RTE 1032 - Unit 4 (Spine)
1/103
Earn XP
Description and Tags
Spine
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
104 Terms
AP Open Mouth: Eval Criteria
Entire odontoid process, atlantoaxial joint, and lateral masses of C1 demoed
Upper incisors and base of skull are superimposed
Atlantoaxial joint is symmetrical
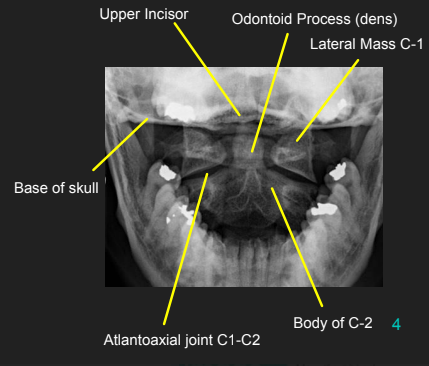

AP Open Mouth: Is this Image Good?
No.
Base of skull superimposed over dens and lateral masses
Atlantoaxial joint is not clearly demoed
Extensive extension of skull
Reposition by slight flexion of the neck or angle the CR slightly caudal
How do you take an AP Open Mouth with a C-collar on?
Have the patient open their mouth, then match your CR angle to the biting plane of their upper teeth
Usually about 3-5 degree caudal angle
Do not take off the C-collar

AP Open Mouth: Is this Image Good?
No.
Front incisors are superimposed over C1-C2
Atlantoaxial joint is not demoed
Excessive flexion of skull and neck
Reposition with slight extension of the neck or angle the CR slightly cephalic
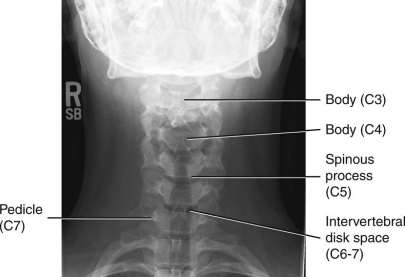
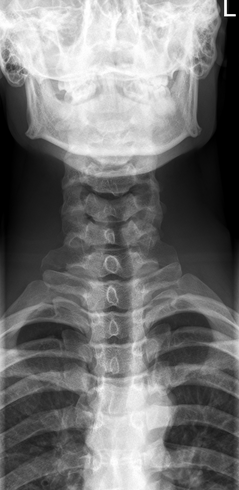
AP Axial C-Spine: Eval Criteria
Angle CR 15 to 20 degree cephalad neck extended slightly
C3 to T2 demoed
Space between pedicles and intervertebral disk spaces clearly seen
Mandible and base of the skull should superimpose C1-2
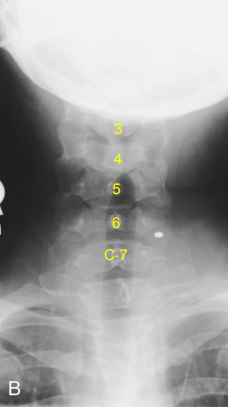
AP Axial C-Spine: Is this Image Good?
No.
Vertebral body of C3 is partially superimposed by base of skull
Incorrect CR angle (caudal) produced foreshortening of vertebral bodies and closure of intervertebral joint spaces
Excessive extension superimposed base of skull over upper C-Spine
Correct the angle and adjust head so that a line from lower margin of upper incisors to the base of the skull is perp. to IR
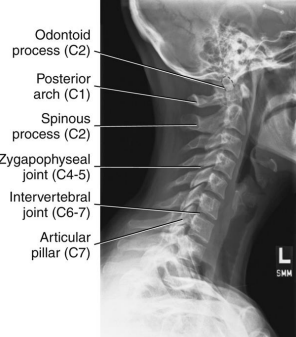
Lateral C-Spine: Eval Criteria
Cervical vertebral bodies, intervertebral joint spaces, articular pillars, spinous processes, and zygapophyseal joints demoed
C1 through C7-T1 intervertebral joint spaces are clearly seen
R and L articular pillars and zygapophyseal joints should be superimposed for each vertebra
Bodies free of superimposition of the articular pillars
Spinous process seen in profile
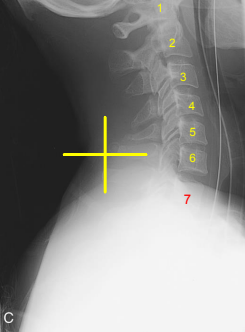
Lateral C-Spine: Is this Image Good?
No
C7 is obscured
C1 anatomy is clipped and spine is not centered
Need to center higher and more anterior
Tilt leads to poor superimposition of zygapophyseal joints
Used AEC but it wasn’t centered to bone (underexposed)
Swimmers: Eval Criteria
CR to T1
Vertebral bodies and intervertebral disk spaces of C5 to T3 are shown
Humeral head and arm farthest from the IR are magnified and appear inferior to T4 or T5
Minimal vertebral rotation indicated by superimposition of cervical zygapophyseal joints and articular pillars, and posterior ribs
Humeral heads should be separated vertically

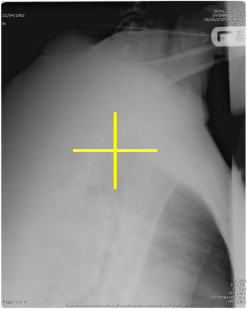
Swimmers: Is this Image Good?
No
CR is too low
Move up to T1
Foggy, noisy, low contrast (underexposure)
Increase kVp
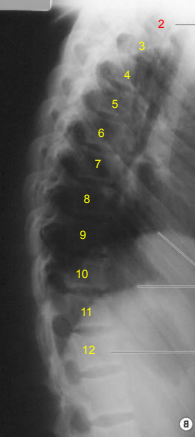
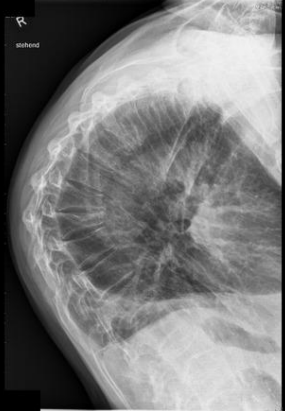
Lateral T-Spine: Eval Criteria
Thoracic vertebral bodies, intervertebral joint spaces, and intervertebral foramina
T1 to T3 will not be well demoed
Intervertebral disk spaces should be seen
Excessive rotation indicated by > 1/2” of space between separated posterior ribs
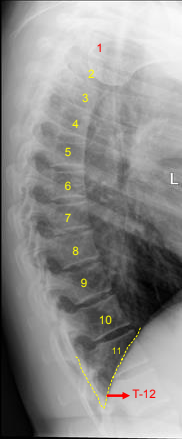
Lateral T-Spine: Is this Image Good?
No
Missing part of T1
Blurry - we want ribs blurred not the vertebrae
Ask pt to stay still while taking breaths
Separated posterior ribs indicate rotation at the superior aspect of spine
Overexposed
Decrease mAs
How does rotation manifest on an AP Open Mouth odontoid?
Asymmetrical lateral masses and off-center alignment of spinous process of C2
How does rotation manifest on an AP Axial C-Spine?
Spinous processes will be off-centered
How does rotation manifest on a Lateral C-Spine?
Poor superimposition of the zygapophyseal joints and articular pillars
How does rotation manifest on a Swimmer's?
Poor superimposition of zygapophyseal joints, articular pillars, and posterior ribs
How does rotation manifest on a Lateral T-Spine?
Poor superimposition of posterior aspects of vertebral bodies and >0.5" of separation between posterior ribs
To accomplish proper flexion or extension of the head and neck for an AP Open Mouth Odontoid, the ___ and ___ should be superimposed.
Upper incisors and base of skull
For AP Open Mouth Odontoid imaging, the base of the skull and/or the upper incisors will be projected about 1" for every ____ angulation.
5 degrees caudal
Poor superimposition of the zygapophyseal joints on a lateral c-spine indicates ____.
Tilt
Excessive rotation of a lateral T-spine is indicated by ____ space between the posterior ribs.
>1/2 inch
Exposure Factors for Spine Imaging
No changes in exposure factors for anything but patient size
What are symptoms of spinal injuries?
Pain, sensory loss, weakness, paralysis, and/or death
Compression
Partial collapse
Distraction
Horizontal fx and separation of posterior elements
Subluxation
Partial dislocation
Once baseline AP/Lat x-rays have been taken, ____ is usually indicated for spinal injuries.
CT
Paralysis
Loss of motor and sensory function below the spinal cord injury
Upper c-spine injuries can cause tetraplegia (quadriplegia)
Life expectancy for ventilated tetraplegic patients is ____.
Risks of tetraplegia include:
1-2 yrs
Blood clots and sepsis due to pneumonia, urinary infections, renal failure, and pressure sores
True or false: It is possible to reverse complete spinal cord damage and paralysis.
False; only patients with partial paralysis may regain functionality
Lordosis is exaggerated/abnormal ___ curvature of the ___ spine.
Concave
Lumbar
Kyphosis is exaggerated/abnormal ____ curvature of the ____ spine.
Convex
Thoracic

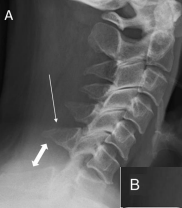
Clay Shoveler’s Fx
Avulsion fx of the spinous processes of C6-T1 due to excessive strain on the neck when lifting heavy objects above head
Clay shoveler's fractures are best demonstrated on a ___.
Lateral C-Spine
Clay shoveler's fractures are considered stable fractures, meaning that the bone is ____ but still in alignment with ____.
Cleanly broken
Ligaments and tissues intact
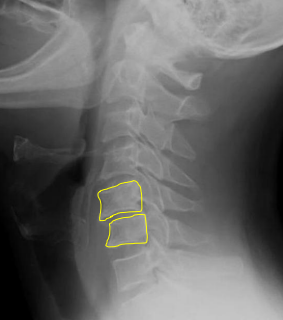
Facets - Unilateral Subluxation
C-spine injury involving flexion, distraction, and rotation resulting in only 1 zygapophyseal joint out of alignment
Spine is not stable, surgery required
A unilateral subluxation of the facet will result in the vertebral body being ____, creating a ____ artifact on the lateral C-spine image.
Rotated
Bowtie
Facet subluxation will require post-op ____.
Halo immobilization

Halo Vest
Brace used to immobilize and protect the c-spine after surgery or trauma; usually worn for 6-12 weeks
Create OID on XR
Halo vests are attached via ____ into the skull. The sites of these attachments must be frequently monitored for ____.
Pins
Infection
Facets - Bilateral Locks
Extreme flexion and distraction, with both right and left zygapophyseal joints on the same level disrupted created bilateral locked facets
In bilateral facet locks, the affected vertebral body ____ the body immediately inferior.
Jumps over
___ is required for bilateral facet locks due to distress of the spinal cord.
Surgery
Halo post-op
Hangman’s Fx
Extreme hyperextension, resulting in fx that extends through the pedicles of C2, with or without anterior displacement of C2 on C3
Immb. or surgery
A patient with a hangman's fracture is not stable because the intact ____ is pressed posteriorly against the ____.
Odontoid
Brain stem
Hangman's fracture is best demonstrated on ____.
Lateral C-Spine

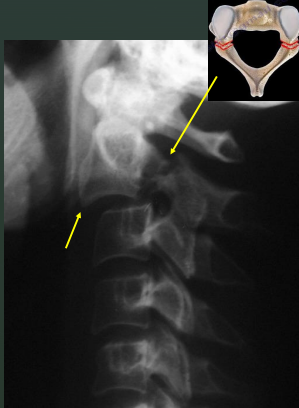
Jefferson Fx
Comminuted atlas fx as a result of axial loading, e.g. landing on one’s head or abruptly on one’s feet
Ant. and post. arches of C1 are fx
Post-op halo
Jefferson fractures are indicated by asymmetry in the odontoid view with displacement of the _____ away from the dens.
Lateral masses

Odontoid Fx
Fx of dens and can extend into the lateral masses or arches of C1
Odontoid fractures may result from _____ or a _____ injury.
Hyperflexion/extension
Compression
If an odontoid fracture causes further fracture dislocation/injury to the upper spinal cord, it may lead to _____ or _____.
Tetraplegia or respiratory arrest
Odontoid fractures are best demonstrated on ____.
AP Open Mouth

Teardrop Burst Fx
Comminuted fx to the lower cervical vertebral bodies caused by compression with hyperflexion
Teardrop burst fractures indicate extensive underlying ______ injury and spinal _____.
Ligamentous
Instability
It is highly probable that a teardrop burst fracture will cause ____.
Neurologic Damage/Quadriplegia
In a teardrop burst fracture, triangular fragments avulsed from the ____ border of the vertebral body and fragments from the ____ border are displaced into the spinal canal.
Anteroinferior
Posterior
Kyphosis
Abnormal or exaggerated convex curvature of the T-spine that results in stooped posture and reduced height
Kyphosis is often caused by compression fractures of the ____ edges of vertebral bodies.
Anterior
Risk factors for kyphosis include:
Osteoporosis
Poor Posture
Rickets

Scoliosis
Abnormal or exaggerated lateral curvature of the spine
Most common in 10-14 y/o, more in females
Severe scoliosis cases may complicate ____ function and require surgery.
Cardiac and respiratory
Treatment for scoliosis includes ____ which can be adjusted as the child grows.
Expandable, permanent correction rods
Spondylitis
Inflammation of the vertebrae
Spondylosis
Neck stiffness due to age-related degeneration of intervertebral disks.
Can contribute to arthritic changes
Spondylolisthesis
Forward movement of one vertebra in relation to another.
Spondylolisthesis commonly occurs due to a developmental defect in the ____, spondylolysis, or severe osteoarthritis.
Pars Interarticularis
Spondylolysis
Stress fx through the pars interarticularis of the lumbar vertebrae

C-Spine Odontoid: Which options are true?
A repeat with more flexion of the head/neck is needed
A repeat with more extension of the head/neck is needed
The R/L marker is incorrect
This is a well-positioned radiograph; no repeat required.
2 and 3
Repeat with more extension of the head/neck is needed
R/L marker is incorrect

Which of the following statements are correct regarding the Odontoid radiograph below?
The atlantoaxial articulation is well demonstrated
The odontoid process is incompletely visualized
More flexion is required to move upper incisors inferiorly
More extension is required to move base of skull more inferiorly
1, 2, and 3
The atlantoaxial articulation is well demonstrated
The odontoid process is incompletely visualized
More flexion is required to move upper incisors inferiorly
Evaluate the AP Axial C-spine radiograph below and select any of the statements that are true (multiple answers possible):
Not all required vertebrae are demonstrated
There is excessive extension of the head/neck
The R/L marker is incorrect
This is a well-positioned radiograph; no repeat required.
1 only
Not all required vertebrae are demonstrated

Evaluate the Lateral C-spine radiograph below and select any of the statements that are true (multiple answers possible):
All required vertebrae are demonstrated
A repeat with more flexion of the head/neck is needed
The R/L marker is correct
This is a well-positioned radiograph; no repeat required.
3 only
The R/L marker is correct
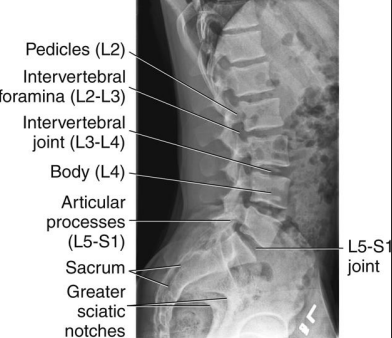
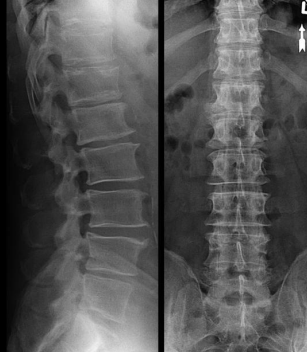
AP L-Spine: Eval Criteria
Centered at the crest (or 1.5” above) to include T12 to sacrum
No rotation
Open intervertebral joint spaces
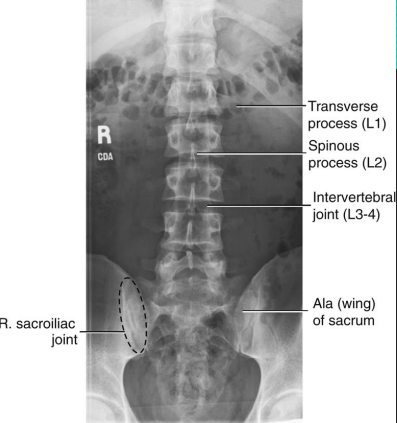
How does rotation manifest on an AP L-spine?
SI joints unequal from spinous processes
Spinous processes shifted to either side of midline of vertebral column
Transverse processes of unequal length
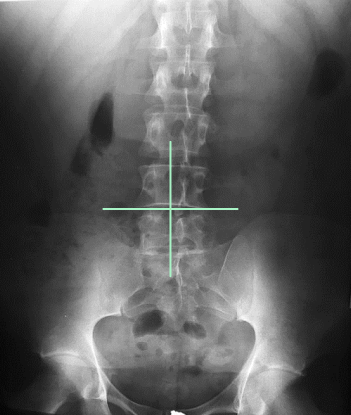
AP L-Spine: Is this Image Good?
No.
Slight right rotation evidenced by spinous processes projected to the left of midline
T12 is clipped due to low centering at the crest
Needs collimation
Needs marker
Lateral L-Spine: Eval Criteria
Centered at the crest to include T12 to sacrum
Spinal column aligned parallel to the IR
No tilt
No rotation

Lateral L-Spine: Is this Image Good?
No
Note: There are 6 lumbar vertebrae
Rotation and tilt begin in L4 and gets progressively worse as you move up the spine
Stack the hips and shoulders (fixes rotation) and place a support sponge under the waist (fixes tilt)
Overexposed; loss of contrast; decrease kVp
Marker cut-off
Rotation Lateral L-Spine
Separated posterior vertebral bodies
Spinous process shifted to the right of midline = slight LPO
Tilt (or ____) Lateral L-Spine
Sagging
Indicated by closed intervertebral foramina and joint spaces
To fix rotation on a lateral L-spine, ensure the ____ are stacked. To fix tilt or sagging, place a _____ under the patient's waist.
Hips and shoulders
Support sponge
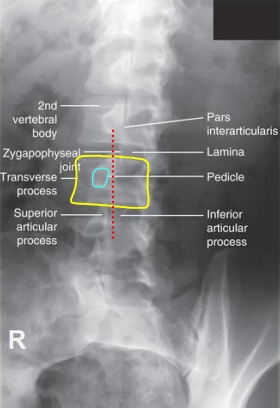
Oblique L-Spine: Eval Criteria
45 degree rotation indicated by 5 Scottie dogs stacked on top of each other
Open zygapophyseal joints and the pedicle between the midline and lateral aspect of the vertebral border
May be different at L1 and L5 - Evaluate the L3 pedicle
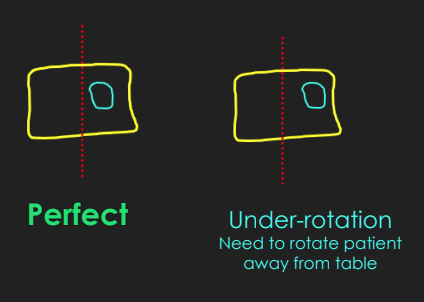
Oblique L-Spine Under-Rotation
Pedicle is situated away from the vertebral body midline toward lateral border
More of the lamina is demoed (body of dog)
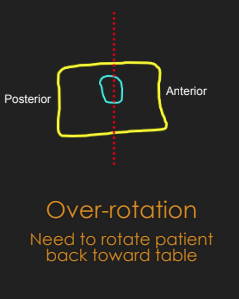
Oblique L-Spine Over-Rotation
Pedicles are demoed closer to vertebral body midline, and less of the lamina is demoed
Lordosis
Abnormal or exaggerated concave lumbar curvature
Lordosis may result from:
Pregnancy
Obesity
Poor Posture
Rickets
Lordosis can cause ____, ____, and ____.
Muscle pain
Numbness
Weakness
_____ will best demonstrate the extent of lordosis. ____ views can also be helpful in indicating more aggressive treatment.
Lateral L-Spine
Flex/Ext

Ankylosing Spondylitis
Inflammatory disease that can cause vertebrae to fuse - new bone forms in an attempt to heal inflammation, more common in males
“Bamboo spine”
Ankylosing spondylitis makes the spine ____, less ____, and can result in ____ posture.
Flatter
Flexible
Hunched
In ankylosing spondylitis, calcification occurs at the ____ ligament.
Anterior longitudinal
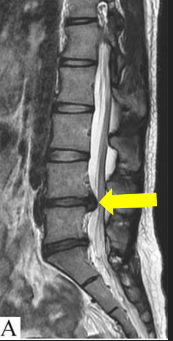
Herniated Nucleus Pulposus
aka Slipped Disk. Soft inner part of the intervertebral disk protrudes through the fibrous outer layer, pressing on the spinal cord or nerves
HNP is usually caused by ___.
Improper lifting
HNP most frequently occurs at vertebral level ___, causing ___.
L4/5
Sciatica
Which modalities are best in evaluating HNP?
CT/MRI
True or False: some HNPs may heal and resolve over time.
True

Chance Fractures
Result from a hyperflexion force that causes fx through the vertebral body and posterior elements
Posterior aspects of the vertebrae that may be damaged in a chance fracture include:
Spinous process
Pedicles
Facets
Transverse processes
Transitional Vertebrae
Often an incidental finding that occurs when the vertebra takes on a characteristic of the adjacent region of the spine
Not directly linked to any problems
Congenital anomaly 25% of population
Sacralization
L5 assimilates to the sacrum
Lumbarization
S1 acts as a 6th rib-free lumbar vertebra
Transitional vertebrae can also affect L1, which has _____ that present as short ribs.
Elongated transverse processes