Human Physiology Midterm #2
1/119
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
120 Terms
Lecture 11
11
spinal cord
composed of inner core of gray matter & outer core of white matter
surrounded by vertebral column
part of CNS
ends at L2 vertebra
nerves extend from cervical → thoracic → lumbar → sacral → coccygeal, total of THIRTY-ONE pairs
cauda equina
area after L2 where spinal cord has ended
myelinated axons
where spinal tap happens
(sacral + coccygeal + lower lumbar nerves)
dorsal & ventral horn
made from gray matter on inside of spinal cord
looks like an H, dorsal horn is top half of H facing back
dorsal→ sensory neurons
ventral→ motor neurons
ascending & descending bundles
ascending are myelinated axons that carry info to brain
desceding are myelinated axons that carry commands to motor neurons
afferent fibers
start in periphery and end in dorsal horn
located in dorsal root ganglia → has cell bodies of afferent neurons
dorsal roots→ afferent limb of each spinal nerve, found in vertebral canal
efferent neurons
carries motor information
cell bodies are in spinal cord
spinal nerves are <1cm
formed by dorsal and ventral roots from same level combining
PNS organization
PNS: autonomic(involuntary) neurons & somatic(voluntary) neurons
autonomic→ sympathetic (excite(fight or flight)) & parasympathetic (rest(and digest))
PNS function
transmits signals btw CNS and effectors throughout the body
autonomic neruons→ control glands and muscles of internal organs
somatic motor neurons→ control skeletal muscles
somatic motor neurons (innervates skeletal muscle)
cell bodies are in brainstem or ventral horn
leaves CNS and pass to skeletal muscles WITHOUT any synapses
release ACh (acetylcholine)
only contracts when excited, no inhibition of skeletal muscles
autonomic neurons (innervates heart, smooth muscle, glands, GI)
made of 2 neurons connecting CNS and effector cells → 1 inside CNS & other is autonomic ganglion
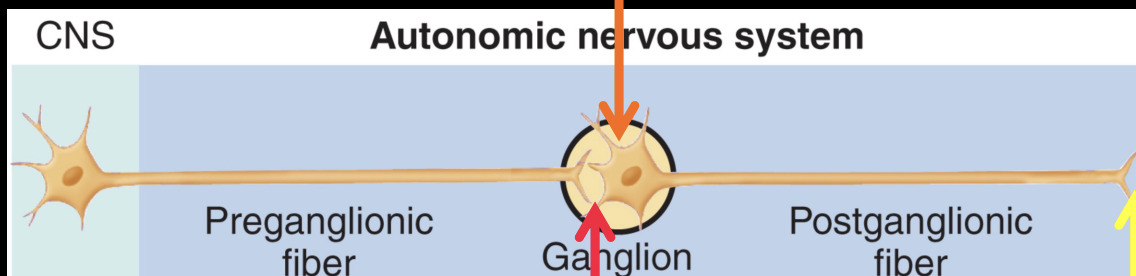
pre & postganglionic neurons release ACh (NT released btw postganglionic neuron and target is diff btw sympathetic & parasympathetic division)
can be inhibitory or excitatory
divided into sympathetic & parasympathetic
dual innervation
parasympathetic & sympathetic parts of autonomic NS innervate almost every organ
sympathetic: fight or flight (↑HR, ↑blood flow, ↑lungs)
parasympathetic: rest & digest (↑digestion, ↑secretions, ↑liver/kidneys/bladder, ↑sex)
sympathetic & parasympathetic leaving CNS
sym: leaves from 2ndL & 1stT regions, ganglia are close to spinal cord and make sympathetic trunks/chain (has postganglionic cell bodies) (looks beaded)
parasym: leaves from brainstem & sacral areas, ganglia lie inside or v v close to organs that it innervates
vagus nerve: originates in medulla oblongata and carries 75% of all Psym fibers
adrenal medulla
is a modified sympathetic ganglion
chromaffin cells release catecholamines (80% epinephrine, 20% norepinephrine) for fight or flight
epinephrine/norepinephrine
this NT is released btw sympathetic postganglionic neurons & effectors
receptors in PNS
ACh receptors present and are effected by agonists(trigger pathway) & antagonists(don’t trigger pathway)
nicotinic ACh receptor → responds to nicotine & ACh
muscarinc ACh receptors (M-AChR) → responds to muscarine (mushroom) & ACh, in autonomic NS
atropine is an antagonists of M-AChR
Adrenergic receptors also present
activated by epinephrine & norepinephrine
cells charge
intracellular:
slightly negative
K+ is major cation
Po- is major anion
extracellular:
slightly positive
Na+ is major cation
Cl- is major anion
law of conservation
net amount of electrical charge must be zero
also note that separating + & - charges takes energy
material charges move thru is a conductor (water), separated charges can’t move through insulator (CM)
cell membrane
enables separation of electrical charge in body, not permeable to ions
to create a membrane potential difference → use active transporter to move ions against conc gradient → creates an electrical gradient (diff in net charge btw inside and outside) & concentration gradient (more ± outside compared to inside) → electrochemical gradient
electrical gradient btw extracellular fluid and intracellular fluid → resting membrane potential
relative electrical gradients
relative scale measures difference in charge using a voltmeter → used for living systems
absolute scale means counting # of ions on either side of plasma membrane
voltmeter: uses 2 electrodes filled with conductor to measure electrical difference btw
RECORDING electrode goes from CM into cytoplasm & REFERENCE electrode is placed in external bath → recorder usually reports resting potential of -40 to -90mv
K+ leak channels
in CM, allows K+ to leak out of cell moving down conc gradient → creates a negative charge inside cell → electrical gradient
opp charges attract so K+ is being pulled back inside by negative ions → eventually driving force of K into cell = chemical conc gradient driving K out → net movement of K stops
resting membrane potential is mostly due to movement of K+ out of cell down its conc gradient (makes inside cell more neg) BUT small # of Na+ channels are open in resting state so some Na+ move into cell
equillibrium potential (Eion)
uses Nernst equation to calculate: Eion(x) (equilibrium potential for ion) , when cell is permeable to only 1 ion(x)
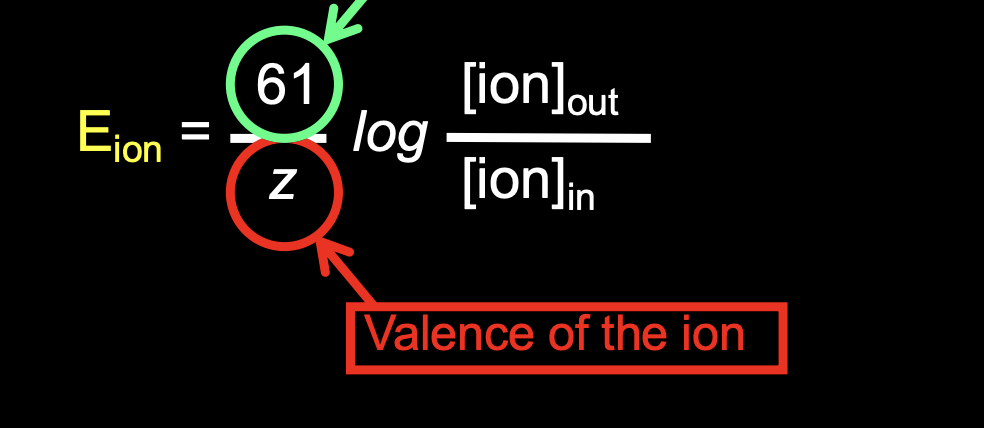
61 is Faraday’s constant
concentration gradient
the greater the membrane permeability to an ion the greater the contribution that ion species will make to the membrane potential
GHK equation
calculates relative membrane permeabilities for Na+, K+, Cl-
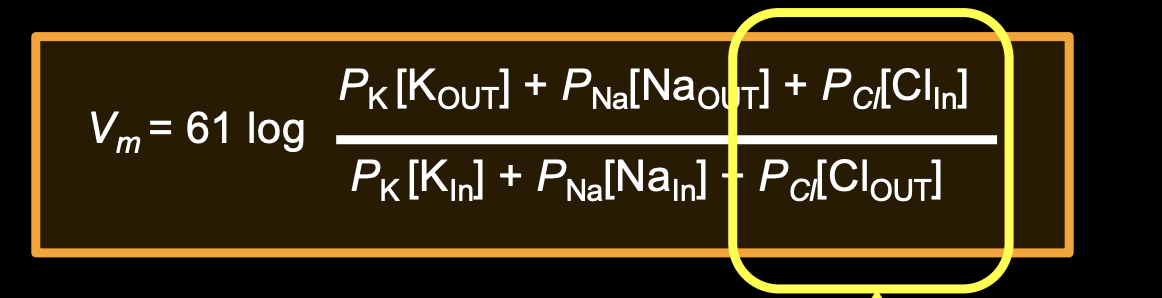
(Cl is reversed because its an anion)
usually around -70mV
Na/K ATPase pump
maintains Na & K concentrations
pumps 3 Na+ out for every 2 K+ pumped in → makes cell inside more negative and creates small electrical gradient which maintains conc gradient
2 types of changes in membrane potential
graded & action potentials
graded potential
transient changes in membrane potential that occur in dendrites or cell body, confined to small area of CM
charge flows from place of origin to adjacent regions, after depolarization by chemical signal → opens cation channels → makes a less negative potential in that area → + charges in cell flow away from depolarized region and move towards more negative membrane areas → outside cell + charges flow from positive membrane towards less positive regions
charge is lost across membrane thru membrane permeability/leakage
summation
when additional stimuli occurs before graded potential has died away
will be added to depolarization from first
action potentials
changes in membrane potential starting in trigger zone and propagated down axon
polarized
outside and inside of cell have a diff net charge
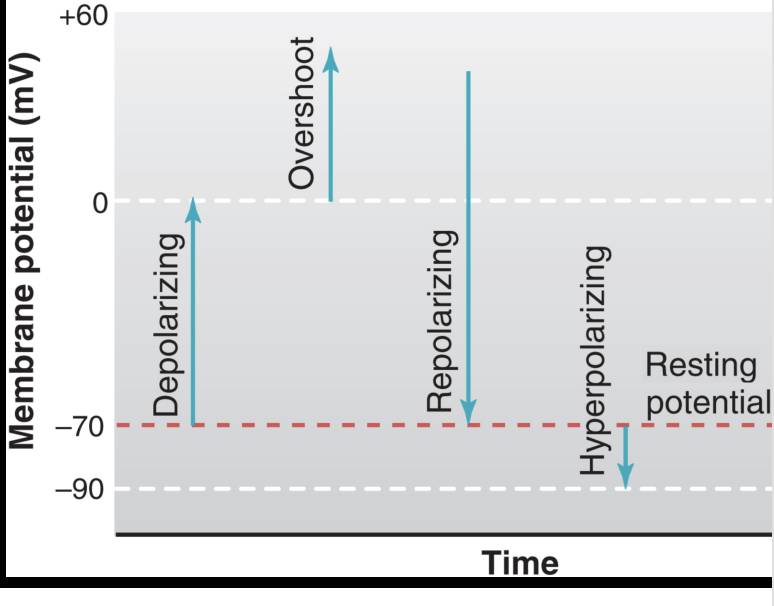
depolarized
membrane potential becomes less negative (towards 0)
overshoot
reversal of membrane potential resulting in inside of cell becoming positive relative to outside
repolarizing
depolarized membrane returning towards resting value
hyperpolarized
potential is more negative than resting level
if an ion concentration increases outside the cell, the equilibrium potential
will increase to oppose movement of ion
equilibrium potential and electrical gradient should always be equal and opposite to achieve electrochemical equilibrium
electrical potential vs chemical gradient
electrical potential→ ion moving according to charge, opp charges attract and move tg
chemical gradient→ ion moving from high to low conc regardless of charges
all mammalian cell types have a separation
of positive and negative charges across CM
action vs graded potentials
all cells can conduct graded potentials but only excitable CMs (neurons, muscle cells, endocrine/immune/reproductive) can have action potentials
this happens through voltage gated ion channels → open or close in response to changes in membrane potential (mostly Na+ or K+)
Na+ & K+ channels
both reversibly change shape
Na+ → responds QUICKLY & opens well before K+ channels, closes faster during repolarization as well
have inactivation gate that limits Na+ flux by blocking channel, closed → open → inactivated → closed ….
K+ → responds slower
action potential steps with ligand gated channels
stimulation of LG channels depolarizes membrane to threshold membrane potential
when threshold value is reached (-55mV) → Na+ channels open and increases depolarization (+ feedback)
+ feedback loop creates overshoot of membrane potential
as membrane potential peaks Na+ permeability declines as inactivation gates break + feedback loop by blocking Na+ channels
depolarized membrane causes K+ channels to open → K+ flows out of cell → repolarizes membrane towards resting value
repolarization causes Na+ channels to go from inactivated to closed & for K+ channels to close
before closing K+ channels the membrane gets slightly hyperpolarized before evening out to resting (-70mV)
subthreshold potentials
depolarizations less than threshold value
action potentials will not occur → will return to resting potential after stimulus is removed
action potentials are all or none
EPSP (Excitatory PostSynaptic Potential)
a depolarizing graded potential that makes a neuron more likely to fire an AP
IPSP (Inhibitory PostSynaptic Potential)
a hyperpolarizing graded potential that makes a neuron less likely to fire an action potential
absolute refractory period
when VG Na+ channels are inactivated → inactivation can only be removed by membrane repolarization
so a second stimulus will not make a second AP during this time
after absolute refractory period is the relative refractory period
relative refractory period
some (not all) of VG Na+ channels are in closed state & some K+ channels are open → new stimulus can depolarize membrane above threshold BUT only if it is big or lasts longer than the absolute refractory period
inside vs outside the cell conc
sodium is > outside
potassium is > inside
chlorine is > outside
trigger zone
where action potentials start and travels down axon terminal
action potentials can travel over long distances without losing amplitude
triggered by depolarizing graded potentials in dendrites that reach threshold value
Na+ & K+ channels open or closed during AP phases
resting→ Na is closed, K is closed
depolarization→ Na open, K closed
repolarization→ Na inactivated, K open
hyperpolarization→ Na closed, K open
hyper/hypo kalemia
hyperkalemia→ high blood potassium
most dangerous as it makes it harder to start an action potential in heart because it is hyperpolarized
hypokalemia→ low blood potassium
dangerous as it gives depolarization of heart cells since less K leaves cell
axon potentials don’t occur on dendrites
because they require VG Na+ channels (which open at threshold potential) and these channels are only in axon hillock (not in dendrites or cell body)
propagation of AP
membrane depolarization @ trigger zone opens Na+ channels → further depolarizaiton → + charges flow from depolarized trigger zone spreads to adjacent sections → flow of current towards axon terminal creates conduction of AP (feedback loop)
positive feedback loop of AP
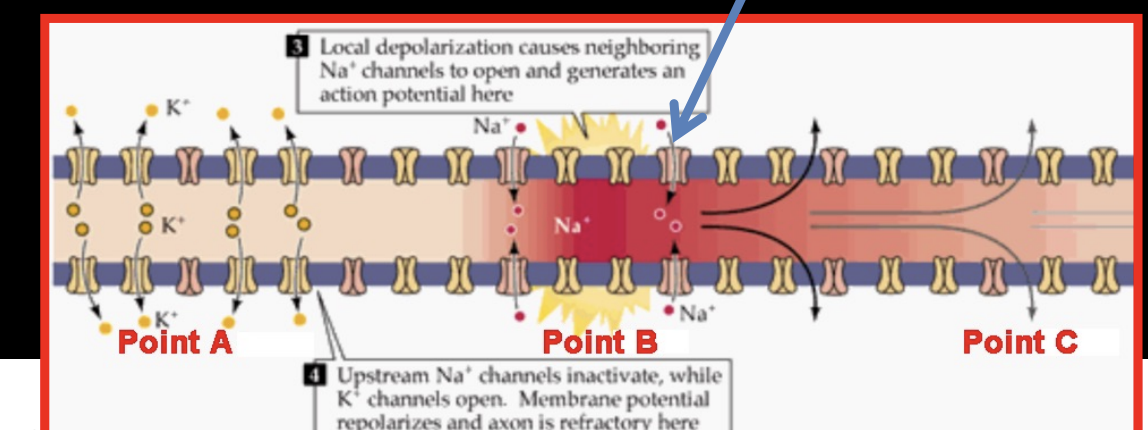
when point B depolarizes it opens Na+ channels → @ point A the Na+ channels are inactivated while K+ channels are open → K+ leaves and repolarizes membrane → positive charge from B flows backward (to A) and forwards to C but backward has no effect because it is in absolute refractory period
AP CANNOT MOVE BACKWARDS
myelinated axons
APs travel faster across
myelinated axons limit touching with extracellular fluid → bare sections are nodes of ranvier
unmyelinated axons have current leakage because axon membrane is in contact w extracellular fluid where there are leak channels
nodes of ranvier
every node has lots of VG Na+ channels → Na+ ions entering at node increases depolarization and restores/regenerates amplitude of AP as it passes from node to node
jumping of AP is called SALTATORY CONDUCTION
electrical synapses
occurs mainly in neurons of CNS (also in glial, cardiac, smooth muscle)
flows in BOTH directions
has rapid conduction of signals from cell to cell that synchronizes activity within a network of cells
chemical synapses
use NTs to pass information from presynaptic neuron to postsynaptic cell
NT cross synaptic cleft after being released from synaptic vesicles
ONE WAY conduction
structure: in postsyn membrane there is PSD (post synaptic density) which is protein dense area that ensures receptors are close to presynaptic NT release sites
NT release mechanism
AP reaches terminal of presynaptic membrane → terminals have VG Ca, K, & Na channels so when depolarization occurs it opens Ca channels and Ca flows into axon terminals → Ca activates fusion of vesicles w terminal membrane → Ca binds synaptotagmin & SNARE which anchor vesicles to CM and undergo conformational change to stimulate vesicle fusion w CM → after fusion vesicles either kiss and run or completely fuse
to remove NT from synaptic cleft
diffusion
enzymatically transformed into inactive substances
actively transported back into presynaptic axon terminal (reuptake)
diff types of muscle
skeletal
cardiac
smooth
skeletal
attached to at least 2 bones by tendons
moves skeleton
multinucleate, unbranched, voluntary
cardiac
heart
pumps blood
1 or 2 nuclei, branched, non-voluntary
smooth
intestines/arteries
moves food
1 nucleus, unbranched, non-voluntary
muscle structure
entire muscle is coated with epimysium (also attached to tendon) → all fascicles are surrounded by 1 large epimysium and perimysium surrounds groups of fascicles → endomysium surrounds individual muscle fibers → sarcolemma (CM of muscle fibers)→ muscle fiber/cell
sarcoplasm
muscle fibers cytoplasm → helps muscle contract
full of myofibrils
sarcolemma is CM of muscle fiber
myofibril
help contract/relax muscle
organelles in sarcolemma
composed of repetitive units → sarcomeres
sarcoplasmic reticulum
surrounds each of myofibrils and helps activate muscle contraction
sarcomere
has thick (MYOSIN (II) ) & thin (ACTIN) filaments
makes muscle striped/striated
contractile units of muscle
myosin
myosin I→ carries substrates as a single unit
myosin II→ forms dimer (2 tails twist around to form coil) → creates thick filament and heads stick out from strand and interact with actin (thin) filaments
heads have actin-binding site & enzymatic domain that hydrolyzes ATP
sarcomere structure
has repeating I band→ A band → I band
sliding filament theory
muscles contract by shortening by all sarcomeres
no change in length of filaments → they slide past each other and increase overlap
myosin activity cycle
ATP binding to myosin head makes it detach from actin filament (this allows sliding, w/o ATP → rigor since all myosin is still attached to actin)
ATP hydrolysis makes head move into ‘cocked’ position → myosin binds weakly to new actin
binding of myosin to actin makes conformational change → releases Pi (inorganic phosphate from ATP hydrolysis)
release of Pi initiates power stroke → returns head to initial uncocked position → release of ADP
troponin
on actin
made of 3 subunits → one is a Ca2+ binding subunit called TnC (TnI, TnT)
tropomyosin
on actin
rod shaped protein that overlaps w 7 actin monomers that cover myosin binding sites
Ca2+ binding
to troponin makes conformational change that shifts tropomyosin into position → reveals myosin-binding sites on actin
allows binding
T-tubules & sarcoplasmic reticulum
work tg to contract muscle
AP follows T-tubules into deep muscle fiber → Ca gets released from sarcoplasmic reticulum → Ca & ATP are needed for myosin/actin interaction → after AP is over Ca is pumped back into sarcoplasmic reticulum by Ca2+ pump proteins
calcium is released by ion channels in sarcoplasmic reticulum CM
AP triggers conformational change in DHP in T-tubules → opens the ion channel ryanodine receptor → releases Ca into cytoplasm
anatomy of sarcomere
region of myofibril btw 2 Z discs
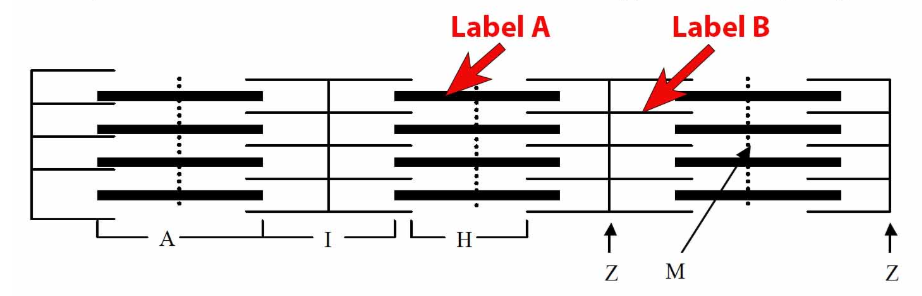
A is thick filament, B is thin filament
A band
extends length of thick filament and small part of thin filament
I band
area btw ends of thick filaments, only encompasses thin filament
H zone
areas btw ends of thin filament, only encompasses small part of thick filament, in middle of A band
Z disc
vertical line separating each sarcomere, in middle of I band
M line
vertical line that connects thick filaments, in middle of H zone
shortening is limited in muscle contraction
only so much overlapping can occur, Z discs may run into ends of thick filament
when contraction occurs→ thin filaments slide past thick, H & I bands get smaller, overlap increases, width of A band is constant
motor neurons
only activating a motor neuron can activate an AP in skeletal muscles
located in ventral horn of spinal cord/brainstem
myelinated and largest axons in entire body → propagate signals at high velocities
motor unit
a motor neuron + muscle fibers it innervates
when AP occurs in motor neuron → all muscle fibers in its unit contract
muscle fibers in 1 motor units are in one muscle but scattered throughout muscle
NMJ (neuromuscular junction)
junction of axon terminal w motor end plate (muscle fiber CM)
vesicles found within axon terminals of motor neuron have NT ACh
interneuronal synapses vs neuromuscular junction
ISPS don’t occur in humans ALL NEUROMUSCULAR JUNCTIONS ARE EXCITATORY
depolarization of 1 motor end plate (EPP) is >>>> excitatory graded potential (EPSP) because @ NMJ a NT is released over large area and binds/open more N-AChR → every AP in motor neuron makes an AP in each muscle fiber
tubocurarine
active ingredient in curare, neuromuscular blocking agent → muscle relaxant
nicotinic ACh receptor are in motor end plate → tubocurarine binds and competitive binds to stop ACh from binding → stops depolarization → flaccid muscle paralysis
blood / plasma
cells in plasma (water)
made of plasma, leukocytes, platelets, hematocrit
all blood constituents are moved thru body tg in 1 direction → bulk flow
plasma makes up 55% of blood volume
leukocytes + platelets make up less than 1%
hematocrit (erythrocytes→red blood cells) makes up 42-45%
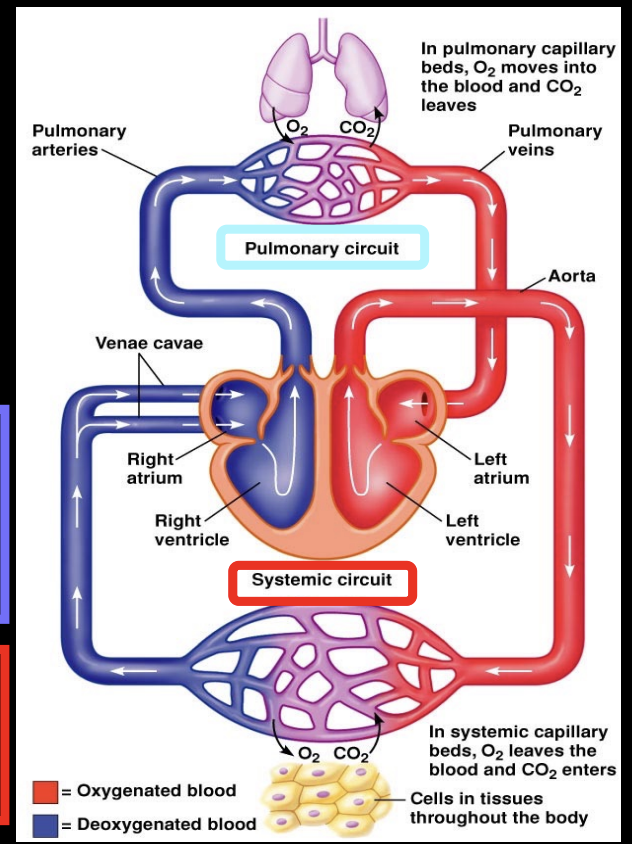
cardiovascular system
has 2 circuits and heart is divided into 2 halves each with an ↑atrium & ↓ventricle
blood flows from atrium to ventricle
deoxygenated blood is moved from right ventricle into pulmonary circuit to lungs → oxygenated blood is returned into left atrium → oxygenated blood is moved from left ventricle into systemic circulation of whole body
arteries & veins
Arteries carry blood AwAy from heart
veins carry blood to heart
blood flows from high pressure to low pressure
heart creates high pressure when it contracts
highest pressure is in aorta, lowest pressure is in venae cavae before it empties into right atrium
aorta → arteries → arterioles → capillaries → venules → veins → venae cavae
Flow calculations
∆P (pressure diff) = P1-P2, measured in mmHg → higher the pressure the greater the fluid flow
Flow = ∆P/R (flow is inverse to pressure)
Resistance (R) = (8 L (length of tube) n (viscosity of fluid)) / (pi * r^4 (radius of tube))
length and viscosity won’t change in adult human, but BUT radius can
vasoconstriction: ↓ blood vessel diameter
vasodilation: ↑ blood vessel diameter
heart structure
outer pericardium layer & inner epicardium
wall of heart is made of myocardium (cardiac muscle cells)
inner surface of chambers in lined with endothelial cells
heart valves (AV)
called AV (AtrioVentricular) valves and have one-way flow
left AV (MITRAL/BICUSPID)→ has 2 flaps
right AV (TRICUSPID)→ has 3 flaps (Right Side has Tricuspid)
interventricular septum→ muscular wall that separates ventricles
during ventricular contraction the AV valves are closed to prevent blood flow back into atria
heart valves (SL)
semilunar and have one-way flow
from right ventricle into pulmonary artery→ pulmonary valve
& left ventricle into aorta → aortic valve
lets blood flow into arteries during ventricular contraction but stops blood from moving in opp direction during ventricular relaxation
heart/myocardial cells gets blood supply via
coronary arteries that branch from aorta
cardiac veins drain into coronary sinus vein which empties into right atrium
AP in heart starts
atria contract first then ventricles
gap junctions connect myocardial cells and allow AP to spread → depolarization from AP starts in SA (SinoAtrial) node in right atrium near superior vena cava → AP spreads then to atria then ventricles
steps for AP throughout the heart
atrial excitation→ depolarization of SA node generates AP that depolarizes all other cardiac muscle cells → SA node determines heart rate
atrial excitation ends→ depolarization spreads thru muscle cell of atria, left & right atria contract @ same time
ventricular excitation→ AP propagates AV node very slowly (allows for atrial contraction completion) → depolarization of AV transmits AP down to Bundle of His
Bundle of His & AV node are only electrical connection btw atria & ventricles
ventricular excitation ends→ depolarization/contraction starts in apex of ventricles then spreads upwards → this makes a contraction that moves blood up towards semilunar valves
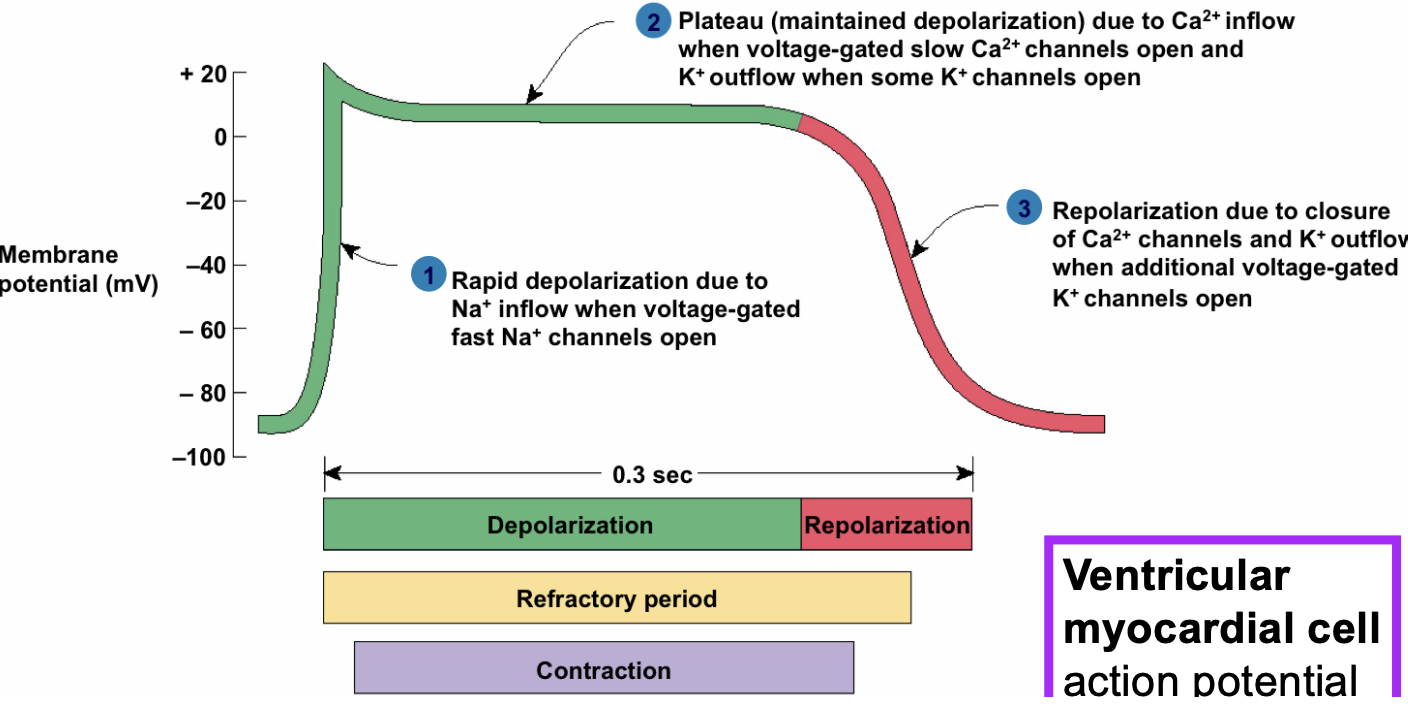
L-type Ca+ channels (long lasting)
cardiac cells uniquely have L-type Ca channels open→ influx of Ca keeps membrane depolarized at plateau level