Physiology Exam 3
1/103
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
104 Terms
what are the different components of the blood?
plasma, buffy coat (leukocytes & platelets), erythrocytes (red blood cells)
what is hematocrit and what can it demonstrate?
the percent of total blood volume made up of RBC. higher hematocrit can indicate polycythemia, lower hematocrit can indicate anemia
what is plasma? what is it made of?
the liquid portion of the blood used for transport, made of 90% water and 10% proteins, electrolytes, nutrients, hormones, waste products
what are the different plasma proteins, and what are their functions?
albumin: maintains osmotic pressure, regulates blood volume and pressure, acts as a carrier protein
globulins: alpha/beta transport lipids, fat-soluble vitamins, and metal ions. gamma are antibodies that fight infection by recognizing and binding to pathogens
fibrinogen: when bleeding occurs, fibrinogen is converted into fibrin which forms a mesh to stop the bleeding
what is the structure and function of erythrocytes?
structure: bioconcave discs, no nucleus/organelles, very flexible
function: transport oxygen from lungs to tissues, transport CO2 from tissues to lungs, help maintain blood pH
understand the structure and function of hemoglobin
structure: 4 subunits, each with a heme group with an iron at its center. oxygen binds to this iron, so 4 oxygens can bind to one hemoglobin
function: bind oxygen in lungs, release oxygen in tissues
how many oxygen molecules does each hemoglobin molecule bind?
4
hemoglobin can bind to other substances other than oxygen. what is the beneficial and harmful binding that can occur?
beneficial: CO2, H+, nitric oxide
harmful: CO, nitrates
what is erythropoiesis and how does it occur?
erythropoiesis is the production of new red blood cells from stem cells in the bone marrow; occurs because hypoxia (low oxygen levels) triggers the kidneys to release erythropoietin, which stimulates the production of RBC. hyperoxic conditions relieve the negative feedback loop
what are the different blood groups, and how are donors and recipients determined in blood transfusions?
antigens are markers on RBCs, antibodies are proteins in plasma that attack foreign antigens.
Blood Type | RBC Antigens | Plasma Antibodies |
A | A antigen | Anti-B antibodies |
B | B antigen | Anti-A antibodies |
AB | A and B antigens | No anti-A or anti-B antibodies |
O | No A or B antigens | Anti-A and Anti-B antibodies |
what is the universal donor?
O
has no A or B antigen, no Rh antigen
what is the universal recipient?
AB
has A, B, and Rh antigens; does not have anti A or anti B antibodies
How does Rh factor work, and when can it cause complications in pregnancy?
Rh is another antigen, can be + or -, if mother is negative and fetus is positive, her body will try to fight off the foreign antigen
what are leukocytes? what are the five main types and their functions?
leukocytes: white blood cells formed in bone marrow; mobile units of the body’s immune defense system
polymorphonuclear granulocytes: granulated cytoplasm, lobed nucleus
neutrophils: phagocytosis
eosinophils: attack parasitic worms
basophils: release histamine
mononuclear agranulocytes: no granules, single round nucleus
monocytes: become tissue macrophages, microglia, or osteoclasts
lymphocytes: B produce antibodies, T cell-mediated immunity
what are platelets and what are their functions?
cell fragments from megakaryocytes, function in hemostasis (blood clotting)
explain the three steps of clot formation or hemostasis. how is clot formation accomplished?
vascular spasm (vasoconstriction): after injury, blood vessel constricts to restrict flow to damaged area
platelet plug formation: platelets adhere to damaged vessel wall and release chemicals to activate more platelets (aggregation), release PF3
coagulation (blood clot formation):
prothrombin —> thrombin (requires PF3)
fibrinogen —> fibrin: thrombin converts soluble protein into insoluble fibers
clot formation: fibrin strands form a mesh to trap RBC and platelets, stable blood clot formed
what is the difference between the intrinsic and extrinsic clotting cascade?
intrinsic: activated by damage inside vessel (which activates factor XII, or Hageman), slower, all factors present in blood
extrinsic: activated by damage to external tissue, fast, 4 steps, uses tissue factors external to blood, tissue thromboplastin can activate factor X, common pathway
what is clot retraction?
once blood clot seals a wound, platelets trapped in the fibrin clot contract and shrink the fibrin mesh, pulling the edges of the damaged vessel together
how is clot dissolution accomplished?
plasmin becomes trapped in the clot and later dissolves it by slowly breaking down the fibrin meshwork (plasminogen → plasmin → fibrin breakdown)
why do researchers think some frogs and lizards have green blood? what causes their blood to be green? How do some glass frogs make themselves even more cryptic when on green vegetation?
accumulation of biliverdin makes their blood green; can be useful for camouflage or toxic to parasites; glass frogs move their RBCs to their liver to make themselves more transparent
what are the three main components of the circulatory system? What are their overall functions?
heart - established a pressure gradient to pump blood
blood vessels - passageways for pumped blood throughout the body
arteries: carry blood away from ventricles
veins: carry blood to atria
blood - transport medium, serves body cells
red vs. blue
how does blood flow from and to the heart?
deoxygenated blood enters right atrium via superior/inferior vena cava → right AV (tricuspid) valve → right ventricle → pulmonary semilunar valve → pulmonary arteries → lungs → Co2 released, O2 picked up → pulmonary veins → left atrium → left AV (bicuspid/mitral) valve → left ventricle → aortic semilunar valve → aorta → arteries throughout body → O2 delivered, CO2 picked up → veins → right atrium :)
how do the valves of the heart work?
one way valves prevent backflow of blood, open and close based on pressure differences
explain the differences between the atrioventricular (AV) and semilunar valves
atrioventricular: between atria and ventricles, open when atrial pressure > ventricular pressure
right side: tricuspid valve
left side: bicuspid/mitral valve
semilunar: between ventricles and major arteries, opens when ventricular pressure > arterial pressure
pulmonary: right ventricle → pulmonary artery
aortic: left ventricle → aorta
what are the three main layers of the heart wall?
endocardium, myocardium, epicardium
understand the intercalated discs of the myocardium, the cell junctions they contain, and their functions.
intercalated discs: cardiac muscle arranged spirally around ventricle, “wrings” blood when it contracts
desmosomes: mechanical strength
resist mechanical stress
hold cardiac cells together
gap junctions: electrical communication
areas of low electrical resistance
allows action potentials to spread from one cell to adjacent cells
Functional Syncytium: the heart behaves as one coordinated unit because all excited cardiac cells contract together
what is the pericardial sac? what is its function?
a thin, double-layered membrane that encloses the heart
fibrous pericardium: tough outer layer that anchors heart in place
serous pericardium: secretory lining to secrete pericardial fluid and provide lubrication to prevent friction between pericardial layers
how is heart contraction triggered at the cellular level?
autorhythmicity: the heart contracts rhythmically as a result of action potentials that it generates by itself
an action potential reaches a contractile cardiac muscle cell
depolarization opens voltage-gated L-type Ca2+ channels in the membrane
a small amount of Ca2+ enters the cell
this triggers the sarcoplasmic reticulum to release more Ca2+ (calcium-induced calcium release)
Ca2+ binds troponin, shifting tropomyosin
actin-myosin cross-bridges form → contraction occurs
what are the differences between autorhythmic and contractile cells, how are they depolarized, and what are their roles in the electrical activity and contraction of the heart?
autorhythmic: 1%
initiate and conduct action potentials responsible for contraction of working cells
electrical impulses, do not contract themselves
don’t have resting potential
slow, drifting depolarization (pacemaker activity)
contractile: do mechanical work of pumping
produce force
depolarization triggered by electrical spread from autorhythmic cells via gap junctions
stable resting membrane potential
know figure of action potentials of autorhythmic and contractile cells
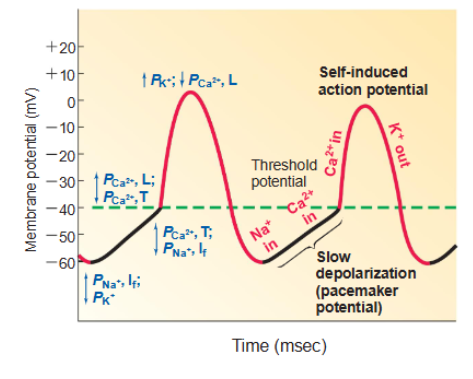
what are the important ion channels involves in autorhythmic and contractile action potentials?
autorhythmic:
Na+ funny channels
T-type Ca2+ channels
L-type Ca2+ channels
K+ channels
contractile:
voltage-gated Na+ channels
L-type Ca2+ channels
Ca2+ channels
which ions are driving the formation of action potentials?
Na+, Ca2+, K+
why are long refractory periods in contractile cells important?
prevent tetanic contraction, ensures heart fully relaxes between beats, allows proper filling of chambers before next contraction, essential for coordinated pumping, not continuous tension
where are the noncontractile cells located in the heart?
SA node: right atrium wall near superior vena cava
AV node: base of right atrium near septum
bundle of his: originate at AV node and enter interventricular septum, divides to form right and left bundle branches
purkinje fibers: extend from bundle of his and spread through ventricular myocardium
how do the locations of the noncontractile cells drive electrical activity around the heart during a contraction/excitation?
they create a controlled electrical pathway so that contraction occurs in order:
atria contract first (fill ventricles)
ventricles contract second (pump blood out)
electrical conduction pathway:
SA node → atria → AV node → bundle of his → right + left bundle branches → purkinje fibers → ventricular contraction
key role of each region:
SA node: starts heartbeat
AV node: delays signal so ventricles fill
bundle of his: connects atria → ventricles
purkinje fibers: rapidly distribute signal for strong ventricular contraction
why is the SA node the pacemaker of the heart?
has the fastest spontaneous depolarization rate, its cells reach threshold before other autorhythmic cells, so it cells the dominant rhythm
what happens if the SA node breaks down or is damaged?
other autorhythmic cells take over at slower rates, will still pump but slower and less coordinated with reduced efficiency
AV node becomes backup pacemaker (~40-60bpm)
if AV fails, purkinje fibers take over (~20-40bpm)
what is an electrocardiogram and what is it measuring?
a graph of electrical activity from the heart, measuring activity in fluids that reach the body surface. recording represents spread of activity through the heart during depolarization and repolarization
what are the components of the ECG trace and what do they represent in the cardiac cycle?
P-wave: atrial depolarization
PR segment: AV node delay
QRS complex: ventricular depolarization, atria repolarization
ST segment: ventricles contract (empty)
T-wave: ventricular repolarization
TP interval: ventricles relax and fill
what is the purpose of measuring an ECG? What are the heart rate abnormalities that it can pick up on?
abnormalities in rhythm (arrhythmia)
extra systoles (contractions)
atrial flutter
atrial fibrillation: pulse deficit, no P wave
ventricular fibrillation: uncoordinated contractions, inefficient pumping
heart block: atrial rate normal, ventricular rate slower
cardiac myopathies: damage to heart muscle
myocardial infarction: heart attack, abnormal QRS complex
what is systole and diastole?
systole - contraction and emptying
diastole - relaxation and filling
Explain one complete cardiac cycle, in terms of the ECG trace, the atrial, ventricular, and aortic pressures, the left ventricular volume, and the heart sounds. What is happening in the heart at each step?
mid ventricular diastole (filling)
TP segment
atrial pressure slightly > ventricular pressure
AV valve open and passive filling of ventricle occurs
late ventricular diastole (filling)
P wave
atrial depolarization and contraction
AV valve open
end of ventricular diastole (filling)
atrial contraction and ventricular filling are complete
end-diastolic volume (EDC) = 135 mL
onset of ventricular systole (contraction)
QRS complex - ventricular excitation, induces contraction
backward pressures closes AV valve
first heart sound
isometric ventricular contraction
after AV closed, ventricular pressure must increase until it exceeds aortic pressure
all valves close briefly
isovolumetric = constant volume and length
ventricular pressure continues to rise
ventricular ejection
ventricular pressure > aortic pressure - aortic valve forced open
blood ejection from heart begins
SV = stroke volume, amount of blood pumped out of each ventricle
end of ventricular systole
only about half of blood is pumped out
end-systolic volume (ESV) = 65 mL
stroke volume (SV) = EDV - ESV = 70 mL
onset of ventricular diastole
T wave
ventricular pressure < aortic pressure = aortic semilunar valve closes
closing results in dicrotic notch = second heart sound
isometric ventricular relaxation
all valves closed again
no blood leaves or enters the ventricle and pressure falls
ventricular filling
ventricular pressure < atrial pressure = AV valve opens
blood fills ventricle again
Wiggers diagram
some key terms: isometric ventricular ejection, isovolumetric ventricular relaxation, end-diastolic volume, end-systolic volume
End-Diastolic Volume (EDV): max blood in ventricle (before contraction)
End-Systolic Volume (ESV): blood left after contraction
Stroke Volume = EDV − ESV
Isovolumetric contraction: pressure ↑, volume same (all valves closed)
Isovolumetric relaxation: pressure ↓, volume same (all valves closed)
what causes the two heart sounds?
lub (1st): associated with closing of AV valves
dup (2nd): associated with closing at semilunar valves
(caused by vibrations, not the valves snapping shut)
what is stroke volume (SV)? how do you calculate it?
stroke volume: how much blood the ventricle pumps out in one beat
SV = EDV - ESV
SV = 135 - 65 = 70
70 mL pumped out of each ventricle during each contraction
(EDV: amount of blood in the ventricle before contraction, ESV: amount of blood left after contraction)
what is ejection fraction? how do you calculate it?
ejection fraction: percentage of blood that is pumped out of the ventricle each beat, tells you how efficiently the heart is pumping
Ef = SV/EDV
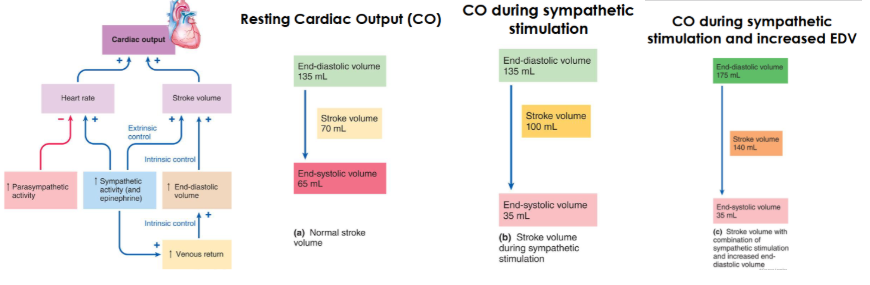
what is the relationship between cardiac output, stroke volume, and heart rate?
cardiac output (CO) = stroke volume (SV) x heart rate (HR)
if SV or HR increases, CO increases
if SV or HR decreases, CO decreases
how does cardiac output (CO) vary so much with exercise?
goes from ~5L to 20L or more
varies via control of HR and SV
explain the parasympathetic and sympathetic control of heart rate
parasympathetic: vagus nerve supplies SA and AV nodes → release of acetylcholine → increased permeability to K+ → hyperpolarizes membrane → even slower drift due to threshold → decreased heart rate
sympathetic: norepinephrine (from sympathetic nerve endings) → decreased K+ permeability → cell depolarized → faster drift to threshold → increased heart rate
epinephrine: released from adrenal medulla upon sympathetic stimulation, increased sympathetic activity
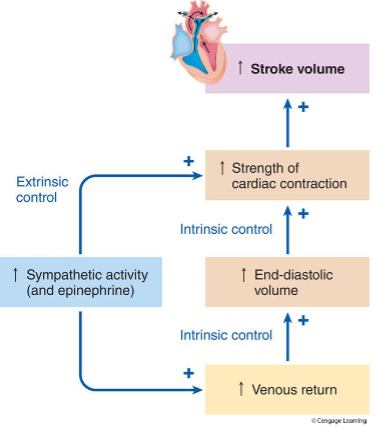
explain the intrinsic and extrinsic control of stroke volume. draw a diagram
what is the frank-starling curve, or law of the heart?
depicts relationship between EDV and SV or between muscle fiber length and muscle tension
“the more the heart fills with blood during diastole (increased EDV), the stronger it contracts, and the greater the stroke volume (SV)”
how does the frank-starling curve relate to cardiac muscle tension and cardiac muscle fiber length, and stroke volume and end diastolic volume? diagram
stroke volume is dependent on venous return
cardiac muscle fibers stretch - greater tension
increased EDV = more stretch = increased SV
increased EDV = increased stretch = increased force = increased EDV
fiber length ←→ tension
EDV ←→ Sv
how can sympathetic stimulation compensate for a failing heart?
sympathetic stimulation can shift curve to the LEFT, increasing stroke volume towards normal
compensates by increasing EDV above normal
failing heart pumping same amount of blood at greater cardiac muscle length
has to boost: HR, force of contraction, or EDV
explain how end-diastolic volume, stroke volume and end-systolic volume relate to cardiac output during resting and during sympathetic stimulation of the heart. What if the end-diastolic volume also increases? what is the most important determinant of end-diastolic volume? draw a flow chart
what are the reconditioning organs and what do they do? which organs can withstand decreases in blood supply for short periods, and which cannot?
reconditioning organs: organs that can withstand a temporary reduction or redirection of blood flow (kidneys, digestive tract, skin)
non-conditioning organs: the brain and the heart
explain how the blood flows through the vascular tree
heart → arteries → arterioles → capillaries (gas exchange) → venules → veins → heart
what is microcirculation?
the blood flow through the smallest vessels where actual exchange happens arterioles → capillaries → venules
how do you calculate flow rate? what are they key determinants of flow rate?
flow rate determines how much exchange of O2, CO2, and nutrients takes place
F = delta P/R
F = flow rate of given volume of blood through a vessel
delta P = pressure gradient (from beginning to end of vessel)
R = resistance
blood flows from area of high to low pressure (pressure gradient)
what is resistance (relating to blood flow)?
opposition to blood flow through a vessel
what is resistance proportional to? what is it inversely proportional to?
directly proportional to viscosity (n - thicker blood = more resistance) and vessel length (L - constant in adults, longer vessel = more resistance)
inversely proportion to vessel radius (r) - doubling or halving the radius will decrease/increase resistance by 16-FOLD
what is the major determinant of resistance to blood flow
radius
(since its to a factor of 4, minor changes will drastically change resistance) doubling radius = decrease resistance 16-FOLD
for the same volume of blood: increase in radius decreases surface area in contact with blood and decreases resistance to flow
how do changes in vessel radius change the distribution of cardiac output around the body?
change in vessel radius changes the distribution of cardiac input (blood flow is matched to tissue needs, vasodilation/constriction accordingly)
which body systems or organs receive increased, decreased, or no change in blood flow during moderate exercise/sympathetic stimulation?
increase: skeletal muscle (1066%), skin (370%), heart (367%)
neutral: brain
decrease: digestive system, liver, kidneys, bones
what are the key differences in vessel anatomy between arteries, arterioles, capillaries, and veins?
arteries: pressure reservoirs
very thick
high pressure
elastic recoil
arterioles: resistance vessels
thin compared to arteries but still muscular
significant pressure drop
major site of vasoconstriction/dilation
capillaries: sites of exchange of nutrients and gases
one cell thick
low pressure
thin walls for diffusion/exchange
venules (veins): blood reservoirs and return to heart
thin
very low pressure
valves to prevent backflow
why are arteries considered pressure reservoirs? explain elastic recoil
they store energy when the heart pumps and release it when the heart relaxes to keep the blood flow and pressure continuous
elastic recoil: ability of arterial walls to stretch and spring back due to their high content of elastic fibers
systole (heart contracts): blood is forced into arteries, stretching the arterial walls and storing energy
diastole (heart relaxed): arteries recoil (snap back) and stored energy pushes blood forward
describe how you measure blood pressure with a stethoscope and a blood pressure cuff. what indicates systolic pressure? diastolic pressure? what are korotkoff sounds? how do you calculate pulse pressure?
systolic pressure: 1st sound, maximum pressure when blood ejected into arteries
diastolic pressure: last sound, minimum pressure while blood drains
korotkoff sounds: auscultation of blood flow correlated with blood pressure readings
pulse pressure = systole - diastole
what is mean arterial pressure, and how do you calculate it?
MAP: average pressure in the arteries over one full cardiac cycle (important because it represents the pressure driving blood flow to tissues)
MAP = diastolic - 1/3 (systolic - diastolic) ← (or pulse pressure - same thing)
how does MAP change throughout the vascular tree?
arteries: highest MAP, high pressure
arterioles: huge drop in MAP due to high resistance (small radius) - protects capillaries from high pressure
low pressure (ideal for exchange)
venules and veins: very low pressure, approaches 0 mmHg near heart
why are arterioles considered resistance vessels?
their small, adjustable radius produces the greatest changes in resistance and blood flow, MAP drops significantly and pressure drop drives blood flow
what is vascular tone?
baseline level of constriction in blood vessels, normal diameter, established baseline vascular resistance
what is vasoconstriction?
decreased blood vessel radius via smooth muscle contraction
what is vasodilation?
increased blood vessel radius via smooth muscle relaxation
what are the intrinsic/local and extrinsic controls of arteriolar resistance, and thus the distribution of blood flow throughout the body?
review question 42 im confused
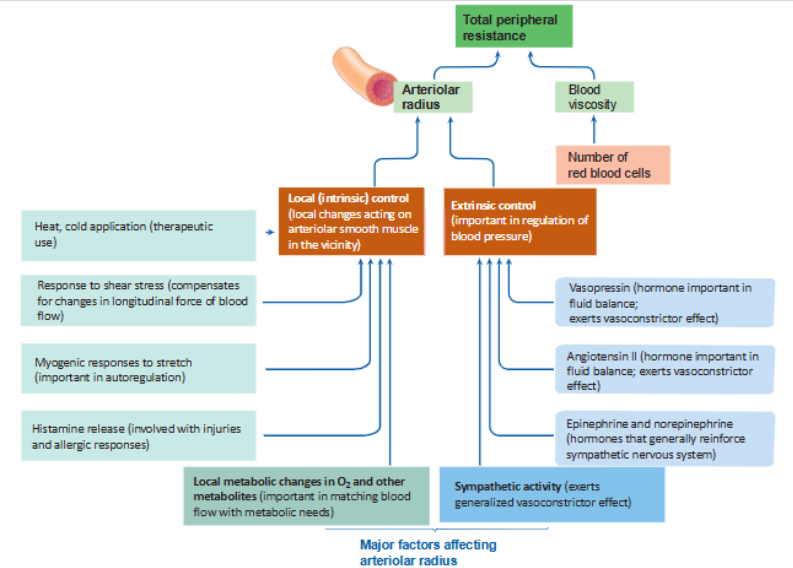
what is the difference between active hyperemia, reactive hyperemia, and myogenic autoregulation? understand negative feedback loops!
active hyperemia: increased blood flow to a tissue because the tissue is working harder
reactive hyperemia: increased blood flow that occurs after a temporary blockage of blood flow is removed
myogenic autoregulation: ability of blood vessels (especially arteries) to maintain constant flow despite changes in blood pressure & MAP
negative feedbacks: change disrupts homeostasis → vascular response → correction of that change
active hyperemia: corrects metabolic imbalance
reactive hyperemia: corrects oxygen debt
myogenic: corrects pressure changes
what is the main purpose of capillaries?
exchange of gases and nutrients
how does capillary structure inform their function?
vessel structure minimizes diffusion distances, narrow diameter makes red blood cells squeeze through single-file, extensive branching (capillaries touch ALL cells, maximizes surface area)
explain the change in flow rate vs flow velocity at each level of the vascular tree. how can capillaries have a decreased velocity of flow while maintaining the same blood flow rate?
explain capillary diffusion. how do different substances pass through capillary walls? what can pass through membranes, the pores, via vesicular transport, and what substances are usually excluded?
how do capillary beds open and close? what is the purpose of this?
what are the two processes that allow the exchange between blood and tissues across capillary walls? explain the difference
what hydrostatic and osmotic pressure differences drive bulk flow? which are the most important contributors?
how do you calculate net exchange pressure, and how does this determine the direction of bulk flow?
what are the functions of the lymphatic system?
why is the lymphatic system important for the functioning of the capillaries/maintaining composition?
how does the structure of the lymphatic vessels inform their function, and what happens when they aren’t working properly?
why are veins blood reserves?
how does veins structure inform their function?
how much of the total blood in circulation is typically found in systemic veins at a given time?
what is venous capacity and how is it determined?
what is the circulating blood volume?
what is venous return?
why is venous return important?
what are the many factors that enhance venous return?
what is the skeletal pump and how does it impact venous return?
how does the skeletal pump counteract the effect of gravity?
how do venous valves counteract gravity?
how do baroreceptors monitor mean arterial blood pressure and where are they located?
what is the series of events that occurs if MAP is above normal?
what is the series of events that occurs if MAP is below normal?