Patho Exam 2
1/118
Earn XP
Description and Tags
from written review pages
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
119 Terms
Anemia Definition + most common type
reduction of RBC mass
dec oxygen carrying capacity

Iron Regulation in the body

Location of Iron in the Body
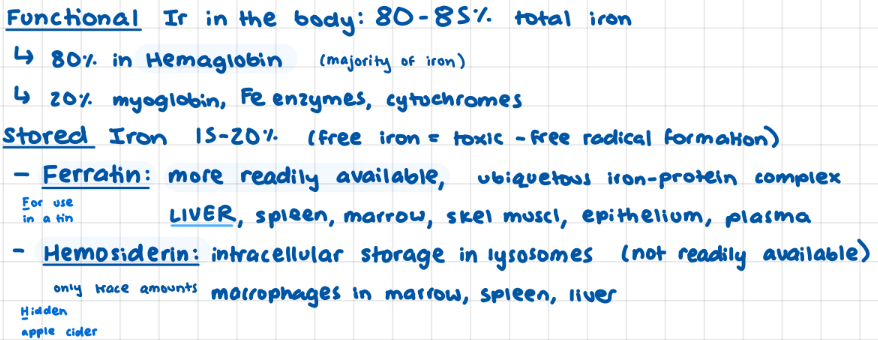
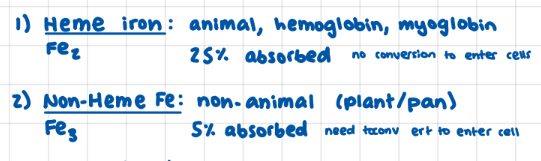
Types of Iron Sources from Diet
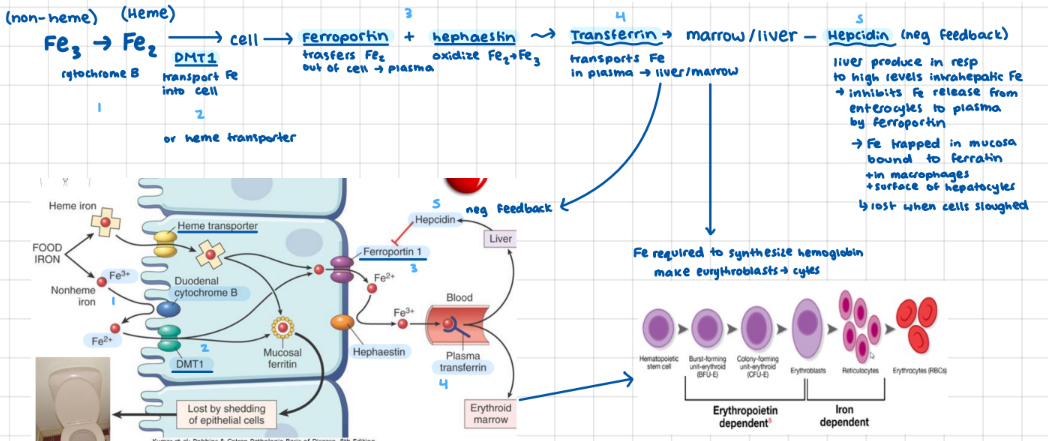
Iron Absorption (+regulation)
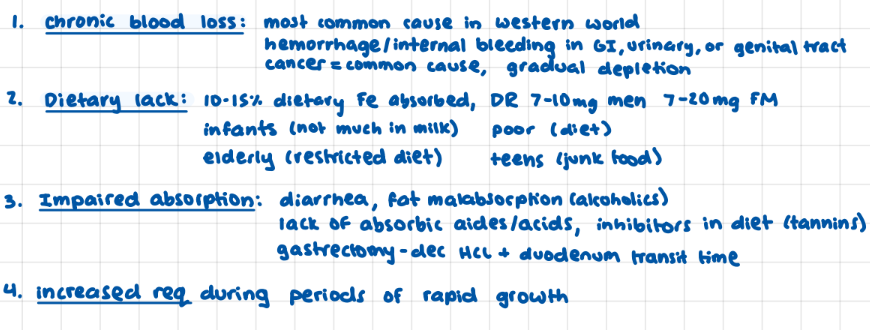
4 main causes of Iron Deficient Anemia
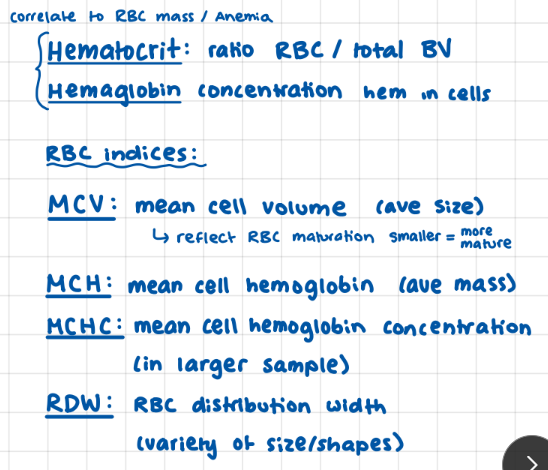
RBC Measurements
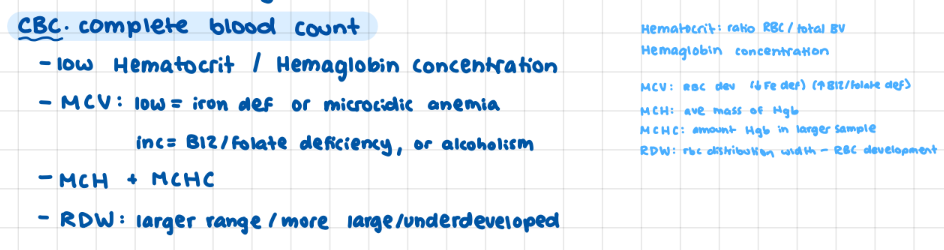
Diagnostic Testing for Anemia
MCV
(low: fe def/microacidic anemia) (high: B12/folate deficiency)
Anemia Characteristics in Peripheral blood smear
small = low MCV

Bone Marrow Biopsy (anemia)
gold standard test, rarely needed, prussian blue stain limited stain bc little Fe in macrophages
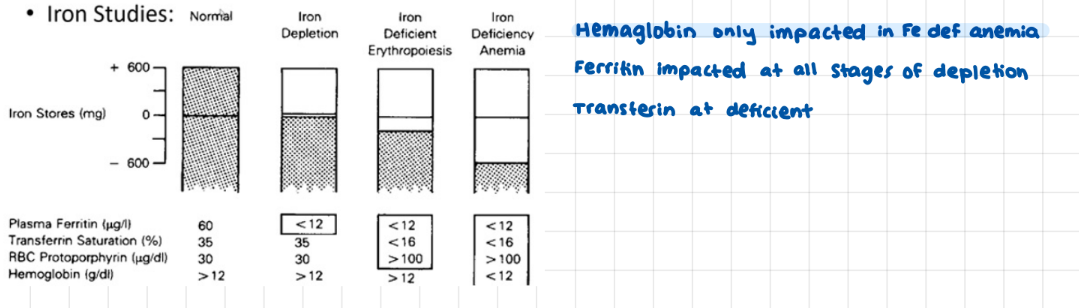
Iron Studies Results comparing what factors appear at what stages of iron deficiency
ferratin, transferin, hemaglobin
(further along match further along steps)
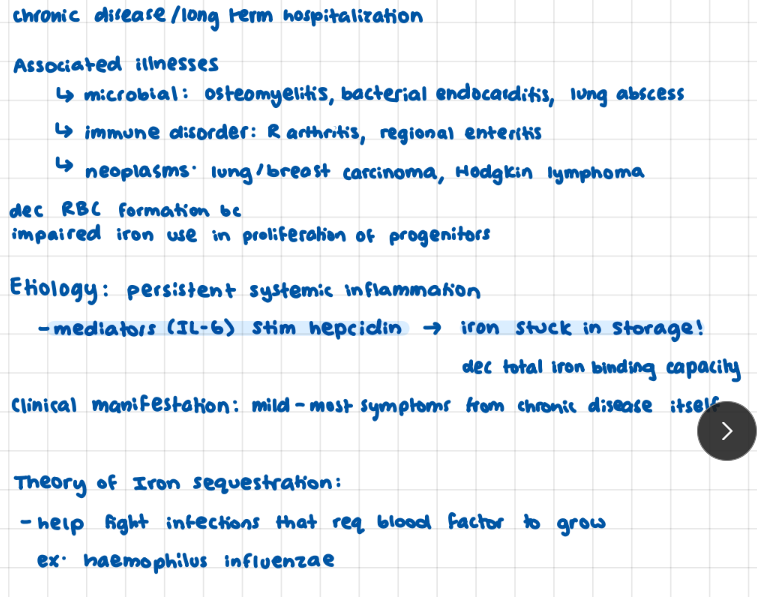
Anemia of Chronic Disease: associated illnesses * (immune)
microbial: osteomyelitis, bacterial endocarditis, lung abscess, immune: R arthritis, regional enteritis, neoplasms: breast/lung, hodgkins lymphoma
Anemia of Chronic disease: associated illnesses
Anemia of Chronic Disease Etiology
IL-6 stip hepcidin → iron sequestration (attached to ferratin on mucosal lining, sloughed off)
Factors that influence Oxygen Economics (Supply vs Demand)

Ischemic Heart Disease (def, struct, funct)
structurally: CAD blcoked plumbing
functionally: reduce O2 carrying capacity: anemia or carboxyhemoglobin (ex from CO2 poisoning)

CAD (what it “is”)
blocked plumbing, leads to 90% of ischemic disease
blocked plumbing limit flow so can’t meet moments of higher demand
cause Angina Pectoris 3 presentations (before Ischemic Heart disease)
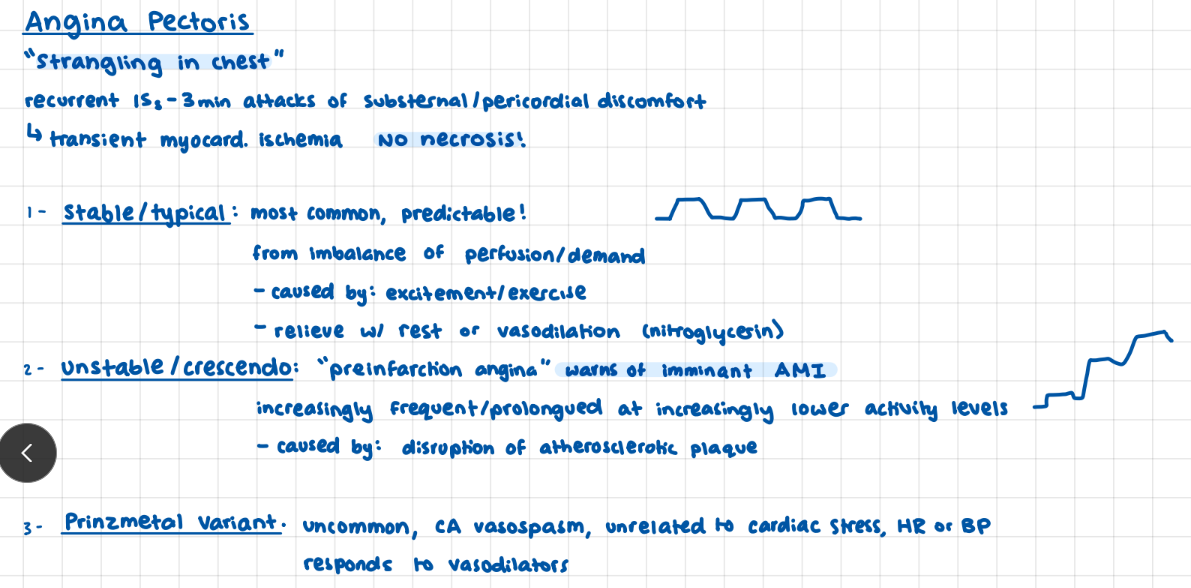
Angina Pectoris (def + discomfort location + necrosis?)
recurrent 15s - 3 min transient ischemic attacks
substernal/pericardial discomfort
no necrosis!
Types of Angina Pectoris (3 types)
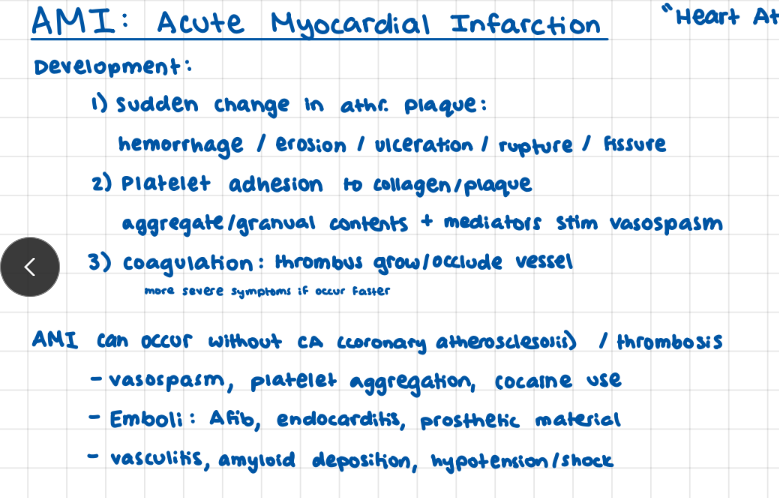
Development of an AMI (acute myocardial infarc)
can occur without coronary atherosclerosis
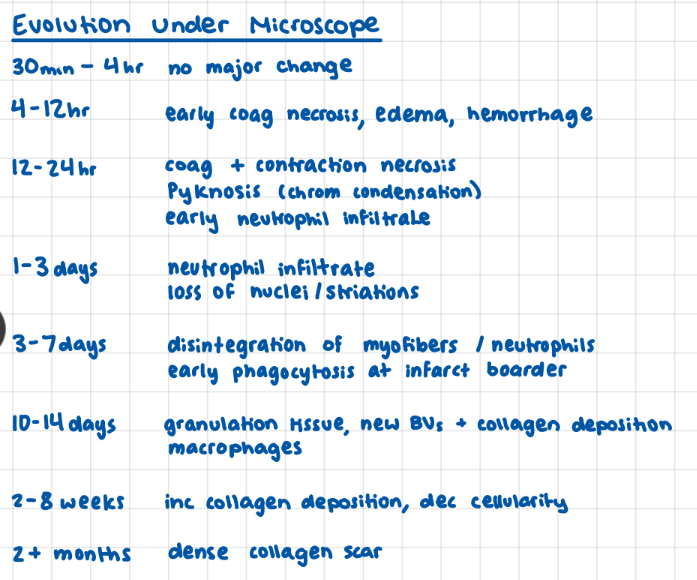
AMI evolution under a microscope*
ami, i hear nothing from you for 4 hours then you tell me you have
coag necrosis, edema, hemorrhage
then on top of that you have both coag and contract nec plus pyknosis?
yeah neutrophils are here but you go on to tell me how now your breaking down and have no nuclei or nuclear striations then on top of that your myofibrils disintegrate
all for you to have granulation tissue, blood vessel, and collagen deposition
for you to inc collagen dep and dec cellularity
all to leave you with a dense collagenous scar?!
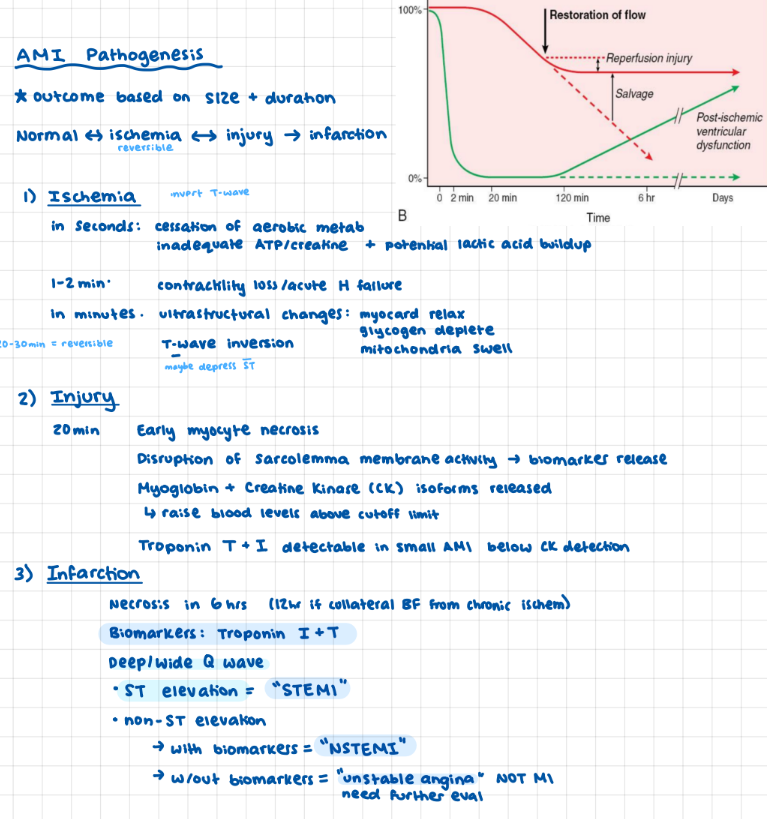
AMI Pathogenesis
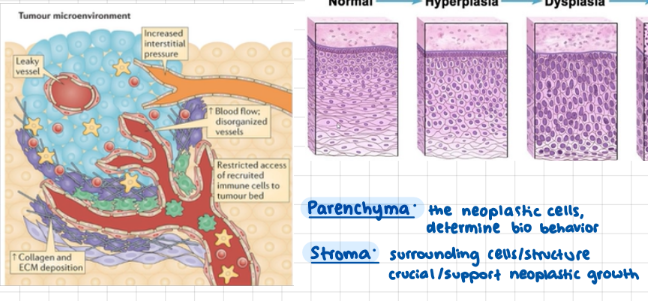
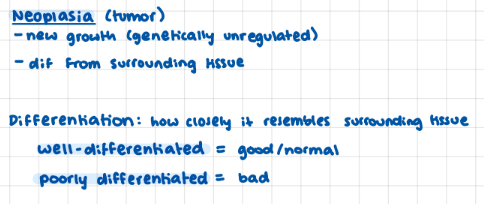
Parts of a Neoplasia
parenchyma + stroma
Neoplasia Differentiation meaning
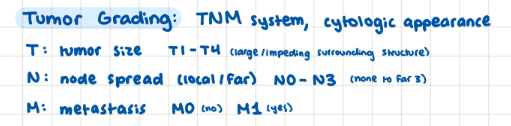
Tumor Grading System
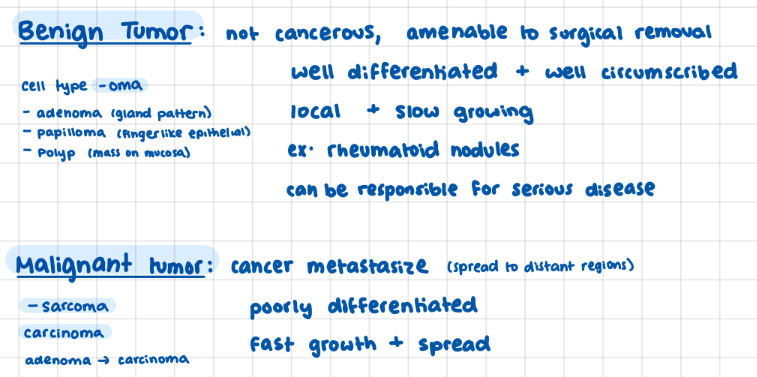
Tumor Nomenclature
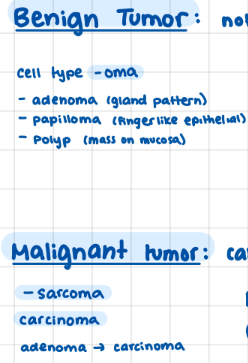
Benign vs Malignant Tumor
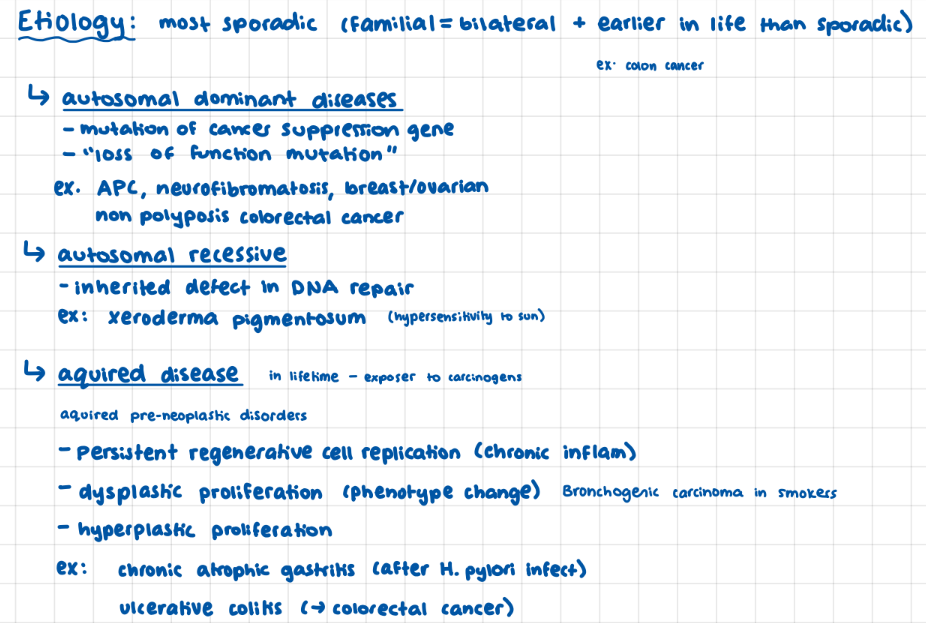
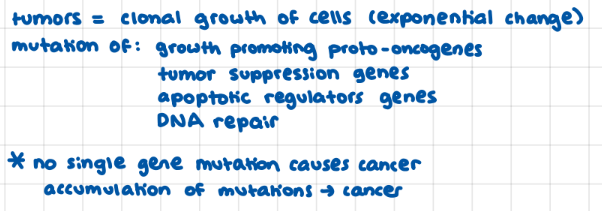
Tumor/Cancer Etiology (genetic types + aquired)
autosomal dom: “loss of funct mutation” cancer suppressor
autosomal recessive: issue with DNA repair
aquired: affect proliferation/regeneration (chronic gastritis/ulceraative coilitits)
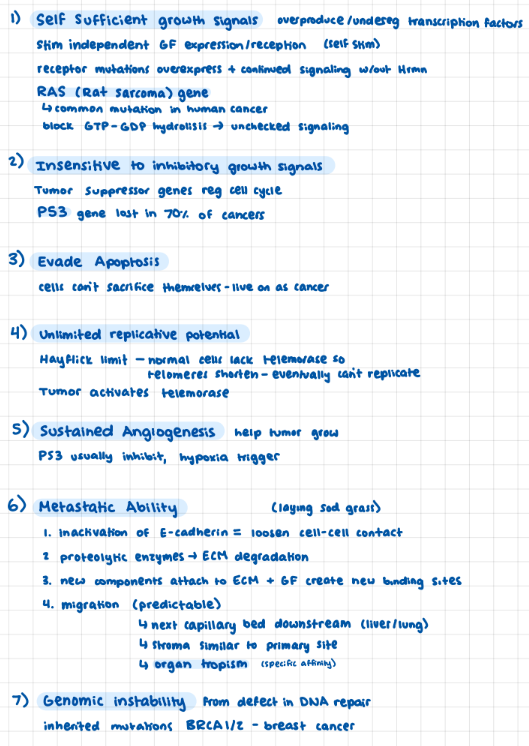
7 Fundamental Changes in Tumors > malignancy
1) self-sufficient growth hormone (RAS- rat sarcoma gene)
2) uninhibited (lack P53 gene)
3) unlimited replicative potential (telomerase)
4) evade apoptosis (don’t sacrifice self)
5) sustained angiogenesis (no P53 to reg)
6) malignant capability
7) genomic instability (DNA mutations)
Carcinogenesis
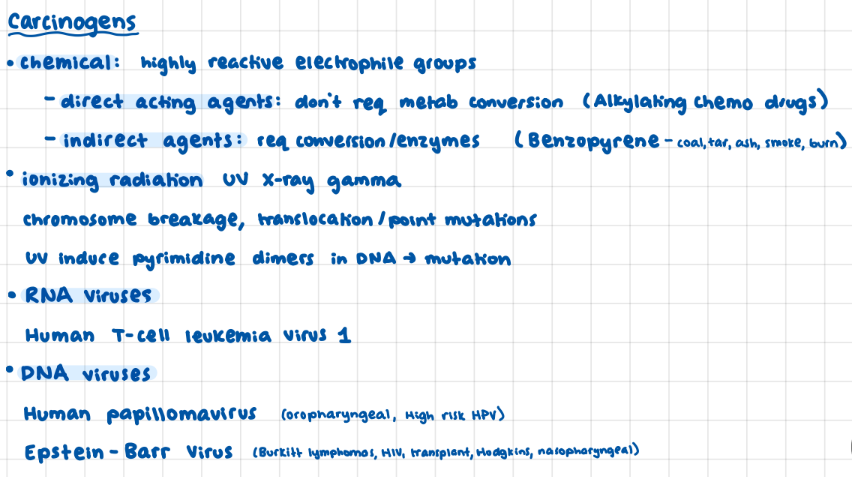
Carcinogens
chemical: direct vs indirect
ionizing radiation
RNA: human T-cell lymphoma
DNA: human papillo + epstein barr
Pathogens (simple definition)
organisms that cause illness for their own survival “survival mode”
Human Microbiom % body comp
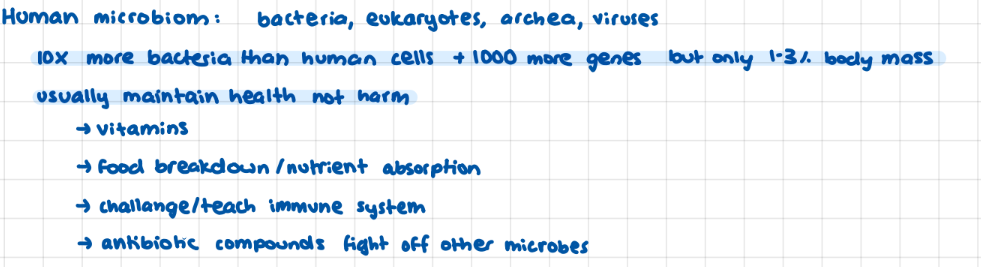
Opportunistic vs Primary/Obligate pathogens
TB, gonorrhea, T palladium, HIV

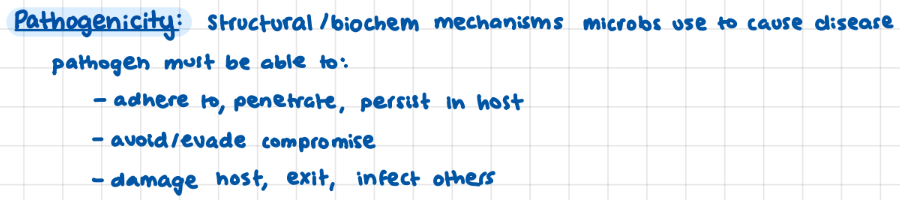
Pathogenicity
structural/biochemical mechanisms microbes use to cause disease
include invasiveness + toxicity
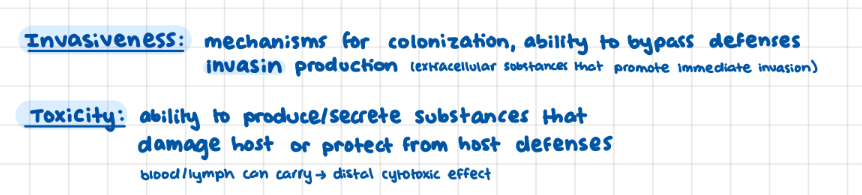
Pathogen Invasiveness + Toxicity
Portal of Entry (Pathogens)
parenteral routes = breaks in barriers

Virulence
pathogens ability to overcome host defenses and establish themselves

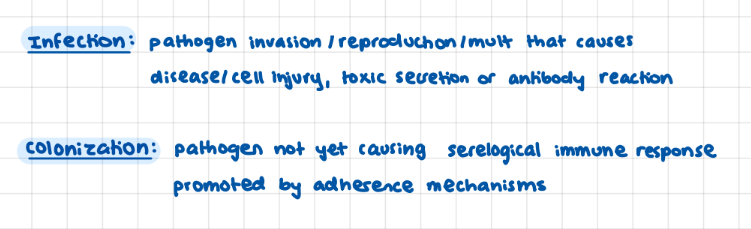
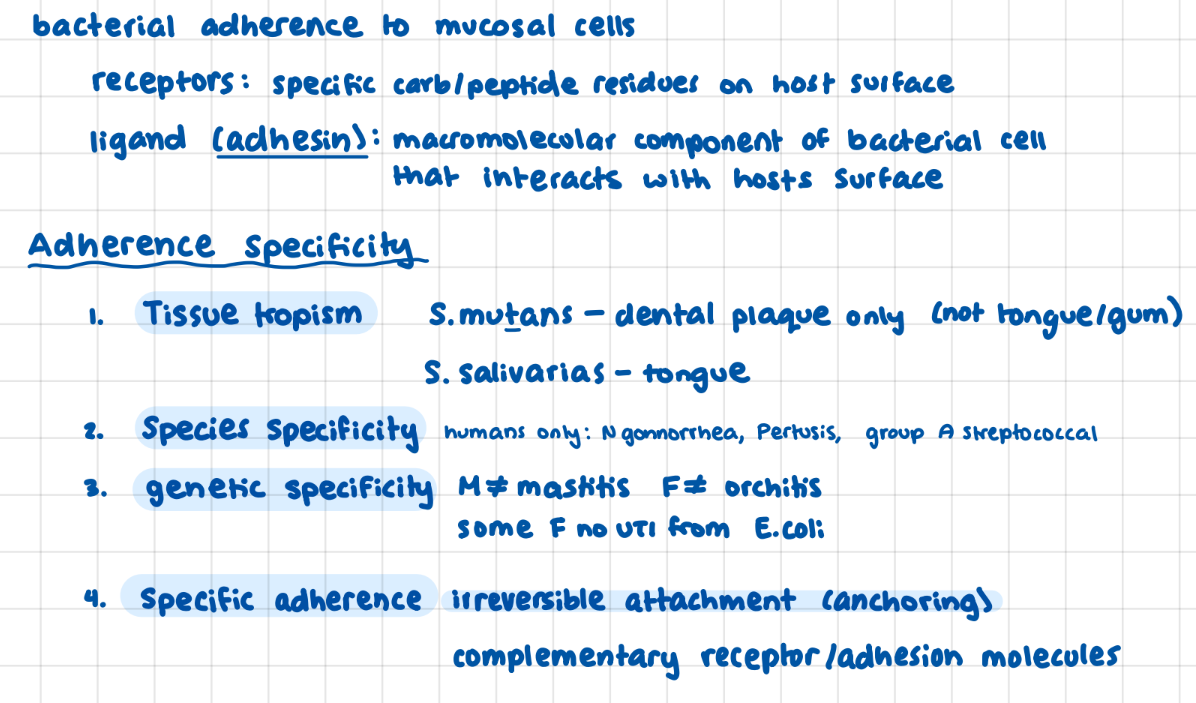
Colonization + Infection
colinization promoted by adherense mechanisms
Pathogen Adherence Specitivity (4 types)
Viruses (Basic Def)
usually can only use specific tissue/animal

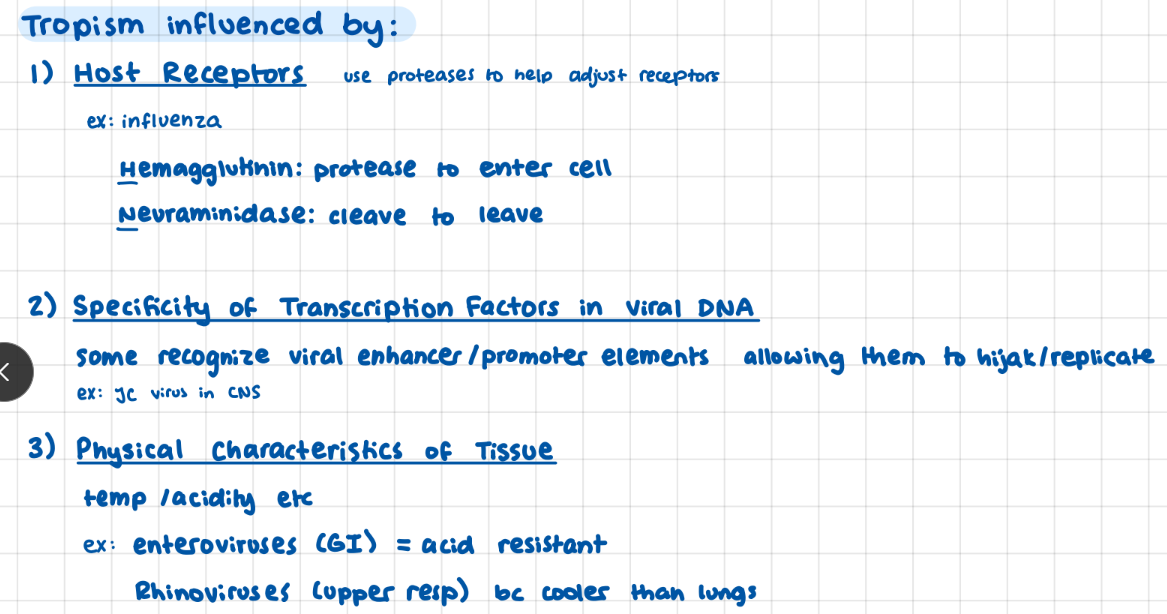
What influences virus tropism? (3)
host receptors
environment
DNA transcription factors
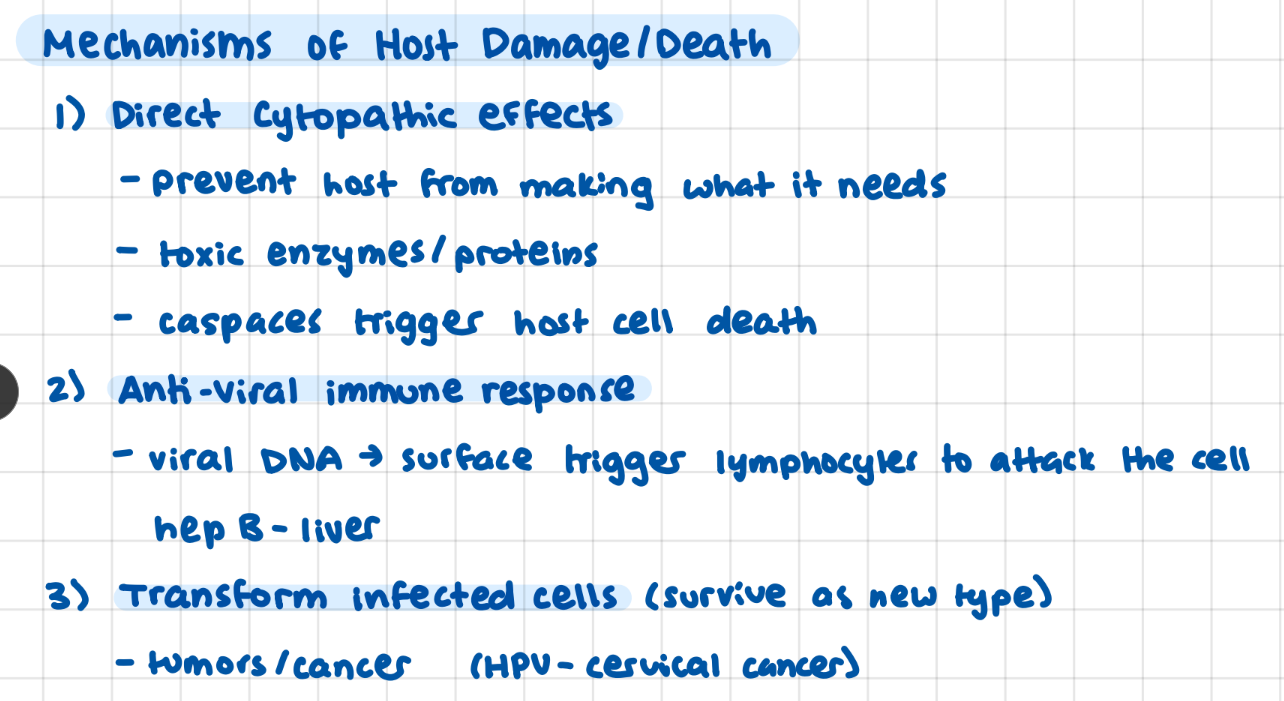
Viral Mechanisms that Damage Host (3)
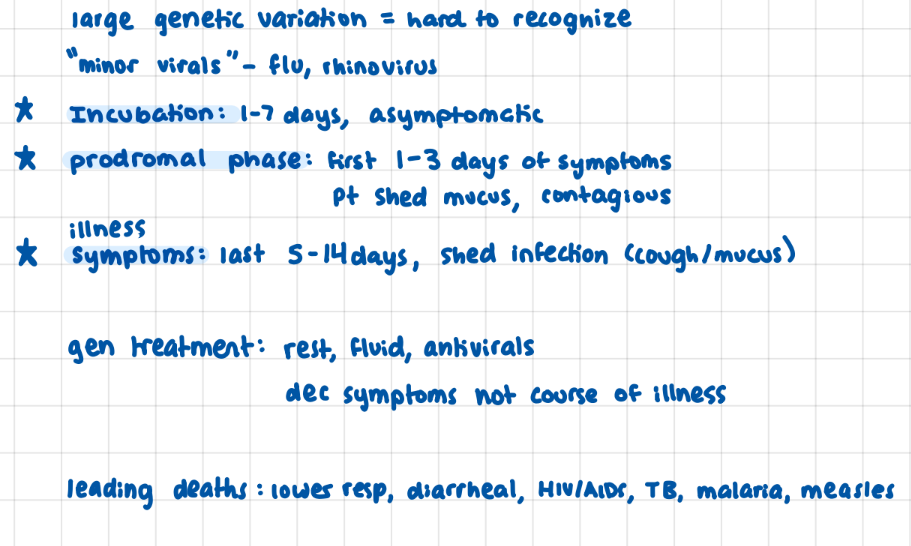
Viral Infection Presentation / Course of Infection
incubation 1-7, prodromal (hard hitting symptoms, mucus, contageous) 1-3 days, symptomatic 5-14 days (shed illness)
COVID 19 Viral entry / transmission
enveloped positive stranded RNA
spike S protein bind to ACE 2 receptors
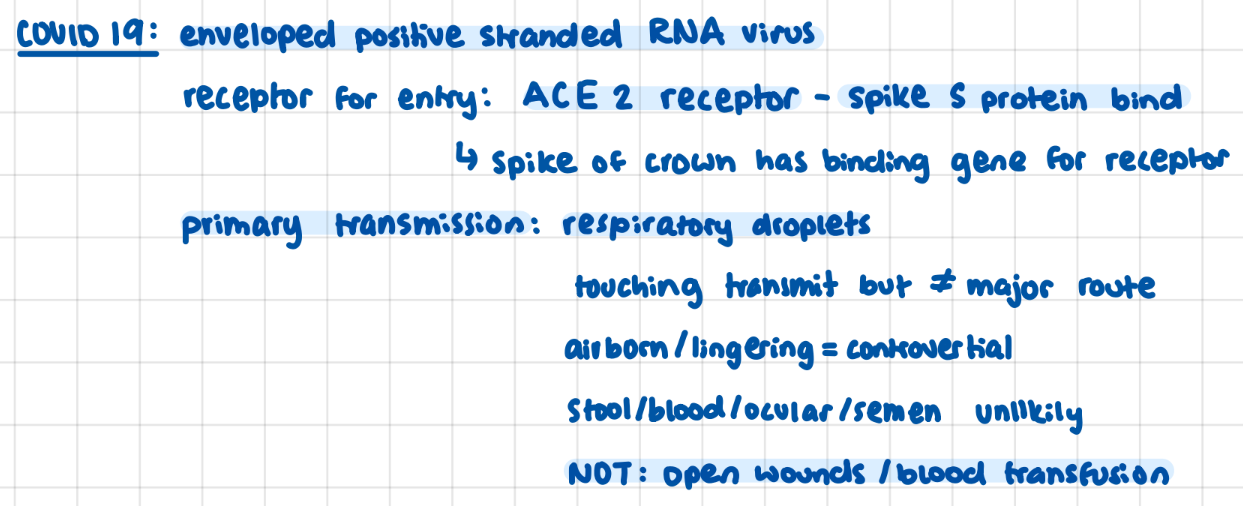
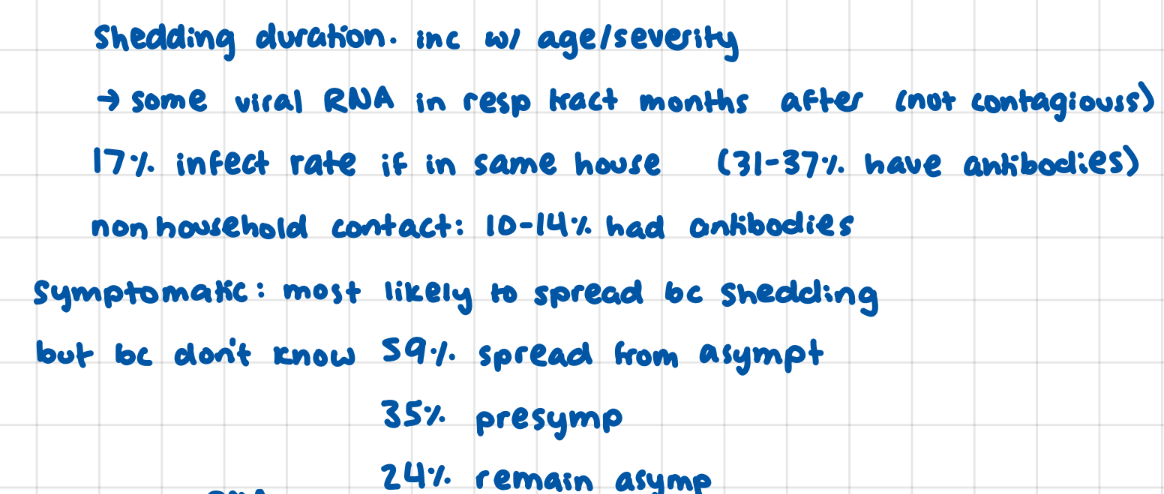
COVID 19 Spread rates
COVID 19 Vaccines: Pfizer vs Johnson & Johnson

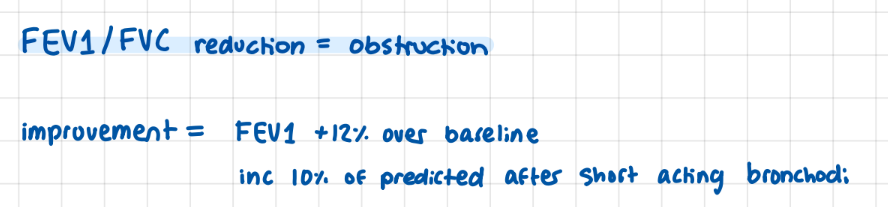
FVC vs FEV1
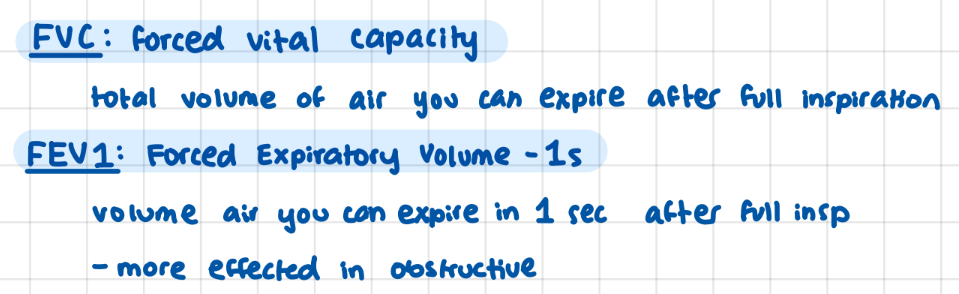
FEV1 / FVC ratio

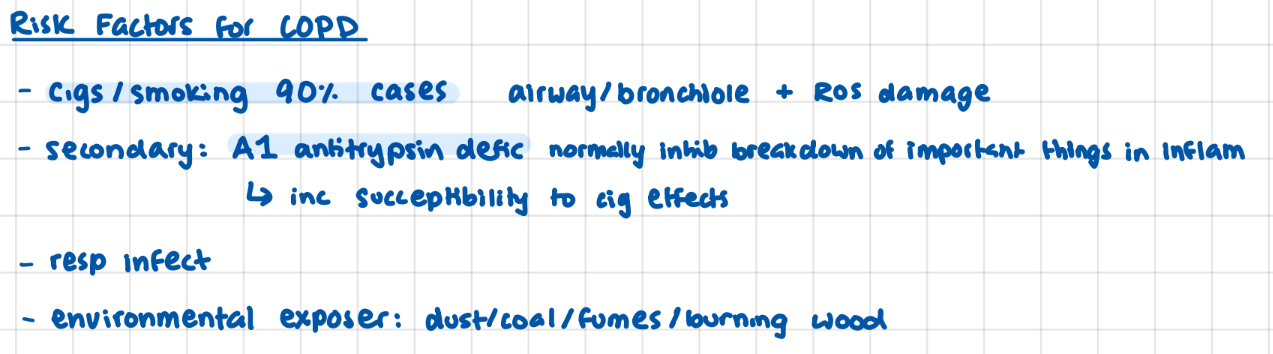
Risk Factors for COPD
smoking (90% cases)
A1 Antitrypsin deficiency (inc susceptibility to effects of cigs)
resp infect + envi exposure
COPD (basic def)
chronic obstructive pulmonary disease
airflow limitation not fully reversible

Name the 3 concurrent factors that appear in COPD
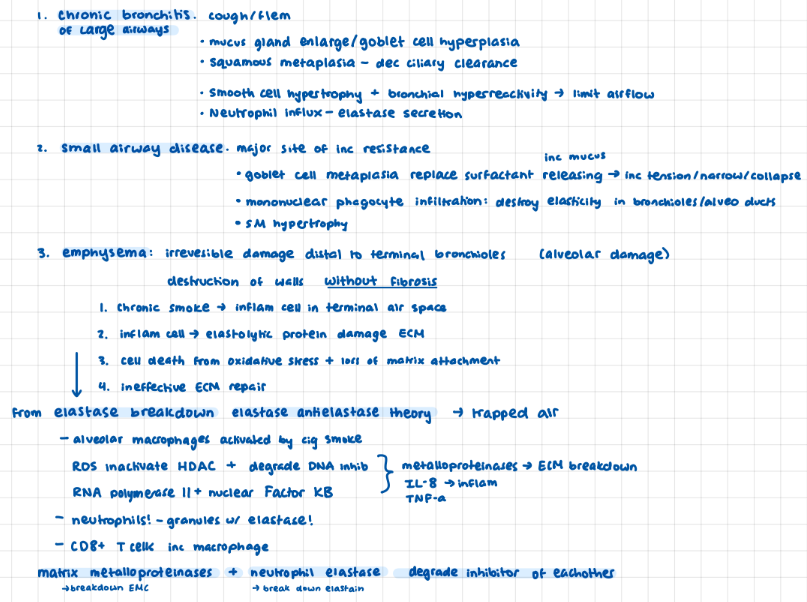
chronic bronchitis of large airways, small airway disease (main site of resistance), emphysema (alveolar damage)
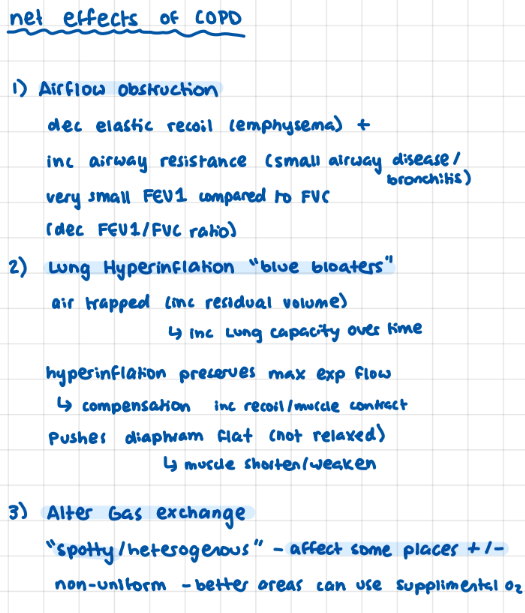
Net Effects of COPD (3)
1) airflow obstruction
2) lung hyperinflation “blue bloaters”
3) altered gas exchange
COPD: chronic bronchitis
Large airways, mucus, smooth cell hypertrophy, bronchial hyperreactivity (dec airflow)

COPD: small airway disease (elast)
bronchioles <2mm, major site of resistance, goblet cell replace surfactant cells, mononuclear phagocytes destroy elasticity, smooth muscle hypertrophy

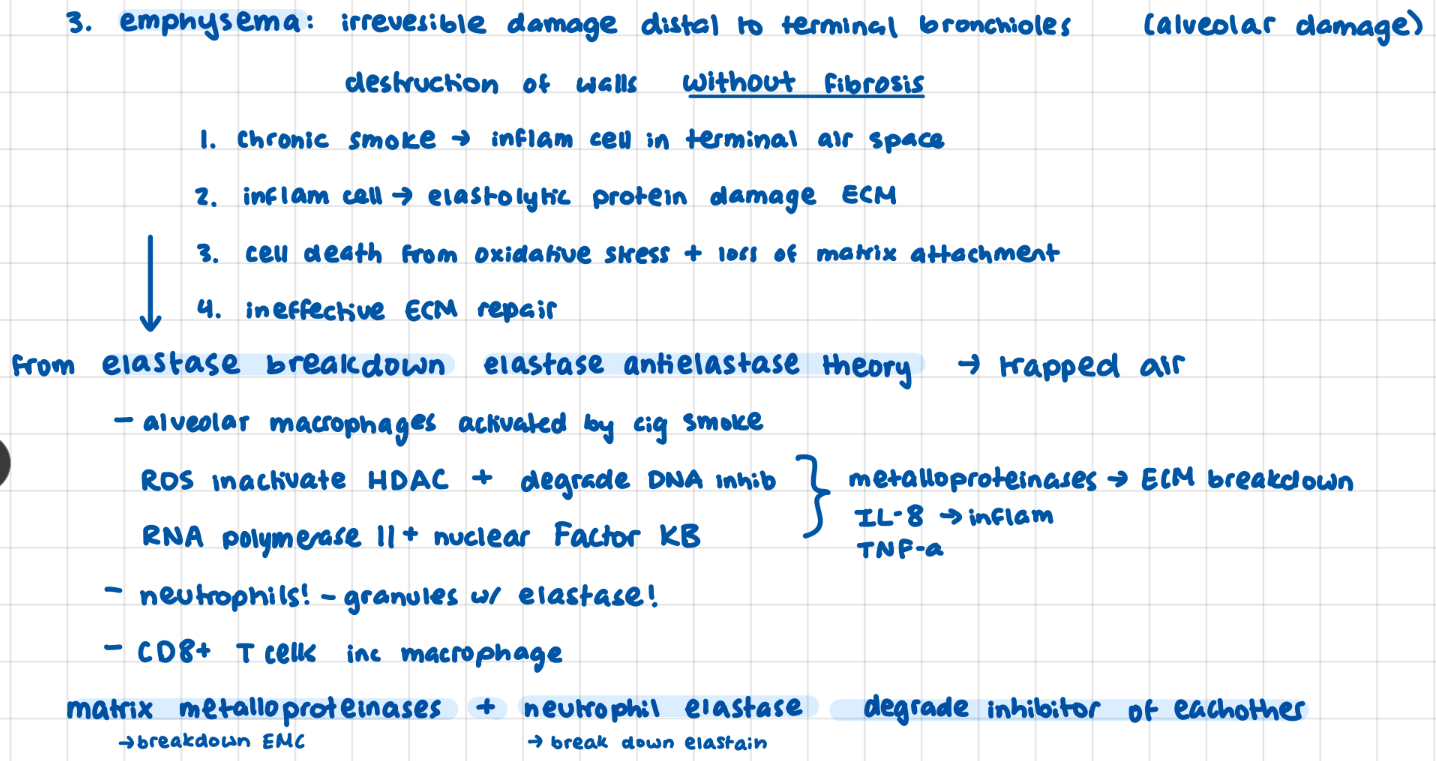
COPD: emphysema*
irreversible alveolar damage without fibrosis
inflammation
neutrophil elastase ← → matrix metalloproteinases ECM
degrade inhibitor of eachother
detectable 9 yrs after last cig
Main Respiratory passages + what keeps them open (3)
trachea: cartilage rings, bronchi: cruved cartilage plates, bronchioles: pressure
Inspiration energy use / types of work
3-5% total energy
compliance (elastic), airway + tissue resistance
Inspiration vs Experation Mechanics
picture it expanding in all directions/shrinking in all directions
Asthma (basic def + phys changes)
chronic inflammatory disorder with reversible obstructive episodes
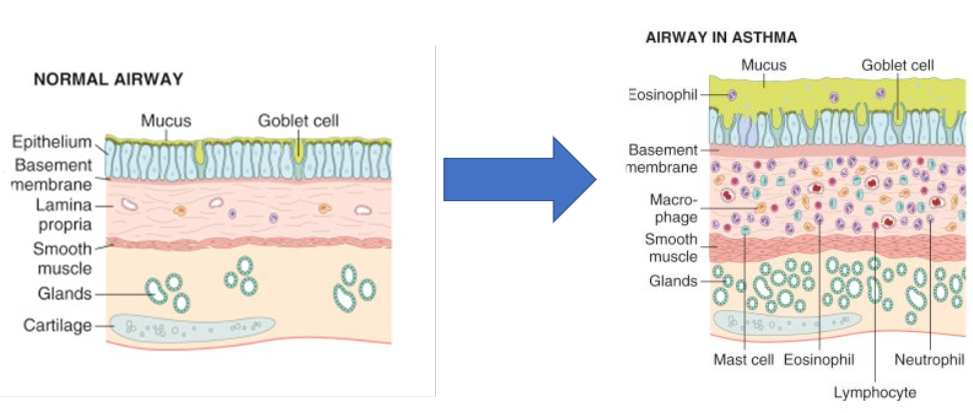
Physiological Changes in Asthma
goblet cells (mucus)
eosinophils/macrophage/mast cells > edema/inflam
smooth muscle hypertrophy
Asthma: symptoms
Asthma: triggers

Asthma: Airflow Resistance
usually airflow resistance at larger bronchioles near bronchi
alveoli / distal bronchioles not effected
during periods of disease state smaller bronchioles effected bc muscle constrict/mucous easier to effect
2 types of Asthmatic Responses
Atopic vs Non-Atopic
atopic: allergen, non-atopic: infection/inhaled pollutant

Asthma: Name 3 cytokines / their effects
T-cell activation + cytokines > inflam resp
IL-4 / 13 : blood based immune resp, IL-13 mucous too, IL-5 eosinophil allergic resp
Asthma: phases (2) early vs late
early phase: acute breathing / bronchiole obstruction (mucous, edema, muscle)
late phase: inflammation (epithelial cell chemokines recruit more mediators)
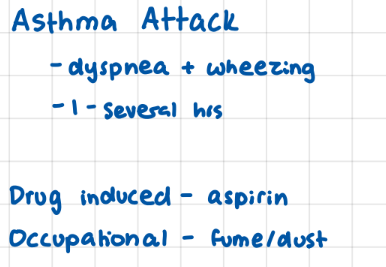
Asthma Attack
dyspnea/wheezing 1-several hours
caused by triggers (exercise, emotion, allergen, weather, viral infect)
aspirin
Asthma: Spirometry
assesses obstruction / reversability
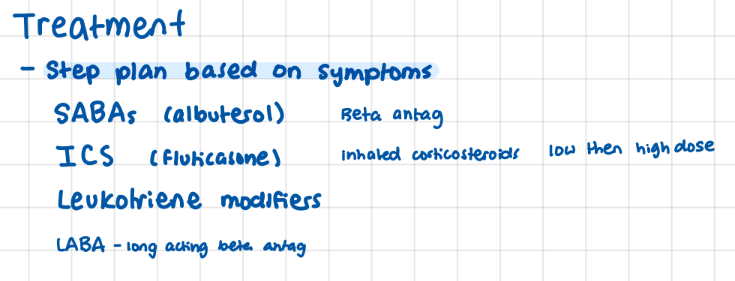
Asthma: treatment
step plan according to symptoms
leukotriene Modifiers
IBS: systems that control GI system
enteric (intrinsic), autonomic (connect enteric to CNS) (symp/parasymp), CNS
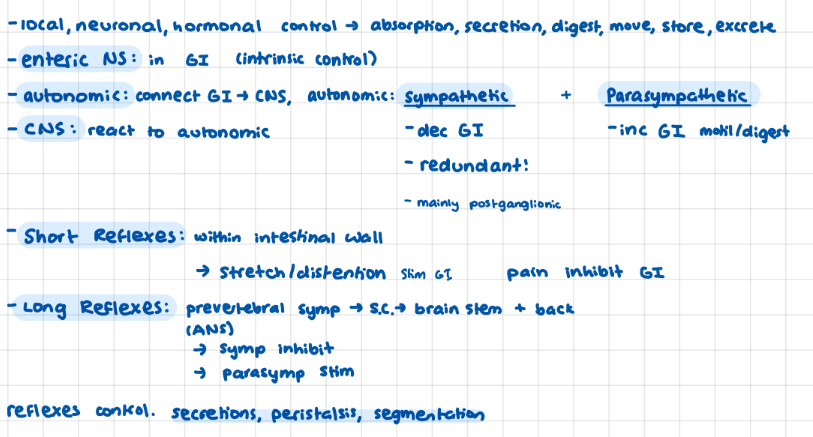
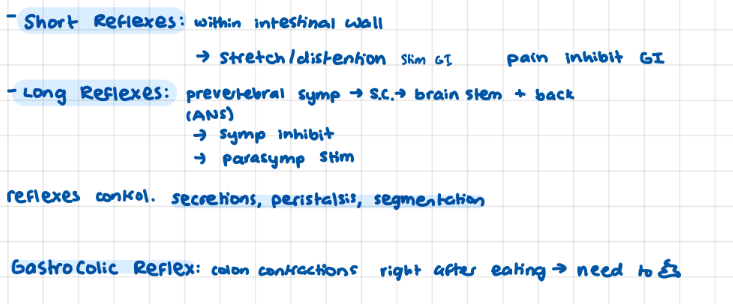
IBS: GI reflexes (+ what they control)
short: enteric, long: ANS
control: secretions, peristalsis, segmentation
IBS (basic def)
chronic, continuous, or remittent
bowel disturbance + abdominal pain

Rome IV criteria
used to diagnose IBS
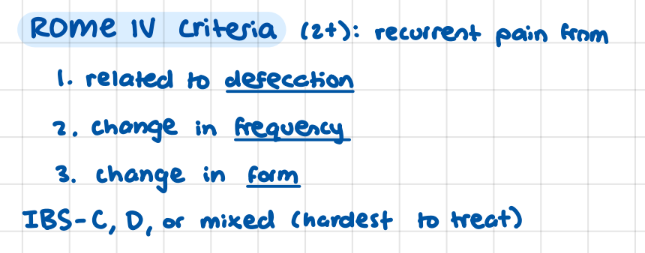
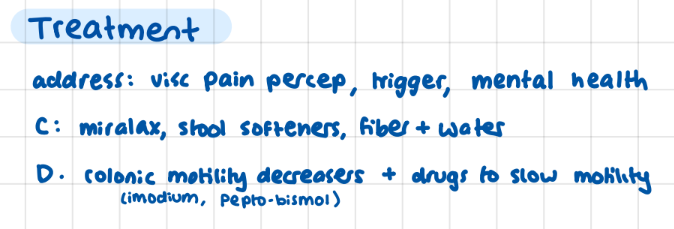
IBS: treatment (C vs D)
IBS: list the 5 components of IBS pathology
altered visceral (pain) perception, abnormal motility, abnormal secretion, triggers (bacterial growth), ANS dysfunction
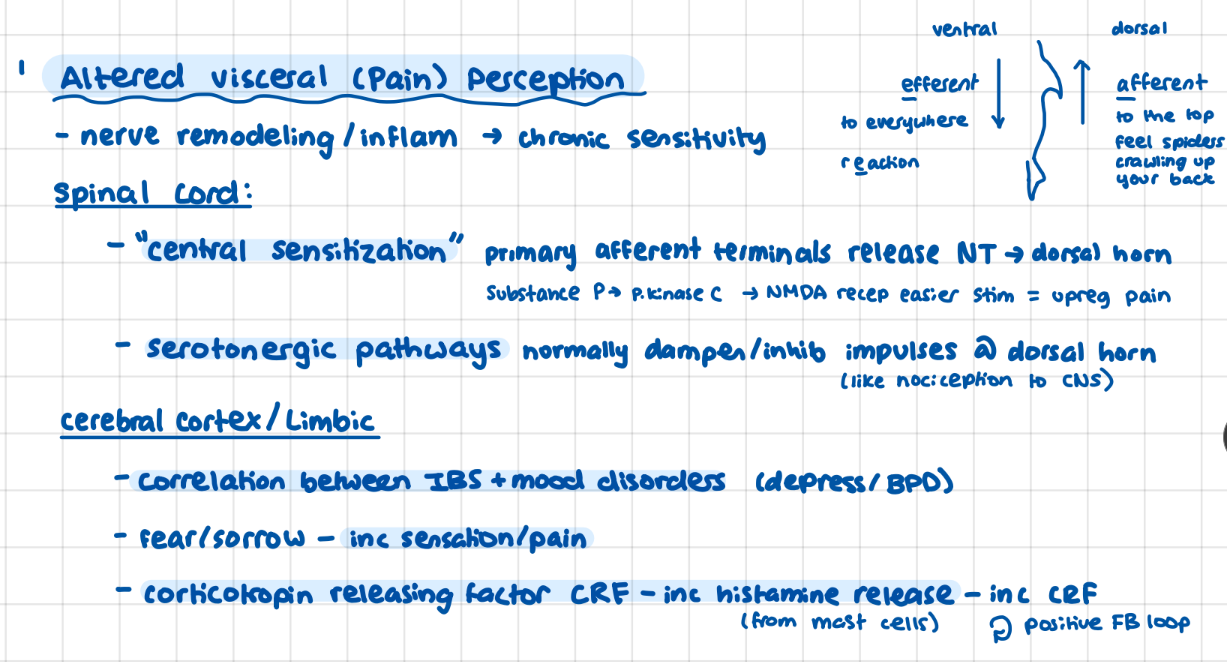
IBS: altered visceral perception
[limbic system positive feedback loop]
spinal cord: central desensitization, serotonergic pathways
Limbic system: correlation with mood disorder + fear/sorrow inc pain, corticotropin > histamine > CRF positive feedback loop
aaaaaa spiders crawling up your back (afferent)
IBS: altered motility
small bowel dysmotility (transit times), colon dysmotility (varietion in slow wave freq, more common in IBS-D)
IBS: altered secretions (what cells do what)
secretory, goblet, crypt/pits lieberkuhn, tubular, complex glands
secretory: digestive enzymes, goblet: mucous, crypt/lieberkuhn: specialized secretory, tubular: acid/pepsinogen, complex glands: salivary/pancreatic
IBS: triggers
65-84% IBS pt have bacterial overgrowth of small intestine
post-gastroenteritis
food intolerances (lactose, sorbitol, fructose)
psychological
IBS: ANS dysfunction
main characteristic of IBS, C: inc sympathetic + vagal tone, D: inc parasymp
Kidney: (% use of body blood + oxygen) + (bloodflow)
25% Cardiac output
10% oxygen
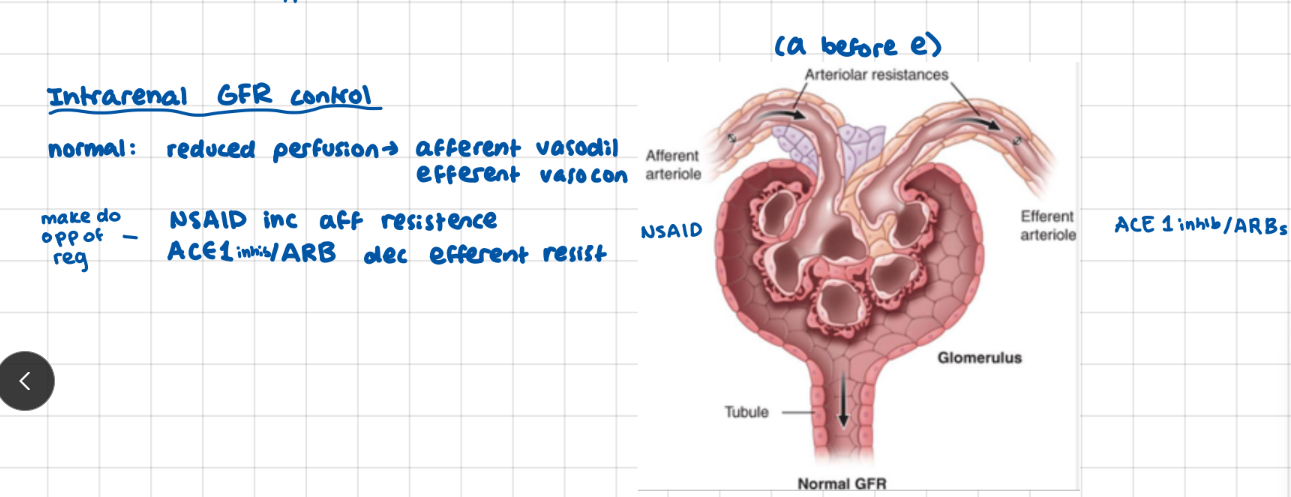
Kidneys: GRF control
afferent arterioles -> glomeral capillaries -> efferent arterioles
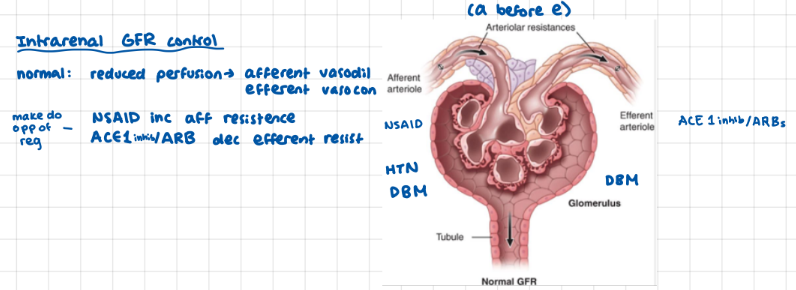
How do NSAIDs and ACE 1 inhibitors / ARBs effect GFR?
Acute Kidney Injury (Basic def)
abrupt 48 hr decline in kidney function
→ accumulation of waste products
usually reversible
3 Indicators of Acute Kidney Injury (AKI)
inc serum Creatine (retained waste), oliguria (dec urine output), Azotemia (nitrogen in blood- BUN)

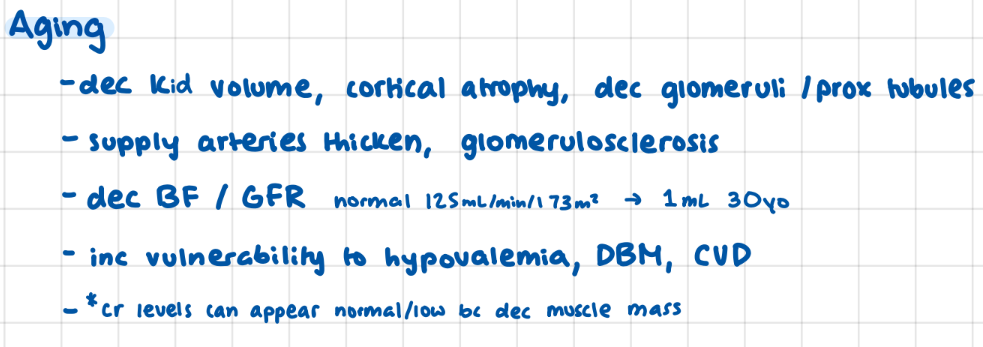
Risk factors for AKI
factors associated with aging: dec kidney volume (atrophy), arterial thickening, dec BF / GFR
*Cr levels can appear low/normal bc dec muscle mass
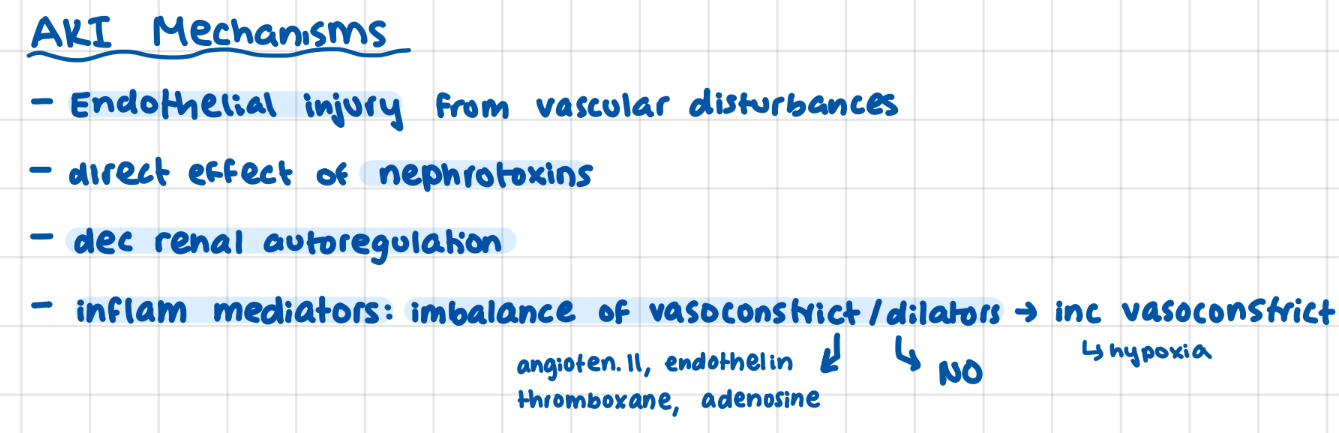
4 mechanisms that contribute to AKI
endi
endothelial injury (from vascular disturbances)
nephrotoxins
dec autoregulation
inflammatory mediators (imbalance → inc vasoconstriction)
List the 3 categories of AKI
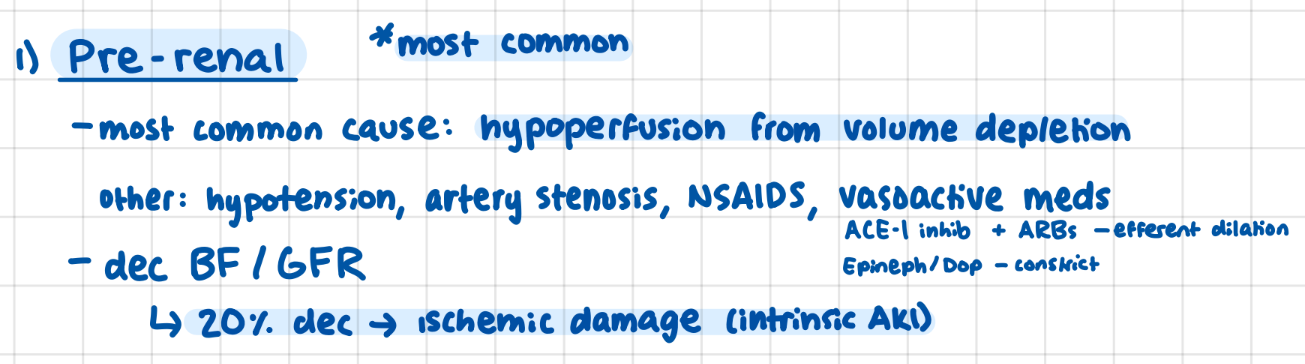
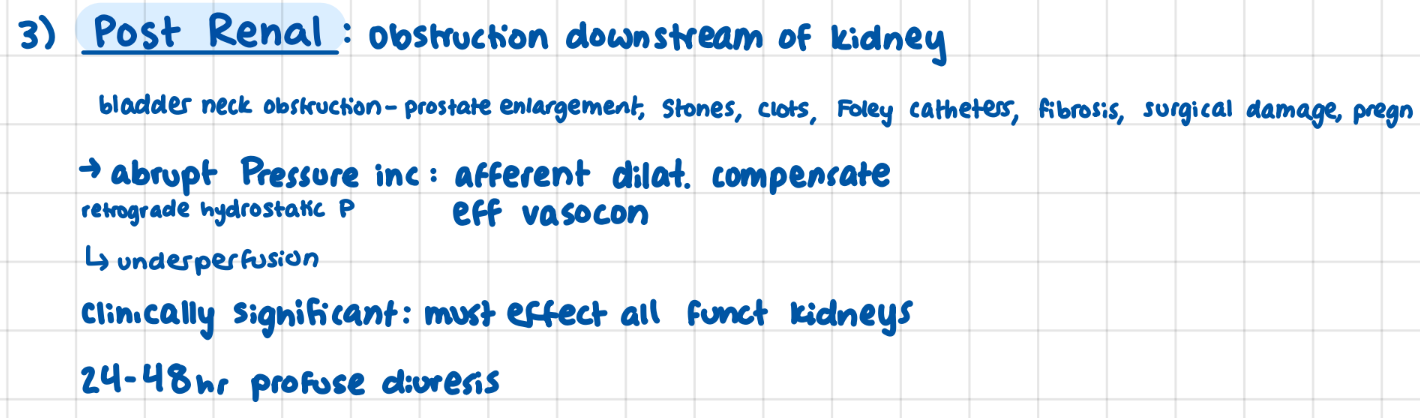
Pre-renal (most common), Intrinsic (acute tubular necrosis, acute interstitial nephritis, contrast induced nephropathy), Post-renal (downsteam blockage)
Pre-renal AKI
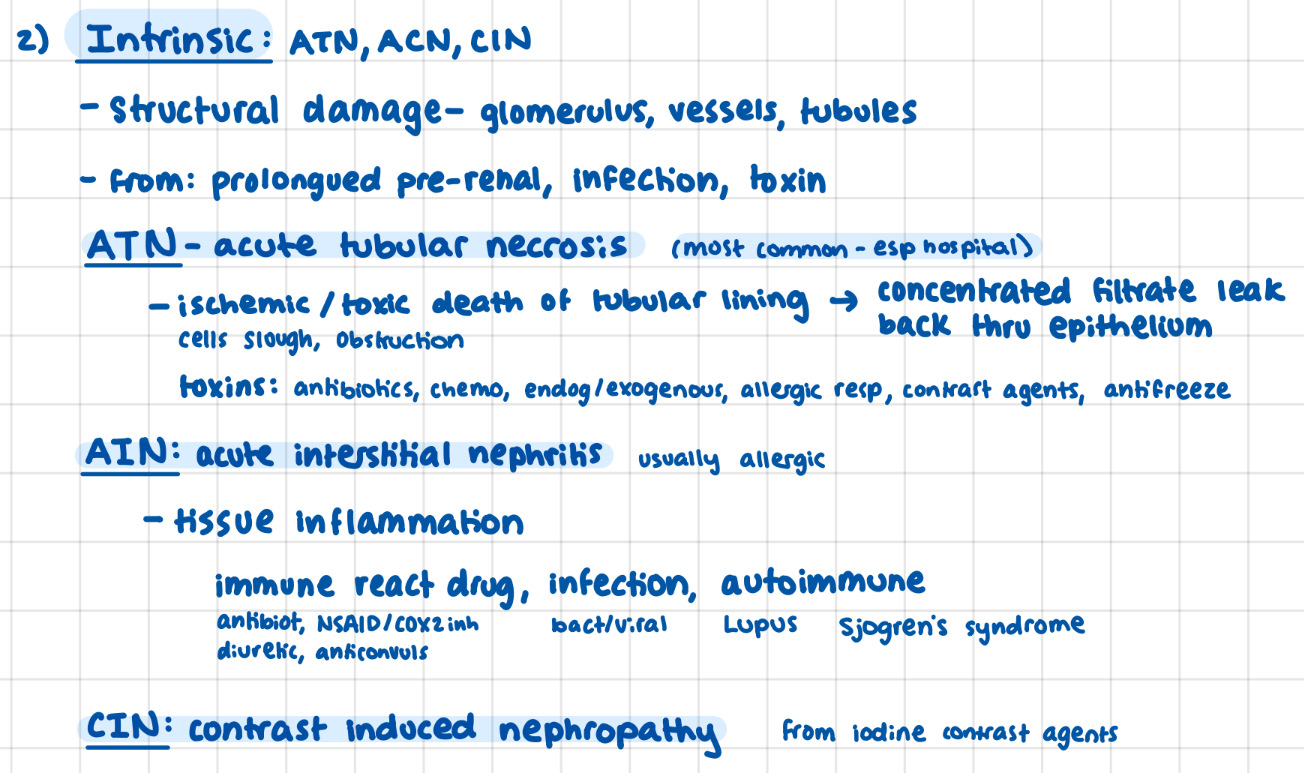
Intrinsic AKI
structural damage to nephron
Acute tubular necrosis (ischemic/toxic death)
Acute Interstitial nephritis (inflam- allergic resp)
Contrast induced nephropathy
Post-renal AKI
abrupt BP inc
afferent dilate to compensate > underperfusion
efferent change to avoide damage
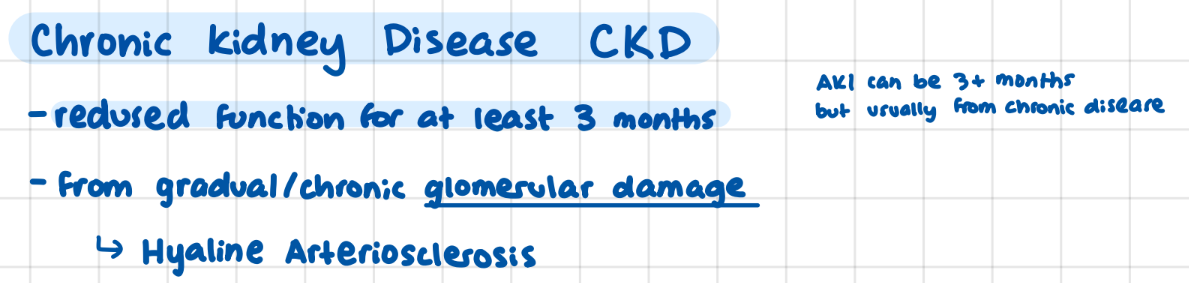
Chronic Kidney Disease (Basic def)
reduced function for 3 months
gradual/chronic glomerular damage
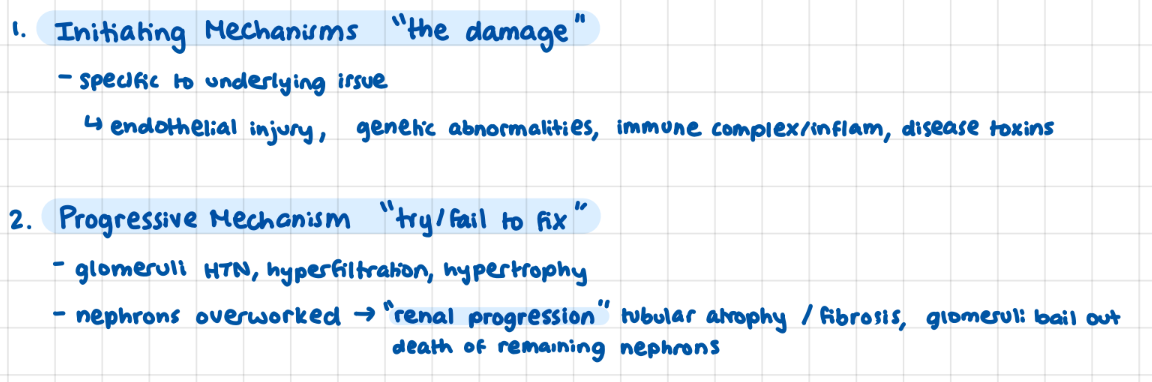
CKD steps (2) (+ term for turning point)
1) initiating mechanisms/damages, 2) progressive mechanism: trying/failing to fix (overwork/bail out)
little lady: “so how do we want to progress from here”
*renal progression: point at which remaining nephrons begin to die
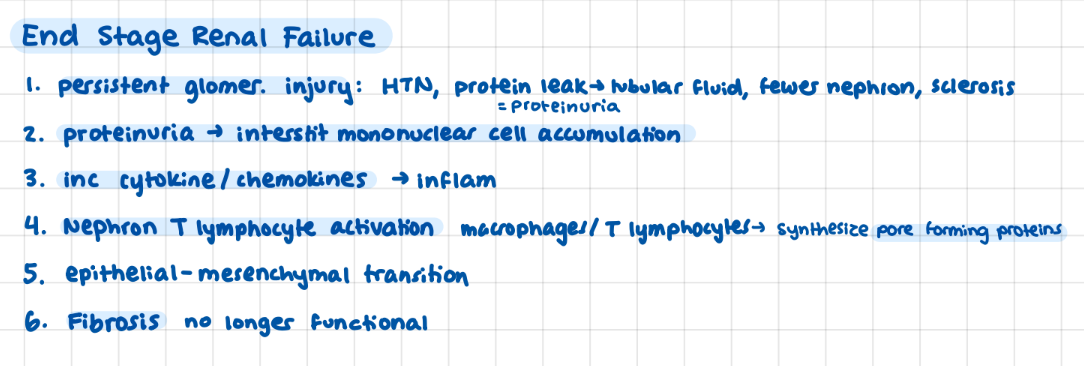
Steps in End Stage Renal Failure *
persistent injury → HTN, Proteinuria, Sclerosis
proteinuria → mononuclear cell + cytochemokines → inflam
T lymphocyle activation → Synth pore forming proteins
mesenchymal transition → Fibrosis not functional
2 categories of Cerebrovascular Disease
ischemic: impaired BF/oxygenetation
hemorrhagic: BV rupture (aneurysm)
5th leading cause of death in US
cerebrovascular disease
3 Basic Processes / Ways Cerebrovascular Disease Occurs
1) thrombotic occlussion (blood clot)
2) emboolic occlusion (piece of clot)
3) vascular rupture (aneurysm)
Brain function: what is the limiting substance?
Oxygen
Cerebral bloodflow: consistency / control
remains constant over dif BP and intracranial pressure bc
autoregulation + vascular resistance