Topic 4: lung volumes
1/28
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
29 Terms
diseases of the lungs
1. restrictive (trouble with inhalation --> Reduced lung capacity (volunme of air) + LOW lung compliuacne
But normal airway resistance and very minimal airway narrowing)
2. obstrcutive (trouble with exhalation)
restrictive vs obstirctive disease
restrictive: low compliance
obstructive: low elastie recoil
2 tyeps of obstrictive diseases
athsma and Chronic obstructive pulmonary disease (COPD)
what is athsma and what triggers it
Inflammation and smooth muscle contriciton of large airways
Hyperresponsice to triggers:
- Exercise
- Smoke
- Pollutant
how to treat athsma?
1. Anti-inflammatory drug
2. Bronchodilators
- Mimic epinephrine (often beta-2 agonist eg. salmutamol)
- Inhibits acetocholine
- These both relax the airways
What is COPD often caused by
a noxious chemical (eg. tobacco)
2 examples of COPD caused by the same agents:
1. Emphysema
Destructuion and collaps of smaller airways
2. Chronic bronchitis
Chronic inflammation of airways and excessive mucous production in smaller airways
how to treat COPD
Similar to asthma (antiinflamatory and bromchodilator)
May only be partially reversible unlike asthma
what do obstrictive diseases result in? what does that cause in the patient?
Each disease results in:
- increased airway resistance
- decreased air flow rate
This causes:
- Increased work of breathing
- Compromises gas exchange
- Impaired oxygenation of blood
what is restrictive lung disease caused by
pulmonary fibrosis (thickening of alveolar elastic tissue) or neuromuscular disorder
lung volumes
tidal volume: avg vol of eair entering and leavign during a single rest breath
inspiratory reserve volume: max extra volume ur can inspire ontop of tv
Exiratory reserve volume: max extra vol u can activley expir at the end of a resting tidal volume
residual volume: vol of air that remains in lungs even after max expiration
lung capactities
inspiratory capacity: IRV + TV
max vol that can be inspired starting from the end of a normal expiration
vital capacity: IRV + TV + ERV
vol of air that can be move in and out of lung in a single maximal breath
Total lung capacity: IRC + TV + ERV + RV
functional resisdual capactiy: ERV + RV
vol of air in lungs at end of normal rest expiration
what lung value can be changed with exercise (dynamic values?)
TV can inc w chronic exercise which then changes ur IRV, ERV and IC
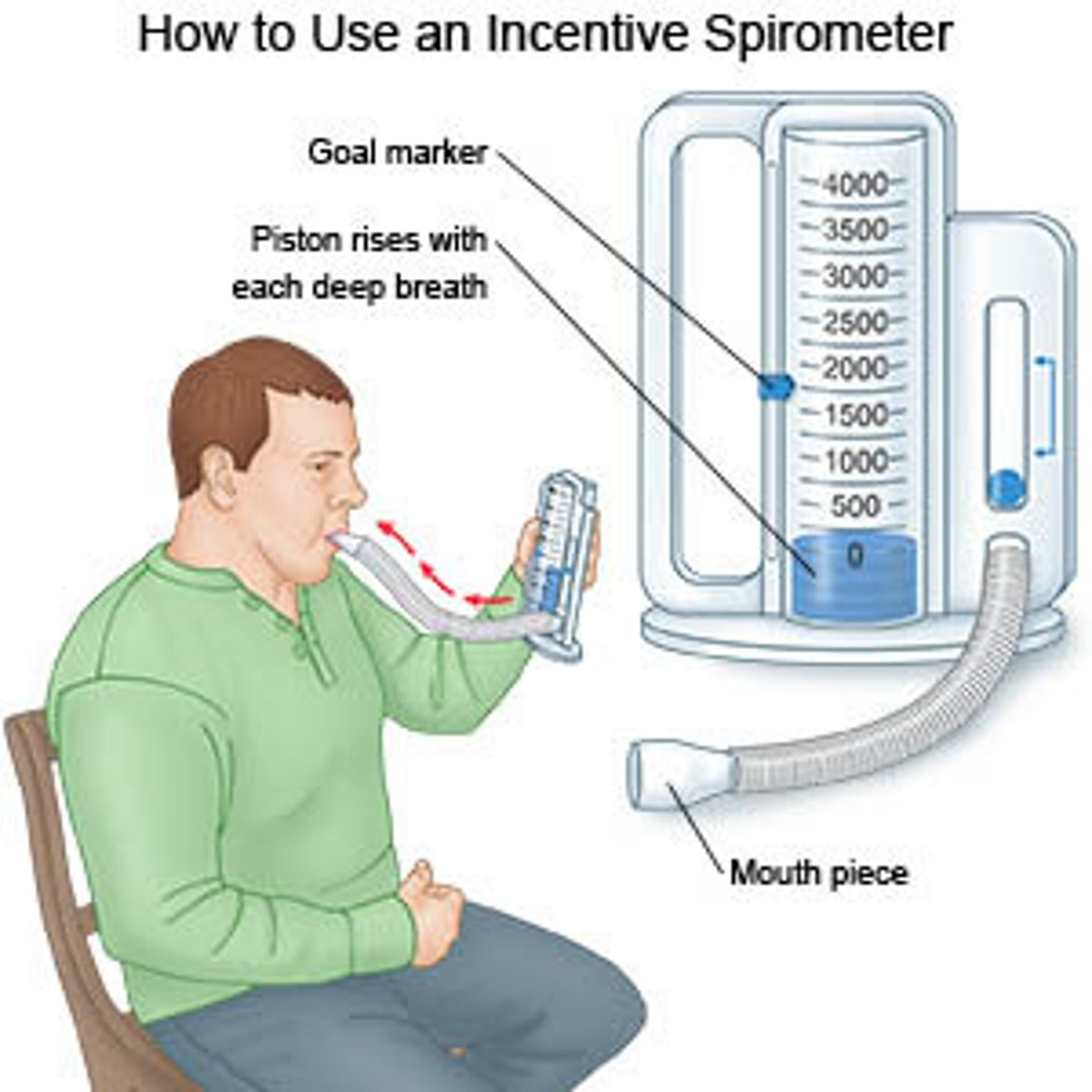
hwo to measure lung volumes
spirometer a air fulled drum floating in a water chanmer to measure the vol of air breathed in and out
* can also track time to determine flow
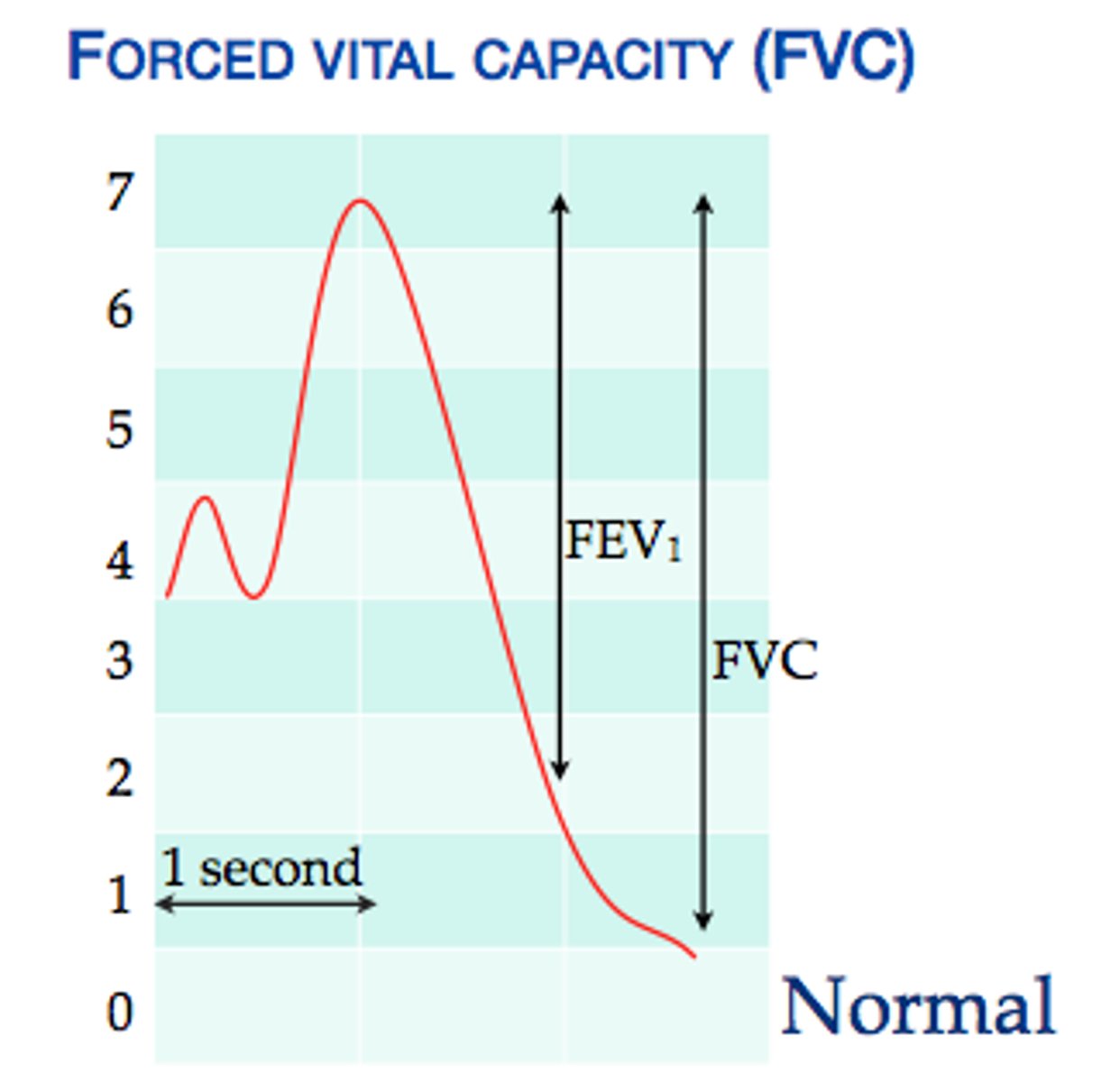
forced maneuver lung volumes
FEV1 = forced expiratory volume in 1 second (after a max inpiration)
FVC = Forced vital capacity (Vital apacity but measured during a maximal expiration effort starting from TLC)
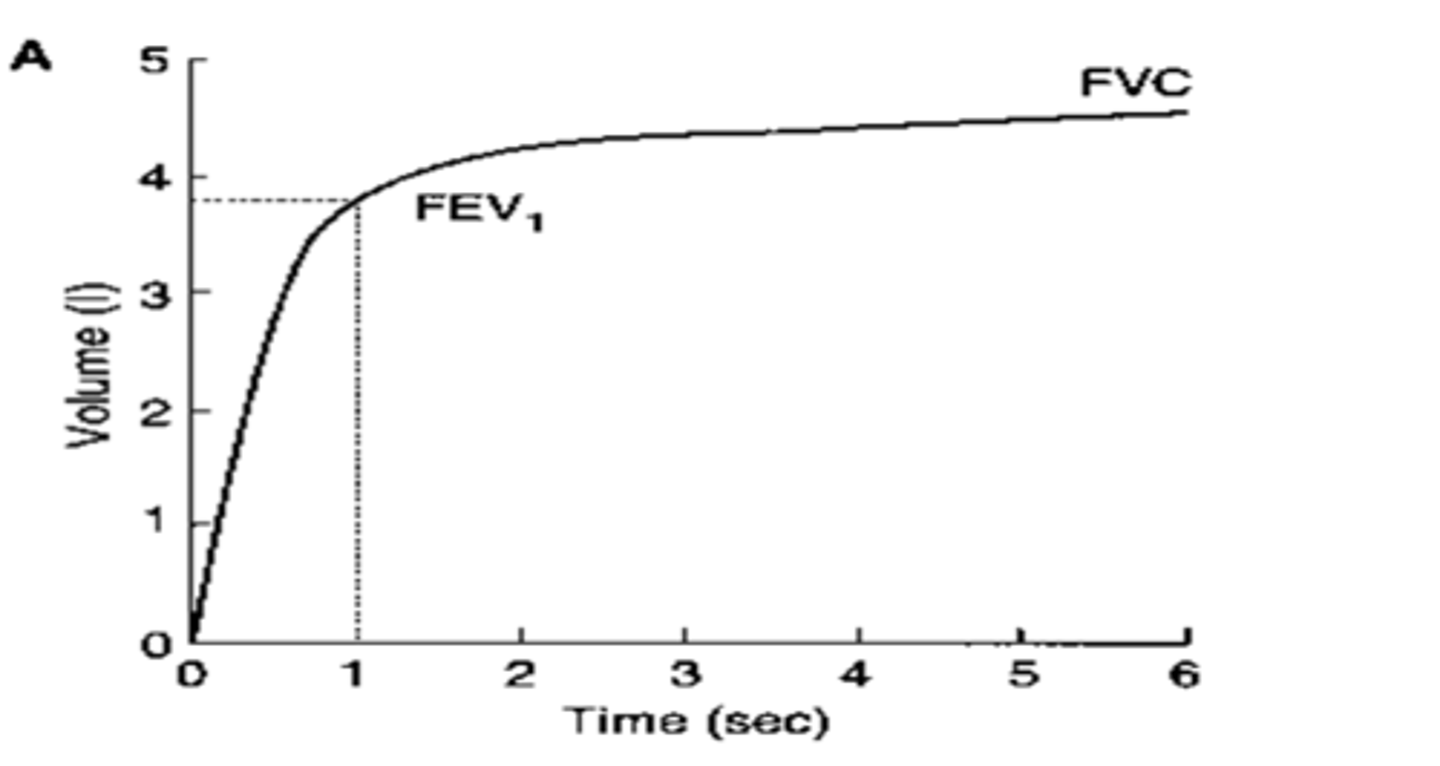
FEV1/FVC ratio ( what and range)
tells you the fraction of ur total FVC you can expire in the first secodn
0.7 - 0.85 is normal --> below 0.7 indicates obstrictive disease
- decreases with age
- typically higher in females
Spirometry Tracing (flow vs time graph)
how to read a flow-volume loop?
yaxis - flow (L/s)
x-axis - volume (L) **start at 6L --> 2L
above 0 flow value = exiration
below 0 flow value = inspiration
Little circle : resting eupnaic breathing
Large loop: vital capacity
Dashed loop: durign exercis
Peak expiratory flow/PEF (at top)
Fev1 (somwhere around 3L)
FVC (width of the loop)
RV (whats passed the right of the loop)
IC (from left of loop to right of little loop)
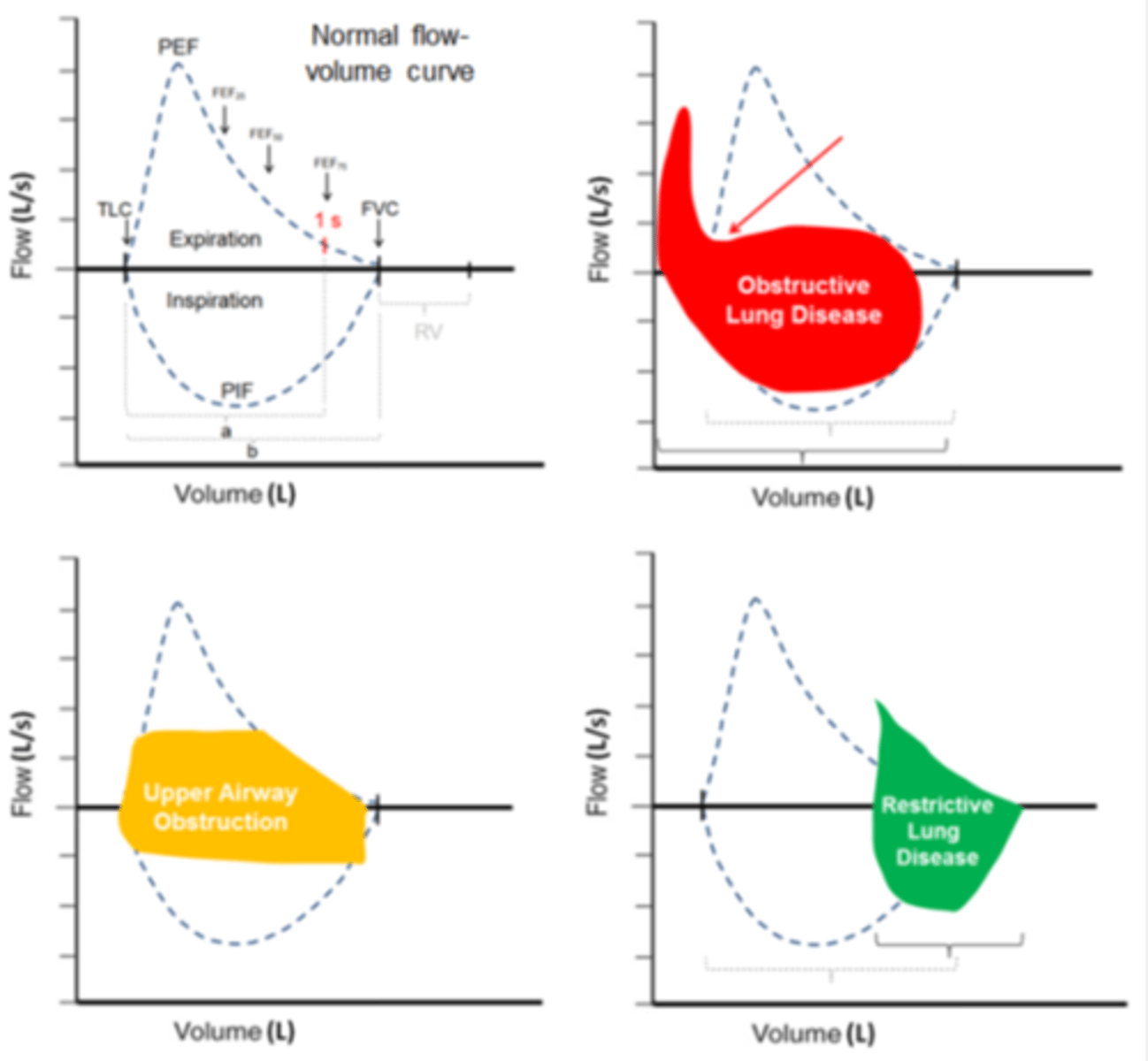
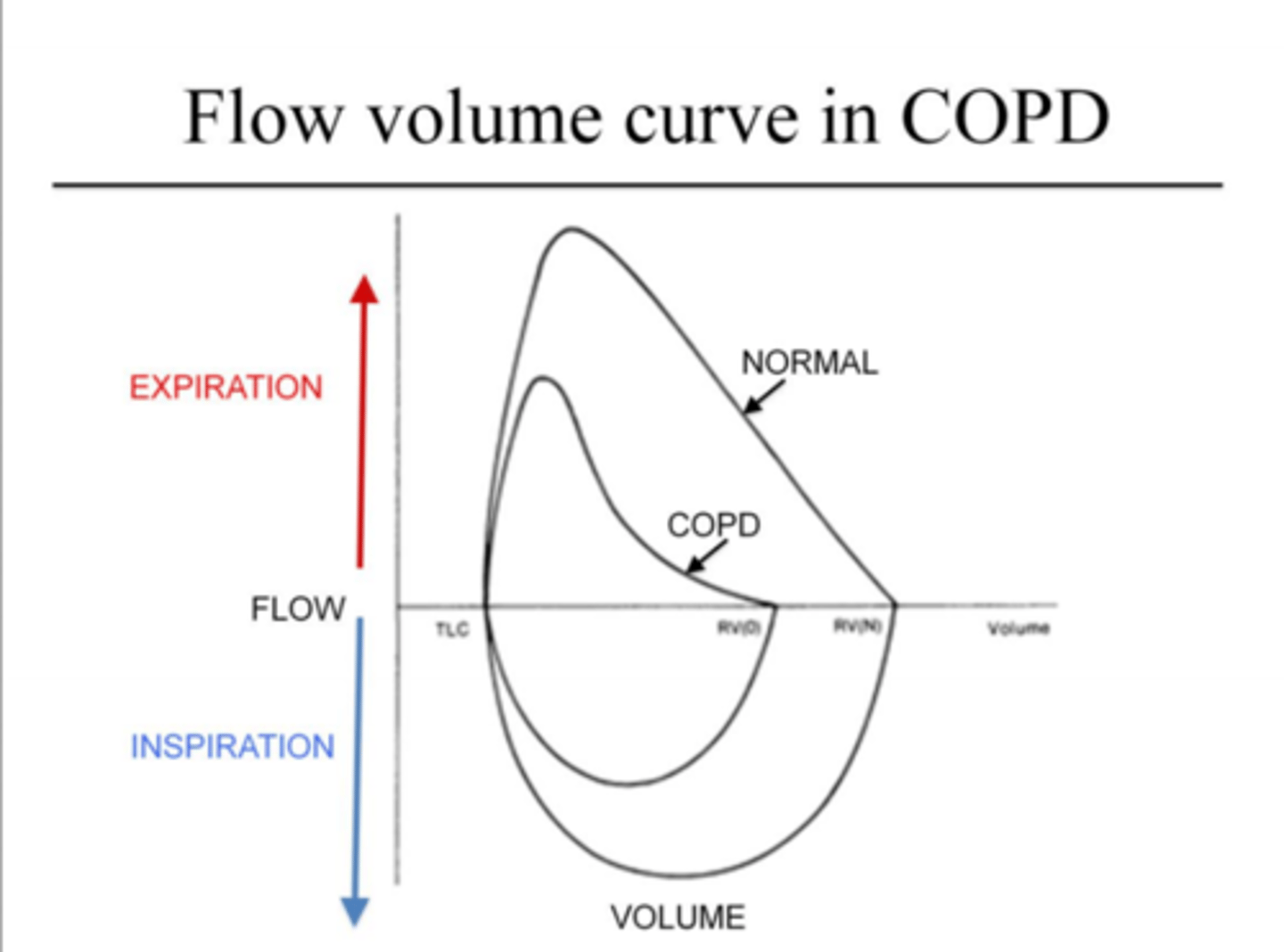
Obstructive lung disease (COPD) flow volume curve (changes and why)
(PEF, FEV1, FVC, ratio etc)
- severe limitations with expuratioins (top of loop)
- lower PEF
- major scooping: imparment in max expiratory flow... leads to:
- Much wer FEV1 --> FEV1/FVC <0.7
why?
1. airway narrowing --> ↑ resistance
2. loss of elastic recoil/very compliant
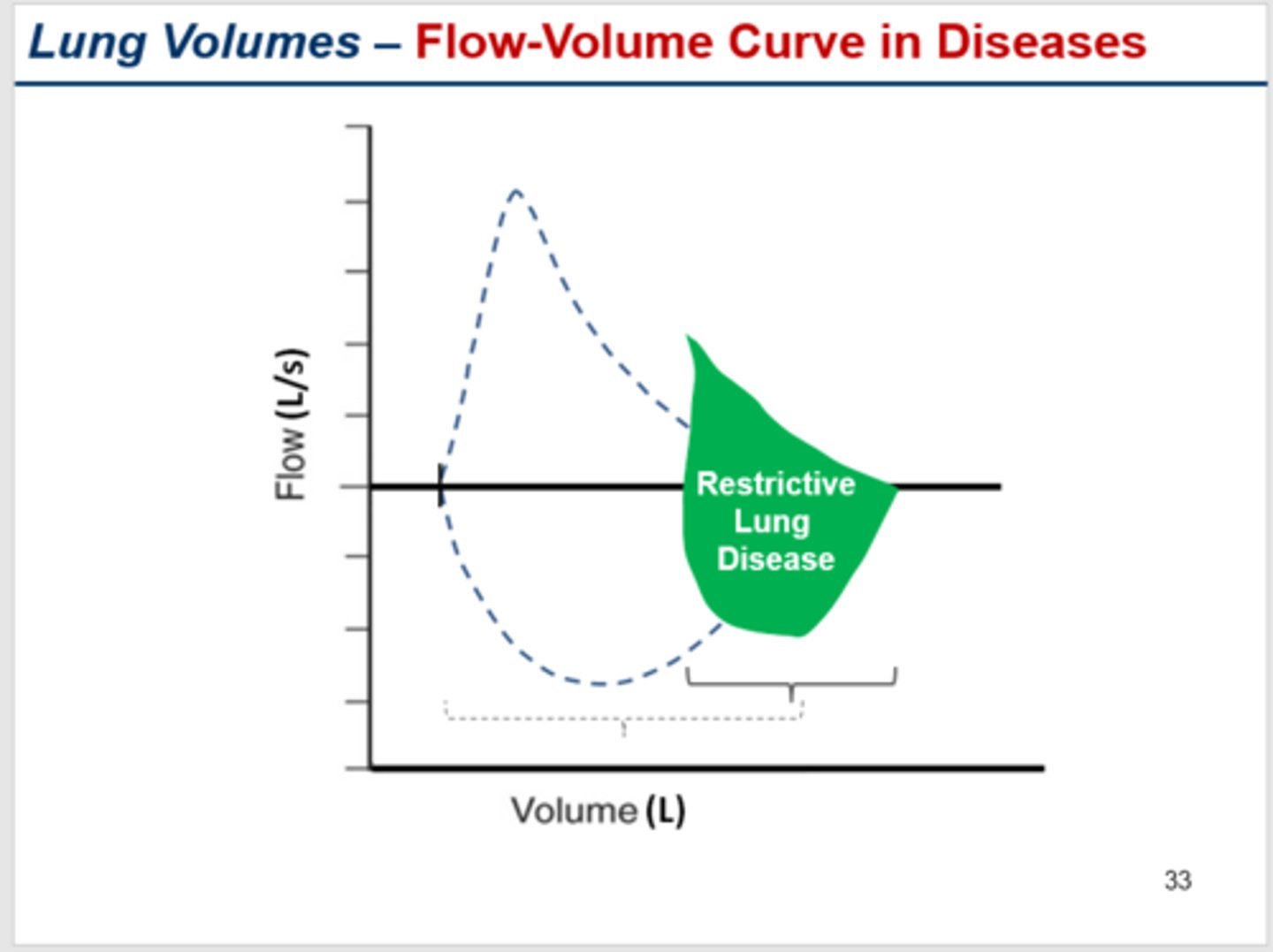
Restrictive lung disease (interstitial lung disease eg. pulm fibrosis) flow volume curve
(PEF, FEV1, FVC, ratio etc)
- cannot inflate sufficiently --> severe volume limits --> shifts right
- smaller FVC
- normal PEF
- FEV1 will be impaired (bc of LOW FVC NOT airways resistance)
- FEV1/FVC ratio normal or high >0.7 >0.8 in severe cases bc fvc is so low
why?
1. very low compliance/high recoil
ventilation (what is it)
the amount of air moved in and out of the alveoli expressed as a rate
Minute Ventilation (VE)
amt of air moved in and out in a minute
Minute ventilation = Tidal volume x Respiratory rate/frequency
VE (ml/min) = TV (ml/breath) x f (breaths/min)
alveolar ventilation
the amount of air that reaches the alveoli (Ve - Vd deadspace ventilation)
VA (ml/min) = (TV - VD)(ml/breath) x f (breath/min)
how much air is lose in deadspace that doesnt reach alveoli (ecample value)
So the amount of air available for gas exchange VA is not the same as the amount of air moved VE
= not all of the air we breath in and our actually reaches the alveoli and gets caught in the conducting zone eg. 30%
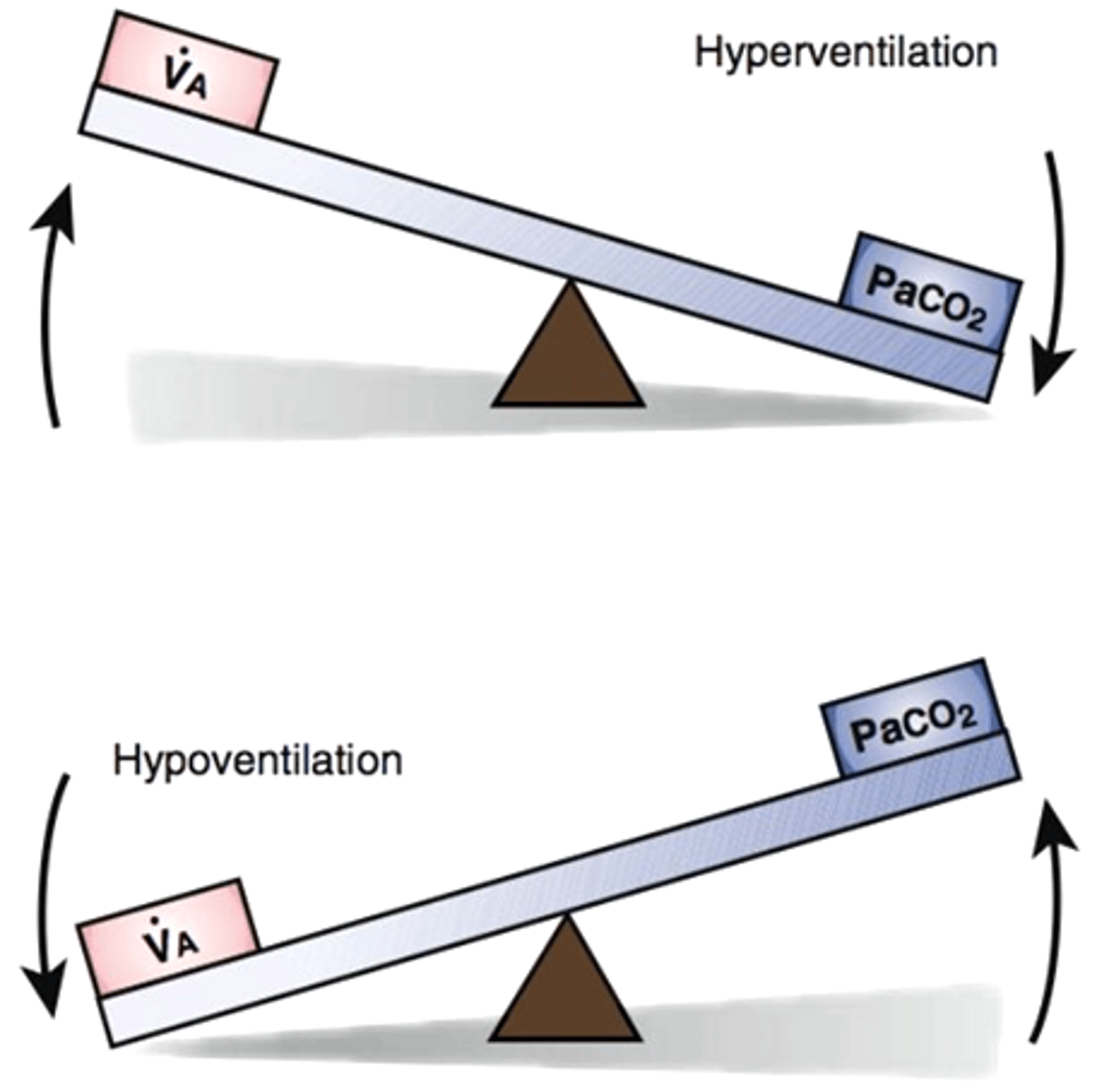
How do we know if alveolar ventilation is sufficient?
By looking at our article blood O2 and Co2 content
If alveolar ventilation is not enough → ↑CO2 ↓O2
If alveolar ventilation is too much → ↓CO2 ↑O2
what are the correct range for artierial o2 and co2
if alveolar ventilation is suffencuent then...
→ arterial O2 content will be in normal physiological range = 96-100% Hb saturation
→Alveolar/Arterial CO2 is within a narrow physiological range (i.e. ~36-40 mmHg)
alveolar ventilation equation:
P_ACO2 = VCO2/VA x K
P_ACO2: concentration of expired co2 in alveoli/simmilar to areterial blood
VCO2: volume of expired co2
VA: alveolar ventilation
K: constant
what happens to alveolar ventilation when exercising (think of equation)
we need arterial/alveolar co2 to remain 36-40mmhg
but during exercise: VCO2 increases
so:
alveolar ventilation (VA) increases --> why we breath faster
what happens to arterial/alveolar CO2 if VCO2 remains constant then you start increasing ventilation? what if u hold ur breath?
inc ventilation:
arterial Co2 concentration is going to drop the SAME AMT
holding breath:
→ arterial CO2 concentration will increase bc we are not expiring it