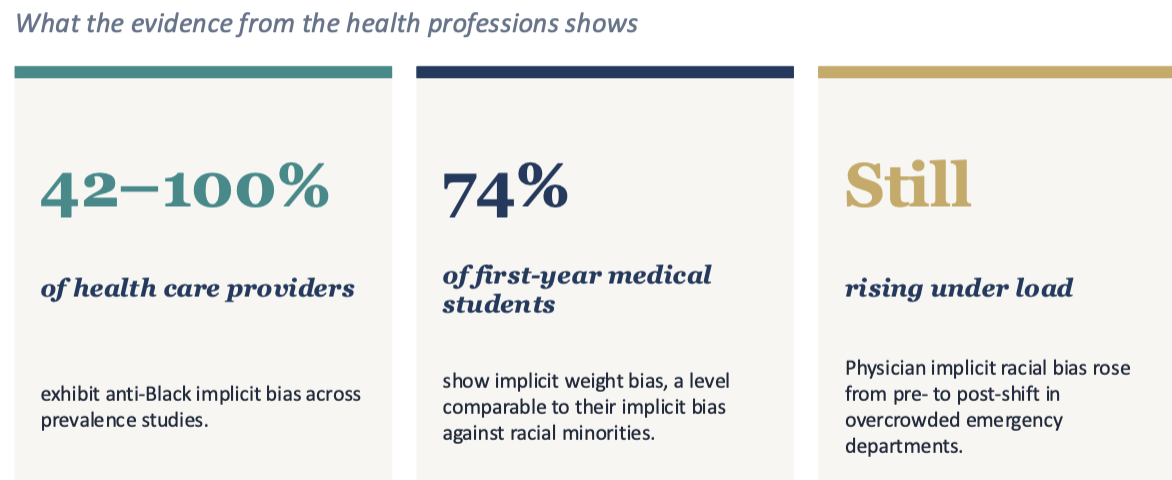
How pervasive is implicit bias?
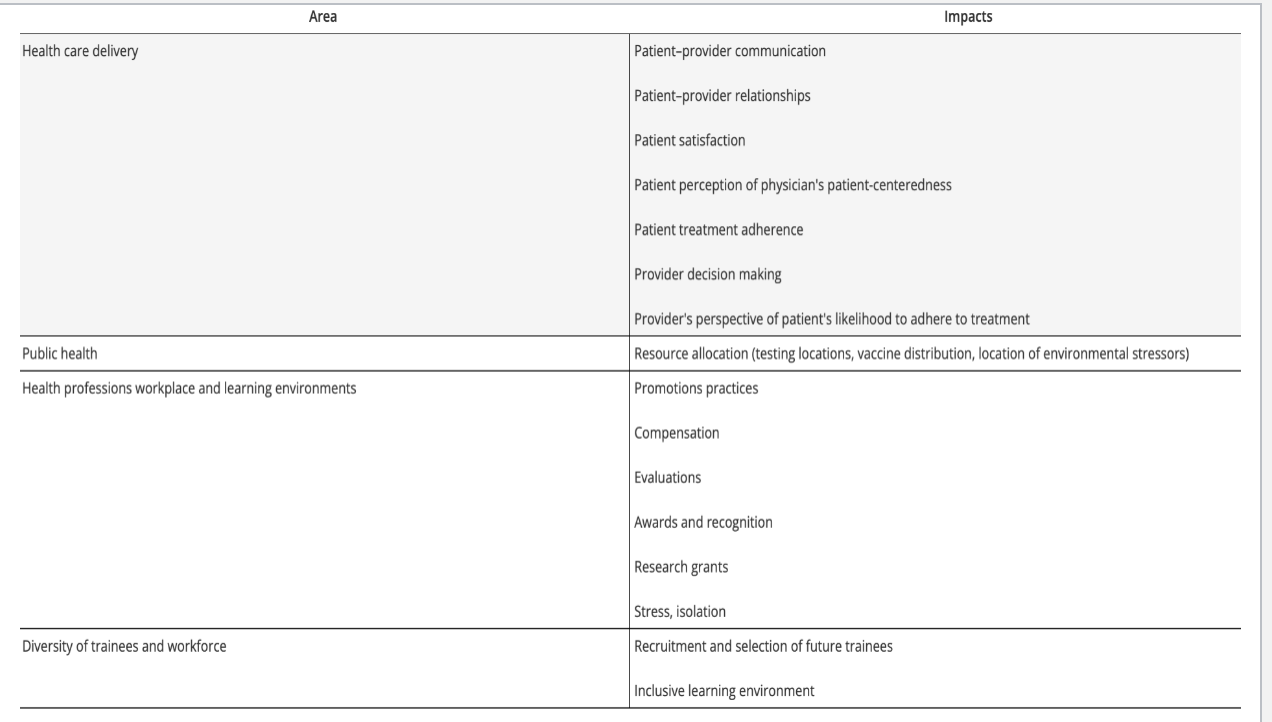
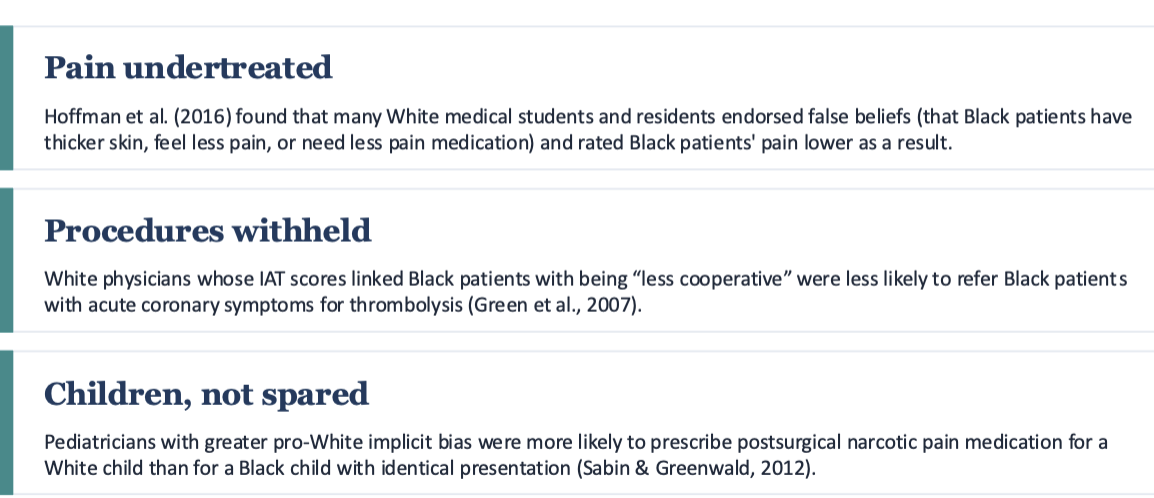
When does bias becomes care?
when pain is under-treated, procedures withheld, and children are not spared
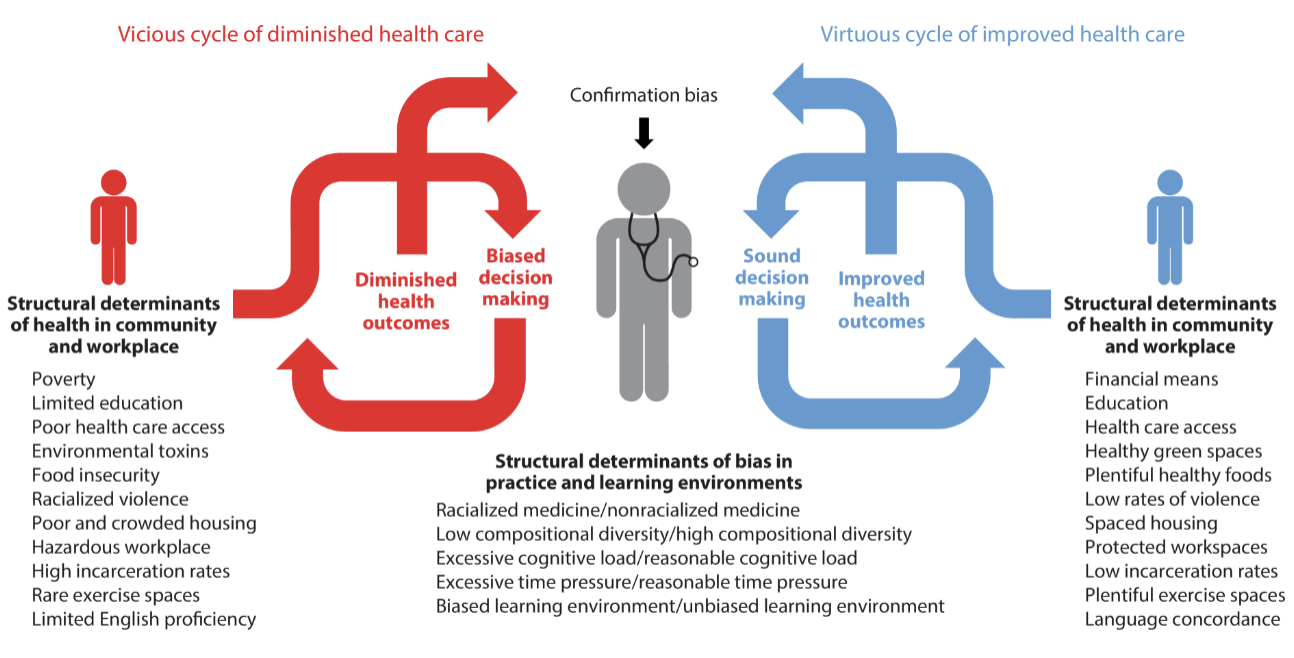
How does medical education feed the cycle?
Race as an “independent risk factor” in lectures and case presentations where Race-based algorithms for eGFR, pulmonary function, hypertension guidelines, and even pediatric UTI screening showed disparities taught without naming the structural history that produced them
Faculty and resident role-modeling → whose patients get time, whose get eye contact
Whose names appear on awards like AOA, and whose don't
Microaggressions that isolate minoritized trainees and produce stereotype threat
Differences in evaluation language across race and gender
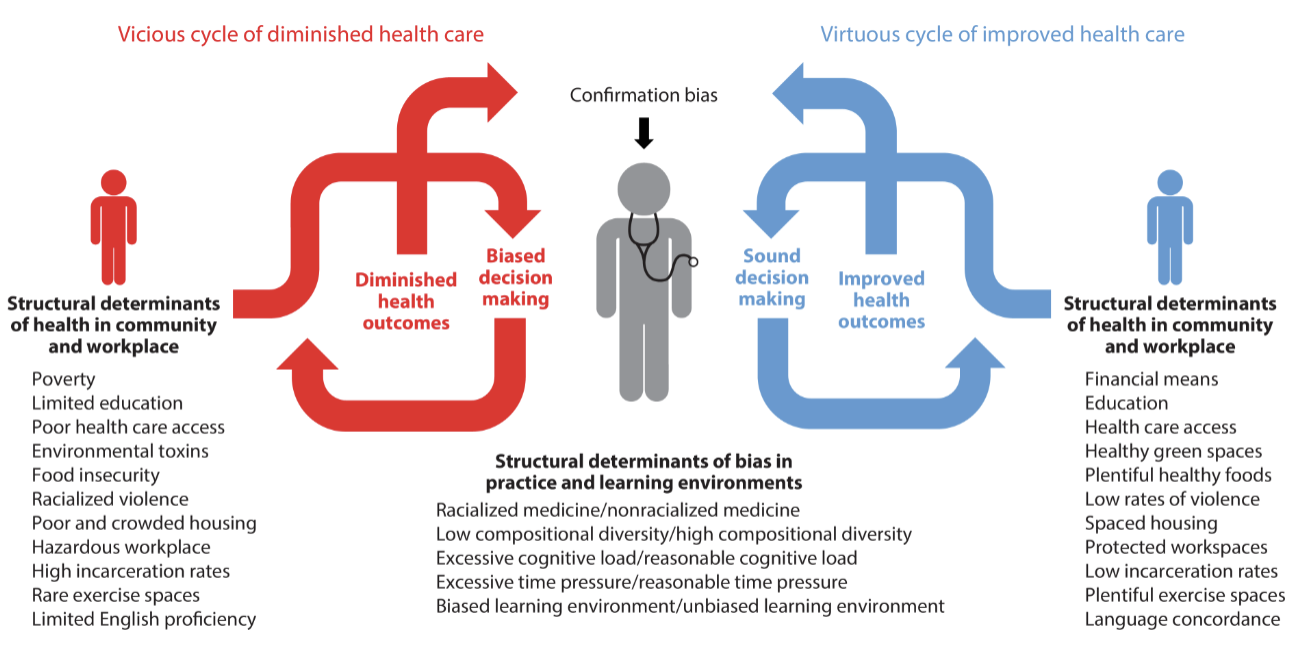
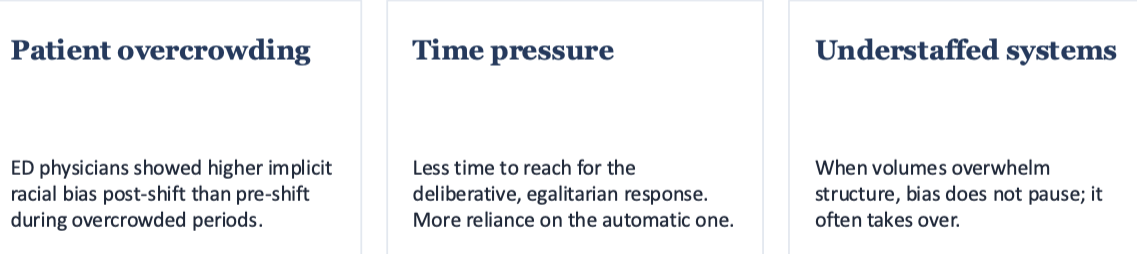
When bias stronger?
stronger when systems are strained due to being under higher cognitive load
patient overcrowding
time pressure
understaffed systems
Individuals-level strategies:
stereotype replacement
individuation
increased contact
counter-stereotyping imaging
perspective-taking
bias literacy
Stereotype replacement:
noticing a stereotyped response and deliberately substituting a non-stereotyped one
Counter-stereotypic imaging:
bringing to mind specific, vivid examples that contradict the stereotype
Transformative Learning Theory (TLT):
disrupt existing assumptions, then create a brave space for critical reflection and dialogue
Sherman et al.'s residents and faculty showed sustained commitment at 4 months
Implicit Bias Recognition and Management (IBRM):
accept that biases may not disappear and teach skills to recognize, interrupt, and manage them in real clinical moments