Surg Med - Drains, Tubes, and Lines - Exam 2
1/50
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
51 Terms
Surgical Drain Function
Allows air to escape
Allows liquid accumulation to be evacuated
Prevents collections that would elevate a skin flap
Minimizes dead space
Decompresses the wound
Intra-abdominal drains are a window into the abdomen
Seroma
Serous fluid in dead space that prevents proper tissue adhesion and healing
Seroma RF
obesity
lymphatic disruption
any surgically created dead space
Seroma Presentation
painless, fluctuant swelling
fluid wave
clinical +/- US
what is the diagnosis for a seroma?
Seroma Dx
prevent with drains
compression
aspiration
Hematoma
post-op bleeding into tissue
promotes infection, delays wound healing, increases inflammation and pressure
Anticoags, poor hemostasis
what are risk factors for a hematoma?
Hematoma Presentation
tender, firm swelling with discoloration
clinical, imaging if deep
what is the dx for a hematoma?
Hematoma Tx
observation vs surgical evacuation
Active Drains (Jackson-Pratt, Blake, Hemovac)
Use suction (bulb or wall) to draw fluid
Reduces infection risk
Hemovac
Used in ortho, spine, abdominal surgeries
Bulky but larger reservoir (up to 400 mL)
Slightly stronger suction
Passive Drains (Penrose)
Rely on gravity/capillary action
Allow fluid to exit without suction
Remove before 5 days or granulation tissue forms
Drain Removal
Most drains can be removed if they are putting out less than 30cc/day
Always wear gloves
Apply pressure at insertion site
Sometimes significant force may be required to remove the drain
Suturing of the drain site on case-by-case basis
Gastrostomy Tube
Placed percutaneously directly into stomach or through open surgical incision in the abdomen
PEG (percutaneous endoscopic gastrostomy) vs "open" G-tube
Provides adequate nutrition and delivery of medications
G Tube Indications
Dysphagia
Difficulty chewing
Poor PO intake/malnutrition
Aspiration
Intractable emesis
Severe reflux
Duodenostomy Tube
A tube placed into the duodenum, most commonly used for: Decompression, Drainage, Protection of a duodenal repair
NOT typically routine long-term feeding
D Tube Indications
Duodenal trauma
Perforated ulcer repair
Complex upper GI surgery
Anastomotic protection
Jejunostomy Tube
Feeding tube surgically placed into the jejunum
J Tube Indications
Esophageal/stomach/duodenal pathologies
Esophageal cancer
Gastroparesis - poor gastric emptying
Duodenal injury
Do not bolus feed
Cholecystostomy Tube
Used when gallbladder is too inflamed for removal
May be useful when patient is too ill to tolerate surgery
May be done percutaneously by IR or during laparoscopic/open procedure
Access for cholangiography
Goal is to decompress biliary system
T-Tube (Biliary Drainage)
Placed into common bile duct to drain bile
Decompress the biliary tree after surgery
Prevents pressure buildup or leakage
Allow access for imaging (T-Tube cholangiogram)
T Tube Indications
Cholangitis
Biliary stricture
Bile duct surgery/repair
Chest Tube
Removes air in the pleural space - pneumothorax
Removes fluid in the pleural space - hemothorax, pleural effusion, chylothorax
Removes pus from pleural space - empyema
Thoracostomy Tube
Free end is attached to an underwater seal below the level of the chest
Allows air or fluid to be removed from the pleural space but prevents anything from returning to the chest
Local anesthetic used; small incision made
Patient instructed to do a deep inspiration to depress the diaphragm
Cecostomy Tube
Accesses the colon directly for removing gas, stool, or irrigating the colon
Flushes help push stool toward the rectum
Reverse enema port
C Tube Indicatons
Neurogenic Bowel/Chronic Constipation
Severe Fecal Impaction
Central Venous Access
Fast, reliable central access - often urgent/emergent placement
Often for patients in intensive care
Monitoring for central venous pressure (CVP)
CVA Common Sites
Internal jugular
Subclavian (lower infection risk)
Femoral (higher infection/thrombosis risk)
Terminates in the SVC just above the right atrium
CVA Indications
Drugs that can't be given peripherally - vesicants/irritants that can cause severe damage to tissue if extravasated
Frequent blood draws
Resuscitation
Long term abx
Long term TPN - high osmolality solution that can damage peripheral veins
CVA - Common Drugs
Calcium Chloride
Chemo
Hypertonic saline
Potassium chloride
Amiodarone, levophed, epi
CVA Comp
Always CXR after placement
Look for correct placement and possible comp → PTX/hemothorax
Other comp: Infxn, Hemorrhage, Hematoma, Arrhythmia, Air embolism
CVA Removal
Trendelenberg position if possible
Ask patient to hold breath or time the removal on the patient's expiration
Hold pressure on the removal site for 5 minutes and cover with occlusive dressing
Leave dressing in palace for 24 hours
Tunneled Central Venous Catheter (Hickman)
Visible, external tubing
Direct external access
Requires routine flushing + drainage
Higher infection risk
Ideal for daily access (TPN, frequent labs)

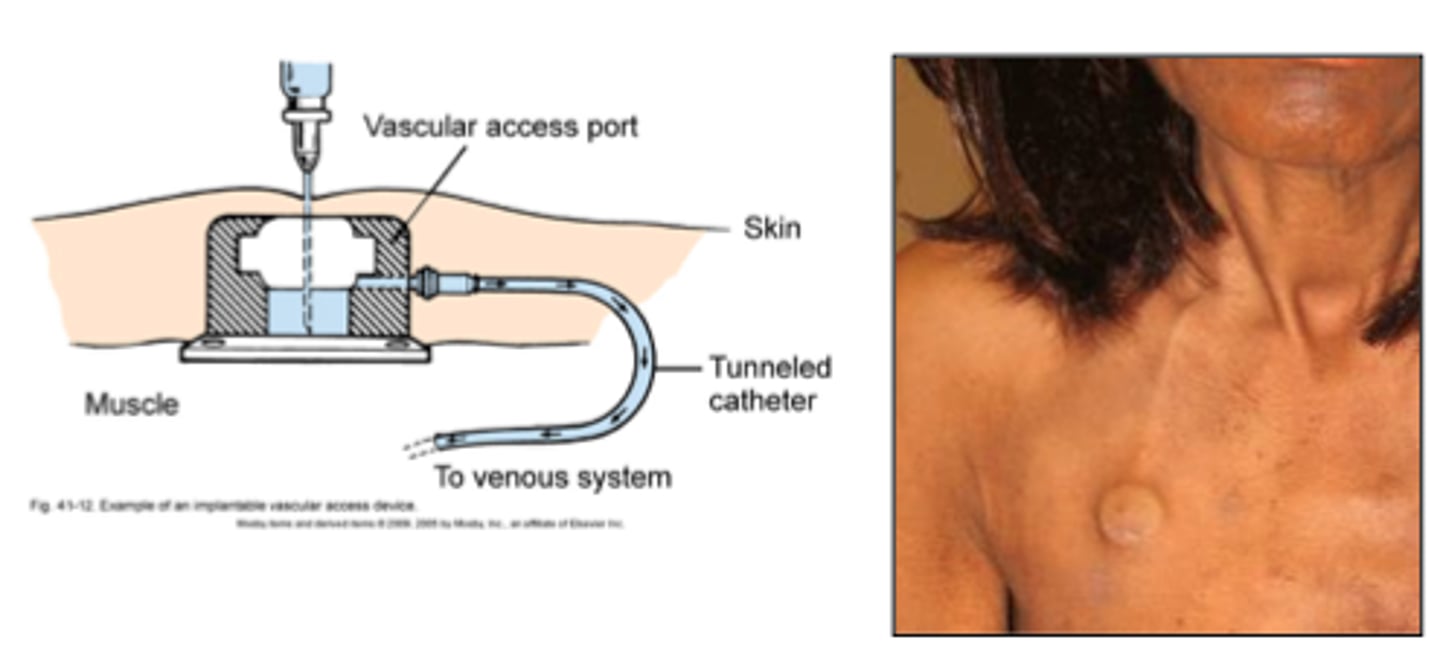
Implanted Venous Access Ports (Port-A-Cath)
Not visible (completely under skin)
Needle access through skin
Maintenance minimal when not accessed
Lower infxn risk
Ideal for intermittent chemo, outpatient use
Peripherally Inserted Central Catheters (PICC)
Inserted:
Basilic/brachial/cephalic vein
Tip ends centrally in the SVC, just above the right atrium
PICC Advantages
Bedside placement
Good for prolonged abx
PICC Disadvantages
DVT risk
Cannot always support high flow
Not ideal in CKD patients needing future fistulas
Midline Catheters
Midline tip does NOT reach central circulation
Use:
-Intermediate-duration therapy (<1 month)
-Difficult access
-IV abx not requiring central delivery
-Single lumen
Midline Catheters - Do NOT use
Vesicants
TPN
Many pressors
Peripheral IV Catheter Indications
Short-term
Non-vesicants
Routine fluids/meds
PIV Catheter Limitations
Short duration
Extravasation risk
Limited flow/longevity
Arterial lines
Purpose:
-Continuous BP monitoring
-Frequent ABGs
Most common site: radial artery
Art Line Comp
Thrombosis
Ischemia
infection
Temporary Dialysis Catheter
Large bore
Non-tunneled
IJ preferred
Use: emergent dialysis
Tunneled Dialysis Catheter
Longer-term dialysis access
Lower infection risk
Dialysis Catheters Major Comp
Infection
Central stenosis
Thrombosis
Pulmonary Artery Catheters (Swan-Ganz)
Measures:
-Pulmonary artery pressures
-Cardiac output
-Filling pressures
Pulmonary Art Catheter Uses
Cardiogenic shock
Advanced ICU management
Complex heart failure
Pulmonary Art Catheters Classic Comp
Arrhythmias during insertion
Pathway: RA → RV → PA