Learning and Memory
1/23
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
24 Terms
What are the four steps of memory formation?
Describe what each means
Each new memory is formed by four sequential processes:
Encoding
newly learned information → integrated w/ past knowledge
Consolidation
information converted → form that can be permanently stored.
Associated with structural changes in the brain.
Storage
deposition into final resting places.
Retrieval
accessing stored memories.
Subject to distortion.
Dependent on working memory.
What are the two primary types of memory?
Define each one
two primary types:
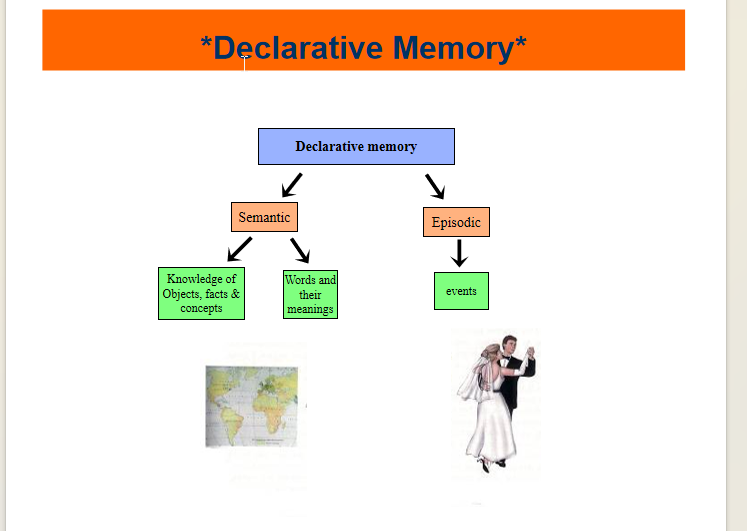
Declarative (explicit) memory
Info available to consciousness and can be expressed by language
EX: remembering telephone # or images of events that have happened.
Nondeclarative (implicit) memory
Info that largely cannot be retrieved @ conscious level,
EX: how to perform tasks - riding a bicycle or gymnastic maneuvers.
NOTE: These primary types of memory are associated with different circuitries that can be distinguished by different types of damage.
Draw out the different type of declarative memory
List the Anatomical Substrates For Declarative Memory
Describe how each substrate contributes to the stages of memory formation
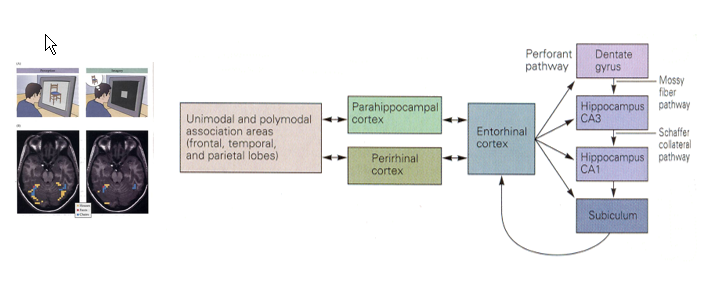
neural circuitry: circuit of Papez
association area of neocortex
(prefrontal, limbic & parieto-occipital-temporal)
cortical region surrounding hippocampus
(perirhinal, parahippocampal & entorhinal cortices)
Hippocampal formation
(dentate gyrus, CA1-3, subiculum)
Steps/Substrate:
Encoding: association cortex
Consolidation: hippocampal formation + surrounding areas cortex
Storage: transferred to association cortex
Retrieval: reactivation of brain regions involved in sensory perception
Draw out the neural pathway for declarative memory formation
Describe what happens in memory if lesion of temporal lobe occur:
consequences
what is spared?
How does this occur?
Lesion of temporal Lobe:
Consequences:
cannot consolidate information → long term memory.
What is spared:
immediate and some short-term memory,
old memories
procedural memory
intelligence
simple reflexive learning.
In general, bilateral injury is required to produce appreciable deficits in this system.
NOTE: Different forms of learning (i.e. spatial representation, words, object recognition) are affected differentially by lesions in different locations of hippocampus and surrounding cortices.
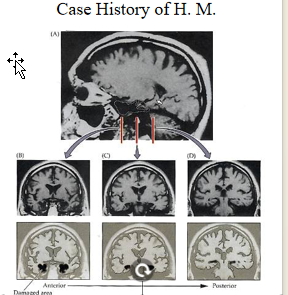
Describe the Case history of HM
MRI scan of H.M. brain: Patient sustained a large bilateral resection of the medial temporal lobes including entorhinal cortex, most of perirhinal cortex, amygdala & about half of hippocampus in an effort to relieve severe epilepsy that resulted in profound impairment in retaining and recollecting new information.
Describe how structures related to declarative memory can be damage and effects:
Which area is sensitive to anoxia? How can this occur?
What is the entorhinal cortex affected by? Consequence?
Korsakoff Syndrome ?
Mech?
Consequences?
Damage to Structures of Declarative Memory
CA1 area = particularly sensitive to anoxia
trauma
cerebral edema
heart attacks
cardiac surgery
Entorhinal cortex:
first region to degenerate in Alzheimer’s disease
associated w/ ability to form long-term declarative memory.
Korsakoff Syndrome
due to prolonged thiamine deficiency seen in alcoholics → degen in
hippocampal formation,
mammilliary bodies
thalamus.
Consequence:
deficits in short & long-term declarative memory.
NOTE: consolidation process = particularly sensitive to processes which damage or interfere with the hippocampus.
Describe the different forms in which non-declarative memory can be encoded
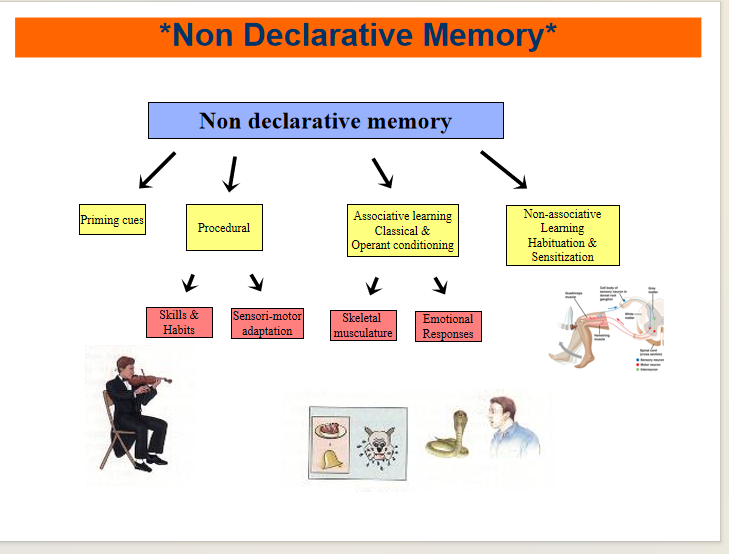
List the Non-declarative Memory Neural Substrates
Implicit memories = stored differently depending upon how they are acquired.
circuits involve:
basal ganglia,
prefrontal cortex,
amygdala,
sensory association cortex,
cerebellum and reflex pathways
but not those of the temporal lobe or midline thalamic nuclei.
Describe the two forms of associative learning:
Pavlov:
What is it?
EX?
Operant Conditioning:
What is it? Involves?
Examples?
Classical (Pavlov) conditioning
learning relationship between two stimuli,
one of them= neutral (light or ring).
Also involve pathways producing the motor behavior.
EX: Fear conditioning:
training that uses fearful stimuli (electric shock) & light, involves the amygdala
EX: Eye blink conditioning to a tone & puff of air involves the cerebellum.
Operant conditioning
learning relationship between behavior and consequences of that behavior
reward/punishment (called trial and error).
involves nucleus accumbens.
EX:
food aversion conditioning
does not require awareness, just nausea
associative learning with reward
can lead to addictive or compulsive behaviors by attaching a positive affect to them.
Describe Non associative learning
What is it?
two Forms
Involves?
Examples?
Non associative learning
results when a person is exposed to one stimulus.
Two Forms:
habituation:
becoming less sensitive to harmless stimulus w/ repeated application
sensitization:
greater responsiveness to a harmful stimulus
Involves:
sensory and motor pathways involved in producing motor responses.
Examples:
spinal flexion reflex in leg withdraw,
startle reflex
Describe the amygdala’s role in learning/memory
Amygdala:
Function:
Associates exteroceptive sensory inputs (from sub/cortex) w/ emotional outputs (via HPA and Autonomic Systems)
has capacity for emotional arousal to modulate memory processing
via outputs to other major memory systems (procedural and declarative memory)
EX: (PTSD)
Describe Procedural memory
Two pathways:
Pathway?
Which type of movement is learned?
Two Pathways:
dorsal striatum Pathways:
associates sensory and motor cortical information → mediates habit and skills.
required in learning skilled movement sequences (procedural learning).
Cortical and subcortical sensory pathways
Through Cerebellum
mediates sensori-motor adaptations
EX: vestibulo-ocular adaptation (clear vision when moving head).
NOTE: The basal ganglia have some of the same characteristics as the declarative systems (loops, tonic activity, modulation with activity)
What is priming?
implicit memory effect in which exposure to a stimulus influences a response to a later stimulus
It may or may not be available to consciousness (often not).
Example: Exposing subjects to a list of words or objects (without a request to remember them) and then some time later, testing to see if memory of the list has been retained by presenting part of the words and asking to complete.
Describe what happens to non-declarative memory if these structures are affected:
Basal ganglia
amygdala
cerebellar
Basal Ganglia:
Huntington’s Disease, Parkinson’s
Consequences:
inability to learn motor skills (as opposed to performance)
Amygdala:
damage = fail to develop fear conditioning
Cerebellar:
interfere with some types of conditioned reflex learning (eye-blink reflex to a tone and puff of air)
Differentiate between the temporal categories of memory
What is consolidation?
Temporal Categories of Memory:
Immediate memory:
fractions of a second.
each sensory modality (visual, tactile, verbal) = own register.
Required to be oriented and responsive in environment.
Working memory (aka-short term memory)
seconds to minutes after
Clinical test is to remember a span of digits presented. (7-9 is normal)
Long term memory
days, weeks or months.
Consolidation:
process of Working memory (short term) → long term memory
Not clear if the process occurs in sequence or in parallel with short term memory.
Describe Working Memory substrates
Locations?
Specificity?
Describe long term memory substrates
Declarative vs episodic vs non-declarative:
location
Damage?
Working memory substrates:
Declarative: hippocampus
More complex tasks: Neocortical/prefrontal
EX: problem solving and behavioral planning.
Specificity:
Areas activated = related to task (to some extent)
EX: one area = focused on facial identity; other areas for spatial memory
Long term memory substrates:
broadly distributed
THUS: Only diffuse damage or overactivation (epilepsy or using electroconvulsive therapy) will produce appreciable deficits in long term memory.
Declarative memory:
Location: distributed fashion in the neocortex
Damage to specific cortical area = loss of specific information and fragmentation of knowledge (agnosia)
EX: In associative visual agnosia, patient cannot name objects but can identify object by selecting the drawing.
Episodic
Location: prefrontal cortex.
Frontal lobe damage → Source Amnesia (forget how information was acquired)
Non declarative memory:
Location: Subcortical structures:
basal ganglia, spinal cord pathways, amygdala and cerebellum
NOTE: cortical storage is not required
What is association?
The association of random objects, words, or numbers with objects significant to the individual can dramatically increase particularly declarative memory, but also non-declarative aspects.
Describe amnesia:
Forms?
Forms:
Anterograde: inability to form new memories
retrograde: difficult in retrieving memories already established
NOTE: These forms may occur together, but also apart and can give a clinical picture of the severity of brain trauma after brain injury. (e.g., the extent of amnesia after head trauma, memory of the accident, before and after can indicate the severity of injury).
Describe what is happening in memory consolidation on the celluar level
Formation requires?
Give examples of changes
Learning in the Cellular level:
Formation of memories = circuitry changes
either in pre/postsynaptic or both
Changes can include:
receptor, channel or enzyme sensitivity
# of NT release or # of NT vesicles available for release
formation of new synapses
increase in # of spines/dendrites
Rewiring
NOTE: Permanent changes in neuronal circuitry are believed to be necessary for memories that persist for weeks, months or years (i.e. declarative memory & procedural memory).
Describe long time potentiation
History
What is it?
Mech:
Describe what happens in early phase
Late Phase
Mech?
LTP:
History:
Described initially in hippocampal formation,
now known to occur in cerebellum, neocortex, amygdala, olfactory bulb, striatum and peripheral system.
best studied synapse is that from Schaffer collateral fibers of CA3 → CA1
What is it?
Tetanus of neural pathway → affected synapse will produce potentiation → same pre-tetanus stimulus will result in a larger response
Mech:
Glu (from pre) → AMPARs (on post) → Na+ entry depolarizes → Depolarization releases Mg2+ from NMDA (glu can now bind) → NMDA activation → Ca++ influx (into dendrites of post)
Early Phase of Potentiation:
increased [Ca++] → Cascade:
Increases AMPARs insertion in post → enhanced efficacy of post response.
Increases AMPARs phosphorylation →
increases open probability or current (increased sensitivity)
maintains early LTP.
via PKC and Ca+2 /calmodulin kinase II
Activates NO synthetase:
NO produces permanent changes in pre → enhance glu release w/ each AP
Late phase of Potentiation:
Requires de novo synthesis of protein (unlike early phase)
Mech:
Calcium/calmodulin complexes → activates AC → cAMP → PKA → phosporylates MAPK → act. CREB-1 → binds to promotor element → regulates transcription
List the Other effects of potentiation
Other Effects:
activation of normally silent synapses
one possible mechanism for the relatively rapid establishment of new circuitry in the process of memory.
Growth of new sites of synaptic transmission between Pre/Post
MECH: increase in dendrites spines on post
allow formation of more synapses and reinforce that circuitry.
Describe long term depression
Produced by?
Mech?
Location?
LTD:
Produced by:
low frequency stimulation (1Hz) for long periods (10-15 minutes).
Result in depresses excitatory potentials for hours.
Mech:
Produces lower increase in Ca++ stores → enhances meta. pathways → decreases AMPARs (by internalization) + decreased AMPARs sensitivity (by depolarization)
Location:
shown to occur in cerebellum
may participate in learned movements
NOTE: Long term depression can occur at the same synapses that potentiation occurs.