LAF Quizzes
1/19
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
20 Terms
Which of the following is true regarding Achilles tendinopathy?
- Increased tendon thickness
- Decreased vascularity
- Decreased neuronal growth
- Presence of inflammatory cells
Increased tendon thickness (remember: INCREASED vascularity & neuronal growth w/ ABSENCE of inflammatory cells)
A 14-year-old male cross-country runner presents to your clinic with heel pain. He describes the pain as point tenderness over the distal Achilles tendon insertion & pain w/ ankle DF. What is the MOST likely pathology?
Severs Disease

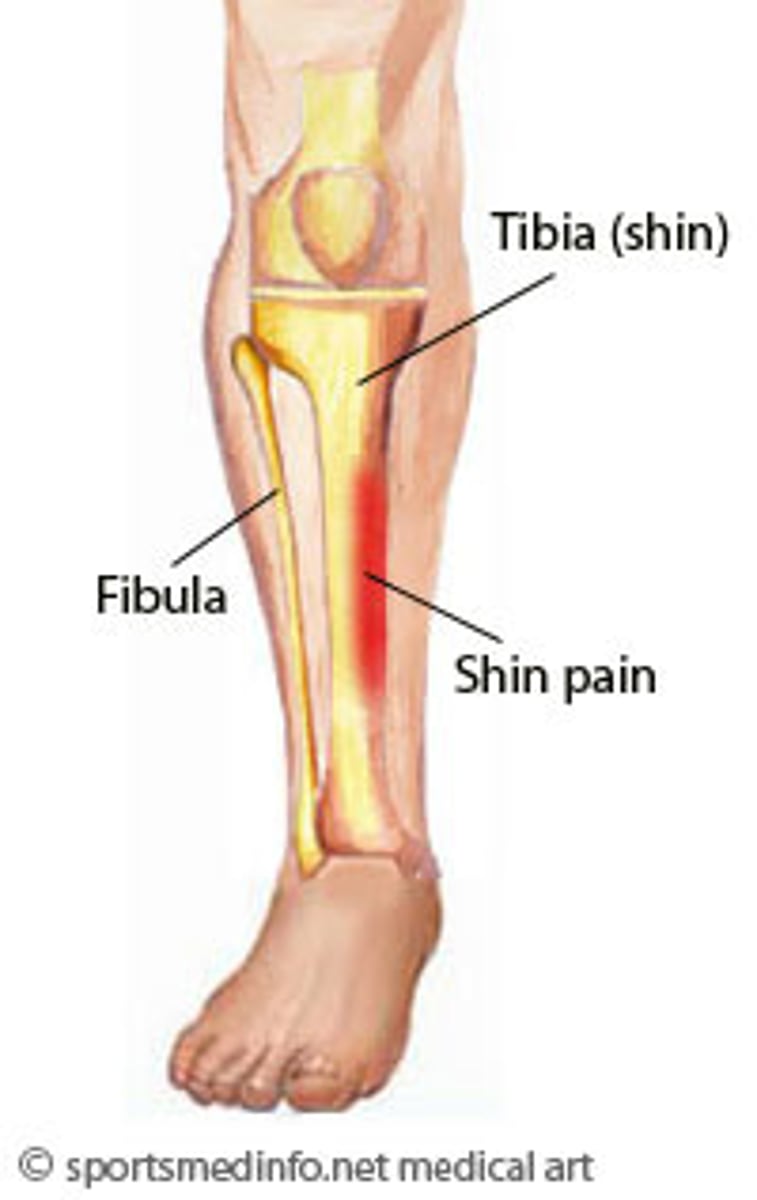
A 17-year-old female cross-country runner presents to your clinic w/ reports of diffuse pain along medial tibia that is exercise-induced. What anatomical finding is most likely?
Increased navicular drop value (based on the case, the MOST likely pathology is medial tibial stress syndrome -- associated w/ increased navicular drop value)
Your patient presents to your clinic w/ exercise-induced pain over the medial lower leg. Which structure is most likely involved?
Tibial periosteum
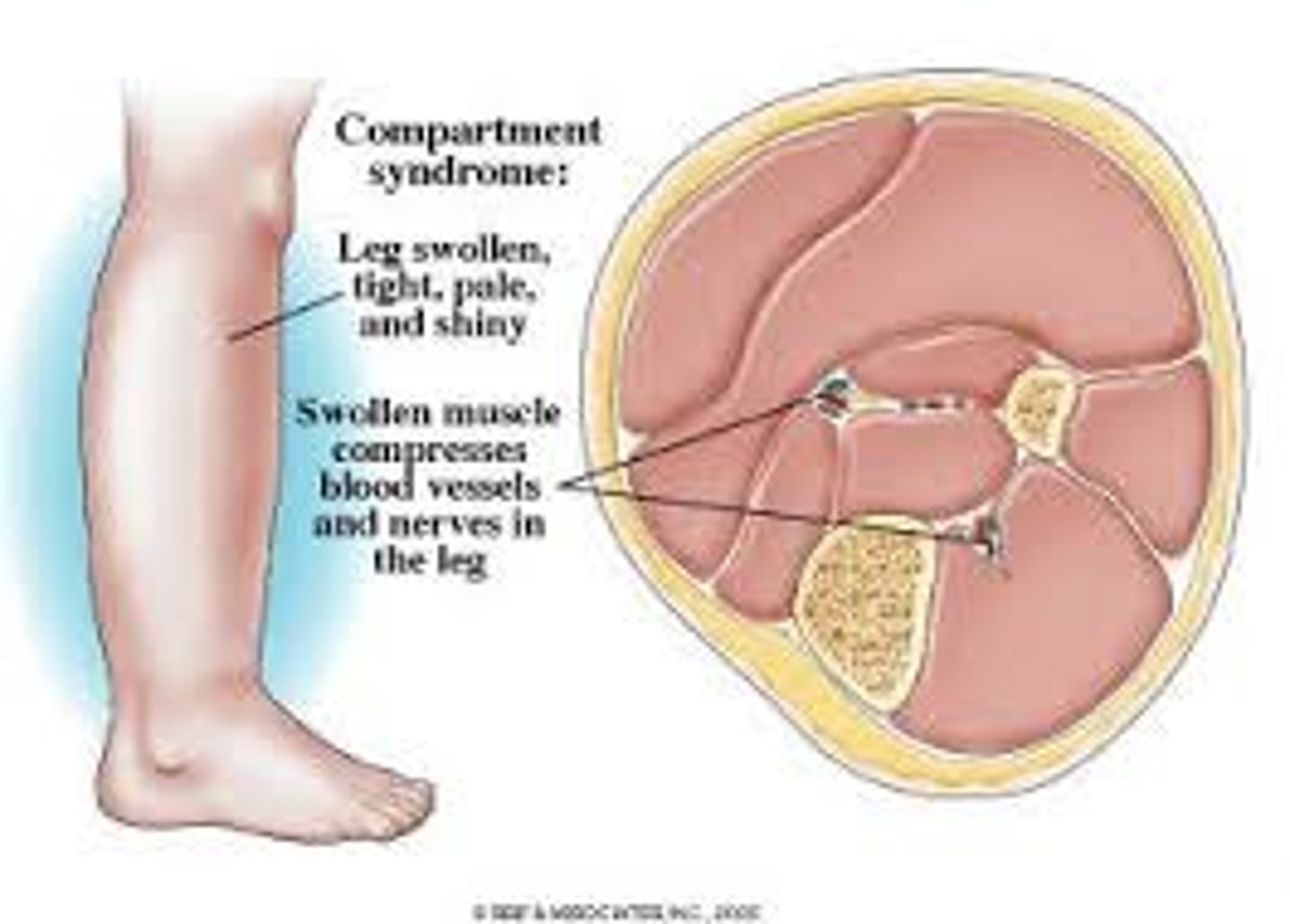
A 20-year-old basketball player reports bilateral exercise-induced anterior lower leg pain. He reports this pain begins 10 minutes into basketball practice. Which pathology is MOST likely?
Compartment syndrome (chronic exertional to be specific)
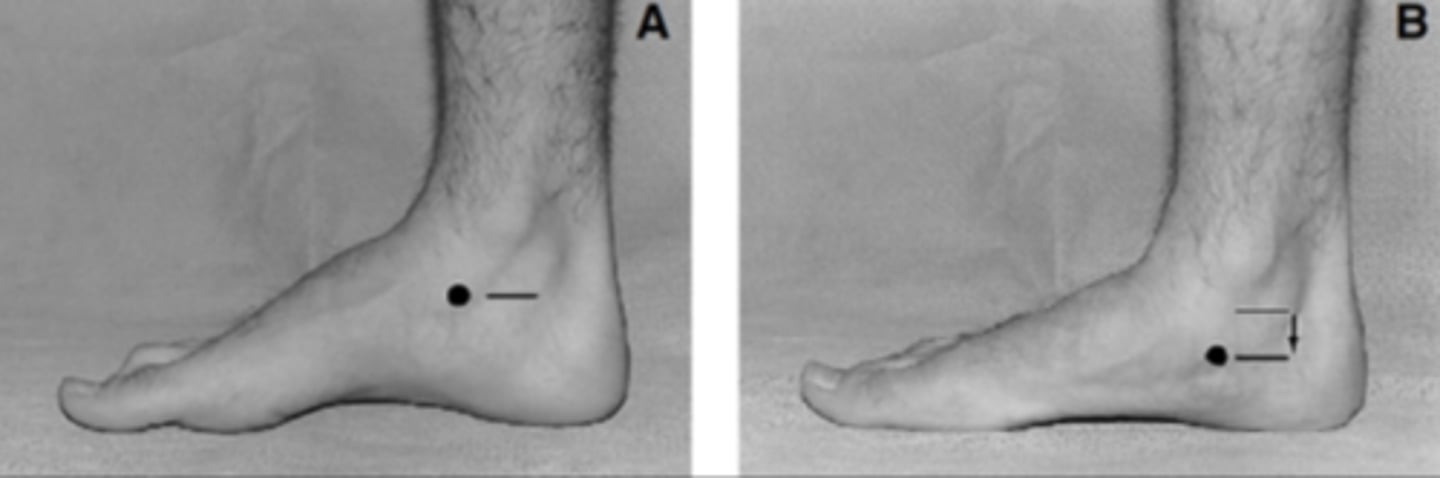
A patient presents to your clinic w/ gradual onset of medial foot pain w/ collapse of the MLA. What motion are they most likely to struggle with?
Single leg heel raise (based on the case, the MOST likely pathology is posterior tibialis tendon dysfunction — associated w/ difficulty PF)
A patient presents to your clinic w/ a minimally collapsed MLA w/ normal alignment of the hind foot. They are able to perform a heel raise. What stage of posterior tibial tendon dysfunction are they in?
Stage 1
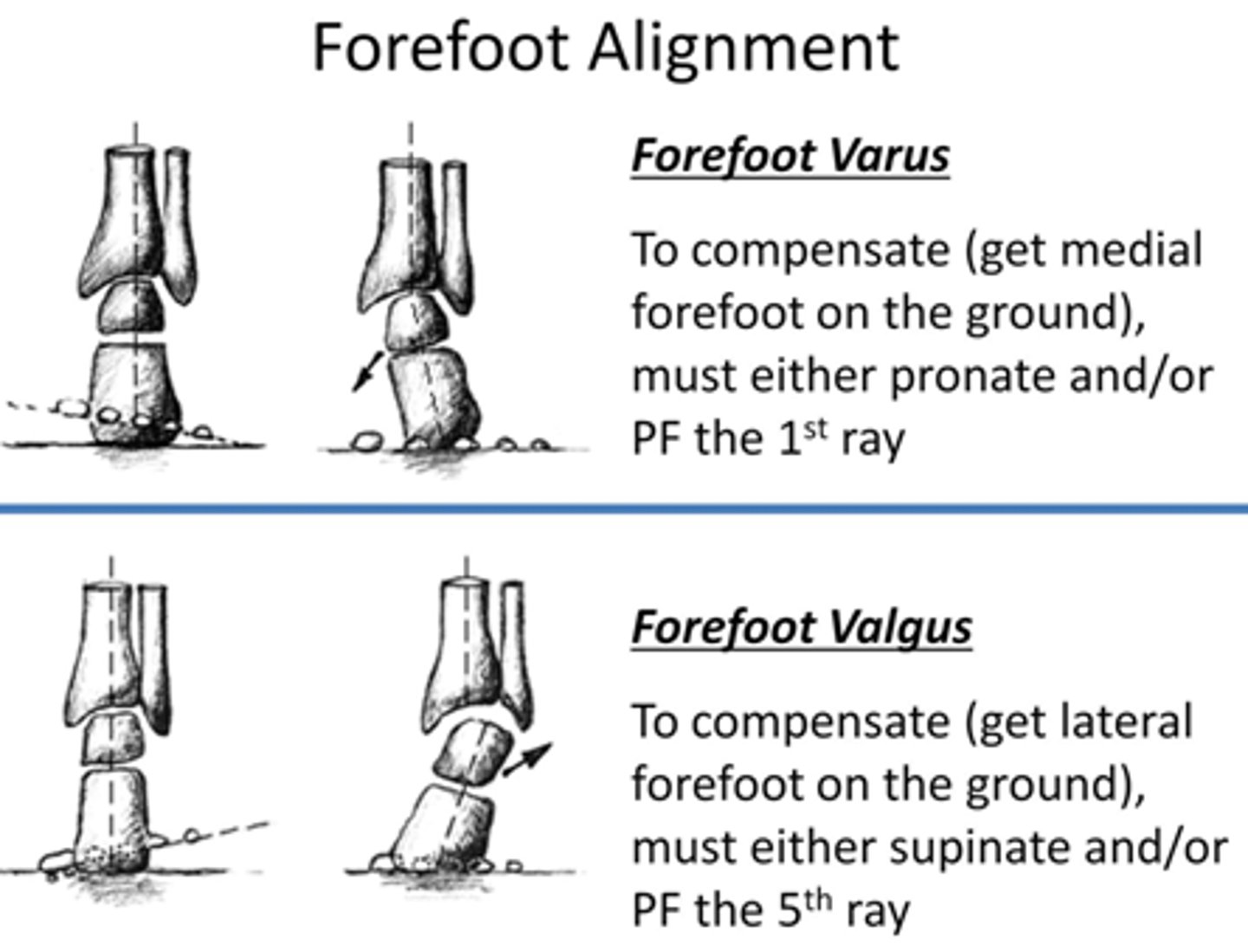
In order to compensate during weight-bearing and gait, forefoot valgus requires midfoot _________
Supination
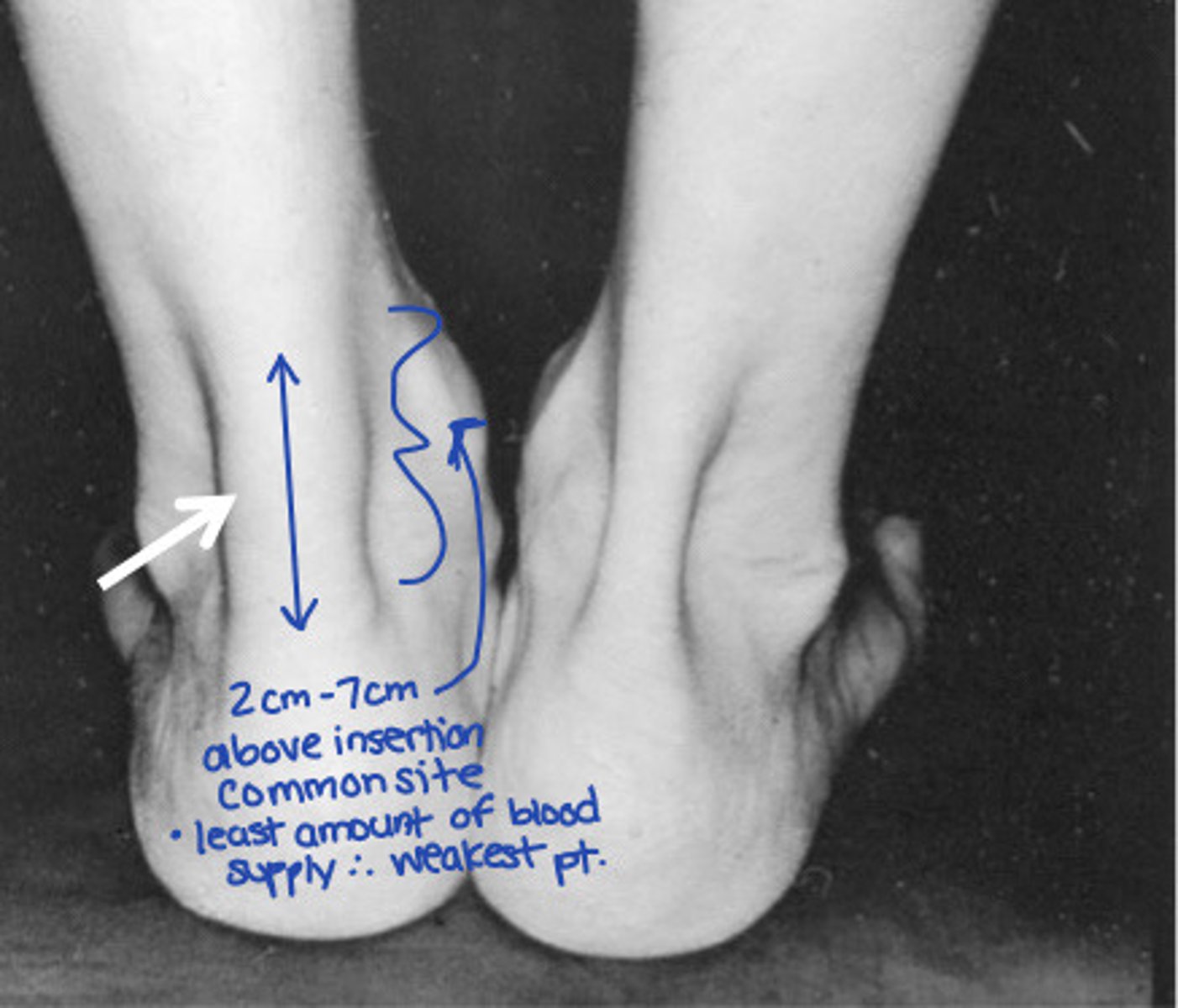
A patient presents to your clinic with 7/10 posterior ankle pain that started 8 weeks ago after increasing running duration. The pain is described as 4 cm proximal to calcaneus. Which special test would be useful?
Royal london hospital test (based on the case, we are hypothesizing Achilles tendinopathy)
A patient presents to your clinic w/ reports of ankle pain above the lateral malleolus due to an eversion ankle injury. The x-ray was negative. There is ongoing edema in lower leg/ankle w/ tenderness at the anterior tibiofibular joint. Which special test would be useful?
Squeeze test

To improve ankle DF STIFFNESS, what is the appropriate grade and mobilization @ proximal tibiofibular joint?
Grade III (or IV) anterior mob
A patient presents to you with recurrent ankle sprains, stiffness, and limited ankle DF. What is an appropriate mobilization?
Rear foot high-velocity, low-amplitude thrust manipulation
To improve eversion ROM @ subtalar joint, what is the appropriate grade and glide?
Grade IV (or III) medial glide
To improve symptoms associated w/ hallux rigidus, what is the appropriate grade and glide?
Grade IV (or III) dorsal glide
(remember: hallux rigidus is essentially OA of the big toe, which causes decreased extension ROM)
Plantar fasciopathy is associated w/ which of the following:
- Increased plantar fascia thickness
- Decreased vascularity
- Increased ankle DF
- Decreased neurogenesis
Increased plantar fascia thickness (remember: increased vascularity, decreased ankle DF, increased neurogenesis)
What is the STRONGEST contributor to disability in plantar fasciopathy?
Pain-related movements
What is the STRONGEST predictor of a (+) response w/ plantar heel pain?
Duration of symptoms
Burning b/w 1st & 2nd toes and inability to DF indicates compartment syndrome damage @ which area?
Anterior
(remember: the anterior compartment contains the deep fibular nerve, which provides sensory innervation b/w the 1st & 2nd toes as well as motor innervation to the dorsiflexors)
A patient presents w/ burning pain below medial malleolus + symptoms that are worse at night...which clinical finding would MOST LIKELY be accurate?
- (+) Windlass test
- Increased strength
- (-) Dorsiflexion-eversion test
- (+) Tinel's sign
(+) Tinel's sign
Note:
- (+) Windlass test correlates to plantar fasciopathy
- Strength would be impaired
- Nerve damage to the tibial nerve would result in a (+) dorsiflexion-eversion test
A patient presents w/ burning pain b/w 3rd & 4th MT head + sensation of stepping on a pebble...what is the MOST LIKELY pathology?
Interdigital nerve damage (Morton's neuroma)