Neuro E2- Strokes & TIAs
1/86
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
87 Terms
What is very important to ask a patient that you suspect is having a stroke?
last time they were normal without signs of stroke
What is the death of brain tissue as a result of impaired perfusion?
cerebral infarction
What is a potentially reversible injury to brain tissue resulting from impaired perfusion?
cerebral ischemia
What is a brief episode of neuro dysfunction caused by focal brain/retinal ischemia with symptoms usually lasting less than 1 hour (completely resolved in 24 hrs)?
Transient ischemic attack (TIA)
What do TIAs indicate?
impending stroke
What is the syndrome of acute neurological deficits resulting form cerebral infarction due to a sudden focal interruption of cerebral blood flow?
stroke / CVA
What type of stroke?
death of CNS tissue due to infarction that results from disruption of blood supply
MC
ischemic
What type of stroke?
rupture of abnormal blood vessel that results in local disrupted tissue structure and toxic effects of blood products that leads to cell death
hemorrhagic
What is the most common type of stroke?
ischemic thrombotic
What is the most common disabling neurological disorder and 5th MCC of death in the US?
stroke
HTN leads to thickening of vessel wall resulting in ______
lacunar infarct
What is the cause of most deaths that occur w/in 1 week after a massive cerebral infarction?
cerebral edema (reaches maximum 5 days after onset)
What is the main risk factor for all types of strokes?
arterial HTN
What are risk factors for strokes?
older age, smoking, DM, cardiac dz, A fib, preceding TIAs, arterial HTN
What is transient global amnesia?
memory disturbance w/o other neurons deficits
What is the most common metabolic disorder that can mimic a stroke?
hypoglycemia
What should you always get with a confused patient?
glucose levels
How does a migraine present differently than a stroke?
more gradual onset & slower development
What type of stroke presents with an abrupt onset followed by rapid improvement?
embolus
What type of stroke can present with an abrupt onset with progression to maximal deficit over mins-hrs, onset during sleep or a stepwise progression; & with gradual improvement over a day-few wks?
thrombus
What type of stroke has an onset associated with severe HA or alterations in consciousness with a rapid deterioration over a period of a few hours?
intracerebral bleed
An ischemic stroke of anterior circulation would involve what arteries?
carotids, anterior & middle cerebral arteries
An ischemic stroke of posterior circulation would involve what arteries?
vertebrobasilar & posterior cerebral arteries
If the dominant hemisphere is affected in carotid artery occlusion, what will the patient present with?
language deficits - slurred speech & aphasia
If the non dominant hemisphere is affected in carotid artery occlusion, what will the patient present with?
neglect & confusion
What is amaurosis fugax?
I/L monocular vision loss - feels as if a “shade” has come down over 1 eye
What syndrome are the following characteristics associated with?
amaurosis fugax
cortical function loss (depending on hemisphere)
**eyes deviate toward infarcted hemisphere
episodic C/L paresis & paresthesia
slurred speech & transient aphasia
I/L vascular type HA
carotid bruit
microemboli/hemorrhage/exudate in I/L retina
Carotid artery syndrome
What may cause a stroke in the internal carotid territory?
atherosclerotic plaques at bifurcation causing embolization or complete occlusion
What may cause a stroke in the anterior cerebral artery territory?
emboli or SAH
What stroke is associated with the following symptoms?
C/L paralysis & sensory loss of leg > arm
C/L grasp reflex
sucking reflex
apraxic gait
abulia
anterior cerebral artery occlusion
What is the inability to complete a motor task?
apraxia
What is abulia?
spontaneity lost & lack of concern that something is wrong
What stroke is associated with the following symptoms?
C/L motor & sensory deficit
homonymous hemianopsia
cortical function loss (gaze deviates toward infarcted hemisphere)
hemiparesis arm > leg
leg circumducted outward
hemisensory loss
hemianopsia
middle cerebral artery occlusion
If the dominant hemisphere is affected in middle cerebral artery occlusion, what symptoms will the patient have?
aphasia, agraphia, acalculia, alexia
If the non dominant hemisphere is affected in middle cerebral artery occlusion, what symptoms will the patient have?
hemispatial neglect (only groom 1 side), apraxia, confusion
The following sx are associated with what stroke?
occipital lobe effects
hemianopsia- visual cortex, alexia w/o agraphia, memory deficit, unformed visual hallucination, thalamic syndrome (sensory loss, athetosis)
brainstem affects
weber syndrome (I/L CN III palsy and C/L hemiplegia/paresis), paralysis of eye, ataxia
posterior cerebral artery occlusion
What stroke is associated with the following symptoms?
binocular vision issues- blurry, diplopia, blindness
vertigo, N, V, tinnitus
sudden loss of postural tone of all 4 extremities (drop attacks) w/ no LOC
slurred speech, ataxia, numbness around lips/face
cranial neuropathy, eye movement abnormality
paralysis, sensory loss
coma
vertebrobasilar artery occlusion
What condition?
stenosis/occlusion in subclavian artery proximal to vertebral artery → reversal of flow in vertebral artery stealing blood from posterior circulation
blood is diverted away from brain to arm when UE is exercised
subclavian steal syndrome
What symptoms are associated with subclavian steal syndrome?
pre-syncope / syncope, neuro deficits, BP diff b/t arms, arm claudication
What is the treatment for subclavian steal syndrome?
endovascular stenting
small vessel disease is also known as _____
lacunar infarcts
What condition?
not usually preceded by TIAs
slowly evolving deficits
pure motor hemiplegia, dysarthria, ataxis hemiparesis, multi-infarct dementia
step wise progression
main risk factor = arterial HTN
small vessel disease
What happens with increased intracranial pressure?
dec respiratory drive → hypoventilation → inc CO2 → cerebral vasodilation → further elevation of ICP
What lab studies should be done for stroke patients?
CBC, ESR, CMP, fingerstick glucose, PT/PTT, & hyper coagulable workup for young pts
What is the most important diagnostic test for strokes?
STAT non contrast CT
Which stroke has the following appearance on a head CT?
dark; may be normal w/in first 24 hours
ischemic stroke

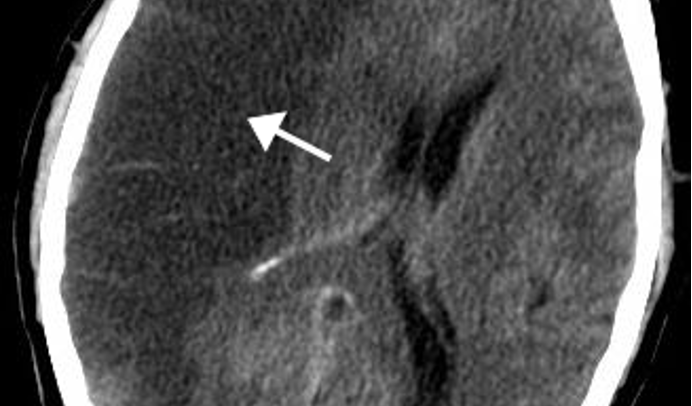
What stroke has the following appearance on a head CT?
bright/white & seen earlier
hemorrhagic stroke
What imaging study can detect acute infarcts sooner and is better at detecting strokes in the brainstem & cerebellum?
MRI
What test is the gold standard for AVM or SAH but has a 1% risk of stroke during the procedure?
conventional angiography
What is the only approved therapy for strokes?
tissue plasminogen activator (tPA)
How soon should tPA be administered for stroke patients?
w/in 3 hours of event (< 60 mins after arriving to ED)
What type of stroke cannot relieve tPA?
hemorrhagic
What should patients presenting with stroke onset who are NOT candidates for tPA be given?
ASA after exclusion of hemorrhage on brain CT
What is exclusion criteria for tPA?
SBP > 185 mmHg or DBP > 110 mmHg
sx of SAH
head trauma / stroke in prior 3 mos
active internal bleeding
hx previous intracranial hemorrhage
low plt count
heparin w/in 48hrs & elevated aPTT
etc
What is the relative exclusion criteria for tPA?
only minor or quickly improving stroke sx
pregnancy
seizure at onset w/ postictal residual neuro impairments
major surgery or serious trauma w/in prior 14 days
recent GI or urinary tract hemorrhage in previous 21 days
recent acute MI in previous 3 mos
BP should not be treated acutely in patients with ischemic strokes UNLESS _____
SBP > 220 mmHg and/or DBP over 120 mmHg
What is the BP management for ischemic stroke patients with elevated pressures meeting requirements for acute treatment?
labetalol IV; lower by 15% during first 24 hrs after onset of stroke
How should a stroke patient be managed after the acute event?
DVT/PE prophylaxis, PT/OT, speech therapy, swallow studies
How are TIAs distinguished from strokes?
complete resolution of focal neuro deficits w/in mins-hrs
When should you consider hospitalization for a patient with a TIA?
Pt w/ first TIA in past 24-48 hrs
sx that are worsening or last > 1 hr
known carotid artery stenosis, afib, or hypercoaguable state
What are treatment options for TIAs?
consider tPA
Antiplts
ASA 325 mg QD
Ticlopidine 250 mg BID (more effective but expensive)
clopidogrel 75 mg QD
carotid endarterectomy
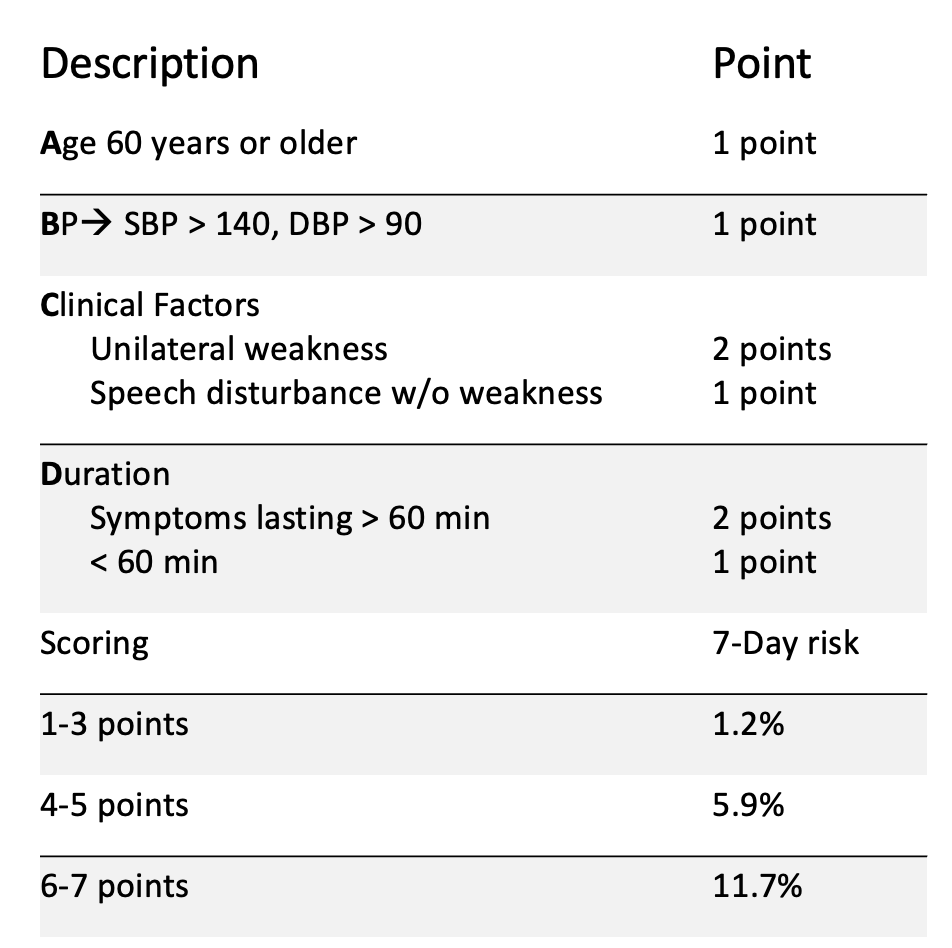
How do you determine risk of stroke for the next 7 days following a TIA?
ABCD rule
20% of all strokes are due to _______
Afib! (pt should be on anticoagulants)
What is more effective than ASA 81 mg in preventing strokes in Afib patients w/o significantly increasing the risk of bleeding complications?
warfarin w/ INR 2-3
What can be used to asses risk of stroke and drug selection?
CHADS2 score
CHF - 1
HTN - 1
Age >75 - 1
DM - 1
prev Stroke or TIA - 2
What drug should a patient with a CHADS2 score of 0 be on?
ASA
What drug should a patient with a CHADS2 score of 1 be on?
ASA or warfarin
What drug should a patient with a CHADS2 score of ≥2 be on?
warfarin
What is the MC underlying cause of non-traumatic intracerebral hemorrhages?
HTN
How does chronic HTN cause intracerebral hemorrhages?
disrupts autoregulation of cerebral blood flow and promotes structural changes in walls of penetrating arteries
What are potential bleeding sites of intracerebral hemorrhages?
deep cerebral (putamen, thalamus), lobar (subcortical), pons, cerebellar
what are signs and symptoms of subarachnoid hemorrhage (SAH)?
“worst HA of my life”, LOC, HA, neck stiffness, nonfocal neuro exam
What kind of hemorrhagic stroke?
usually due to ruptured cerebral arterial aneurysm or AVM → develops from weakness in vessel wall
bleeding causes inc ICP (HA) and dec cerebral blood flow (LOC)
SAH
What condition?
tangle of abnormal blood vessels connecting arteries & veins in brain
MC in brain or spine; rare
may cause HA or seizure; can be found incidentally
arteriovenous malformation (AVM)
What is the treatment for AVMs?
clipping
How does an intracerebral hemorrhage appear on an MRI?
bright center w/ dark periphery; changes as hematoma ages
What is the next step for a patient with a suspected SAH but negative non-contrast CT?
LP → xanthochromia (slightly tinged pink; develops ~4 hrs from hemorrhage)
What is the BP goal for ICH pts w/ SBP 150-220?
lower to 140
What is the BP goal for ICH patients w/ SBP > 220 mmHg?
lower to 140-160
aggressive reduction w/ IV labetolol, nicardipine, clevidipine, esmolol
What is the BP goal for SAH patient?
keep lower than 160
labetalol, nicardipine, lisinopril
(avoid nitroprusside & nitroglycerin)
How do you determine cerebral perfusion pressure (CPP)?
MAP - ICP
In what scenario would lowering BP not be ideal?
increased ICP
(lower BP increases risk of infarction; increased MAP may be the only way to perfuse)
How can you prevent elevated ICP in a hemorrhagic stroke patient?
elevate head of bed; consider sedation (barbiturate coma), mannitol, and hyperventilation (dec CO2 → vasodilation → lower pressure)
What should be done for ICH if risk for hydrocephalus?
external ventricular drainage (EVD)
What ICH patients are candidates for surgical treatment?
Grade 1: normal LOC & mild sx
Grade 3: confused & focal neuro deficits
What ICH patients are NOT candidates for surgical treatment?
Grade 5: coma & decerebrate posturing
What conditions carry high risk of mortality?
ICH & SAH