Neoplasia and Neoplastic Disease
1/84
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
85 Terms
Uncontrolled, abnormal growth of cells or tissues
Tumor, Nodule, Mass, (nonspecific term)
●Neoplasia (new growth) - a process involving the abnormal proliferation of cells, leading to tumor formation.
Neoplasia
Neoplasm
●Neoplasm - an abnormal mass of tissue that results from neoplasia, which can be benign or malignant.
Does not imply benign or malignant.
I.e. there are benign neoplasms and malignant neoplasms
Disease in which abnormal cells divide uncontrollably and destroy body tissue
Cancer
Branch of medicine that specializes in the diagnosis and treatment of cancer
Oncology
Malignancy
The presence of cancerous cells
Metastasis
A pathogenic agent’s spread from an initial or primary site to a different or secondary site.
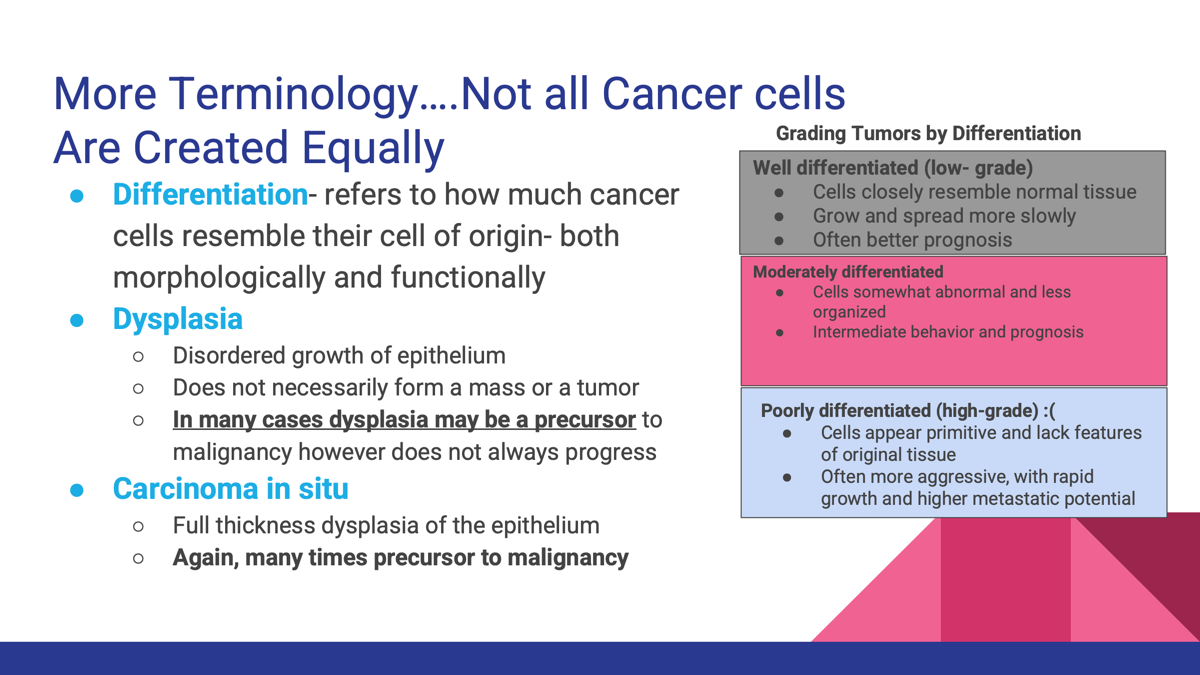
Refers to how much cancer cells resemble their cell of origin- both morphologically and functionally.
Differentiation- Well-differentiated refers to tumor cells that closely resemble normal cells, while poorly differentiated indicates significant deviation from original cell types.
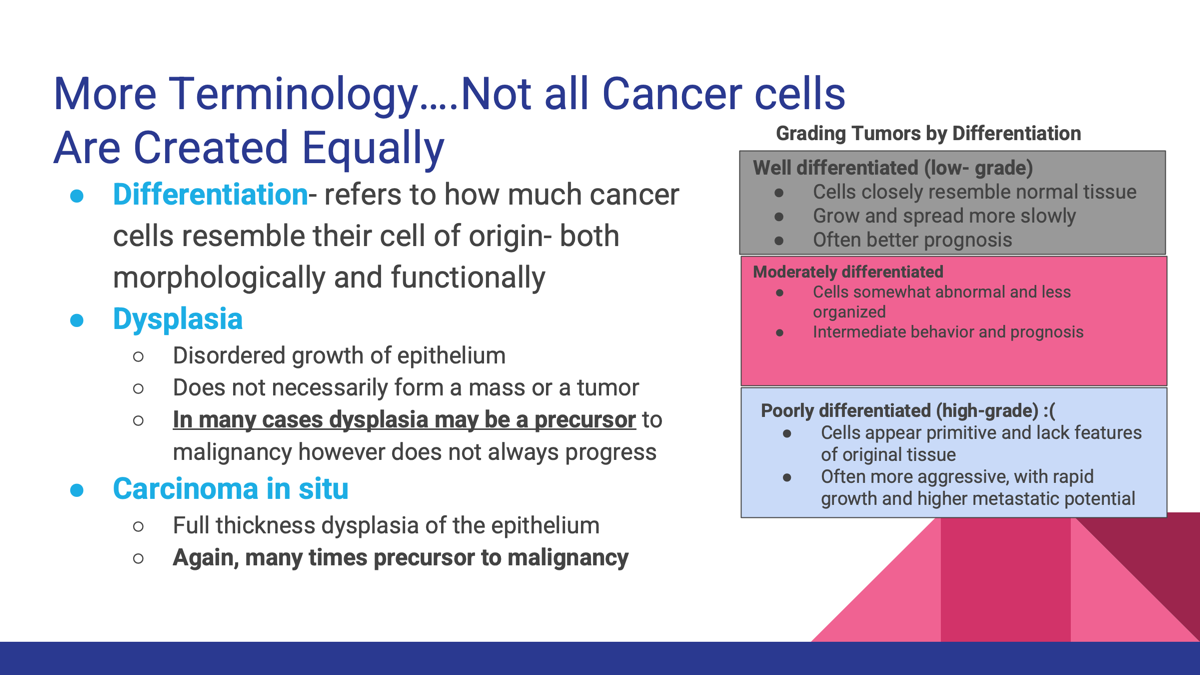
Dysplasia
Disorder growth of epithelium.
Does not neceform mass or tumor.
In many cases dysplasia may be a precursor to malignancy however does not always progress.
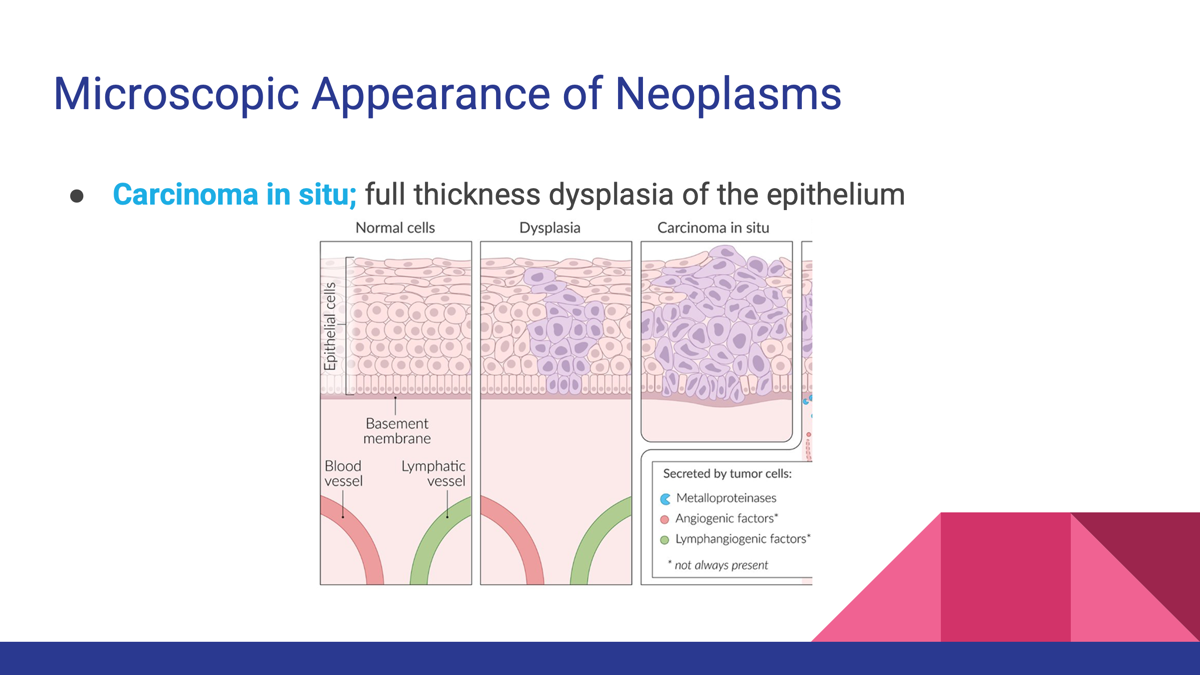
Carcinoma id Situ
full thickness of the epithelium.
○Again, many times precursor to malignancy
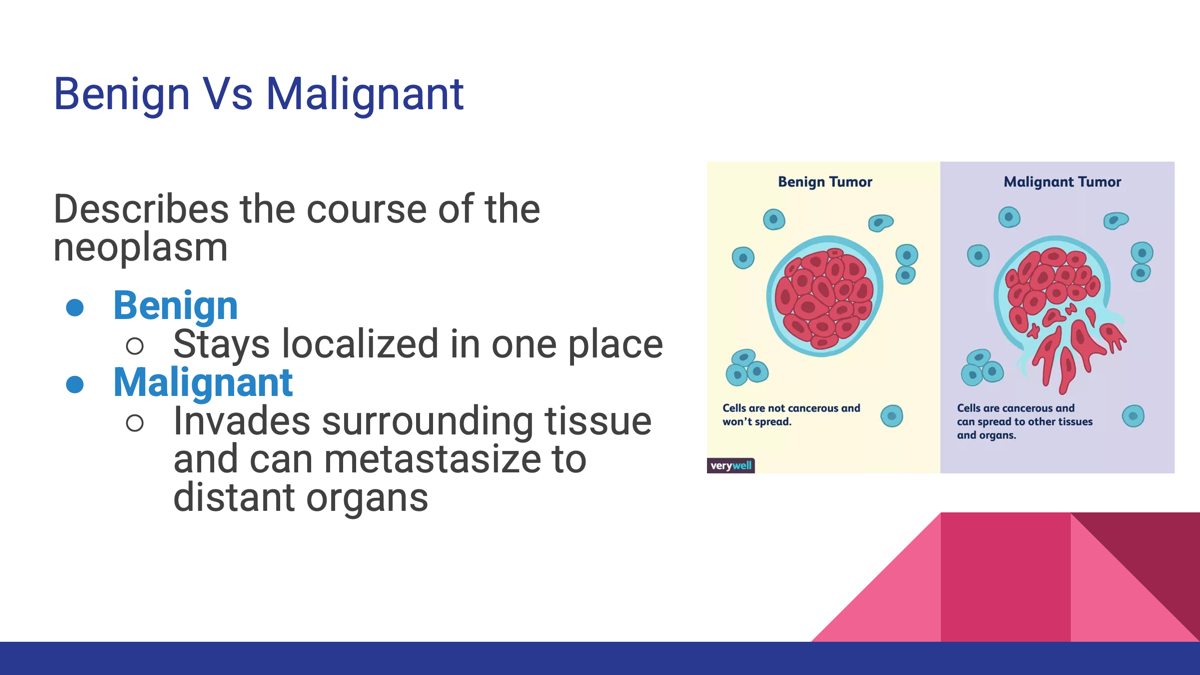
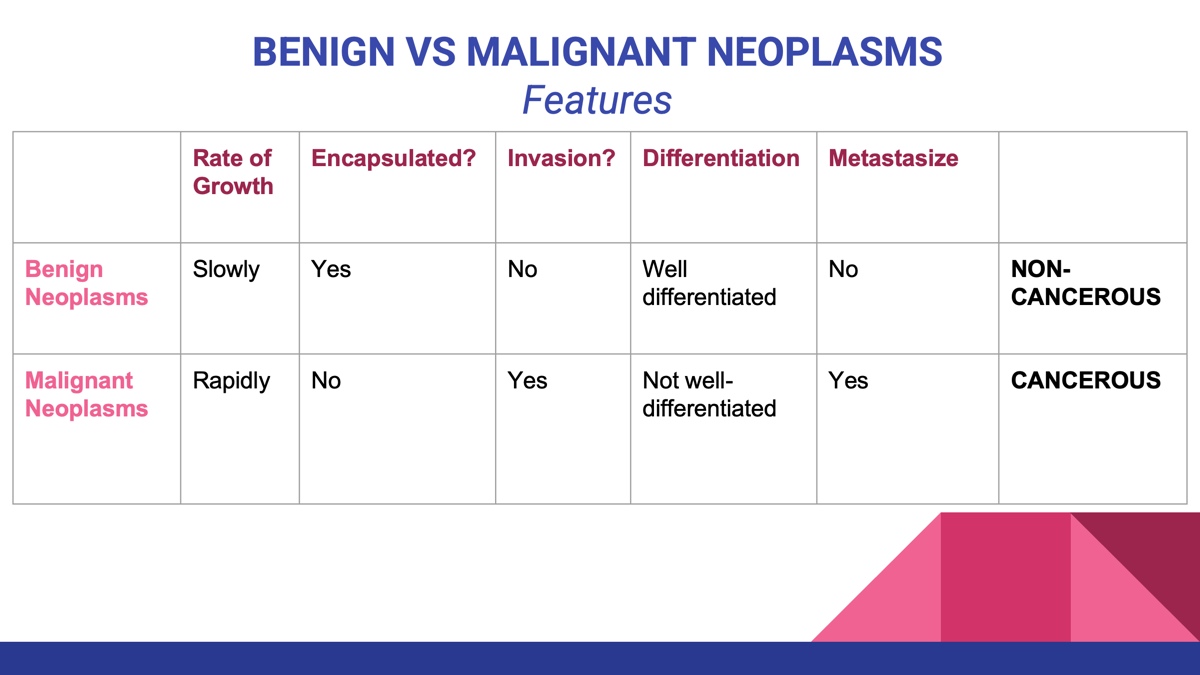
What is the difference between Benign and Malignant?
Benign tumors are non-cancerous, typically grow slowly, and do not invade surrounding tissues or metastasize, while malignant tumors are cancerous, can grow rapidly, invade nearby tissues, and spread to other parts of the body.
A benign neoplasm often ends in?
-oma, indicating a tumor that is generally non-invasive.
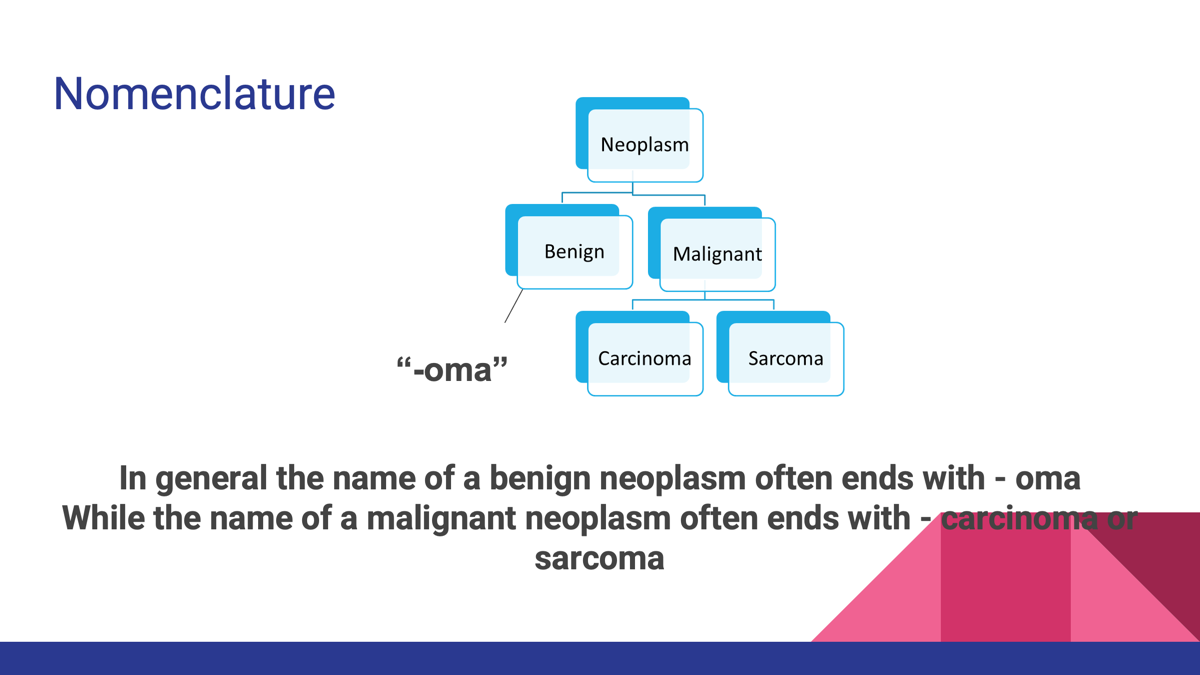
A malignant neoplasm often ends in?
-carcinoma or -sarcoma, indicating a tumor that is invasive and cancerous.
Exceptions to the neoplasm nomenclature:
What is the most common type of cancer common in adults?
Carcinoma-
○Derived from ectodermal and endodermal tissue
○Includes epithelial tissue cancers
■Lung, colon, breast, prostate cancer
■Think adenocarcinoma, squamous cell carcinoma, intraductal carcinoma
○More common in adults
Feature | Carcinoma | Sarcoma |
|---|---|---|
Origin | Epithelial tissue | Connective tissue |
Tissues involved | Skin, glands, organ linings | Bone, muscle, fat, cartilage, blood vessels |
Frequency | Most common cancers | Much rarer cancers |
Examples | Lung carcinoma, breast carcinoma, colon carcinoma | Osteosarcoma, liposarcoma, chondrosarcoma |
What is the rarer type of cancer and often aggressive?
Sarcoma-
○Originates from mesodermal tissue
○Arises from mesenchymal cell types in connective tissue (fat, cartilage or bone)
■Rhabdomyosarcoma (skeletal muscle)
■Leiomyosarcoma (smooth muscle)
■Angiosarcoma (Blood vessels)
○More common in children
Often times aggressive :(
Feature | Carcinoma | Sarcoma |
|---|---|---|
Origin | Epithelial tissue | Connective tissue |
Tissues involved | Skin, glands, organ linings | Bone, muscle, fat, cartilage, blood vessels |
Frequency | Most common cancers | Much rarer cancers |
Examples | Lung carcinoma, breast carcinoma, colon carcinoma | Osteosarcoma, liposarcoma, chondrosarcoma |
Reliable indicators of malignancy in many organs?
Histologic features
However, in some sites, they do not always distinguish benign from malignant neoplasms
What are microscopic features that make pathologists suspect a tumor is malignant (cancerous)?
Pleomorphism- variation in nuclear and cytoplasmic shape between cells. Cancer cells look irregular and different from one another.
Abnormal mitotic figures and increased numbers of mitotic figures: They may show abnormal mitotic figures, meaning mistakes occur during chromosome separation.
Hyperchromasia- the nucleus stains darker than normal. increase in DNA material in nucleus.
Hypercellularity: Increased number of cells (i.e. within the bone marrow) with a loss of normal polarity
(Abnormal mitotic figures- dysregulated and random nuclear material assembly
Increased numbers of mitotic figures- more cells in mitosis, higher turnover
Polarity- asymmetric distribution of cell’s proteins, organelles, cytoplasm etc)
Differentiation
Refers to how closely a tumor resembles the normal tissue from which it originated, Indicating its level of maturity and function.
This differentiation resembles tissue of origin and are well differentiated:
Benign tumor- closely resembles normal tissue and maintains similar structure.
Poorly differentiated or undifferentiated (anaplastic)
Malignant tumor- that lacks structural and functional features of the tissue of origin, making it difficult to determine its cellular origin.
This refers to poorly differentiated cells that have lost the normal features of the tissue they came from.
Anaplastic
What are examples of microscopic appearance of neoplasms?
Well Differentiated: resembles normal tissue structure. Benign tumor)
Poorly Differentiated: lacks normal architecture. (malignant tumor)
Cells that lose their specialized characteristics and revert to a more primitive - “to form backwards” embryonic state:
Anaplasia
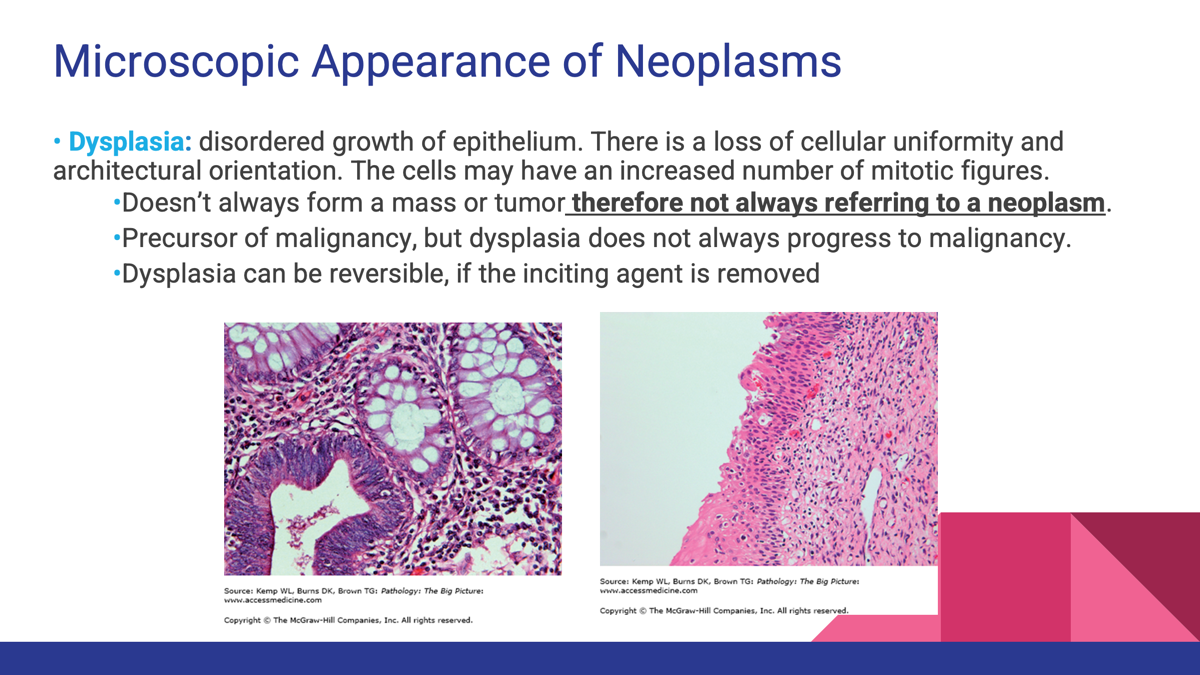
Disordered growth of epithelium where there is loss of cellular uniformity and architectural orientation.
dysplasia
What are the characteristic of Dysplasia?
Doesn’t always form a mass or tumor therefore not always referring to a neoplasm.
•Precursor of malignancy, but dysplasia does not always progress to malignancy.
•Dysplasia can be reversible, if the inciting agent is removed
full thickness dysplasia of the epithelium
carcinoma in situ
Neoplasm that tend to grow slower
benign neoplasm
tend to grow more quickly
malignant neoplasm
Proportion of neoplastic cells in the proliferative phase
Growth fraction
Growth fraction = % of tumor cells that are actively dividing
Infiltration of tumor cells into surrounding organs
Invasion
The spread of tumor cells to distant organs
Metastasis
cancer of epithelial tissues (lining/covering).
Carcinoma- through the lymphatics
cancer of connective tissues (bone, muscle, fat, cartilage
Sarcoma- through the blood
A definite indicator of a malignant neoplasm
Metastasis
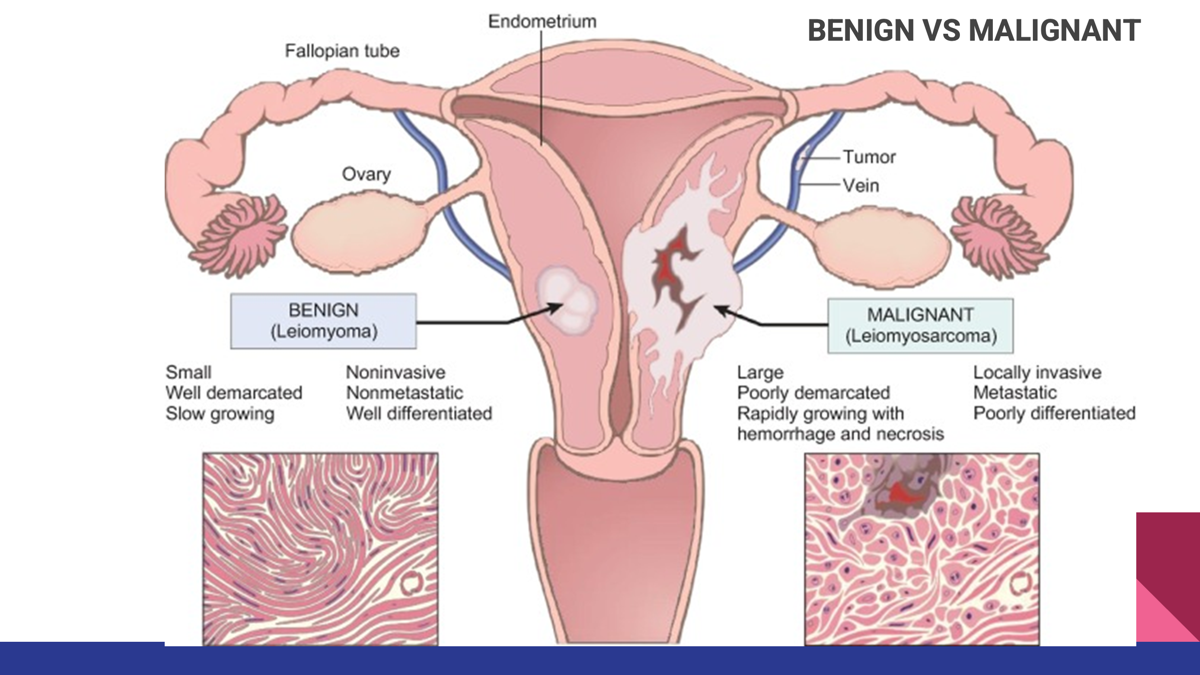
Benign vs Malignant neoplasm
Benign neoplasm
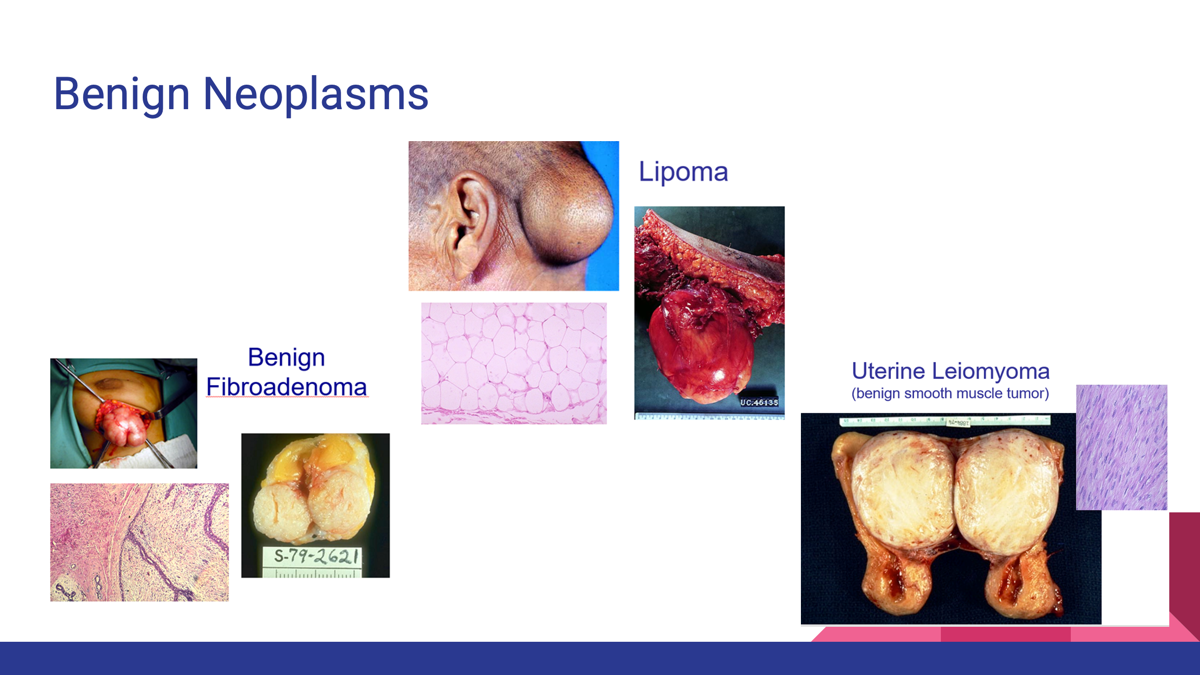
Malignant neoplasm
What is pre clinical phase of cancer?
The pre-clinical phase is the period when cancer is already developing, but the patient has no symptoms yet.
The pre-clinical phase of cancer is the stage when cancer or precancerous changes are present but the patient has no symptoms; the disease can often be detected through screening tests such as mammography or colonoscopy.
normal cellular gene that promotes cellular growth and division
Proto-oncogenes
proto-oncogenes that have mutated and are now capable of producing neoplasms.
Oncogenes:
○Always “on”
○Cause unregulated cell growth through promotion of cellular division, which results in further mutations
what is the function of proto-oncogene?
Function of a Proto-Oncogene
A proto-oncogene is a normal gene that helps regulate:
Cell growth
Cell division
Cell survival
Cell differentiation
Activation of Proto-oncogene?
When a proto-oncogene becomes overactive, it is called an oncogene.
The cell receives constant "grow" signals even when none are needed.
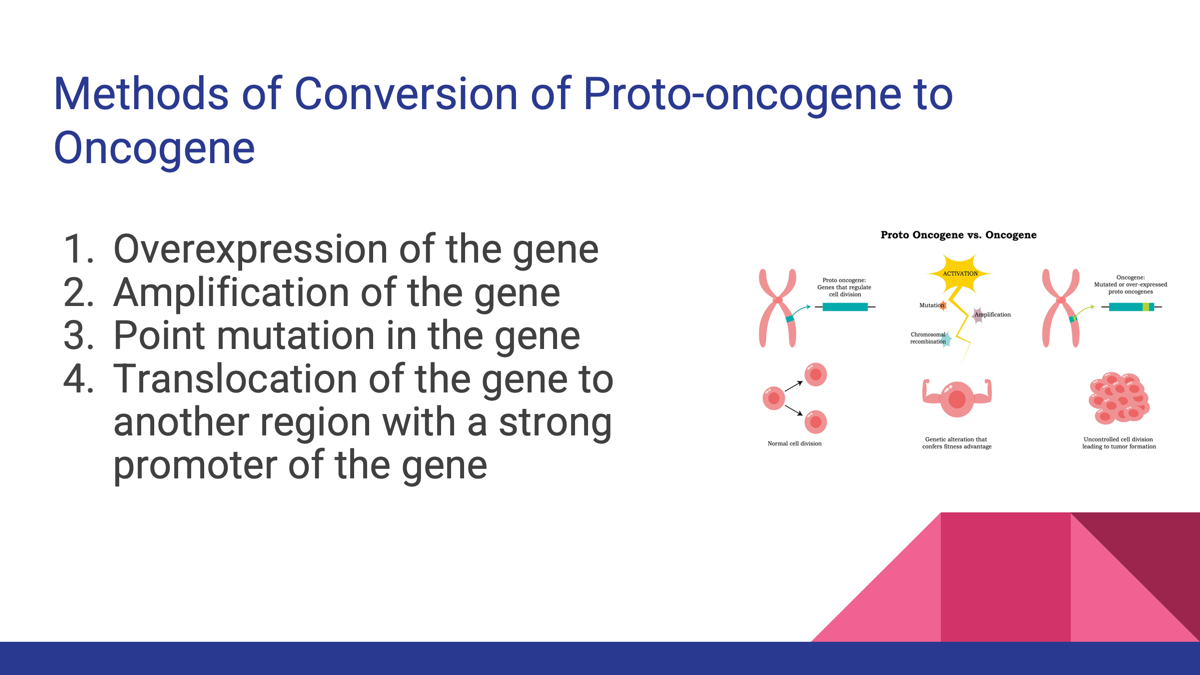
Proto-oncogenes are normal growth-promoting genes that regulate cell proliferation; when activated by mutation, amplification, overexpression, or translocation, they become oncogenes that drive uncontrolled cell growth and cancer.
What are the methods of conversation of Proto-oncogene to Oncogene
1.Overexpression of the gene
2.Amplification of the gene
3.Point mutation in the gene
4.Translocation of the gene to another region with a strong promoter of the gene
Cinical oncologic disorder of RAS
Colon Cancer
Intracellular signaling protein that promotes cell growth and division. Mutations leading to cellular division.
Clinical Oncologic disorder of KRAS
Lung, colon, Pancreatic
Another member of RAS family
Clinical Oncologic Disorders of HER2
Breast cancer
Growth factor receptor
Clinical Oncologic Disorders APC gene
Disruption of this leads to adenomas (non cancerous polyps) which then lead to colon cancer
Unlike RAS and HER2, APC normally prevents excessive cell growth. (Tumor suppressor gene)
Clinical Oncologic Disorders P53
Leukemias
Inactivated in many cancers, cannot repair DNA or lead to apoptosis. (Tumor Suppressor gene)
Clinical Oncologic Disorders: BRCA1 and BRCA 2
Involved in DNA repair
Mutations related to BOTH breast and ovarian cancers
Hepatitis B virus (HBV)
Hepatocellular carcinoma (liver cancer)
Mechanism: Through chronic inflammation; also because HBV protein binds p53(normally a tumor suppressor gene), interfering with its function leading to cancer
Helicobacter pylori
Associated neoplasm: MALTomas of the stomach (neoplasm of mucosa-associated lymphoid tissue)
Human herpesvirus 8 (HHV-8)
Associated neoplasm: Primary effusion lymphoma and Kaposi sarcoma
Role of hormones in Carcinogenes
Hormones can stimulate cell growth and increase the chance of mutations.
Examples
Estrogen → promotes breast cell proliferation
Androgens (testosterone) → promote prostate cell growth
Role of growth factors in carcinogenesis
Growth factors are proteins that tell cells to grow, divide, and survive.
Example: PDGF
Some tumors (such as glioblastomas) produce their own platelet-derived growth factor (PDGF), creating a continuous growth signal.

Role of growth factor receptors
Growth Factor Receptors
Cancer cells may make too many receptors.
Example: HER2 and EGFR
HER2 amplification → breast cancer
EGFR (ERBB1) overexpression → lung cancer
More receptors = stronger growth signals
Synthesize nuclear transcription factors
Nuclear Transcription Factors
These proteins turn genes on inside the nucleus.
Example: MYC
MYC activates genes involved in cell growth and the cell cycle.
When MYC is overexpressed:
➡ Increased transcription
➡ Increased cell division
➡ Cancer development
Associated with Burkitt lymphoma and several solid tumors.

Loss of regulation of cyclins and cyclin-dependent kinases
Cell Cycle Genes Cyclins and Cyclin-Dependent Kinases (CDKs)
These regulate progression through the cell cycle.
If cyclins/CDKs become overactive:
➡ Cell-cycle checkpoints are bypassed
➡ Cells divide uncontrollably
➡ Tumors develop
Early changes in progression of neoplasia:
Early Changes: Dysplasia
Dysplasia is the earliest recognizable precancerous change.
Dysplasia = "abnormal cells but not cancer yet."
○Disordered growth of epithelium
○Does not necessarily form a mass or a tumor
○In many cases dysplasia may be a precursor to malignancy however does not always progress.
middle changes in the progression of neoplasia?
Changes: Carcinoma in situ
Carcinoma in situ refers to a localized tumor that has not invaded surrounding tissues.
late changes in the progression of neoplasia?
malignant neoplasm
The malignant cells break through the basement membrane and invade surrounding tissues.
Malignant neoplasm that originates from mesodermal tissue
Sarcoma
○Originates from mesodermal tissue
○Arises from mesenchymal cell types in connective tissue (fat, cartilage or bone)
■Rhabdomyosarcoma (skeletal muscle)
■Leiomyosarcoma (smooth muscle)
■Angiosarcoma (Blood vessels)
○More common in children
Often times aggressive
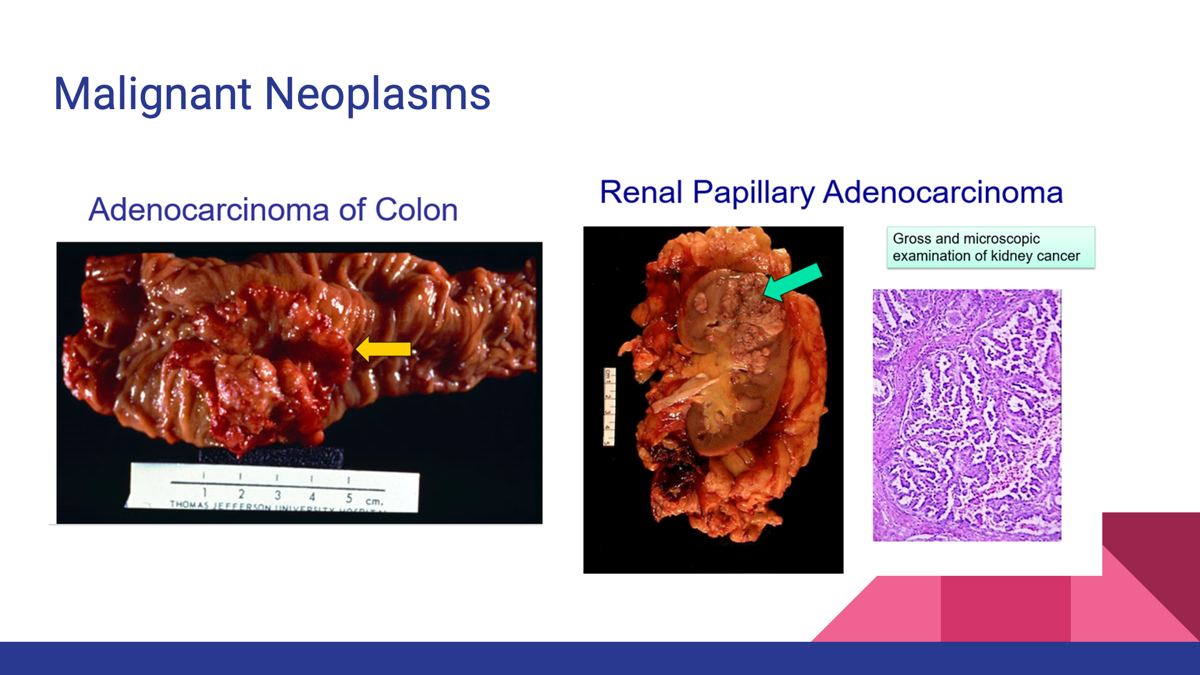
Malignant neoplasm that is derived from ectodermal and endodermal tissue:
Carcinoma
○Most common type of cancer
○Derived from ectodermal and endodermal tissue
○Includes epithelial tissue cancers
■Lung, colon, breast, prostate cancer
■Think adenocarcinoma, squamous cell carcinoma, intraductal carcinoma
○More common in adults
Phenotypic changes in the progression of neoplasia:
Phenotypic Changes of Dysplasia
Dysplasia means disordered growth of epithelial cells.
Phenotypic changes:
Increased cellularity
Hyperchromatic (dark) nuclei
Increased mitotic figures
Loss of normal cell organization (polarity)
Increased nuclear-to-cytoplasmic ratio
At this stage:
Cells look abnormal
Basement membrane remains intact
May be reversible if the cause is removed
📌 Not yet cancer, but often a precursor to cancer.
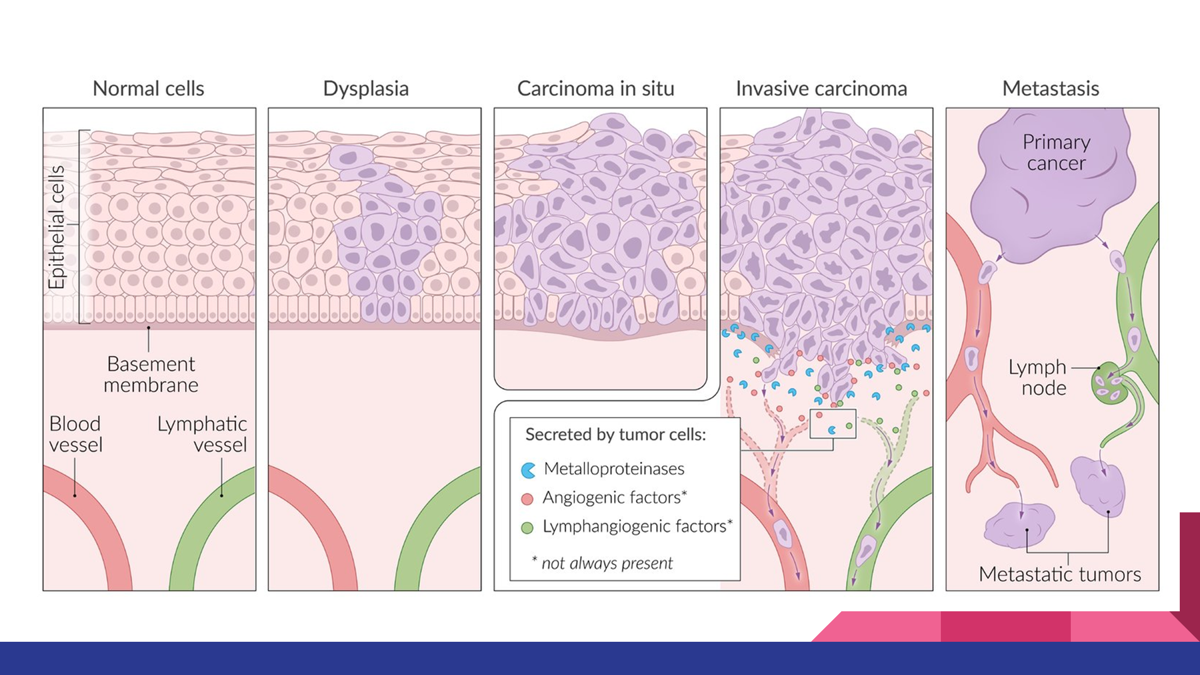
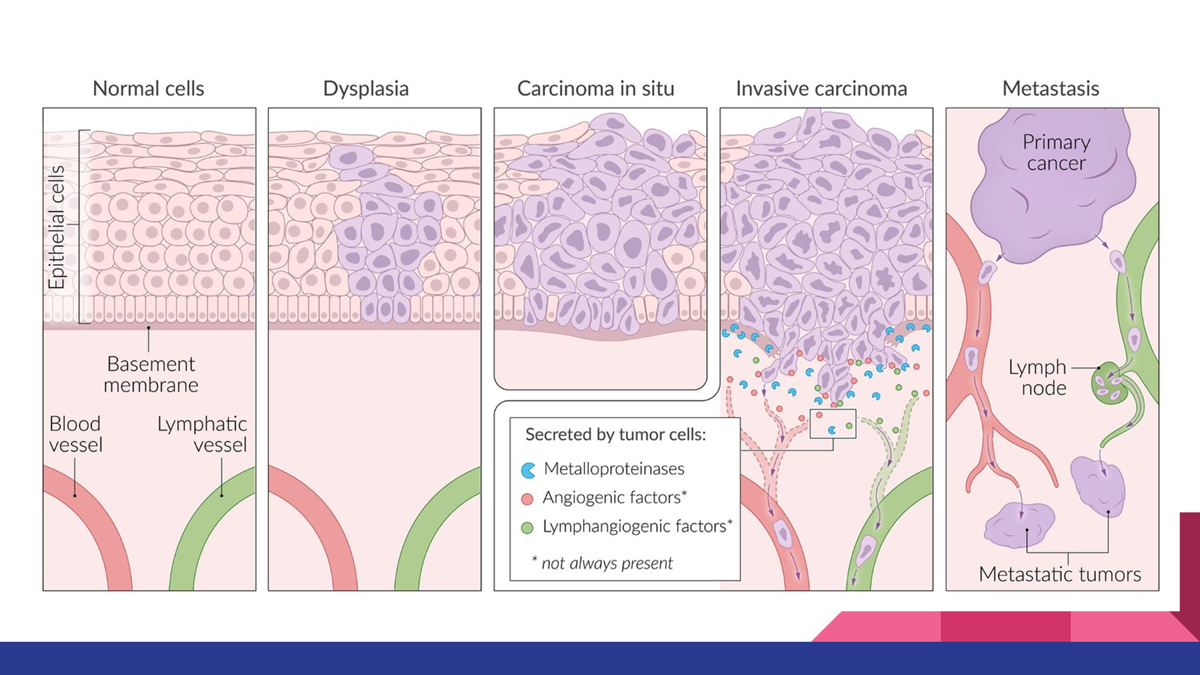
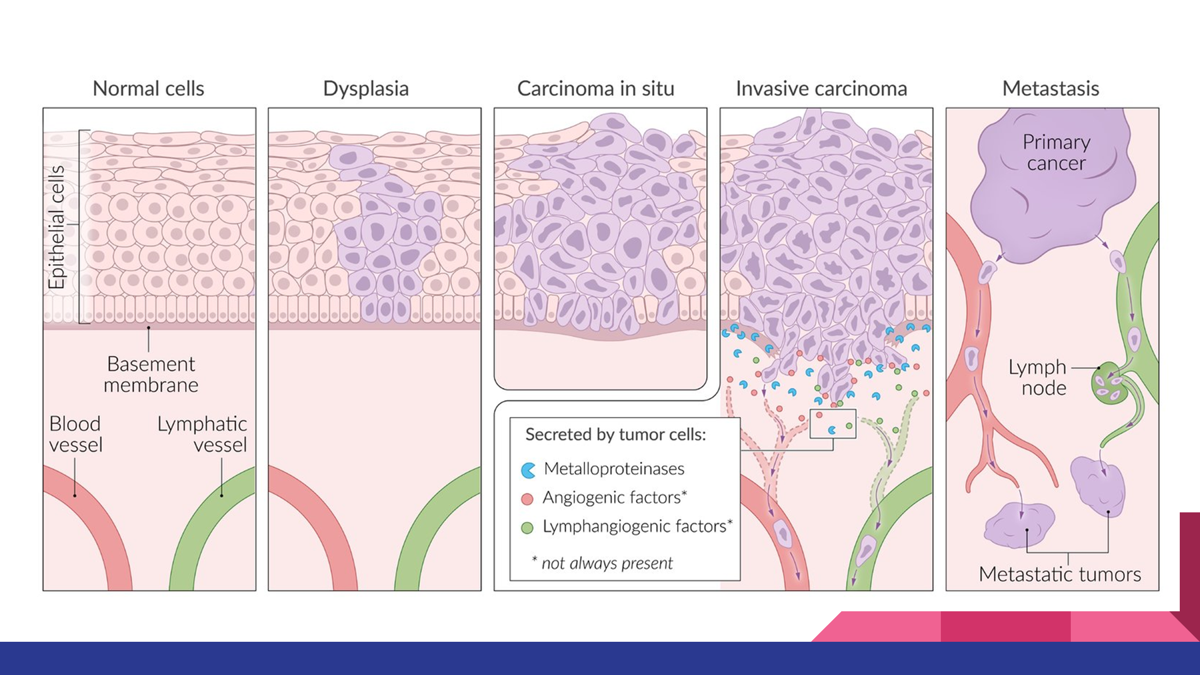
Describe the phenotypic changes in the progression of neoplasia?
The phenotypic progression of neoplasia involves dysplasia (abnormal growth), carcinoma in situ (full-thickness dysplasia without invasion), invasive carcinoma (penetration through the basement membrane), and metastatic carcinoma (spread to distant sites).
Normal Epithelium → Dysplasia → Carcinoma in Situ → Invasive Carcinoma → Metastatic Carcinoma.
Describe the two principal lines of evidence that support the model of stepwise genetic alterations in colon cancer.
The two principal lines of evidence are:
Histologic observation of progressive lesions from normal mucosa to adenoma to carcinoma.
Identification of sequential genetic alterations (APC → KRAS → TP53 and others) that accumulate as the tumor progresses.
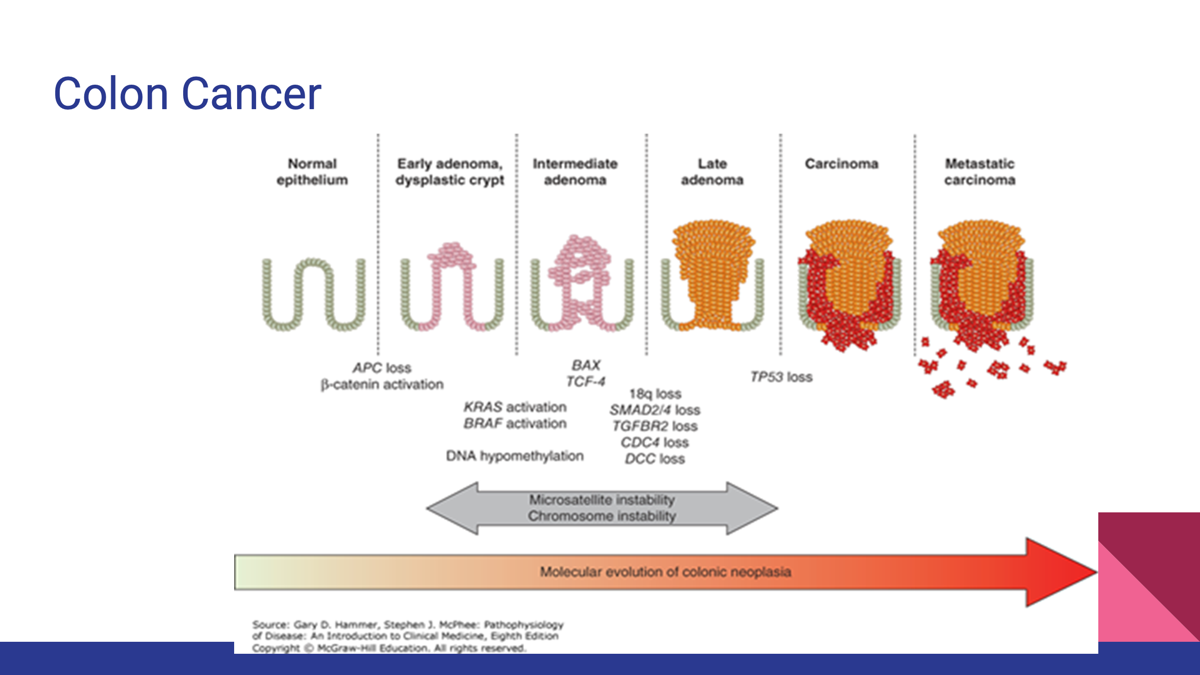
•Model of stepwise genetic alterations in cancer is best illustrated by observation of colonic lesions at different stages of progression to malignancy.
•Schematic illustrates the sequential phases of cellular abnormalities and polyp formation in the colon as shown on a timeline that also depicts the corresponding genetic events associated with each cellular landmark.
•APC tumor suppressor gene mutation —> abnormal cell proliferation —> polyps
•Polyp formation—>oncogenes —> activation of growth factor receptor signaling pathways —> polyps grow bigger
•Mutations in specific genes (DCC) or inactivation of TP53 disrupts cell cycle checkpoints and apoptosis → invasive cancer phenotype develops
•Mismatch repair genes (if mutation in gene, then cannot proofread, and thus errors are propagated)
•As adenomas develop and enlarge, an early feature prior to invasion that occurs, is the development of new vessels or destruction of existing vessels —> microscopic bleeding that can be detected on fecal occult blood tests
What are epithelial based carcinoma?
Colon Cancer and Breast Cancer
Carcinoma = Coverings (epithelium)
Sarcoma = Support tissues (connective tissue)
Lymphoma = Lymphocytes
Leukemia = Bone marrow/blood
Germ Cell = Reproductive cells
Neuroendocrine = Hormone-secreting cells.
Colon Carcinoma
A carcinoma arising from epithelial cells of the colon.
Colon Carcinoma
A carcinoma arising from epithelial cells of the colon.
Develops through a series of genetic alterations:
APC mutation → adenomatous polyp formation
KRAS activation → polyp growth
TP53 loss and other mutations → invasive carcinoma
Most colon cancers are adenocarcinomas
Breast Carcinoma
Ductal/Lobular tissue
Malignant epithelial tumor of the breast.
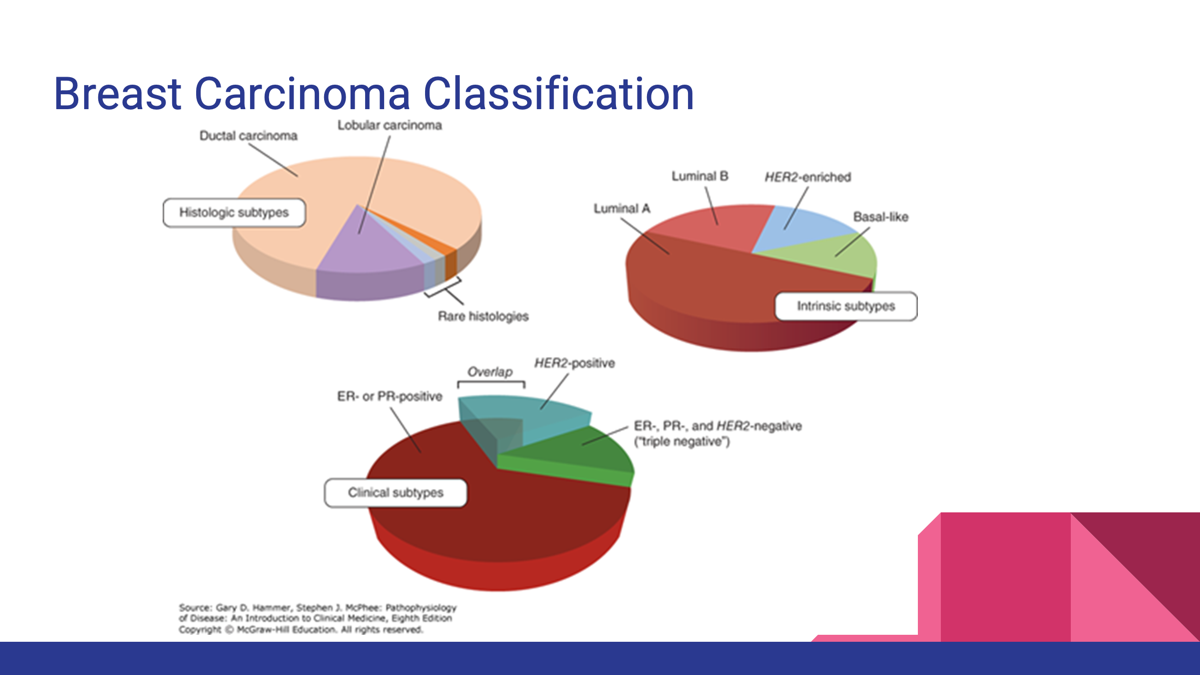
Histologic types:
Ductal carcinoma
Lobular carcinoma
Clinical classification is based on:
Estrogen receptor (ER)
Progesterone receptor (PR)
Human epidermal growth factor receptor 2 (HER2)
HER2-positive tumors may respond to HER2-targeted therapy
Breast cancers are frequently classified using different classification systems. Three are shown here—histologic subtypes (top left), intrinsic subtypes (top right), and clinical subtypes (bottom)—with their proportional incidences shown via pie chart. The clinical subtypes, widely used in clinical management, do not divide breast cancers into exclusive categories, such that a cancer can be both ER/PR positive and HER2 positive (ie, HER2 amplified), as shown by the overlapping area in the bottom pie chart.
Mesenchymal, Neuroendocrine, and Germ Cell Neoplasms
Carcinoid Tumors (Neuroendocrine), Testicular Germ Cell Cancer, Sarcomas (Mesenchymal)
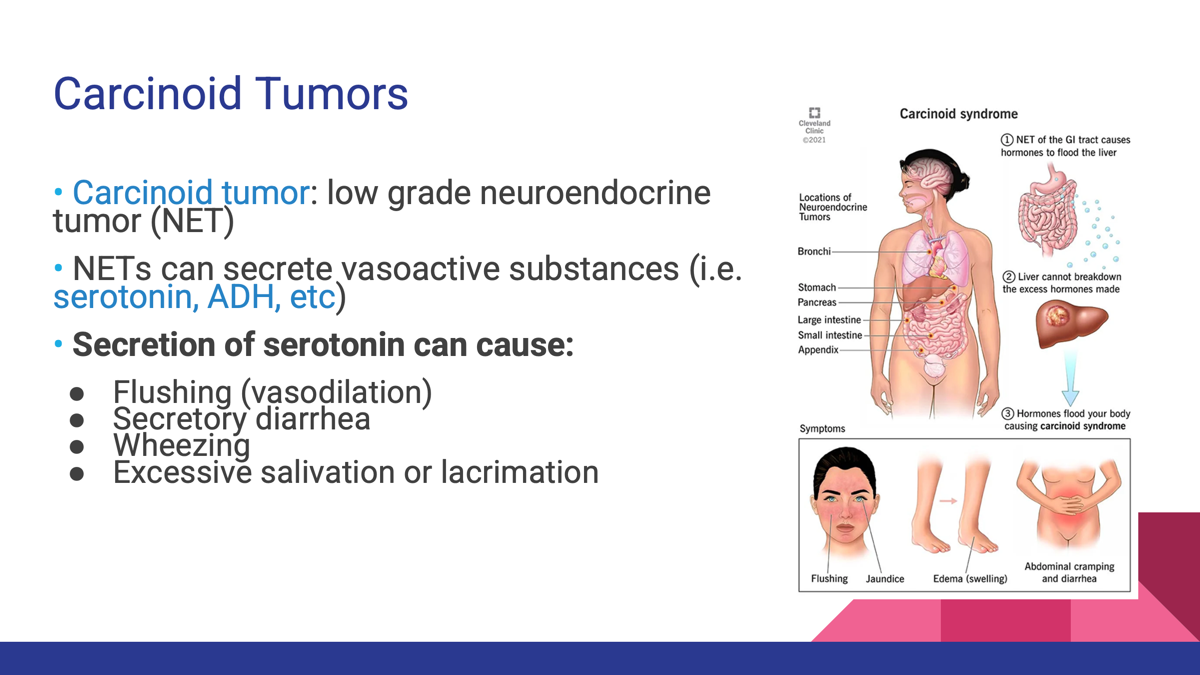
Carcinoid Tumors (Neuroendocrine)
Low-grade neuroendocrine tumors (NETs).
Arise from cells with endocrine and nervous system features.
Can secrete hormones such as serotonin.
Neuroendocrine tumors (NET) arise from neural crest tissue. Cells migrate to submucosal layer of intestines and pulmonary bronchi thus they can at times express enzymes to produce peptide hormones.
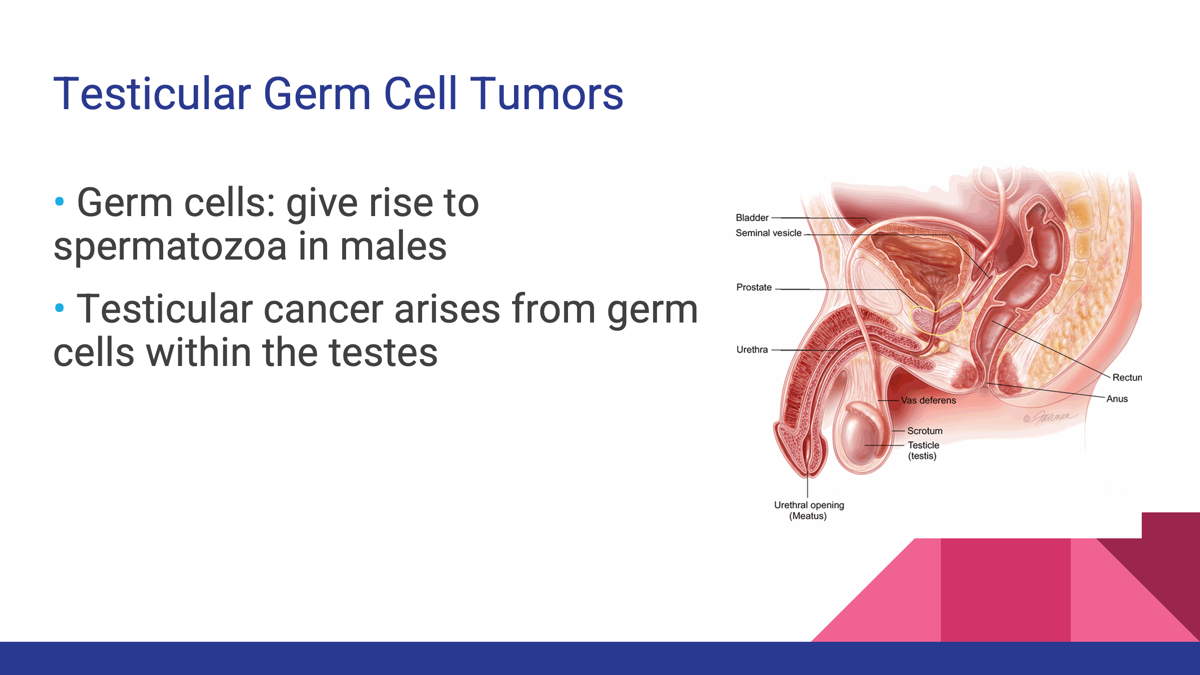
Testicular Germ Cell Cancer
Arises from germ cells that normally produce sperm.
Sarcomas (Mesenchymal)
Arise from mesoderm-derived connective tissues.
More common in children than adults.
Spread primarily through the bloodstream.
Examples:
Osteosarcoma (bone)
Rhabdomyosarcoma (skeletal muscle)
Leiomyosarcoma (smooth muscle)
Liposarcoma (fat)
Hematologic Neoplasms
Lymphomas, Acute Myelogenous Leukemia (AML)
Lymphomas
Malignancies of mature lymphocytes.
Usually involve lymph nodes and lymphatic tissues.
Types:
Hodgkin lymphoma
Non-Hodgkin lymphoma
Acute Myelogenous Leukemia (AML)
Malignancy of immature myeloid (blasts).
Rapid onset and aggressive course.
Causes bone marrow failure leading to:
Anemia
Infection
Bleeding.
Chronic Myelogenous Leukemia (CML)
Myeloproliferative neoplasm with a more indolent course.
Associated with the Philadelphia chromosome t(9;22) producing the BCR-ABL fusion gene.
Can progress to an acute "blast crisis."
Carcinoma = Epithelial
Colon cancer
Breast cancer
Sarcoma = Mesenchymal
Bone, muscle, fat, connective tissue cancers
Neuroendocrine Tumors
Carcinoid tumors
Germ Cell Tumors
Testicular germ cell cancer
Hematologic Tumors
Lymphomas
Leukemias (AML, CML)
How Grading and Staging Predict the Clinical Behavior of a Malignant Tumor
1. Grading = What the Tumor Cells Look Like
Grade describes the microscopic appearance and behavior of tumor cells.
Pathologists evaluate:
Degree of differentiation
Nuclear appearance (chromatin)
Number of mitotic figures (cell division rate)
2. Staging = How Far the Cancer Has Spread
Stage describes the anatomic extent of the cancer.
TNM System
T = Tumor size and local extent
N = Lymph node involvement
M = Presence of distant metastasis
Grading predicts tumor aggressiveness by evaluating how differentiated the tumor cells are microscopically. Staging predicts prognosis by determining the extent of tumor spread using systems such as TNM and stages I–IV. In general, higher grade and higher stage tumors have a worse prognosis and require more aggressive treatment.
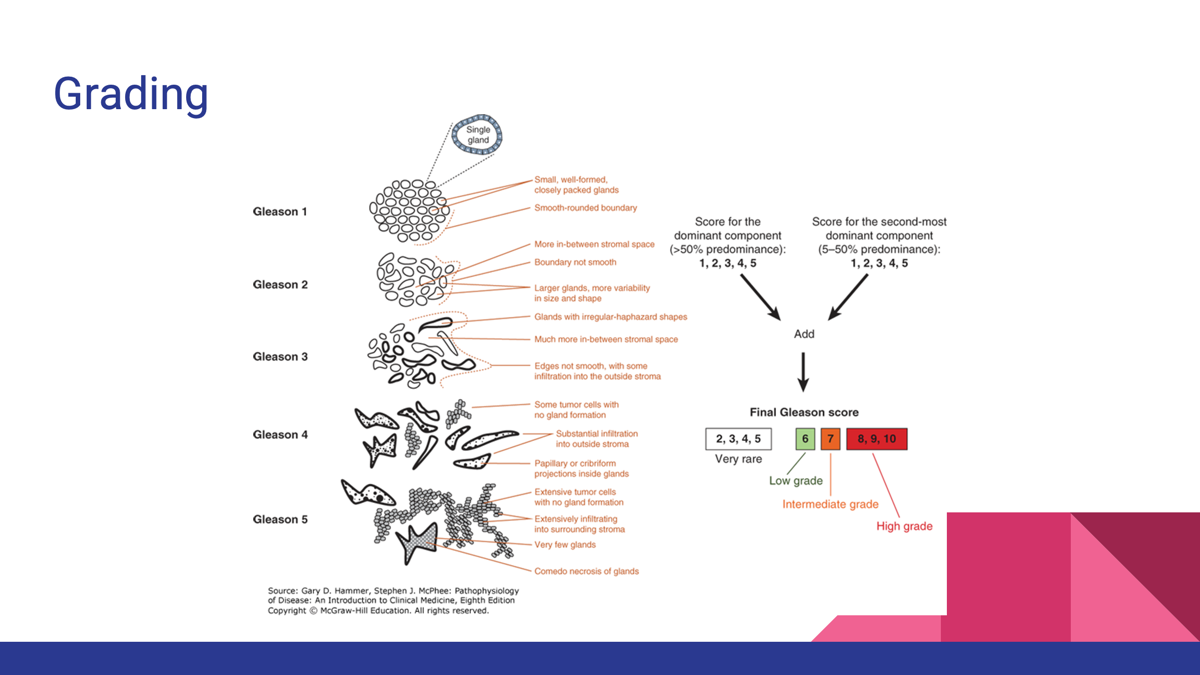
Grading tumor
●Grade
●Describes the appearance and behavior of the tumor cells
●Determined by pathologist based on well-defined criteria developed for the tissue analysis of each type of cancer
●Criteria involved:
○Differentiation of a tumor
○Quality of nuclear chromatin
○Quantitative assessment of proliferative rate (mitoses)
Staging
Different systems used to describe the extent and spread
1. Numerical Staging System (I-IV)
a.Describes the anatomic extent of the cancer at and beyond its site of origin
b.Used for solid tumors
2.TNM Staging System
a.T- tumor size and extent
b.N - number of lymph nodes involved
c.M – metastasis stage ( 0 if no distant metastases, or, 1 if distant metastases present)
•The numbering system for TNM staging is different for each type of cancer
What are the direct effects of of Malignancies
Location/Effect | Clinical Manifestation |
|---|---|
Bone marrow involvement | Pancytopenia, infection, bleeding |
Brain mass | Headache, weakness, numbness, gait abnormalities, visual changes, personality changes |
Nerve invasion | Pain, weakness, numbness |
Blood vessel invasion | Hemorrhage (hemoptysis, hematuria, bleeding into body cavities) |
Compression of blood vessels | Ischemia or infarction |
Bowel obstruction | Constipation, bowel obstruction |
Lung obstruction | Pneumonia |
Bile duct obstruction | Jaundice |
Bone destruction | Pain and pathologic fractures |
Direct effects = problems caused by the physical presence, growth, invasion, or obstruction of the tumor.
Caused by the physical growth and invasion of the tumor, leading to:
Obstruction
Compression
Hemorrhage
Neurologic deficits
Bone destruction
Organ dysfunction
Indirect Effects (Paraneoplastic Syndromes)
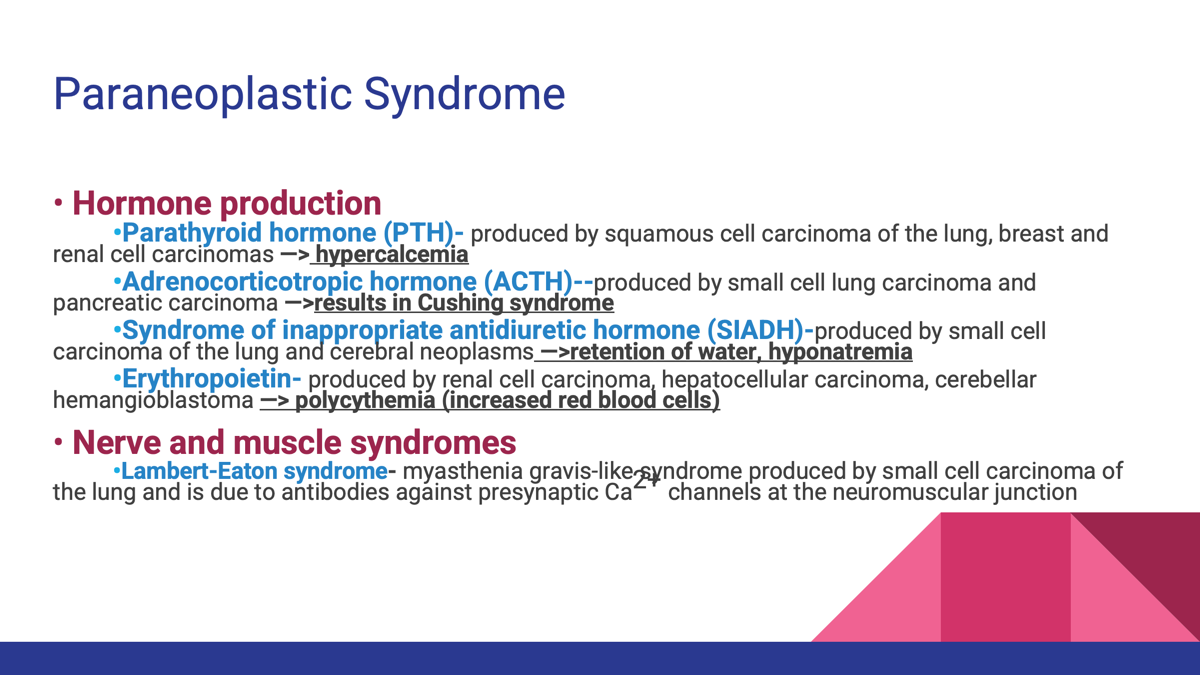
A paraneoplastic syndrome is a symptom or disease caused by a tumor at a distant site, usually through hormone production or immune-mediated mechanisms, rather than by direct tumor invasion.
Caused by hormone secretion or immune responses from the tumor and include:
Cachexia
Hypercalcemia (PTH)
Cushing syndrome (ACTH)
SIADH
Polycythemia (EPO)
Lambert-Eaton syndrome.
Cachexia ("Cancer Wasting")
Loss of body fat and muscle
Weakness
Anorexia (loss of appetite)