Lesson 2 DILATED CARDIOMYOPATHY ETIOLOGY AND PATHOPHYSIOLOGY
1/45
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
46 Terms
WHAT IS DILATED CARDIOMYOPATHY? what is it Characterized by and cannot be explained by what, name two examples of abnormal loading conditions?
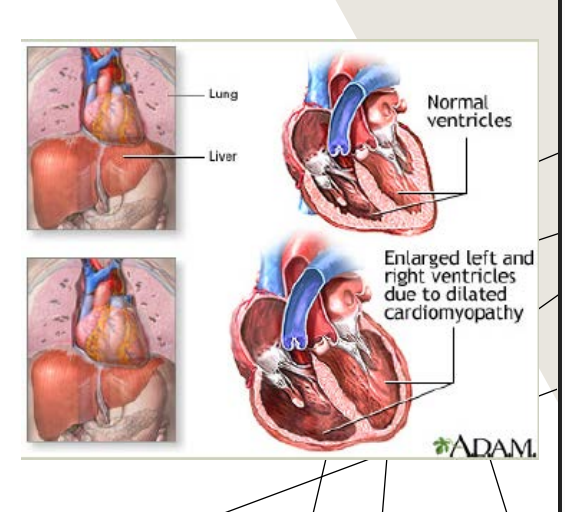
Dilated cardiomyopathy: “Characterized by LV dilation and LV systolic dysfunction that cannot be explained by abnormal loading conditions.” •
Hypertension •
Valvular heart disease
The definition is basically saying:
DCM is when the LV becomes enlarged and weak WITHOUT another condition causing extra pressure or volume stress on the heart.
So your teacher is saying:
If the LV is dilated because of long-term hypertension
Or because of valvular disease
…then technically the dilation may not be considered “primary” dilated cardiomyopathy, because there is another reason the heart got overloaded.
Simple breakdown:
Hypertension = pressure overload
The LV has to pump against high blood pressure for years → eventually weakens and dilates.Valvular heart disease = pressure or volume overload
Example:Aortic stenosis → pressure overload
Mitral regurgitation → volume overload
These conditions “load” the ventricle abnormally.
So when doctors diagnose true DCM, they try to make sure the LV dysfunction is not simply explained by:
chronic hypertension
severe valve disease
That’s why those were listed under the definition slide.
A super simple way to think about it:
Condition | Why LV dilates |
|---|---|
Primary DCM | Heart muscle disease itself |
Hypertension | Heart working against high pressure |
Valve disease | Heart overloaded with pressure or blood volume |
So the phrase:
“cannot be explained by abnormal loading conditions”
basically means:
“the weak, enlarged LV is not just from high BP or valve problems.”
That distinction is important clinically because DCM is a primary myocardial disease, not just a response to increased workload.
what classification is DCM in?
Primary cardiomyopathies, mixed ( can be both genetic and acquired)
what is the Idiopathic ETIOLOGY, and what is the % of cases?
Idiopathic – 50% of cases •
A disease of no known cause •
Not relating to any other disease process
what is the familial etiology and what % of the cases?
due too
what is more common
can be what or what
Familial – 25% of cases
• Hereditary •
Typically, autosomal dominant is more common •
can be recessive or X-linked
the etiology of the known causes of what % of the cases?
Known causes- 25% of cases
name 5 KNOWN CAUSES OF DCM
Infectious (viral, bacterial, fungal)
Immunologic (after vacation)
Metabolic/nutritional (transplant like the liver or kidney and can cause DCM b/c of regection)
Neuromuscular disorders (Muscular dystrophy)
Toxic (alcohol, cocaine use, chemothearpy agents)
EPIDEMIOLOGY:
The estimate for age-adjusted prevalence of DCM in the U.S. was _____cases over _______people
The estimate for age-adjusted prevalence of DCM in the U.S. was 36 cases over 100,000 people
It means that, after adjusting for differences in age between populations, about 36 out of every 100,000 people in the United States have dilated cardiomyopathy (DCM)
EPIDEMIOLOGY:
Updated estimate suggested a higher prevalence showing DCM ____ in ____individuals
Updated estimate suggested a higher prevalence showing DCM 1 in 250 individuals
EPIDEMIOLOGY:
If there is not clinically identifiable cause
what % of patients have a _____reason?
Over how many genes have been linked to DCM
25%-35% of patients have a genetic reason •
Over 50 genes have been linked to DCM
Sometimes doctors cannot find a clear reason WHY someone has dilated cardiomyopathy (DCM). But even when there is no obvious cause, genetics may still be responsible.
more than 50 different genes
that can lead to dilated cardiomyopathy.
Epidemiology means the study of incidence, distribution, and possible control of diseases
how common is DILATED CARDIOMYOPATHY?
The most common cardiomyopathy
Dilated cardiomyopathy is the what number most common cause of heart failure?
3rd most common cause of heart failure
Dilated cardiomyopathy is the most frequent cause of what?
Most frequent cause of heart transplant
H&P, name 6 (History and Physical)
Recent pregnancy
• Infection exposure •
Heart failure history? Symptoms? (SOB, swelling etc.) •
Palpitations •
Cyanosis •
Low blood pressure
CLINICAL PRESENTATION • Signs and symptoms name 6
Fatigue •
Decreased exercise tolerance •
Dyspnea (SOB)
• Orthopnea • (SOB while lying flat)
Paroxysmal nocturnal dyspnea • (SOB while sleeping)
Chest discomfort
PHYSICAL EXAMINATION- EVIDENCE OF LEFT HEART FAILURE name 4
Normal to low BP •
Pulsus alternans (severe left ventricular failure) (strong heart beat and next is small, heart rhytm doesn’t change, changes the strength if the heart beat tells us LV HF, can see this on EKG)
Tachycardia •
Lung crackles (pulmonary edema)
PHYSICAL EXAMINATION- EVIDENCE OF RIGHT HEART FAILURE name 4
Hepatomegaly (enlarged liver)
Elevated JVP • (Elevated jugular venous pressure (JVP) indicates increased pressure in the right atrium and venous system,)
Peripheral edema •’ (swelling in the legs,)
Ascites (abnormal buildup of fluid in the abdominal cavity)
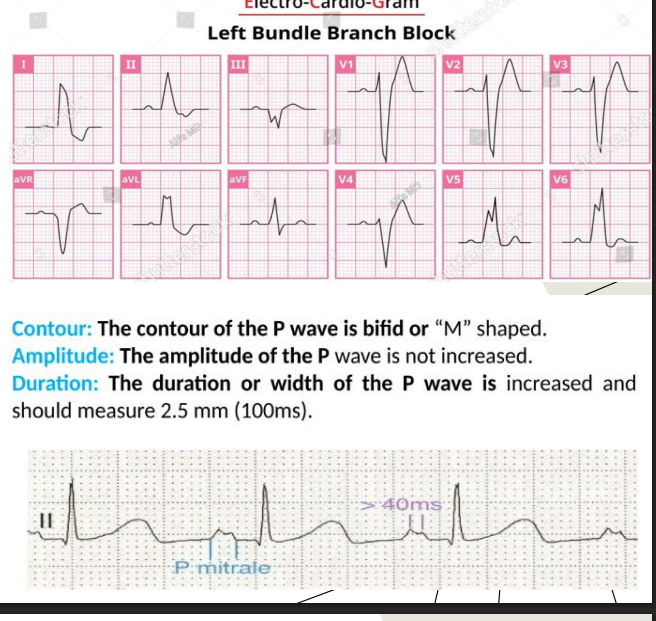
EKG name 6 and describe the p - wave
Sinus tachycardia •
Nonspecific ST-T wave abnormalities •
Atrial arrythmias or atrial fibrillation •
Ventricular arrythmias
• LBBB******
• Left atrial enlargement*****
the p-wave is long / the duration or width of the p wave is increased and the amplitude of the p wave is not increased
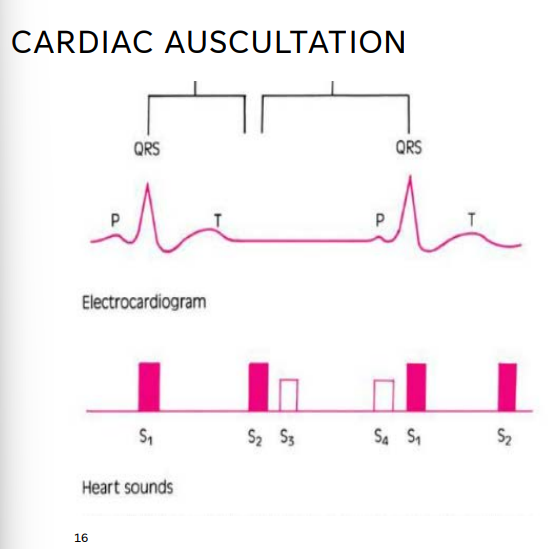
CARDIAC AUSCULTATION
paradoxical splitting of the second heart sound with _____
Accentuated pulmonary component of the 2nd heart sound of what present?
s_ and s_ with ventricular ______
systolic murmurs of what?
Paradoxical splitting of the second heart sound with LBBB
• Accentuated pulmonary component of the 2nd heart sound of pulmonary HTN is present •
S3 with ventricular decompensation •
S4 •
Systolic murmurs of mitral and tricuspid regurgitation
Paradoxical = occurring in the opposite or unexpected way from normal.
LBBB stands for Left Bundle Branch Block.
It means the electrical signal is delayed or blocked in the left bundle branch, so the left ventricle gets activated later than normal.
Normally:
Electrical impulse travels:
AV node → Bundle of His → Right & Left bundle branches
Both ventricles contract almost together.
With LBBB:
The right ventricle activates first
The left ventricle activates late
This causes the ventricles to beat out of sync.
Ventricular decompensation means the ventricle can no longer compensate well enough to maintain normal heart function.
In other words:
The heart muscle has become too weak or overstretched, and the compensatory mechanisms are starting to fail.
Normally, the second heart sound (S2) is:
A2 = aortic valve closes first
P2 = pulmonic valve closes second
During inspiration, they split a little:
“dub … dub”
With LBBB (Left Bundle Branch Block), the electrical signal gets delayed to the left ventricle.
That means:
the LV contracts later
the aortic valve closes later than normal
So now:
P2 happens first
A2 happens second
This reversed order is called paradoxical splitting.
explain the purposse for Genetic Testing/Labs
(guides what or identifies what?)
Guides treatment or identifies risk
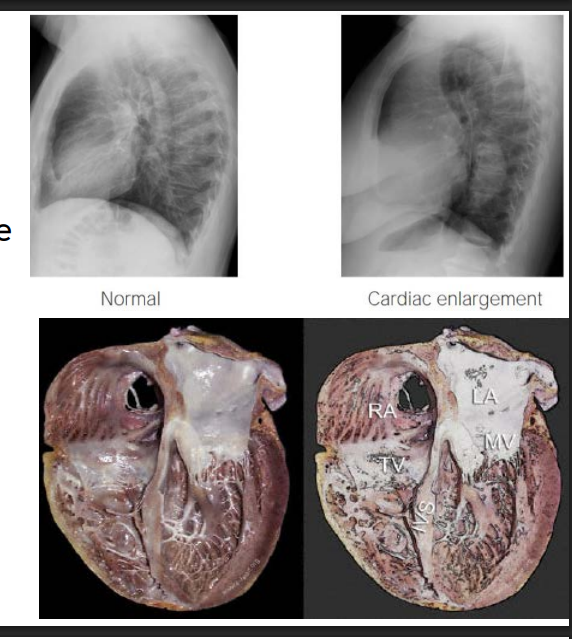
Chest X ray, what do you see
Cardiomegaly, pulmonary congestion
Cardiac Magnetic Resonance Imaging (MRI), used to assess what?
May be used to assess myocardial injury or inflammation
Cardiac Catheterization, evaluate for the presence of what? and what may be considered
Evaluate for the presence of CAD •
Endomyocardial biopsy may be considered
Exercise testing, may help to determine the cause of what?
May help determine the cause of exercise limitation
SYSTOLIC FUNCTION IN DCM
what are the determinants of ventricular function?
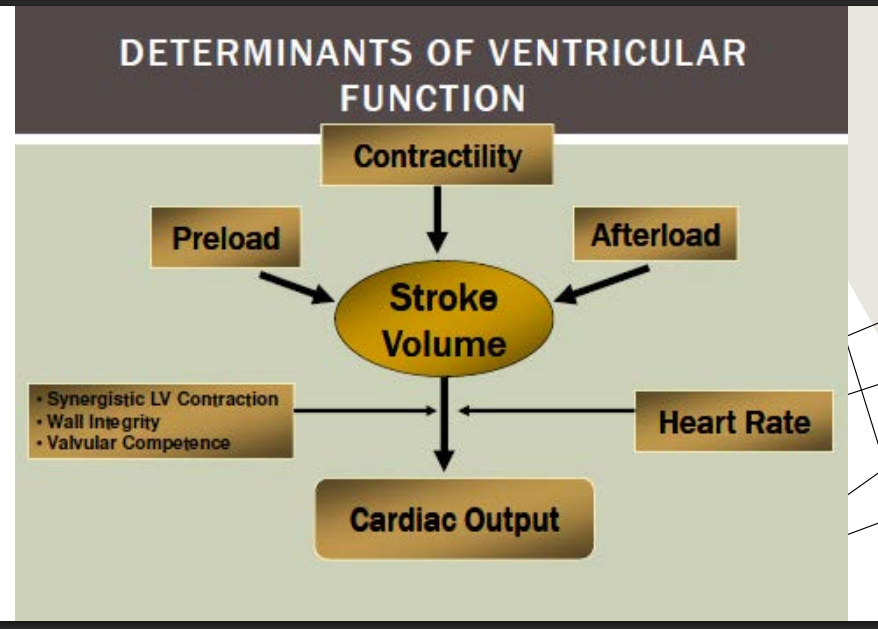
SYSTOLIC DYSFUNCTION, decreased in what 3 things, b/c of the decrease in ____ and ____ what does it cause?
what does it increases (name 4) and cause?
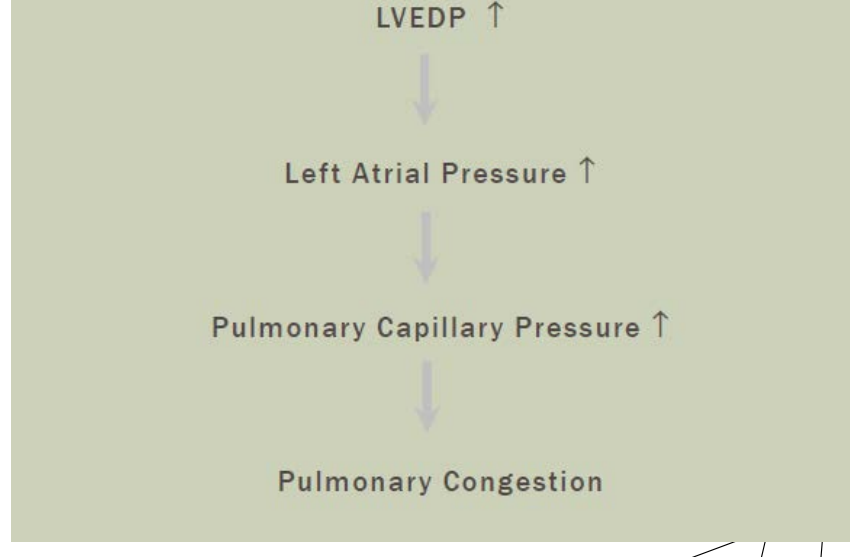
what happens to the LVEDP, LAP, pulmonary capillary pressure- leads to what?
Decreased myocardial contractility
Decreases cardiac output and SV
Because of a decrease in CO and SV…
Causes hypoperfusion to the organs
Increases in ESV, EDV, increased LVEDP/LAP
Pulmonary congestion
Hypoperfusion to the organs is a critical medical condition where blood flow is reduced or restricted, leading to insufficient delivery of oxygen, glucose, and nutrients to tissues.
what are the steps in LV dysfunction
what happens to the volume, pressure, myocardium, contractility, CO - what does it lead to, ESV, EDV- leads to what ? and what is the EF
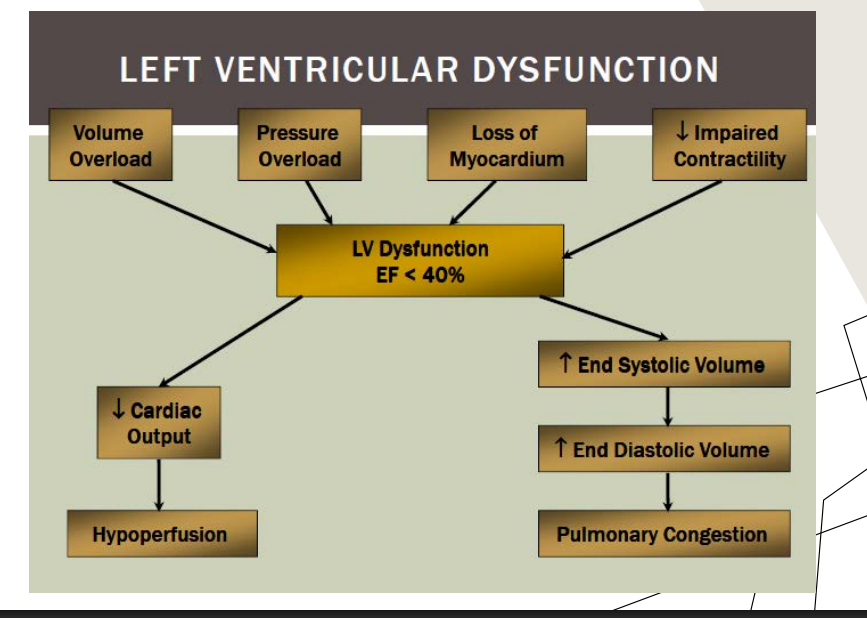
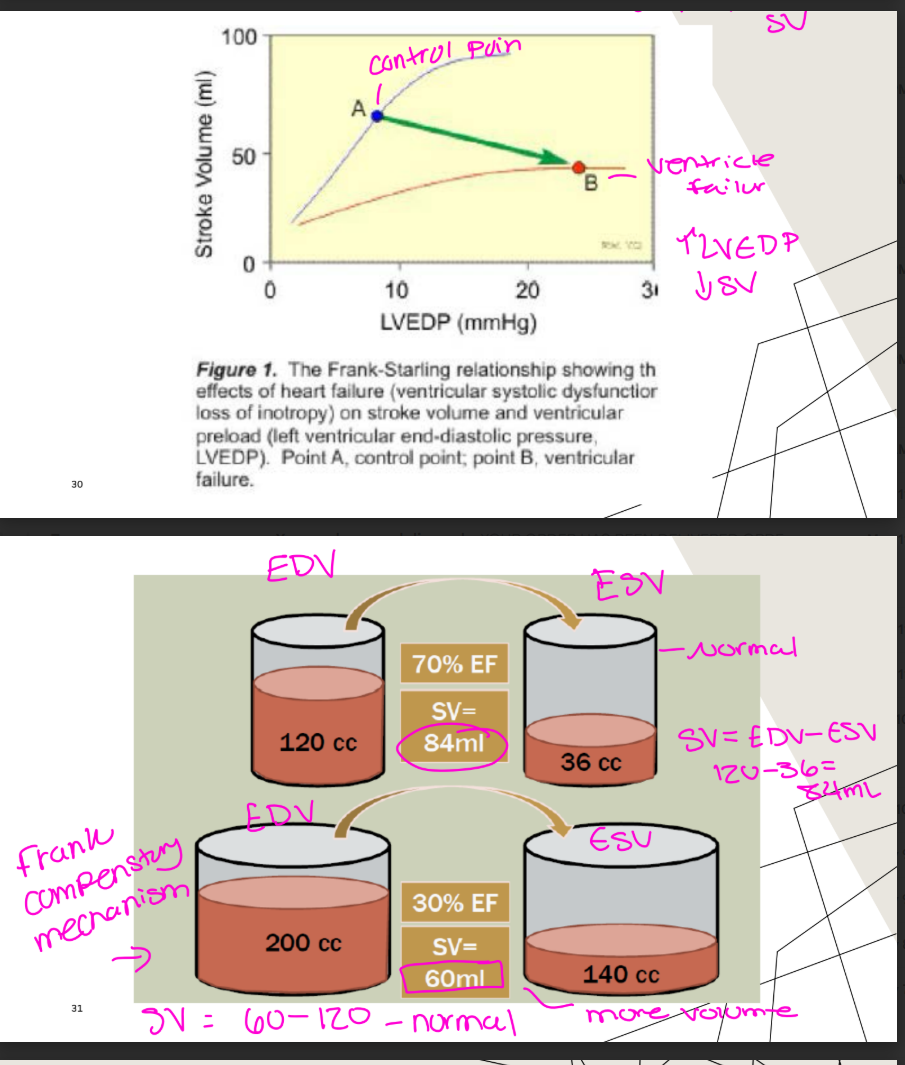
what 3 things VARIABLES DECREASED IN DCM?
Ejection fraction
Stroke volume
Cardiac output
(variables” just means the measurements/values that change in DCM.
So when the slide says “Variables decreased in DCM,” it means these important heart function numbers go down in dilated cardiomyopathy:
1. Ejection fraction decreases
The LV is weak, so it pumps out a smaller percentage of blood.
2. Stroke volume decreases
Each heartbeat pumps out less blood than normal.
3. Cardiac output decreases
Because stroke volume is lower, the total blood pumped to the body per minute can decrease.
Your slide lists these three as decreased in DCM: ejection fraction, stroke volume, and cardiac output.
Simple way:
Variable = measurable thing.
In DCM, the measurable things that decrease are EF, SV, and CO because the LV is dilated and weak.
COMPENSATORY MECHANISMS, how does the heart compenstate to maintain CO? name 3
Ventricular remodeling •
LV enlargement •
Frank starling relationship
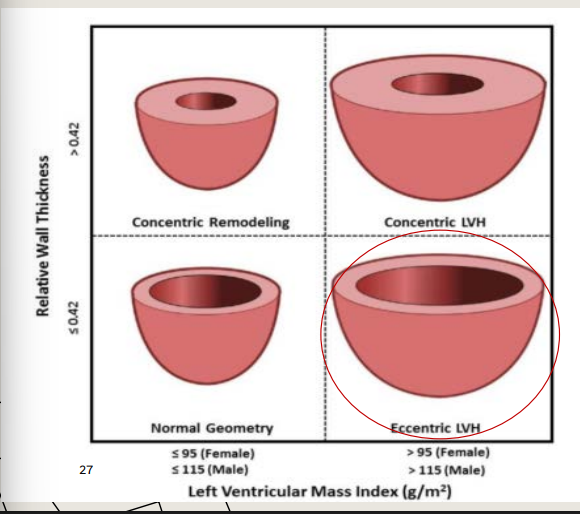
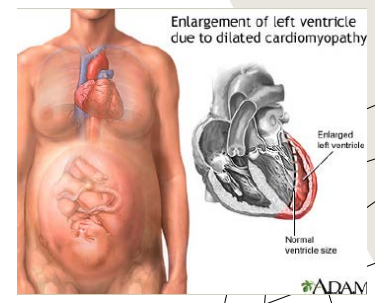
COMPENSATORY MECHANISM: VENTRICULAR REMODELING:
when you hear ventricular remodeling what are the 4 things you should be thinking of and name two things that increase in DCM for a compensatory mechanism? (think of walls too)
Size, shape, structure, function
LV mass
• LV enlargement
(Eccentric LVH, normal to thin walls - leads to cardiomegaly)
The more blood in, will =
^ causes what ?
producung what compensating for what function?
The more blood in, will = more blood out
LV ENLARGEMENT
Producing a higher stroke volume compensating for decreased systolic function
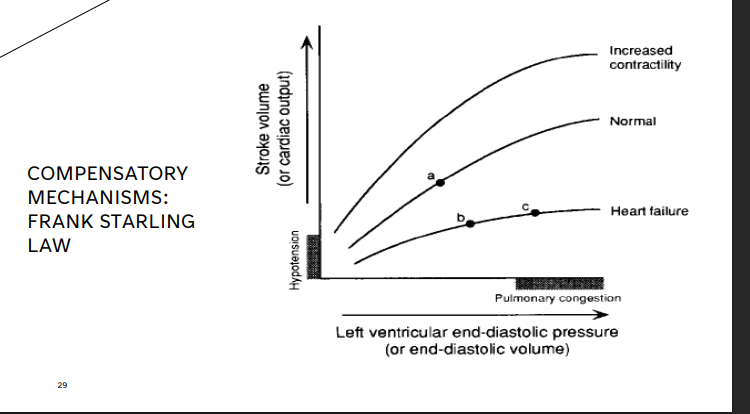
COMPENSATORY MECHANISMS: FRANK STARLING LAW
increase in what leads to stronger ____ and greater ____
increase in LVEDP leads to stronger contraction and greater SV
(when systolic function or contractility decreases in DCM the volume and the LVEDP will increase to help maintain that SV)
-point A normal, normal pressures, normal SV
point B shows a decrease in EF, if pressures and volumes arent increase the SV is very reduce and thats what point B is showing
point C shows a pt with cardiac remodeling done by increaing the pressures and volumes, the SV will increase for a little bit, mechanism works but eventually fails
WHY DIASTOLIC DYSFUNCTION OCCURS IN DCM, list two
LV dilation increases wall stress
Volume overload stretches the LV beyond optimal
LV dilation increases wall stress
the ventricle becomes what size and what shape?
what reduces diastolic compliance?
the LV fills at what pressures? (high or low)
The ventricle becomes large and spherical •
High wall stress reduces diastolic compliance •
The LV fills at higher pressures
Volume overload stretches the LV beyond optimal
what is going on with the preload?
what compensation becomes ineffective?
what does it result in?
Chronic preload elevation •
Frank-starling compensation becomes ineffective •
Results in LVEDP
Results in LVEDP”
LVEDP =
Left Ventricular End-Diastolic Pressure
That means:
pressure inside the LV at the END of filling.
Because:
too much blood stays in the LV
the LV is dilated and stiff
blood backs up
the filling pressure rises.
So:
LVEDP increases.
Simple Flow of What Happens
DCM → weak squeeze → blood stays in LV → preload increases → LV stretches too much → Frank-Starling stops helping → LV pressure rises (LVEDP ↑)
2025 ASE DIASTOLOGY ASSESSMENT IN DCM name 6
Mitral E/A ratio
Mitral TDI- relaxation velocity • - thats what it determines (DCM usally has a reduce septal and lateral e ‘ )
E/e’ ratio- estimates filling pressure • ( elavted filling pressures in DCM)
LA volume index (LAVi)- chronic pressure burden (huge LA)
• LA strain
TR (most likely will see in DCM) (b/c of the annulus being streatched)
in early DCM you may see imparied relaxtion, LV becomes more stiff and the LA pressure rise there might be psedu - normal or retricted filling pattern correlates with advanced HF
LA size is important, progonsis valve b/c LA size contribtes to the SV and dialation can change the SV, pt with LAE are prone to hospitalization and mortaility
what are primary cardiomyopathis?
inflammatory (myocarditis)
peripartum
what are secondary cardiomyopathis?
toxicity, drugs, heavy metals, chemical agents
consequence of cancer therapy
(Pathological myocardial involment as part to many systemic or multiple organ disorders that can lead to CV issues)
INFLAMMATORY (MYOCARDITIS) CARDIOMYOPATHY
________Cardiomyopathy presenting as DCM
AHA classification: is what?
Viral myocarditis can trigger what reaction that causes _______ damage to the ______?
___responsible overlap with that of DCM etiology
may be what?
can it be reversible ?if so how
Primary Cardiomyopathy presenting as DCM •
AHA classification: Acquired •
Viral myocarditis can trigger an autoimmune reaction that causes immunologic damage to the myocardium •
(commonly known as autoimmune myocarditis or inflammatory cardiomyopathy, occurs when the body's immune system mistakenly attacks its own heart muscle.)
Agents responsible overlap with that of DCM etiology •
(The things that CAUSE myocarditis are often the SAME things that can CAUSE DCM.)^^^^
May be acute or chronic •
May be reversible (medications, lifestyle changes etc.)
Acquired” means the condition is considered non-genetic (non-hereditary) and develops later because of something that happens to the person.
In DCM, an immunologic cause means:
the body’s immune system damages the heart muscle.
Sometimes this happens after:
a viral infection
inflammation
an autoimmune reaction
Example:
A virus infects the heart → immune system attacks the virus → sometimes it accidentally attacks the myocardium too → heart muscle becomes weak and dilated.
Your slide mentions:
“Viral myocarditis can trigger an autoimmune reaction that causes immunologic damage to the myocardium.”
Simple flashcard:
Immunologic
= caused by or related to the immune system damaging tissue.
Agents responsible = the causes (viruses, toxins, infections, etc.)
overlap = are shared/similar
DCM etiology = causes of dilated cardiomyopathy
So your teacher is saying:
Many causes of myocarditis are also causes of DCM.
Example:
Viral infection → myocarditis → heart muscle damage → can eventually lead to DCM
Alcohol/toxins → direct heart damage → DCM
Autoimmune inflammation → myocarditis and DCM
Person gets sick with a virus.
Like:
flu
COVID
bad infection
Step 2:
The immune system attacks the infection.
Normally this helps.
BUT sometimes:
the immune system also attacks the HEART muscle accidentally.
Step 3:
The heart muscle becomes inflamed.
Inflammation damages the myocardium.
Now the heart may:
weaken
enlarge
pump poorly
This can look like:
dilated cardiomyopathy (DCM)
Why Does It Become DCM?
When inflammation damages the muscle:
contractility decreases
EF drops
LV enlarges
So the patient develops:
systolic dysfunction
dilated ventricle
which is why myocarditis can PRESENT as DCM.
ETIOLOGY (CAUSE) of INFLAMMATORY (MYOCARDITIS) CARDIOMYOPATHY, name 3 which one is the most common?
CASE STUDY 35 yo F
Diagnosed with covid- 19 2/2021
Arrived at the hospital with respiratory failure
Echo performed 3/2021
whats the Diagnosis-?
Diagnosis- myocarditis and multisystem inflammatory syndrome secondary to covid-19

PERI/POSTPARTUM CARDIOMYOPATHY
Primary or secondary? Cardiomyopathy presenting as DCM •
AHA classification: what is it
explain what it is and the cause
Peripartum = around the time of delivery
Postpartum = after delivery
• Primary Cardiomyopathy presenting as DCM
AHA classification: acquired
Dilated form of cardiomyopathy
• Idiopathic
PERI/POSTPARTUM CARDIOMYOPATHY
when during pregnancy?
may occur in what women age’s?
most common after what age ?
what may be this be from?
is this reversible ?
Late in the 3rd trimester OR in the First 5 months after pregnancy •
May occur in childbearing women of any age •
Most common after age 30 •
May be from the stress of pregnancy (idiopathic cause) •
Reversible DCM
PERI/POSTPARTUM CARDIOMYOPATHY
what are the Risk factors? name 8
Obesity •
h/o other CV disorders • '
Certain medications •
Smoking •
Alcoholism •
Multiple pregnancies •
African American descent •
Poor nourishment
ALCOHOLIC CARDIOMYOPATHY
AHA classification: what is it?
due to what condition that involes what?
its from what? can this be reversible ?
consuming what per day and how many days risks developing what ?
AHA classification: Secondary •
Due to a systemic condition that involves the myocardium
• Toxicity •
May be reversible •
Consuming 6 drinks of alcohol per day > 5 days, risks developing asymptomatic DCM
Simple Way to Think About It Primary cardiomyopathy:
Problem starts mainly in the heart itself.
Secondary cardiomyopathy:
Something ELSE in the body damages the heart.
The heart problem is happening because of another disease or condition affecting the whole body.
Systemic condition = a disease/problem affecting the body overall.
Myocardium = heart muscle.
So:
“Due to a systemic condition that involves the myocardium” means:
A body-wide condition is affecting/damaging the heart muscle, causing cardiomyopathy.
CASE STUDY
09/2021- 36 yo M arrived to ED with LE edema
Hx drinking 30 pk beers/night from age 16 Viral panel negative
Follow up echo 1.5 years later after drinking cessation
ALCOHOLIC CARDIOMYOPATHY

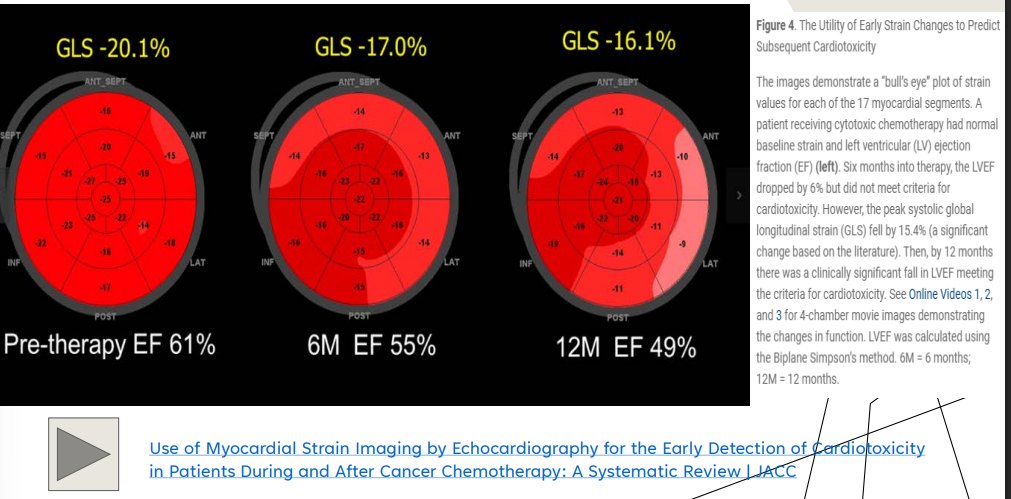
CHEMOTHERAPY CARDIOTOXIC AGENTS, some chemotherapeutic drugs may be what?
may occur when?
follow up every how many if what agent is utilized ?
what is very important to use/ check for this pt
Some chemotherapeutic drugs may be cardiotoxic
May occur during or even years after treatment
Follow up every 3 months if cardiotoxic agent is utilized (STRAIN)
(LV strain - predicts LV function and EF and important to check)
In DCM, cardiotoxic injury can weaken the myocardium so the ventricle dilates and systolic function decreases.
Simple definition:
Cardiotoxic = harmful to the heart muscle or heart function.