401 EXAM 2
1/95
Earn XP
Description and Tags
viruses
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
96 Terms
HSV, VZV, EBV, CMV; ENV+
Herpesviridae
they are not transient nor labile
many establish persistent infections
they often reside in the cell nucleus
genetic material resembles host’s material for transcription and replication and interacts with host machinery
DNA viruses
they are labile and transient
they are prone to mutation
most replicate in the cytoplasm
they must code for their own polymerase
RNA viruses
they are hardier and more resistant to the environment
ex: norovirus, poliovirus, rotavirus, rhinovirus
non-enveloped viruses
they are sensitive to the environment
they cannot survive the GI tract
ex: measles, mumps, rubella, HIV, rabies, coronavirus
enveloped viruses
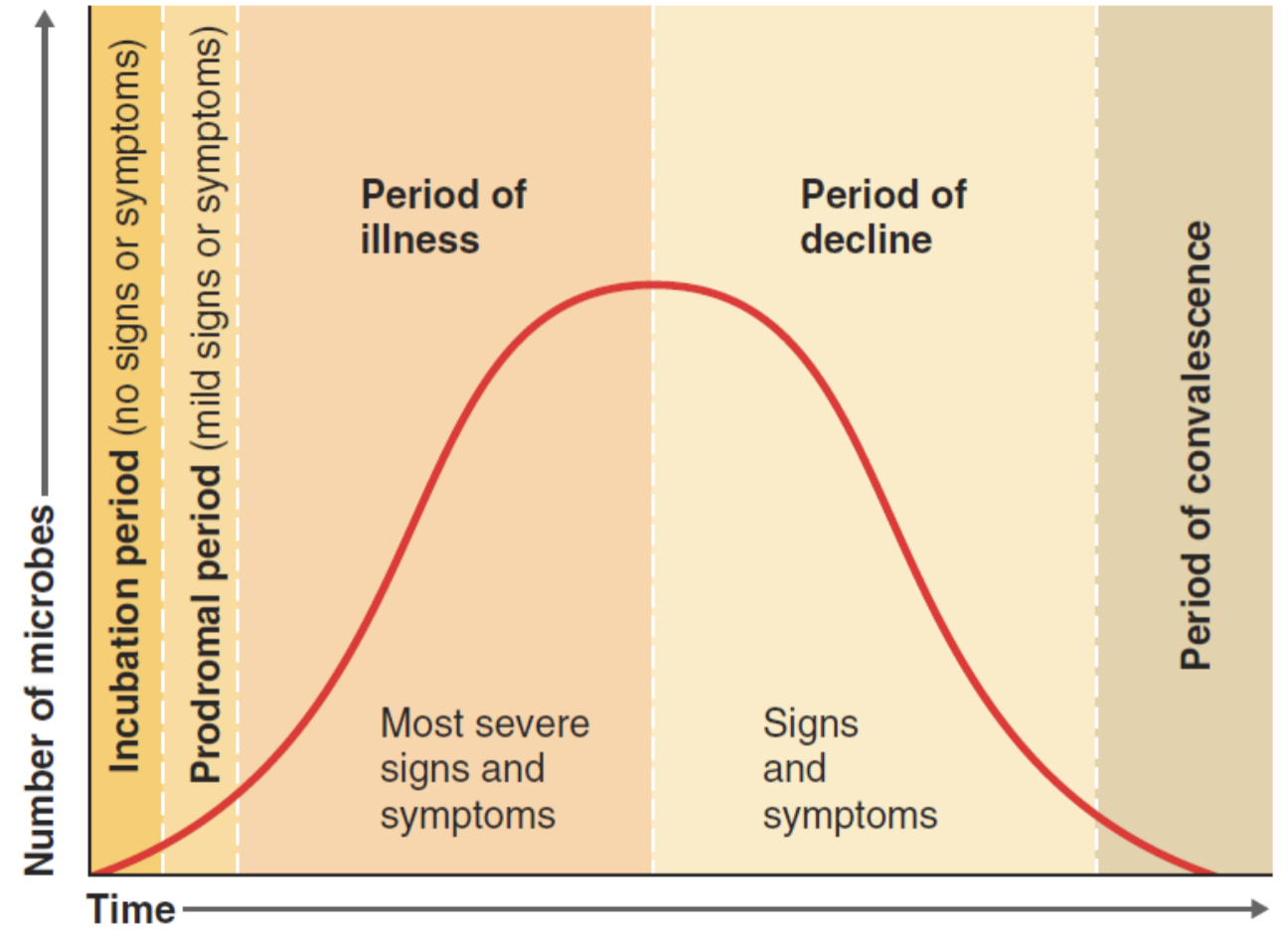
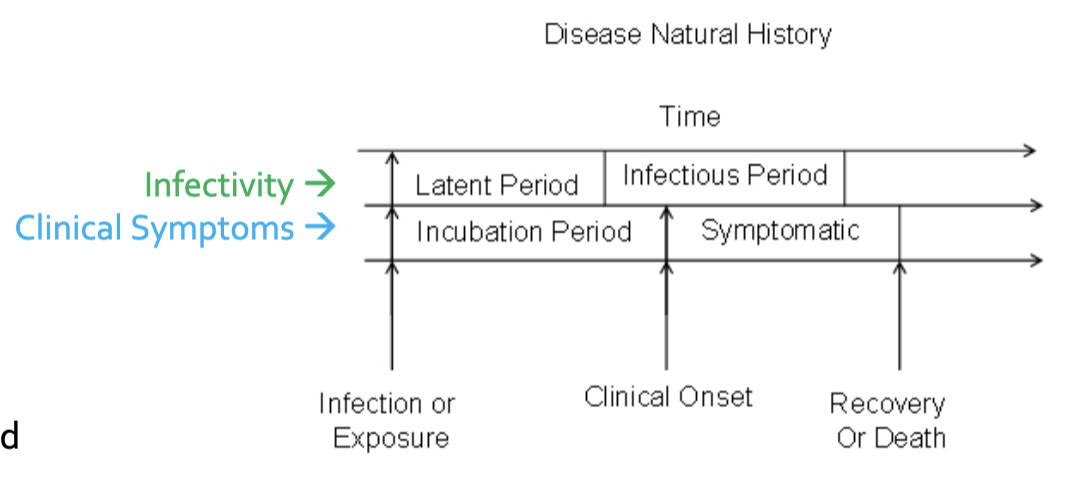
The stages of a disease (5) and which stage exhibits the most severe symptoms?
hint: i, p, i, d, c
enveloped RNA virus that infects CD4+ cells, T helper cells, and immune system
Human Immunodeficiency Virus
(can progress to AIDS)
this type of HIV is the predominant one worldwide
HIV-1
HIV-2 is primarily in west africa, europe, and india
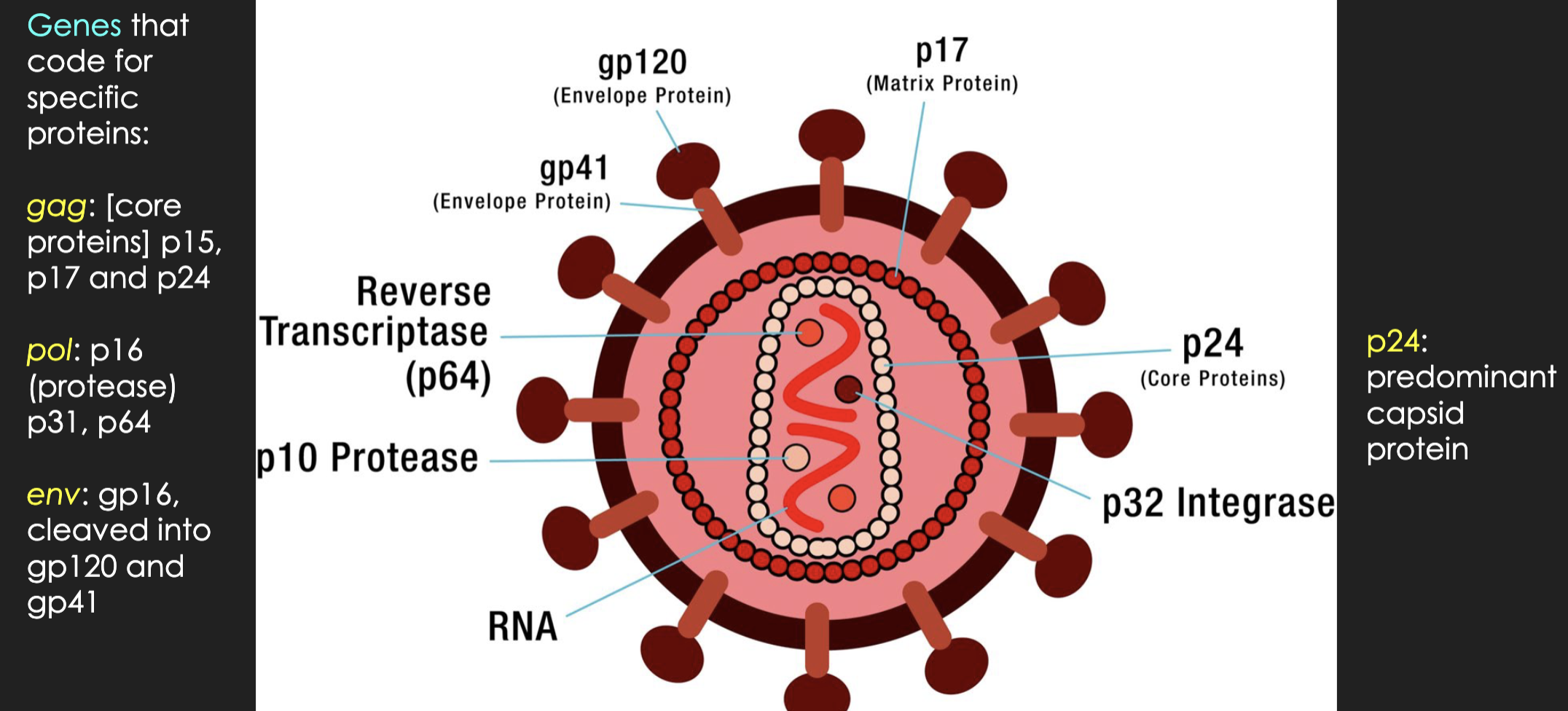
the proteins on an HIV cell that are tested to detect HIV
envelope proteins: gp41, gp120
inside: p17, p24 (predominant capsid protein)
when a person with HIV gets another type, or strain, of the virus. if the new strain is resistant to medicine/therapy that the person is already taking, it may cause quicker illness
superinfection
patient doesn’t adhere to the medication directions
(who the hell has time for nausea??)
inadequate adherence
describe: latent/asymptomatic HIV infection
immune cells are infected with HIV virus but not actively producing new HIV infected cells
T/F: you can test for HIV right away
Fasle: anti-p24 antibodies appear 1-2months; correlated with the decline in p24
if tested too soon, could result in false negative
What is the criteria of AIDS?
AIDS-defining condition
or
CD4 count less than 200 cells/mm3
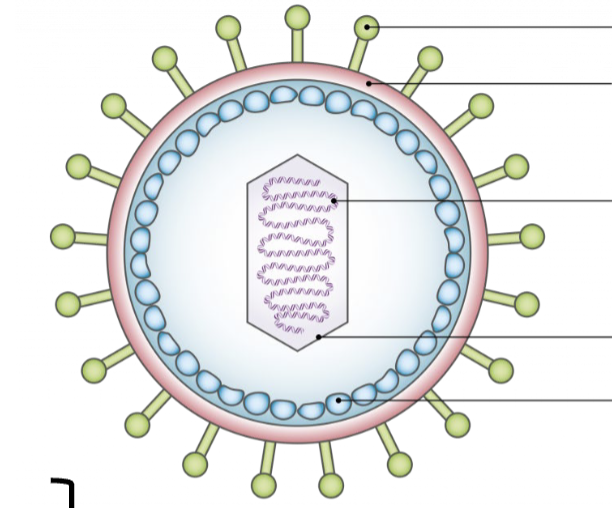
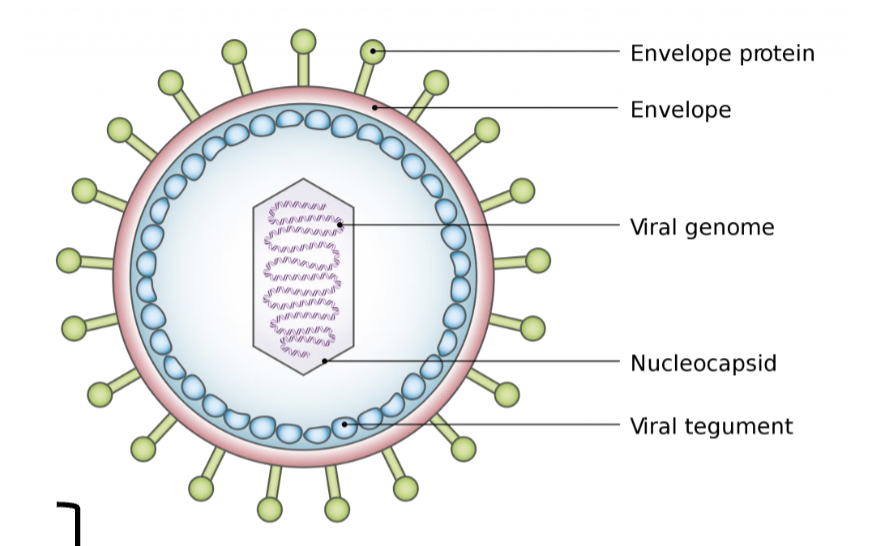
label HSV structure from top to bottom
T/F: incubation period can be longer than the latent period, meaning you can start being infectious while asymptomatic
true!
HIV enters a host cell and has to undergo _______ before integration and replication.
reverse transcription to synthesize cDNA
________ testing uses viral components p24, p31, gp41, gp120/160 to detect HIV
Confirmatory Testing
medication that prevents HIV infection for HIV-negative high risk individuals
PrEP: pre exposure prophylaxis
hepatitis virus(es) with fecal-oral transmission
HAV, HEV
hepatitis virus(es) with DNA genetic material
hint: bloodborne pathogen
HBV
hepatitis virus(es) with 60 – 85% chronicity
hint: bloodborne pathogen
HCV
hepatitis virus(es) that exist(s) as a co-infection
hint: bloodborne pathogen
HDV requires HBV to replicate
another word for icterus is ________
jaundice
acute vs. chronic hepatitis
acute: symptoms present for less than 6 months
chronic: HBsAg present for more than 6 months
replacement of liver tissue with scar tissue (fibrosis)
liver cirrhosis
severe impairment of hepatic functions or severe necrosis of hepatocytes in the absence of pre-existing liver disease
fulminant hepatitis
this marker is used to make the HBV vaccine
HBsAg (surface antigen)
beyond the surface, ______ antigen is found within the Hepatitis B virus structure
core antigen
HBsAg: (-)
Anti-HBs: (-)
Anti-HBc: (-)
what does this mean?
patient is susceptible to HBV
HBsAg: (-)
Anti-HBs: (+)
Anti-HBc: (-)
what does this mean?
patient is vaccinated successfully
HBsAg: (-)
Anti-HBs: (+)
Anti-HBc: (+)
what does this mean?
patient had a past infection but cleared it successfully
HBsAg: (+)
Anti-HBs: (-)
Anti-HBc: (+, IgM)
what does this mean?
patient has an acute HBV infection
HBsAg: (+)
Anti-HBs: (-)
Anti-HBc: (+, IgG)
what does this mean?
patient has a chronic HBV infection
Why can’t HDV survive without HBV?
HDV shares the envelope glycoproteins of HBV. HDV uses HBsAg to enter the cell, so HDV can’t enter host cells alone
rotavirus
norovirus
enterovirus/poliovirus, HAV
are all examples of???
non-enveloped RNA viruses
non-enveloped RNA virus
causes acute infectious gastroenteritis
difficult to disinfect (HIGHLY INFECTIOUS)
known for spreading on cruise ships
norovirus (norwalk virus)
non-enveloped RNA virus
highly infectious
common symptoms include severe watery diarrhea, vomiting, fever, dehydration, crying with few or no tears, decreased urination
population at risk: little babies
rotavirus
“wheel” in latin
nonstructural protein NSP4 that induces secretory diarrhea without any structural organ damage (rotavirus)
enterotoxin
non-enveloped RNA enterovirus
can infect CD155+ cells (intestinal epithelial cells)
fecal-oral transmission
known for causing paralysis
poliovirus


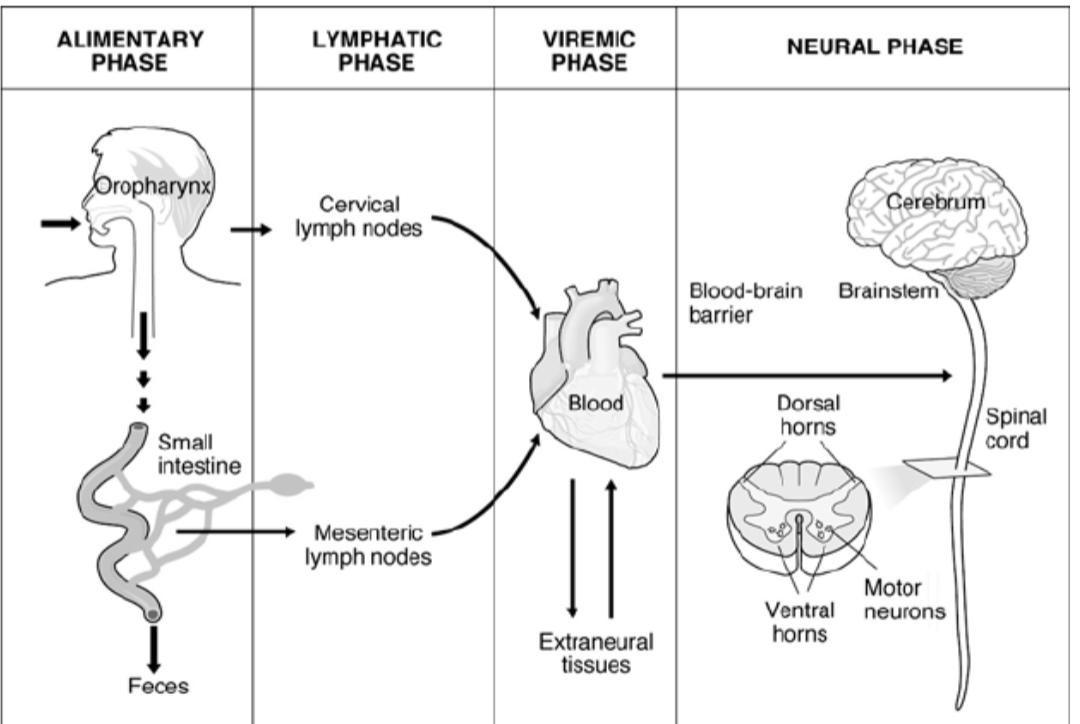
why is poliovirus so deadly?
polio replicates in the oropharyngeal and intestinal mucosa, eventually spreading to the tonsils and lymphatic tissue in the small intestine
once the virus enters the bloodstream in the viremic phase, it can spread to the spinal cord and cross the blood-brain barrier, destroying nerves and causing paralysis
only this type of influenza can cause pandemics
Influenza type A
how is influenza A virus subtyped?
HA: hemagglutinin
NA: neuraminidase
(ex: H1N1)
enveloped virus
population at risk: babies and elderly
most common cause of bronchiolitis and pneumonia in infants and children
acute respiratory tract illness
these tests in the lab are STAT
respiratory syncytial virus (RSV)
enveloped virus
causes barking cough (croup)
upper and lower respiratory illness
human parainfluenza virus (HPIV)
enterovirus that causes the common cold
no vaccine
rhinovirus
enveloped RNA virus
aka “rubeola”
airborne transmission
Koplik spots inside mouth
rash breaks out on face first, then spreads down
measles
enveloped RNA virus
swollen salivary glands
more common during childhood
Mumps
enveloped RNA virus
may cause a rash that begins on face and spreads
causes severe birth defects when exposed to a developing baby in utero, esp in first trimester
hint: vaccine preventable (MMR)
rubella (german measles)
non-enveloped DNA virus
symptoms depend on the serotype but it’s most associated with respiratory complications in young children
vaccine for this virus is for military personnel only
many serotypes (>60)
adenovirus
coxsackievirus, acute flaccid paralysis (enterovirus D68) and viral conjunctivitis are examples of _________ enteroviruses
non-polio enteroviruses
Herpesviridae viruses can cause _______ and ________ infections, meaning they can reactivate, never going away
latent: asymptomatically persist in host
lytic: destroys cell upon release of new virions
this type of Herpes virus hides in nuclei of trigeminal ganglia and reactivates as oral infections
hint: usually oral/cold sores
HSV-1
this type of herpes hides in the sacral ganglia
hint: STD/gential
HSV-2
most common etiology for sporadic non-seasonal encephalitis across the world
high morbidity and mortality
herpes simplex encephalitis (HSE)
reactivated HSV-1 infection, usually pediatric
ocular herpes simplex
this virus causes chicken pox (primary) and shingles (reactivated)
latency in the dorsal root ganglia
viral cell cultures show rounded cells, sandpaper-like appearance
varicella zoster virus
an area of skin in which sensory nerves derive from a single spinal nerve root
shingles
dermatome
(if 2 dermatome, then the shingles is not localized)
latency in B lymphocytes, epithelial cells, and natural killer/T cells (higher likelihood of cancer in these cells)
body fluid transmission
associated with infectious mononucleosis (IM)
epstein barr virus (EBV)
“kissing bug”, “mono”
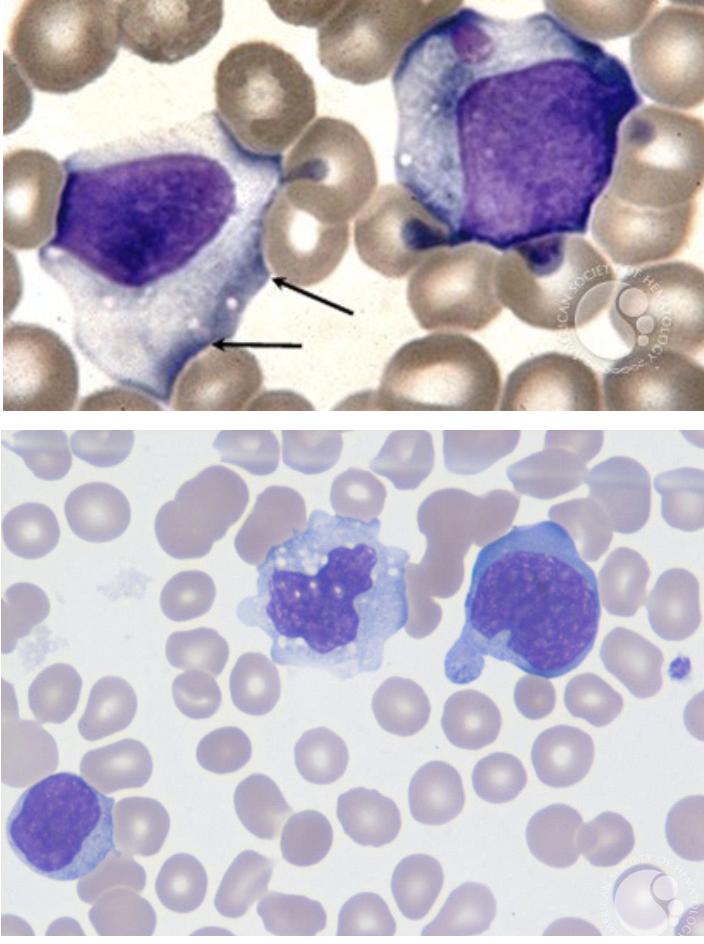
kissing disease caused by EBV
symptoms include enlarged spleen
lymphocytes have scalloped margins, indentations by surrounding RBCs, vacuolated cytoplasm
“ballerina skirt”
infectious mononucleosis
this virus has latency in macrophages
especially dangerous in transplant patients (not a reactivation, it’s primary!)
most common infectious cause of birth defects in US
more common w/ women’s 2nd pregnancies; older child’s illness infects mom and fetus
cytomegalovirus (CMV)
hint: turkel’s mystery rash
TO(SPVL)RCH infections that are associated with miscarriage and/or congenital abnormalities
Toxoplasmosis
Other agents: syphilis, parvovirus, VZV, listeria
Rubella
CMV
Herpes
transmission: mosquito to human
common in puerto rico
2nd infection of different serotype hurts worse; host antibodies welcome new strain (open door)
causes endothelial cell dysfunction and coagulation disorder
Dengue
generally milder disease than dengue
biggest issue is infection during pregnancy (causes microcephaly, brain defects)
transmission: mosquito to human
zika virus
present in the US, even in CA
transmission: mosquito
primary reservoir: birds (crows are very sensitive to this)
able to infect neurons and cause encephalitis, flaccid paralysis, meningitis
west nile virus
transmission: mosquito
reservoir: non-human primates
virus replicates in the liver, leading to hepatocyte apoptosis and lytic necrosis
severe illness presents with high fever, yellow skin, bleeding, shock, organ failure
yellow fever
UCLA and Cedars are treatment facilities for this virus
reservoir: bats
zoonotic disease
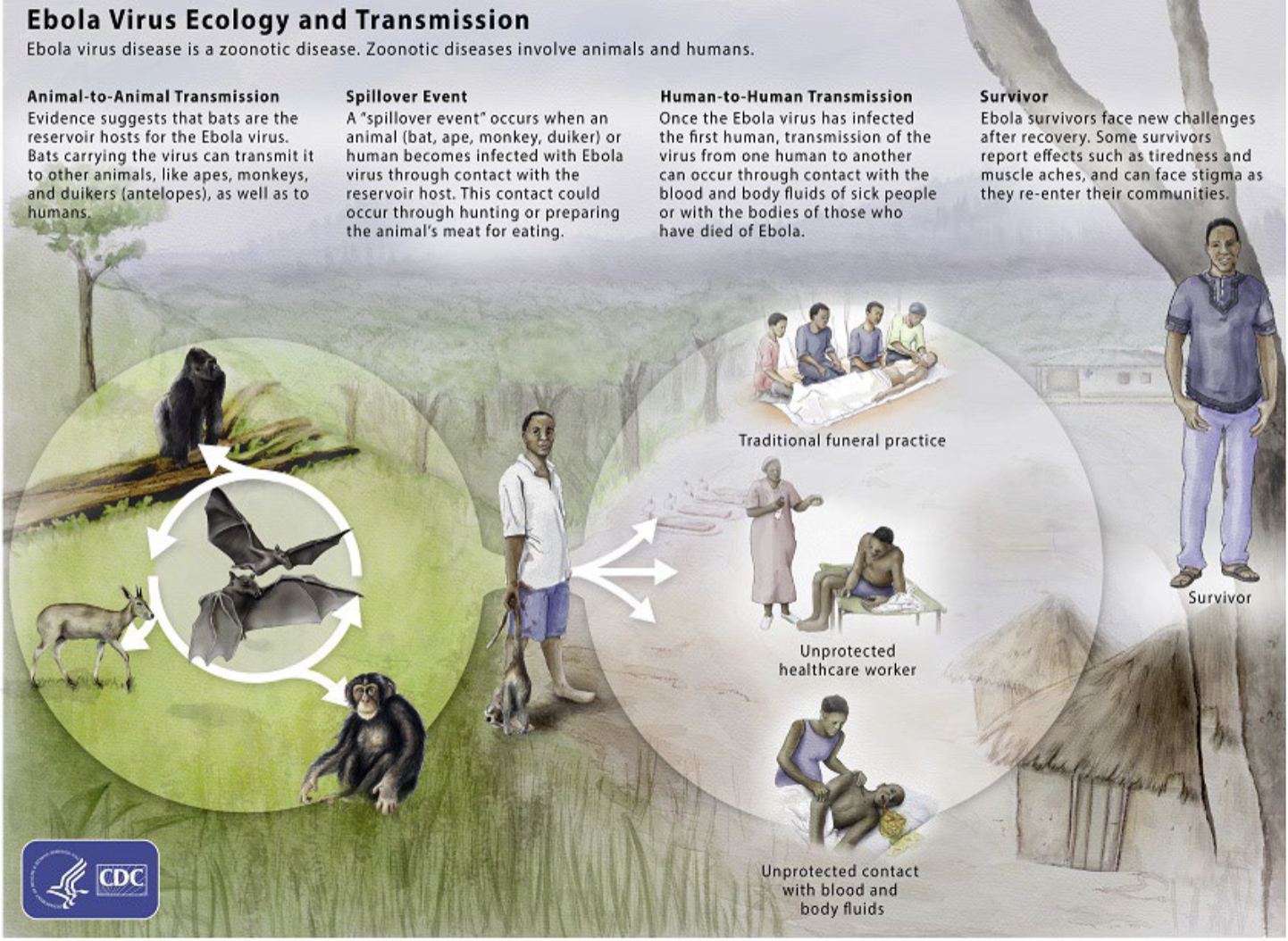
vascular leakage, hypotension, disseminated intravascular coagulation, and endothelial cell death lead to hemorrhagic fever
ebola virus
explain the ebola virus ecology and transmission
hint: animal to animal, spillover event, human to human, survivor
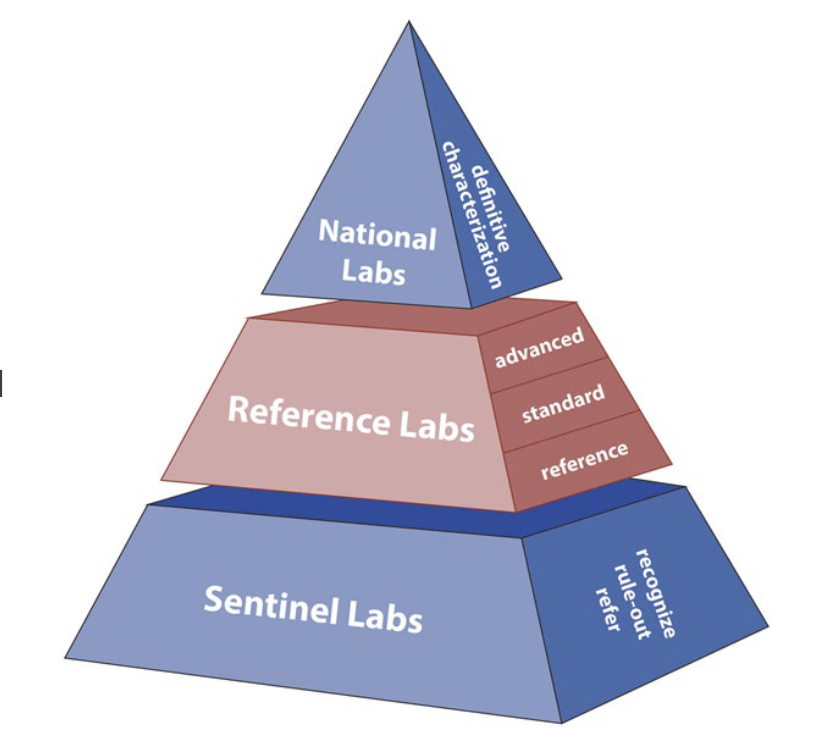
what are the 3 laboratories in the lab response network for diseases like ebola?
national labs
reference labs
sentinel labs
reservoir: bats
rare virus
results in hemorrhagic fever
marburg virus
reservoir: rat
results in hemorrhagic fever
most common complication: deafness
lassa fever
transmission: from deer mouse & white-footed deer mouse (white fur on bellies, large eyes)
new world virus type: Sin Nombre virus (pulmonary failure)
old world virus type: fever with renal failure
hantavirus
virus is attracted to sebaceous glands
terrorized the world for thousands of years; first disease to be eradicated
virus enters blood during primary viremia, then pustules and scabs form upon secondary viremia
pocks progress at the same stage
variolator first used to inoculate an uninfected person with dried scabs for vaccination
smallpox (variola virus)
this virus attacks the central nervous system and causes fatal encephalitis
transmission: infected animal bite
vaccination of post-exposure prophylaxis upon infection must occur QUICKLY within zone of neutralization
rabies
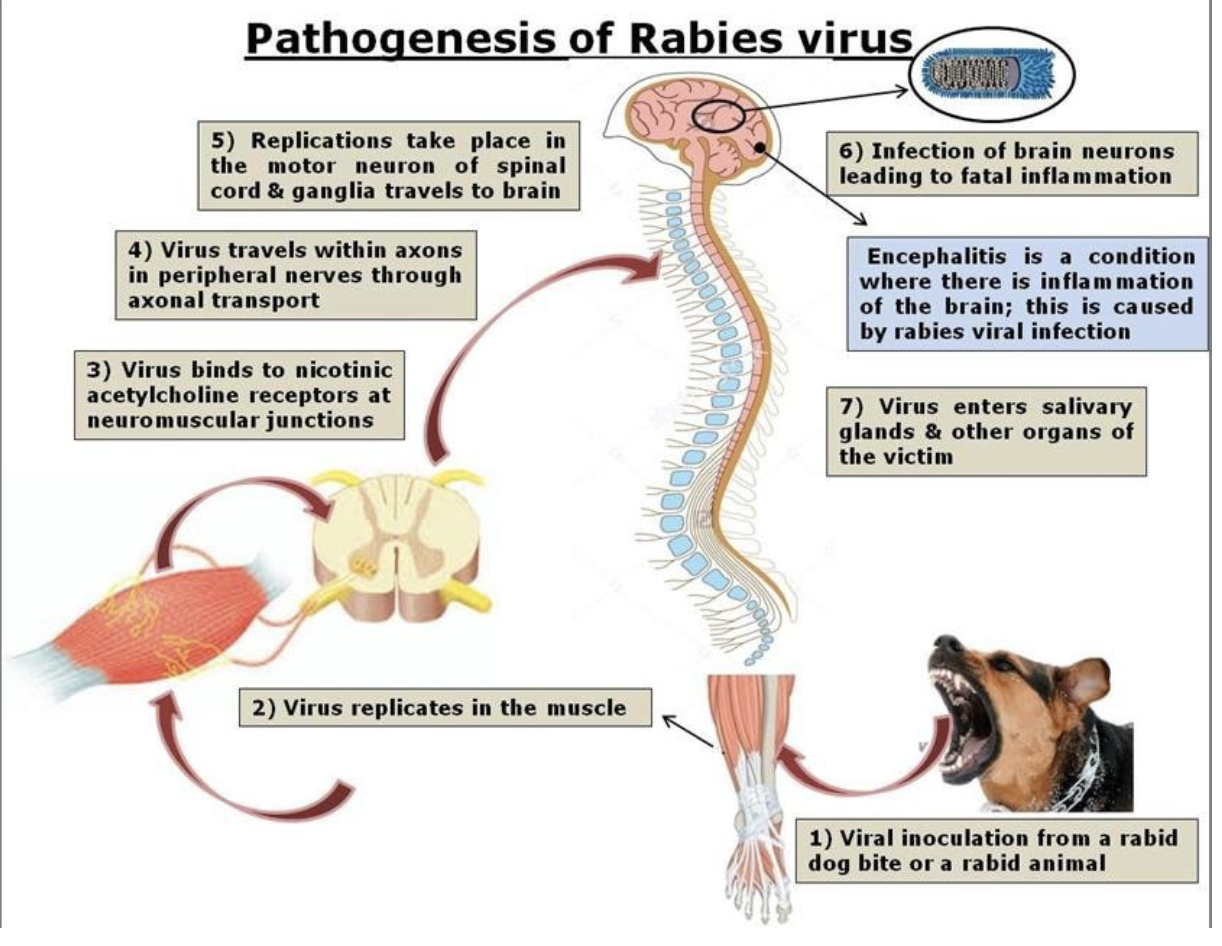
explain the pathogenesis of rabies
virus enters/replicates in muscle; travels through neuromuscular junctions into peripheral nerves; travels to brain via spinal cord and ganglia; brain infection leads to inflammation (encephalitis); virus enters salivary glands & other organs of host
zoonotic disease
associated with direct contact with infected camels
MERS-COV
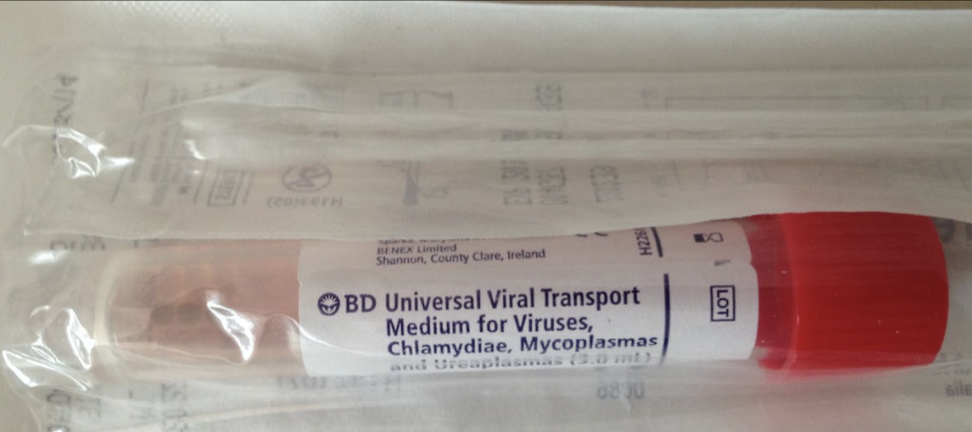
specimen collection and transport uses a swab and either viral transport media or universal transport media. the tube contains what 3 things?
balanced salt solution
human cells
antibiotics
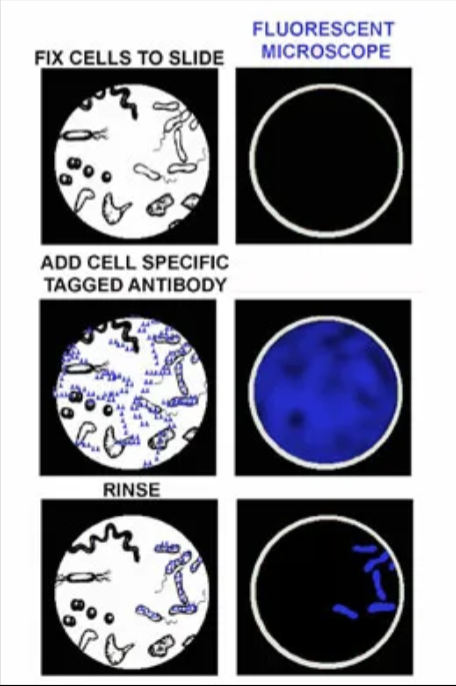
why might a fluorescent antibody stain be used?
can perform directly on specimen
organism is difficult to find/isolate/identify/culture
can identify multiple organisms at once in one specimen using different fluorescent markers
high sensitivity and localization
ex: search for parasites in stool sample
the main reagent in fluorescent antibody staining
fluorescently-labeled monoclonal antibodies
direct vs indirect antibody staining
direct: antibodies attach to target antigen in a single step
indirect: unlabeled antibodies attach to target antigen first, then fluorescently-labeled antibody attach to unlabeled antibody
reagents for enzyme immunoassays
monoclonal antibodies, enzyme, substrate
when are rapid enzyme immunoassays used? how do they work?
used for non-culturable viruses like RSV where we want a rapid diagnosis (babies can’t breathe in ER ☹)
substrate + enzyme interaction create color change when enzyme is attached to antibody that matches a target antigen
as prevalence decreases, the more likely you will have ______ _______.
false positives. sensitivity varies and specificity improves as prevalence of infection in community increases
the control line on enzyme immunoassays is looking for what?
reagent from the test (not sample); so if control line is dysfunctional, test is invalid

we are looking for a specific target antibody in these samples in the well plate. an antigen is added to the wells first, then all the patient samples with unknown antibodies. Then a secondary antibody linked to an enzyme is added. then a substrate (chromogen) is added. if target antibodies are present and match with antigen, then the enzyme and substrate will produce a color change to quantitatively or qualitatively detect the target. what is this method called?
enzyme linked immunosorbent assay (ELISA)
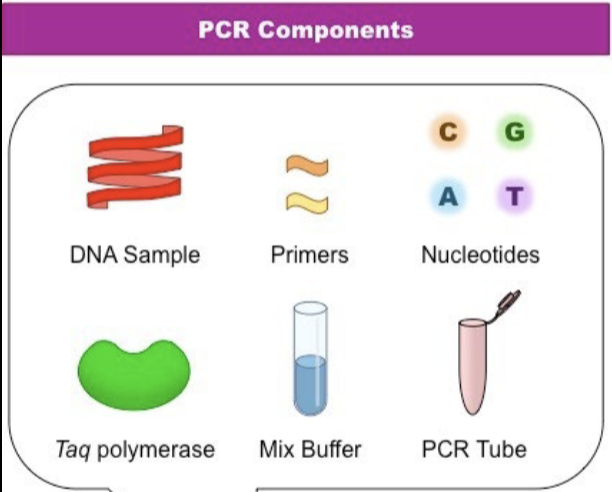
T/F: molecular amplification (PCR) is a test of diagnosis, not cure
true. does not differentiate between live/dead organism
how do we amplify genetic material from an RNA virus?
reverse-transcriptase PCR. there is an added step of reverse transcription of RNA to cDNA to allow for amplification
method where the amplified product is measured as the reaction progresses. fluorescence is measured after each cycle
qPCR, called “real time” PCR
describe the TaqMan probe
probe consists of a reporter and a quencher. as long as the quencher is close enough to the reporter, reporter cannot fluoresce. When DNA polymerase begins to build during extension phase, it cleaves the probe, freeing the reporter from the quencher! = measurable fluorescence. if PCR or binding of probe to DNA is unsuccessful, no fluorescence.
When do qPCR measurements occur?
baseline
exponential
linear
plateau
during the exponential signal phase
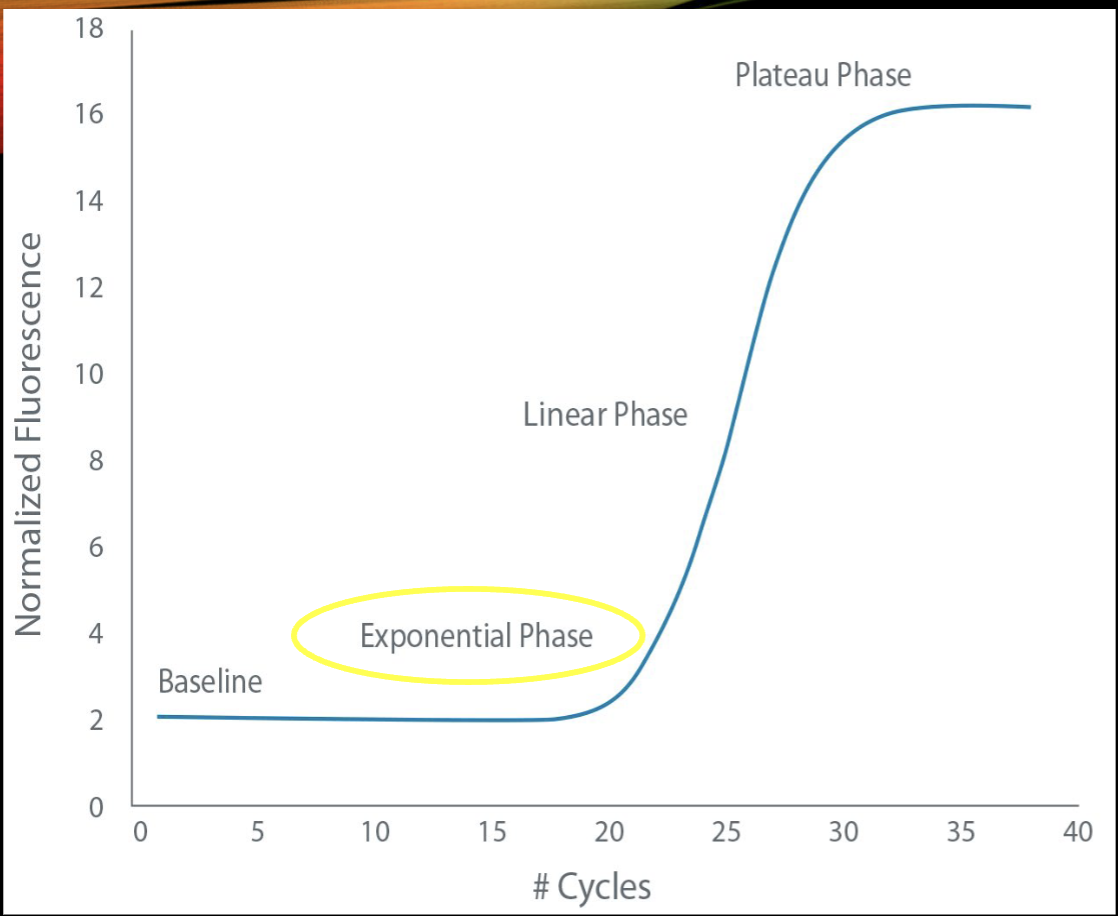
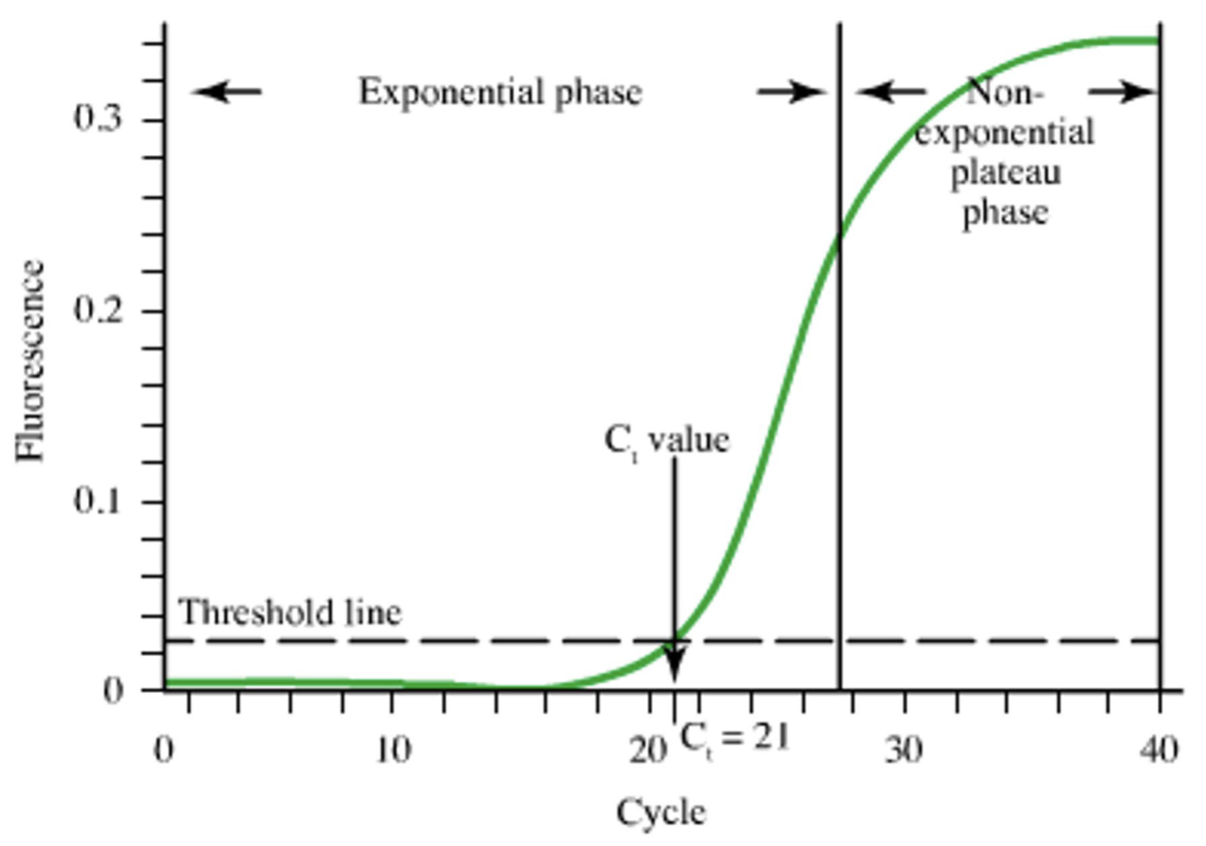
what is the threshold line?
what do lower and higher CT values mean?
threshold line is the level of detection or the point at which a reaction reaches fluorescent intensity above background noise
higher: lower concentration/negative result or gross error
lower: higher concentration of virus
how would you know what a specific CT correlates to, in terms of viral concentration in the specimen AND what the threshold should be?
standard calibration curve
in real-time PCR, r = -1
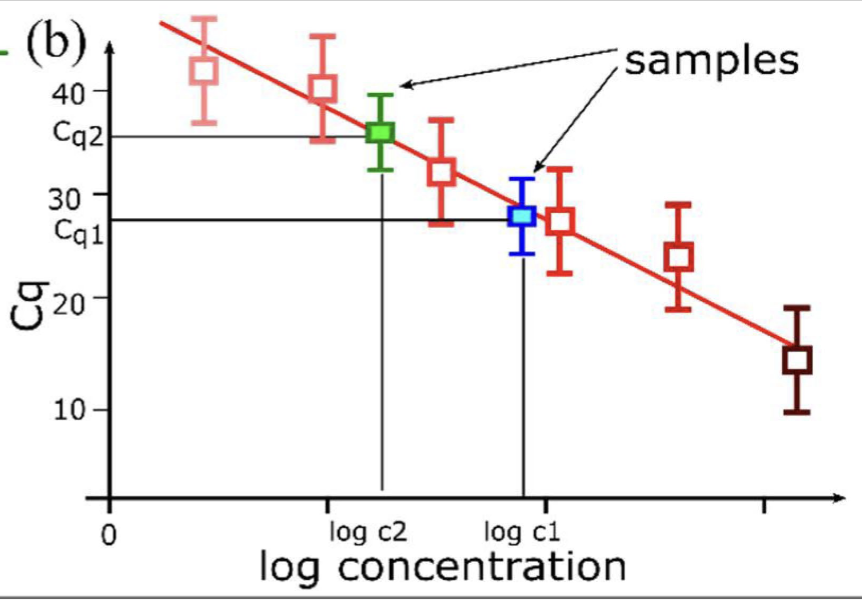
how do you create a standard calibration curve for qPCR?
use a series of known concentrations of viral specimens (standards) to determine the CT of each known standard. then plot CT (y) vs concentration (x)
T/F: if a sample falls outside of the standard curve, quantitation is not reliable
true
VERY expensive real-time multiplexed PCR test designed to simultaneously identify nucleic acids from different viruses, bacteria, and parasites for GI, respiratory, etc
syndromic panels

the gold standard to isolate live viruses and show active infection
performed to show CPE: cytopathic effect (structural changes in host cells caused by viral invasion)
expensive
extensie training
takes a long time
viral culture