Week 4: Colorectal Disease
1/83
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
84 Terms
list the different kinds of diverticular disease
-diverticular hemorrhage
-diverticulitis (uncomplicated and complicated)
-Segmental colitis with diverticula (SCAD)
-symptomatic uncomplicated diverticular disease (SUDD)
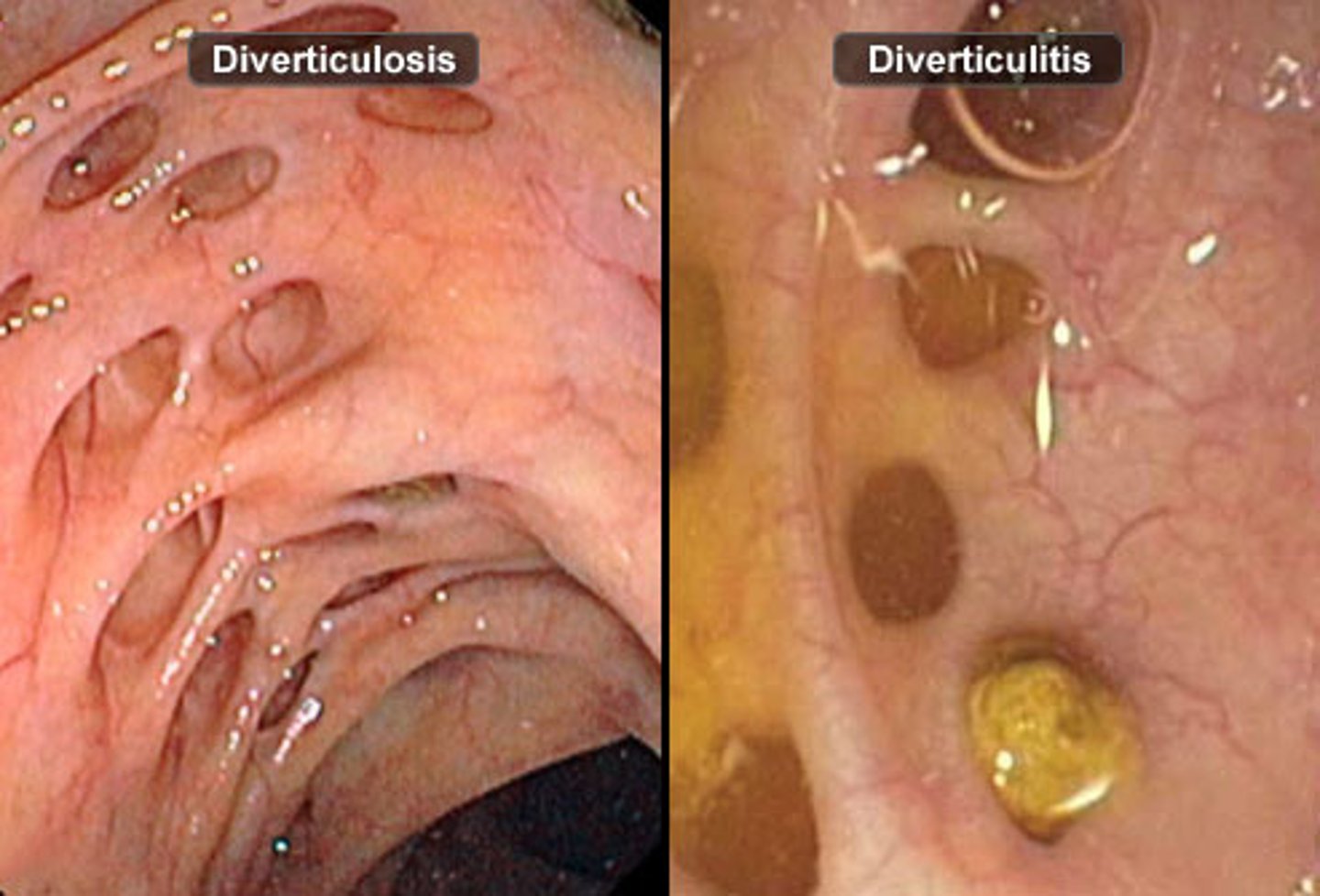
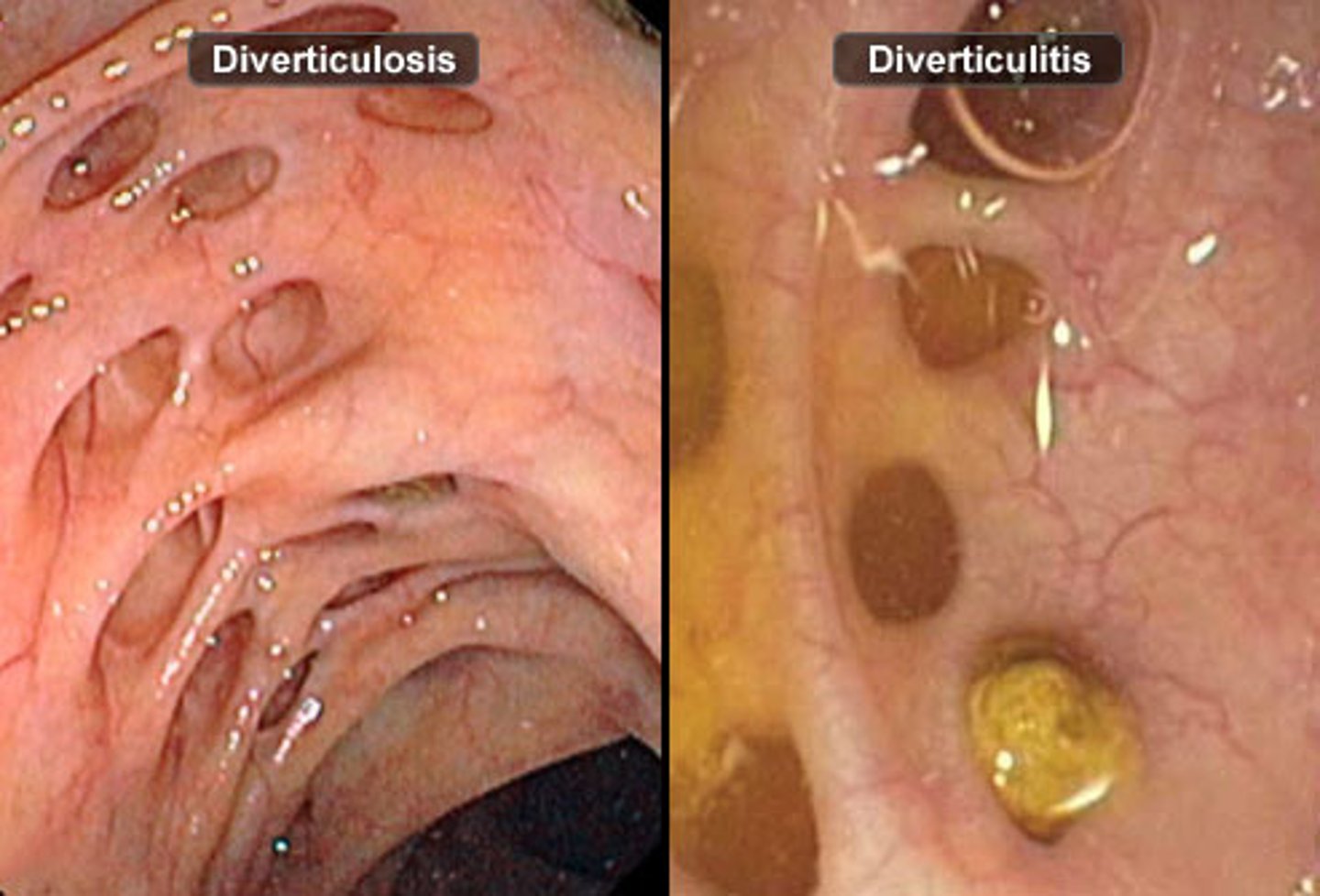
what happens in colonic diverticulosis?
-herniation of the mucosa and submucosa through the muscle layer of the colon
-herniations develop around taenia coli
progression of colonic diverticulosis
-vascular disease or structural weakness -> diverticular hemorrhage
OR
-microperforation/ischemia/ bacterial infection -> acute diverticulitis
theories of the pathogenesis of diverticulosis
-diet
-genetics
-motility
-CT alteration
-endogenous sex hormones (men> women before menopause, men=women after menopause)
right vs left sided diverticulosis
western countries see it more on the left, Eastern countries on the right
(left more common overall)
what is protective in diverticulitis?
having a high fiber diet
theories of the pathogenesis of diverticulitis
-motility
-CT alteration
-endogenous female hormones (women post-menopause > men)
-microbiome
-chronic inflammation
most common complications of diverticulosis/-itis
-phlegmon or abscess
-peritonitis
-obstruction
-fistula
(complicated diverticulitis has increased perforation/abscess, so higher mortality than uncomplicated)
diverticulosis/-itis: recurrence
-most complications seen in 1st or 2nd episode
-treated complicated diverticulitis and uncomplicated have equal risk of reoccurrence
-less recurrence for complicated diverticulitis if colon is removed.
diverticulitis: clinical presentation
inflammation causes:
-LLQ abd pain
-fever
-leukocytosis
diverticulosis: clinical presentation
-asymptomatic
-can be discovered on routine colonoscopy or imaging
Diverticulitis: general work up and management
-high risk or 1st presentation: get CT with PO/IV contrast
-is it complicated or uncomplicated?
-uncomplicated: NPO, pain relief
-complicated: do they have peritonitis or abscess? are they hemodynamically stable? (drainage and surgery as needed)
diverticulitis: outpatient management
-no oral abx unless major comorbities, immunocompromised, or signs of systemic disturbance
-pain control
-liquid diet
-reassess in 2-3 days and weekly until sx resolve
-admit if: persistent abd pain, fever, cannot tolerate fluids
diverticulitis outpatient management: if you do need to give antibiotics, what should they be?
-cipro, levo, or Bactrim with metronidazole
-amox-clavulanate
diverticulitis: inpatient management
-IV abx, fluids, pain meds
-consult surgery
-specimens sent for gram stain and culture -> then alter abx
diverticulitis inpatient management: what abx are appropriate?
-piperacilin-tazobactam
-Cefepime
-Ceftazidime
-carbapenems
epidemiology of a diverticular bleed
-3-15% of pts
-1/3 of these pts will have a massive bleed
-right side more common
-most are self limited
-AA
-60+
what can cause a diverticular bleed?
-recurrent trauma
-thinner wall of right (proximal) colon
diverticular bleed: clinical presentation
painless hematochezia
Hgb initially normal
diverticular bleed: management
-fluid resuscitation
-colonoscopy with endoscopic therapy
-CT angiogram with arterial embolization
-nuclear tagged red cell scan
-surgical: segmental resection, subtotal colectomy
types of constipation
-primary colorectal dysfunction
-secondary constipation
-functional constipation (chronic idiopathic)
primary colorectal dysfunction: causes
-slow transit constipation
-dyssynergic defecation (anorectal muscles not working well)
-IBS-C
causes of secondary constipation
-meds (opioids)
-mechanical
-metabolic
-endocrine (hypothyroidism, DM)
-psych/neuro
-diet
-myopathy
Functional constipation diagnostic criteria
must have 2 or more:
-straining >25% of the time
-lumpy or hard stools >25% of the time
-sensation of incomplete evacuation or blockage >25% of the time
-uses manual maneuvers to aid >25% of the time
-<3 spontaneous bm a week
-loose stools rare
Bristol Stool form scale descriptions
-Type 1: separate hard lumps like nuts (severe constipation)
-Type 2: sausage shaped, lumpy
-Type 3: like sausage with cracks on surface (normal)
-Type 4: like a sausage or snake, smooth and soft (normal)
-Type 5: soft blobs with clear-cut edges (need fiber)
-Type 6: mushy with ragged edges
-Type 7: watery, no solid pieces (severe diarrhea)
Constipation PE: abdomen
-I: distention
-A: high pitched or absent bs
-P: abd mass, hepatomegaly, lymphadenopathy
Constipation PE: rectal exam
-I: skin for fistula, anal wink, hemorrhoids, rectal prolapse
-ask them to bear down
-Digital rectal exam: anal tone, masses, fissures, stool
-occult blood test
complications of constipation
-hemorrhoids -> bleeding
-anal fissure
-rectal prolapse
-fecal impaction
what can result from fecal impaction?
stercoral colitis-> colonic ulceration -> perforation -> peritonitis -> death
treatment of constipation: non-pharm
-increase: water, fiber, activity
-decrease: dairy, red meats, processed food
-discontinue meds that cause constipation
-squatty potty
-pelvic floor therapy
-don't ignore urges!
treatment of constipation: classes of pharm agents you can use
-bulk laxatives
-stimulants
-osmotics
-lubricants
-stool softeners
-5-HT4 receptor agonists
-enemas/suppositories
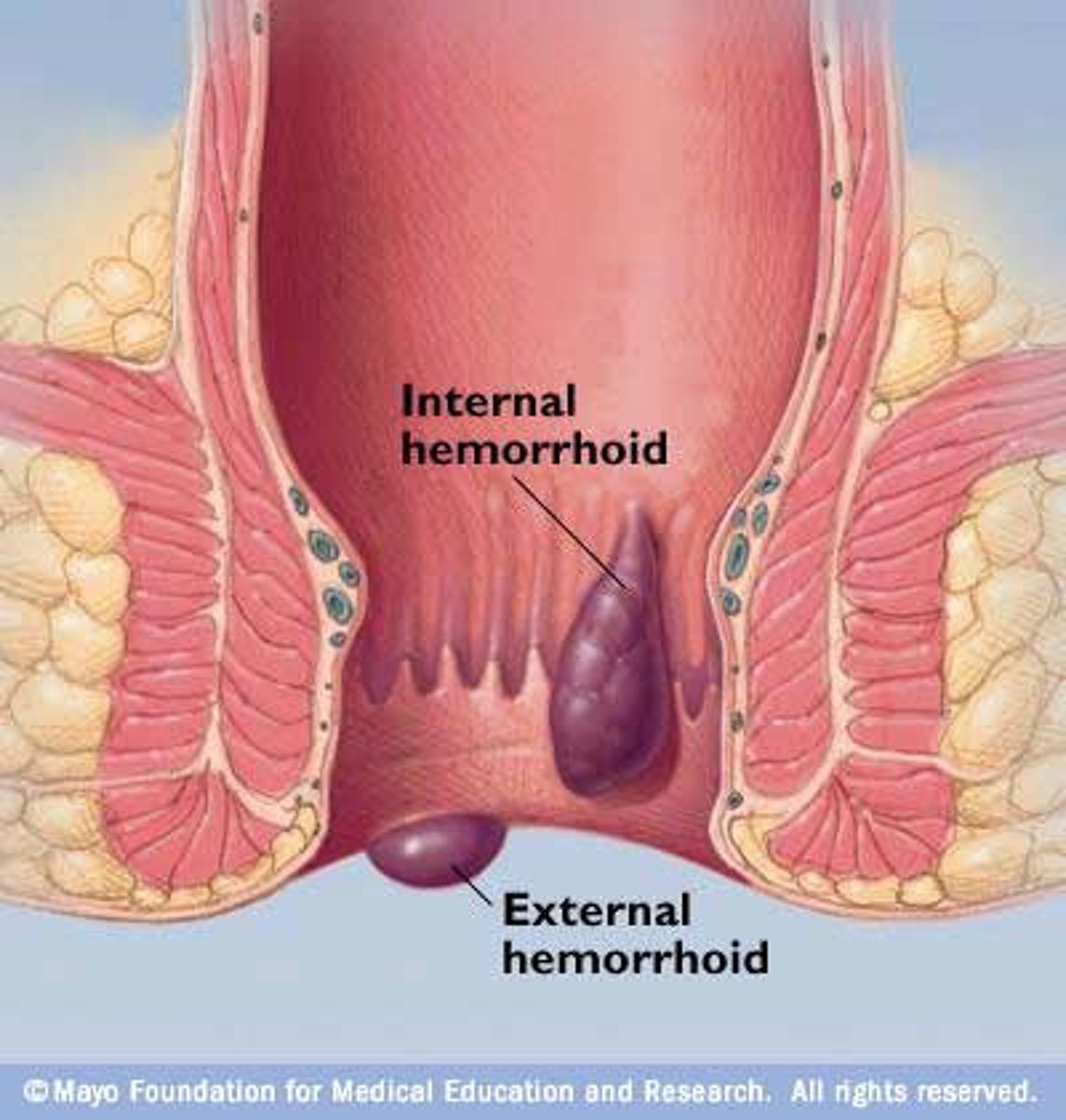
types of hemorrhoids
-internal (above dentate line)
-external (below dentate line)
-external thrombosed hemorrhoids
What are hemorrhoids?
-normal structures that come from the internal and external hemorrhoidal plexus
-internal hemorrhoids form anal cushions that help with continence
what can cause hemorrhoids?
-FH
-chronic diarrhea
-anal sex
-IBD
-extensive straining
-pregnancy
-heavy lifting
-sedentary lifestyle
pathogenesis of hemorrhoids (4)
-increased pressures = decreased venous return in plexus
-blood gets stagnant
-sliding process of anal cushions
-deterioration of anal cushion CT
epidemiology of hemorrhoids
-most common cause of rectal bleeding
-50% of people will have symptomatic hemorrhoids
-peaks around 45-65
presentation of internal hemorrhoids
-BRBPR
-fecal smearing
-mucous
-wetness
-perianal fullness
-pruritus
-usually no pain
presentation of external hemorrhoids
-skin tag
-perianal skin irritation and pain (w/ sitting)
-pruritus

presentation of external thrombosed hemorrhoid
-acute pain
-darker clotted blood
(see surgeon asap)
management of hemorrhoids: conservative therapy
-diet and lifestyle mods
-topical analgesics
-steroids
-antispasmodics
-sitz bath

management of hemorrhoids: nonconservative therapy
-flexible sigmoidoscopy/ colonoscopy with IRC
-rubber band ligation
-excision
-sclerotherapy
-hemorrhoidectomy
IBS: general
functional bowel disorder w/ abd pain or discomfort and altered bowel habits WITHOUT detectable structural abnormalities
diagnostic criteria for IBS
recurrent abd pain/discomfort at least 1 day/week in the last 3 months associated with:
-defecation
-a change in frequency or appearance of stool
what can cause IBS?
-post-infection
-GI motor abnormalities
-visceral hypersensitivity
-altered gut flora
-abnormal serotonin pathway
-immune activation
-CNS dysregulation
IBS: clinical presentation
-abd pain/discomfort with defecation
-altered bowel habits
-bloating
-gas
-typically younger pts, women > men
IBS: management
-low FODMAP diet (low carbs/sugars)
-many pharm options: stool bulking, antispasmodics, antidiarrheals, antidepressants, SSRIs, others
what is a drug used for IBS w/ diarrhea?
Rifaxamin (Xifaxan)
Colorectal abscess: definition
-abnormal, fluid filled
-categorized by where they occur (perianal or perirectal)
-more prevalent in immunocompromised pts
-infection starts in the anal crypt glands between the internal and external anal sphincters
Colorectal abscess: perianal vs perirectal
-perianal: more external, more common
-perirectal: more care required, 3 types (ischiorectal, intersphincteric, supralevator)
Colorectal abscess: pathophysiology
-anal ducts that drain the anal crypts get plugged
-leads to infection
-starts in the intersphincteric area and spreads
-associated with fistula in ano
Colorectal abscess: common causes
-pathogens: E. coli, bacteriodes, enterococcus, MRSA
-other: anal fissures, Crohn disease
Colorectal abscess: clinical presentation
-throbbing, continuous perianal pain or poorly localized within the pelvis
-pain with pressure, sitting
-erythema, edema, indurated skin
-perirectal: fever/chills
+/- dyschezia, blood in stool
dyschezia
painful or difficult bowel movement
Colorectal abscess: severe abscess presentation
fever, rigors, malaise, sepsis
Colorectal abscess: diagnosis
perianal: diagnosed by observing it
perirectal: CT (all types), US (intersphincteric)
Colorectal abscess: management
-incision & drainage (gold standard)
-consider wound culture and antibiotics
-complex abscesses: consult surgery
Colorectal abscess: who should get antibiotics?
-immunocompromised
-prosthetic heart valves
-artificial joints
-Diabetes
-IBD
what is the most common cause of rectal bleeding in infants?
Anal fissures
Anal fissures: anatomy
-ulcers <5 mm
-extend from below the dentate line to the anal verge
-usually posterior midline
-linear or rocket shaped
Anal fissures: causes
-anal sex
-trauma during defecation (straining, constipation, prolonged diarrhea)
-vaginal delivery
-cycle of poor healing of trauma + ischemia
Anal fissures: clinical presentation
-acute <8 weeks, chronic > 8 weeks
-sudden sharp pain w/ BRBPR (minimal compared to hemorrhoids)
-painful bowel movements
Anal fissures: acute presentation
anal pain at rest and exacerbated by defecation (lasting hours)
Anal fissures: chronic presentation
-hypertrophied anal papilla at proximal end of fissure
-a sentinel pile or skin tag at distal end
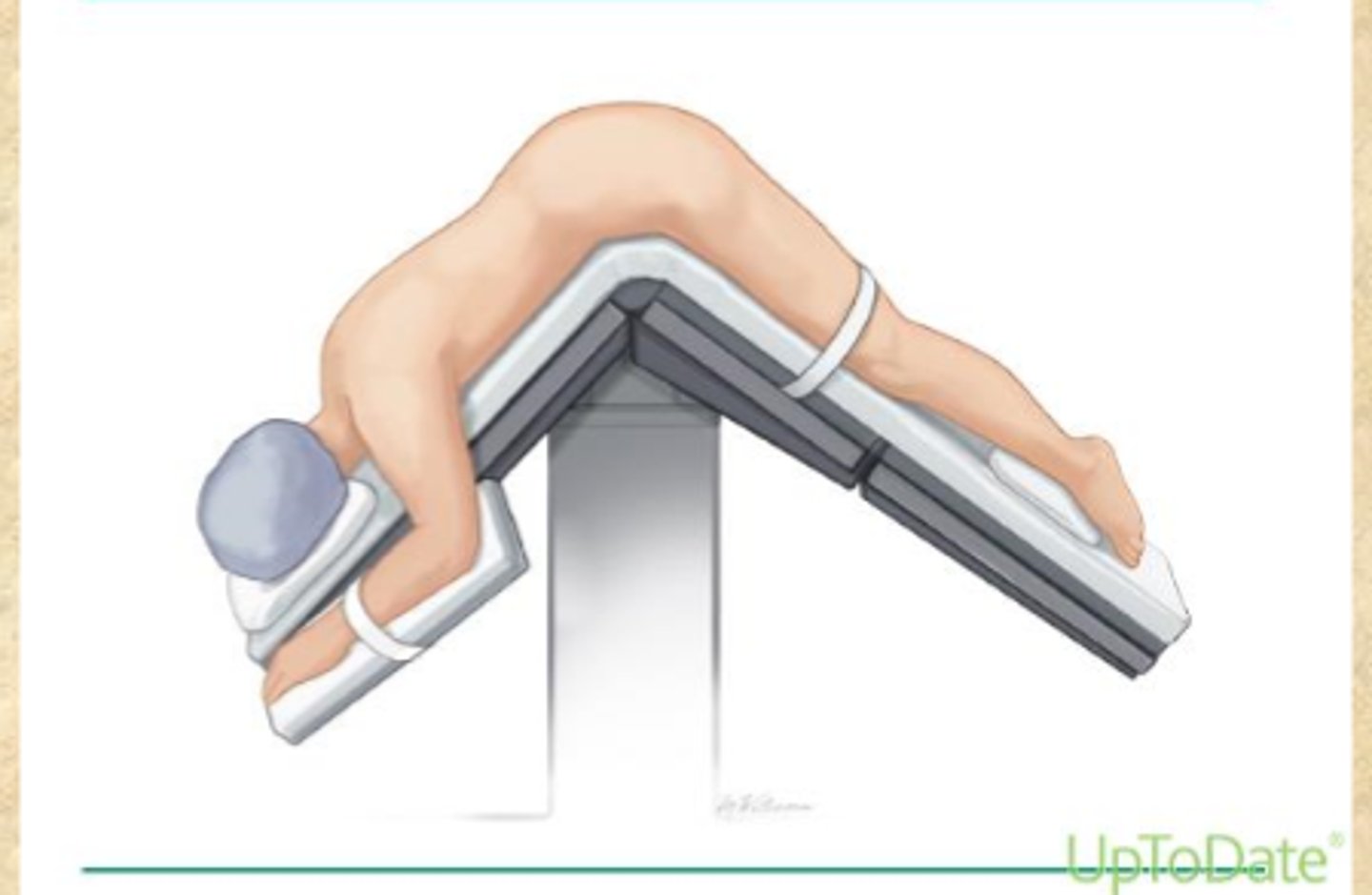
positions for anal exams
-knee-chest position (LLD, child's pose)
-prone jackknife position (for surgical purposes)
Anal fissures: non-pharm management
fiber supplements
Sitz baths
lateral internal sphincterectomy (causes minor incontinence)

Anal fissures: pharmacologic management
-topical anesthetics (temporary relief)
-for chronic fissures: topical nitro, diltiazem or nifedipine ointment, Botox injection
Fecal impaction: pathophys
-lack of ability to sense and respond to stool in rectum (decreased mobility and sensation)
-constipation plays a role
-older adults
Fecal impaction: clinical presentation
-abd cramping/bloating
-anorexia, n/v
-straining
-could have: leakage of watery diarrhea, rectal bleeding, lower back pain, bladder pressure/loss of control
Fecal impaction: DRE
-copious amounts of stool in rectum
-may or may not be hard
-if stool absent on DRE, doesn't rule out fecal impaction (get an abdominal radiograph)
Fecal impaction: potential complications
-increase intraluminal pressure -> ulcers, colitis, ischemia, necrosis
-sustained dilation -> megacolon, increased colonic secretions
Fecal impaction: predisposing factors
-meds
-severe psych disorders
-prolonged bed rest
-neurogenic disorders of the colon
-spinal cord disorders
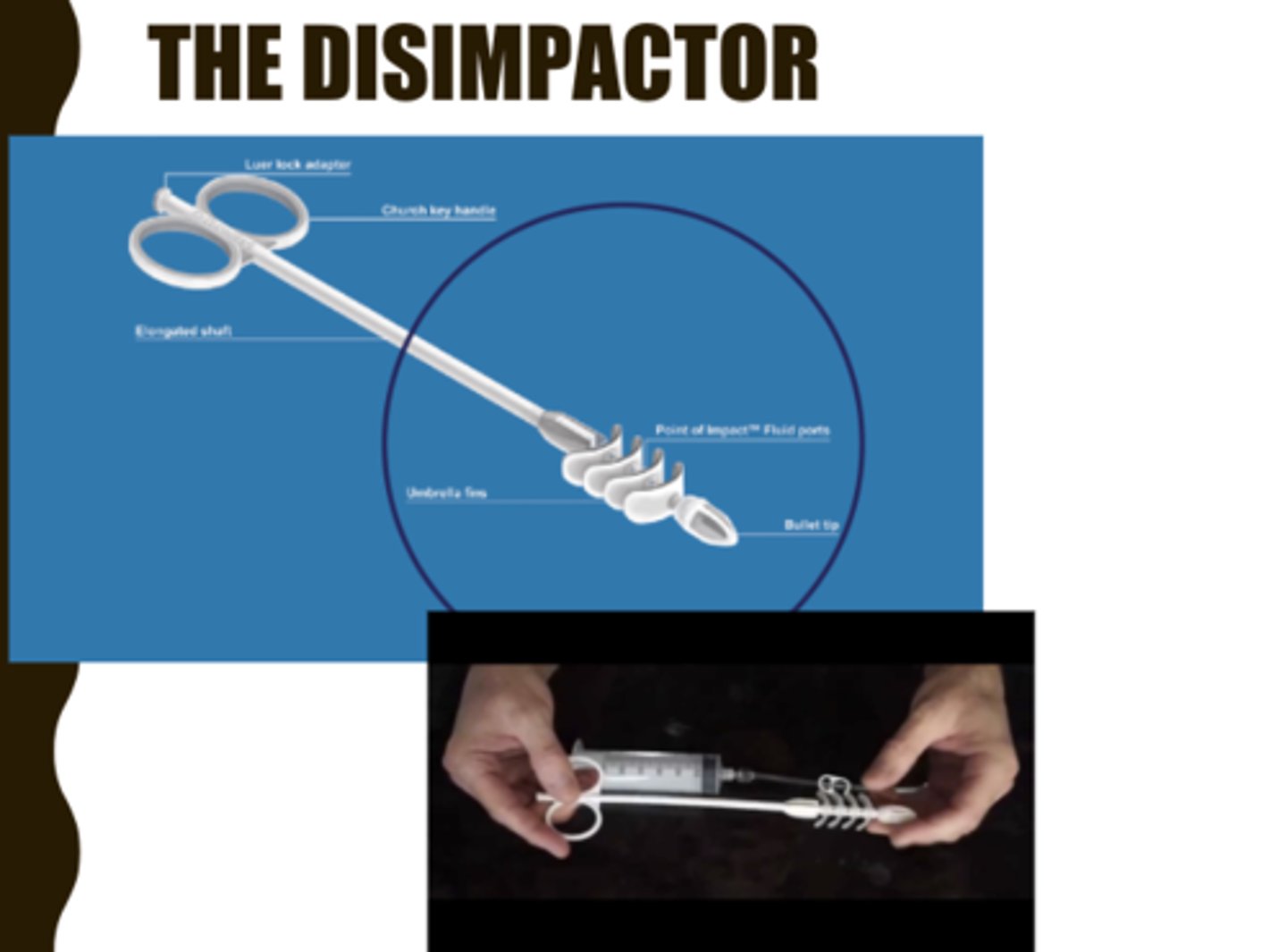
Fecal impaction: non-pharm management
-digital disimpaction (painful) and colon evacuation
-device: The Disimpactor
-if others fail: colonoscope with snare to break it up
-if tenderness/bleeding occur, may indicate perforation or ischemia- SURGERY
Fecal impaction: pharm management
-after digital disimpaction, warm-water enema (if this fails: anesthesia and abdominal massage)
-proximal impaction: polyethylene glycol (PEG) solutions
-increase fiber
Toxic megacolon: general
-total or segmental non-obstructive dilation of colon in setting of systemic toxicity
-cause: any inflammatory or infectious condition of colon
Toxic megacolon: pathophys
inflammation-> increased nitric oxide (NO) production -> inhibits smooth muscle -> smooth muscle layer is inflamed and paralyzed-> colonic dilation
Toxic megacolon: predisposing conditions
-IBD (ulcerative colitis > Crohn)
-recurrent C. diff
-salmonella, shigella or campylobacter
-hemorrhagic colitis
-HUS
-amoebic infection
-CMV
Toxic megacolon: risk factors
hypokalemia
anti motility agents
opioids
anticholinergics
antidepressants
abruptly stopping glucocorticoids
Barium enemas
Toxic megacolon: clinical presentation in pts with IBD
-occurs early in IBD
-severe bloody diarrhea refractory to therapy > 1 week prior to acute colonic dilation
-diarrhea may improve once dilation occurs
Toxic megacolon: clinical presentation in all pts
-severely ill
-tender/distended abdomen
-fever, tachycardia, hypotension
-altered sensorium
-reduced/absent bowel sounds
-peritonitis
Toxic megacolon: diagnostics
-plain radiograph: long air-filled colon >6 cm in diameter, loss of haustra, "thumb printing", mucosal nodules
-leukocytosis

Toxic megacolon: what can mask s/s?
corticosteroids, analgesics or clouded sensorium
Toxic megacolon: potential complications
perforation
sepsis
shock
death
Toxic megacolon: non-pharm management
-admission, consult surgery/ gastroenterology
-if pharm fails, partial or total colectomy
Toxic megacolon: pharm management
steroids
ABX
other immunosuppressive agents