Kine305: Ch. 13 Shoulder Joint
1/38
Earn XP
Description and Tags
Exam 2
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
39 Terms
What movements are associated with the shoulder joint?
Flexion/Extension
Abduction/Adduction
Medial/Lateral rotation
Horizontal Abduction/Horizontal Adduction
Circumduction (moving through all planes)
Scaption (inbetween abduction and flexion)
Shoulder joint flexion ROM
0-180
Shoulder joint extension ROM
0-60
Shoulder joint abduction ROM
0-180
Shoulder joint adduction ROM
0, anatomical position
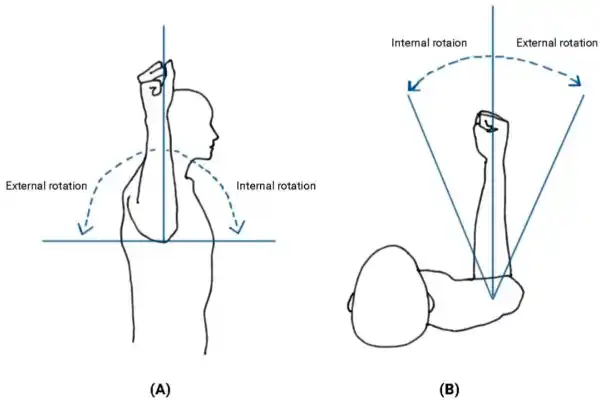
Shoulder joint medial rotation ROM
0-70
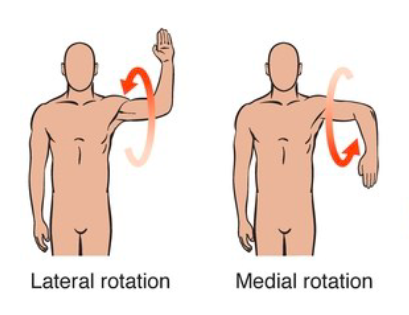
Shoulder joint lateral rotation ROM
0-90
Shoulder joint horizontal abduction ROM
0-30
Shoulder joint horizontal adduction ROM
0-120
What is the concave/convex relationship in a glenohumeral joint?
Convex on concave (think about how the humerus head is bigger than the glenoid fossa) also this means distal and proximal segments are moving opposite to each other
As you abduct the arm, you arm moves ___ and glides ___
superior and inferior
What is the primary arthrokinematic motion with flexion/extension?
spin
What is the labrum?
Fibrocartilage ring attached to the rim of the glenoid fossa, it deepens the fossa in a way to get more stability and encircles that glenoid fossa to provide more stability, also decreases friction on the joint surfaces and helps with shock absorption
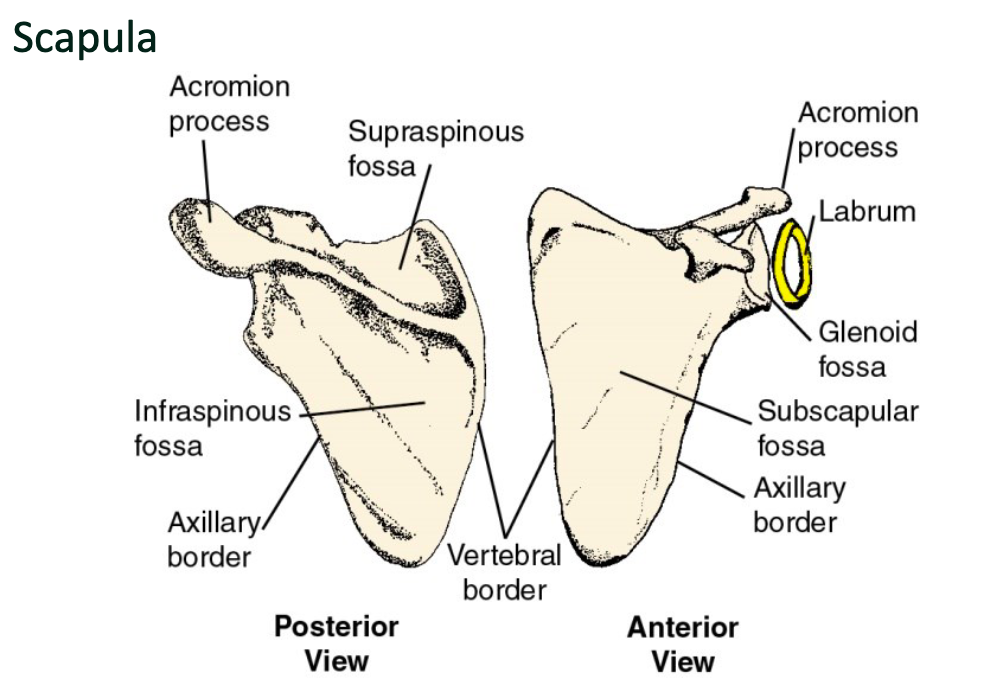
Bones and landmarks of the scapula
Acromion process
Infraglenoid tubercle
Supraglenoid fossa
Coracoid process
Glenoid fossa
Glenoid labrum
Supraspinous fossa
Infrasinous fossa
Axillary border
Subscapular fossa
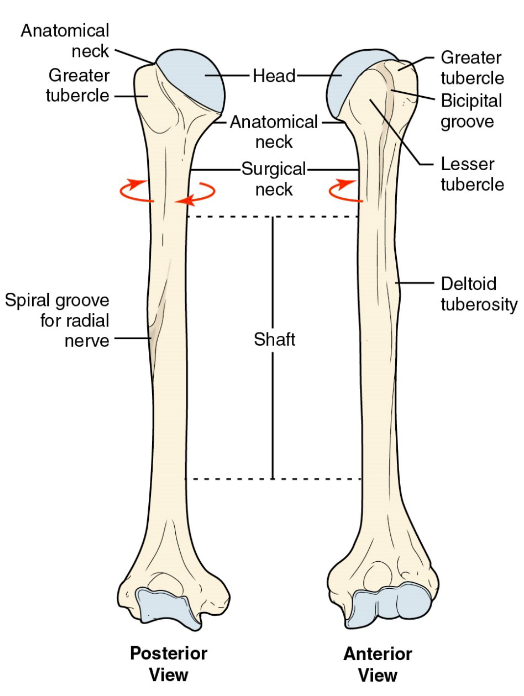
Bones and landmarks of the humerus
Head
Surgical neck (common surgical site)
Anatomical neck
Shaft
Greater tubercle (bigger, more posterior, where rotator cuff insertion points will be)
Lesser tubercle (more anterior, where rotator cuff insertion points will be)
Bicipital groove
Bicipital rides
What are the other ligaments and structures of the shoulder joint?
Joint capsule
Glenohumeral ligaments (superior, middle, inferior)
Coracohumeral ligament
Transverse humeral ligament
Coracohumeral ligament
Spans anteriorly from the corocoid process, medially to the humerus and reinforces the superior portion of the joint so is important for supporting the joint capsule
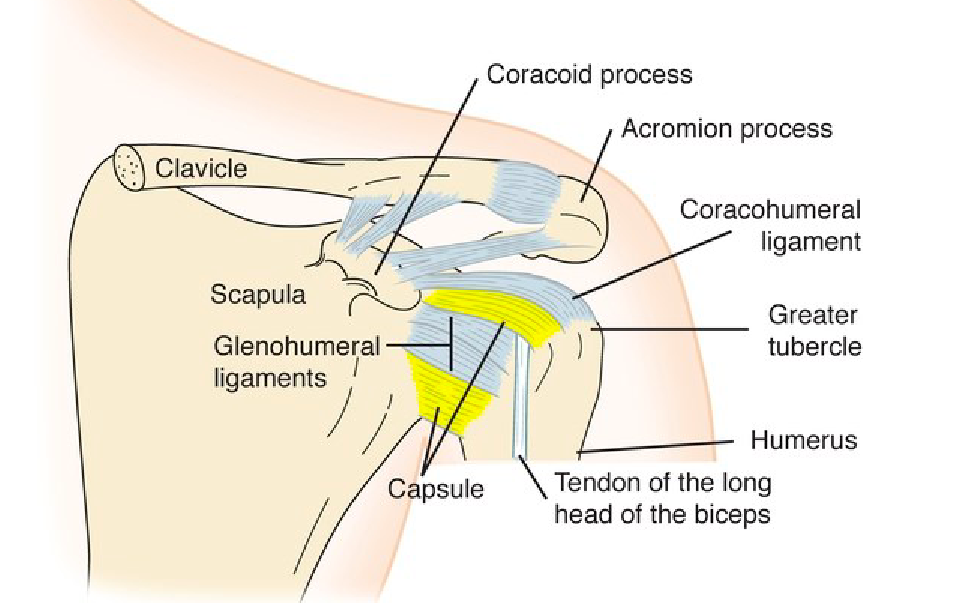
Transverse humeral ligament
Attaches to the tubercles and lip of bicipital groove and closes bicipital groove anteriorly, can click if there is a tear in the ligament which means tendon with a lot of force coming through it thats not staying in place, bumping all around so overtime wear and tear
Why do we need all of this in our GH joint?
Bc there is so much stuff that goes on in our GH joint, a lot of motion and force so you need all these structures to provide that secondary layer for stability
Bursa
Little sacs filled with fluid, shock absorbing and reduce friction based on where they are, the shoulder has a lot of them because there is a lot going on
Subdeltoid bursa and subacromial bursa
Serve the purpose of calming friction down and protecting the tendon from rubbing on the joint, better shelf life for those muscles
What is the close-pack for sternoclavicular and shoulder joint?
Full abduction and external rotation
What is close-pack?
When joint surfaces are closest together
What is the end feel for sternoclavicular and shoulder joint?
Firm
What muscles are innervated by the axillary nerve?
Deltoids and teres minor
What muscles are innervated by the musculocutaneous nerve?
corachobrachialis, biceps brachii, and brachialis
What are the muscles of the shoulder joint?
Deltoid (anterior, middle, and posterior portion)
Latissiumus Dorsi
Teres major
Pec major (clavicular and sternal portion)
Coracobrachialis
Rotator Cuff (SITS- supraspinatus, infraspinatus, teres minor, and subscapularis)
Where does the deltoid insert?
Deltoid tuberosity
Subscapulohumeral rhythm
Scapula has minimal movement through first 30 degrees of SJ abduction
Deltoid and rotator cuff
Force couple, deltoid is strong abductor and as we activate the deltoid, they will provide a superior force to the proximal end of the humerus. so without the rotator cuff, that humeral head would end up jammed in acromion process. rotator cuff is a big stabilizing force in GH joint.
Shoulder subluxation
common pathology, when head of humerus moves but not completely out of glenoid fossa
Shoulder dislocation
common pathology, when you have full seperation of bone out of socket, often need to put back in (primarily anterior bc of extension so falling on an outstretched arm)
Fractures
common pathology, neck, mid humeral (mostly twisting), and pathological (cancer, osteoporosis)
Impingement syndrome
common pathology, most common area is supraspinatus muscle and greater tuberosity (slumping and reaching forward, rotator cuff is being compressed under the acromion) so it will get irritated or inflamed
Adhesive capsulitis
frozen shoulder, not too known why it happens, restricted ROM, story about PT sister who saw patient in thawing phase and had him in flexion and it popped and made loud sound
Torn rotator cuff
tear as one or more tendons of the rotator cuff muscles (most commonly supraspinatus)
Labral tear
Tear of the glenoid labrum (fibrocartilaginous rim attached to the glenoid cavity), leads to shoudler pain, instability or mechanical symptoms, risk factors: athletes (baseball, volleyball), history of shoulder instability, causes: trauma, heavy lifting, sudden traction injury, overhead activity
Calcific tendinitis
like an overuse of the muscle, deposition of calcium hydroxyapatite crystals within a tendon, most commonly affects supraspinatus tendon of the rotator cuff, causes acute or chronic shoulder pain
Biceps brachii tendonitis
Inflammation (acute) of the long head of the biceps tendon, most commonly occur in the bicipital groove of the humerus, often associated with rotator cuff pathology