Small animal critical care nutrition 1 & 2
1/59
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
60 Terms
What is metabolic support?
Method to support metabolic status of hospitalised patients
What is the preferred method of critical care nutrition: enteral or parenteral?
Enteral (utilising GI tract)

If you administer parenteral critical care nutrition, what is an important factor to consider?
Food will not be digested / absorbed in regulated manner —> need to use elementary (basic nutrients) feed + in exact correct volumes & proportions.
Has to be delivered slowly
Has to be delivered to large vein such as jugular (smaller vein = could be damaged)
(only used if total failure of intestinal absorption)
What are the benefits of enteral nutrition over parenteral?
Easier
Fewer complications & lower risk of infection (sepsis)
Cheaper (than parenteral)
More physiological (stimulates GI tract pathways)
Why is malnutrition common in many hospitalised patients?
Animals in hospital typically already sick & struggle to compensate for food deficits → magnified nutritional deficiencies.
What are some examples where anticipation of need to feed would be necessary?
Facial trauma —> surgery? unable to move jaw?
Post surgery —> painful, slow recovery
Prostatic abscess —> if burst → abdo infection + sepsis → surgery + flush → not wanting to eat → increased nutritional need
Polyneuropathy —> paralysis
Megaoesophagus —> food cannot pass → gastrotomy tube needed
What are the 3 general rules for intervention w/ enteral nutrition?
Recent weight loss >10%
Partial/complete anorexia for ≥3 days
Diseases causing excess catabolism i.e. increased energy needs (e.g. diabetes mellitus, cancer, sepsis/infection)
(if one or more of these apply - act now!)
Why should obese patients receive the same level of intervention with enteral nutrition?
Obese patients, if not fed appropriately in hospital setting when ill, will typically metabolise lean body mass (muscle) much faster than their adipose tissue → myopathies etc.
What are the 4 main types of enteral feeding methods?
Encourage feeding
Force feeding
could put animal off wanting to eat for longer period → associates eating w/ nausea
could lead to aspiration pneumonia if not swallow → severe pulmonary dx
Drugs
Tube feeding
address why doesn’t want to eat —> pain?

List ways we can encourage feeding in veterinary patients
Privacy (e.g. separate ward for cats, towel over cage)
Comfortable environment (+ food bowls away from litter trays)
Give favourite foods in small amounts
Feed fresh & try warming
Do not 'overface' (don't worry about the amount @ start, just encourage to eat at all)
What types of diet are commonly given to encourage feeding in veterinary patients?
Formulated highly digestible diet
Cooked meat or fish
Formulated critical care diet
When encouraging feeding, what is an important thing to measure and record?
Total amount provided to patient
Total amount ingested by patient
(allows you to observe how many calories are being ingested by patient)
What drugs can we use to stimulate appetite?
Diazepam
Mirtazapine
Cyproheptadine (H1 antagonist)
Capromorelin (off licence —> imported + expensive)
What is the best appetite stimulant for cats?
Mirtazapine.
When should mirtazapine be used in cats?
For partial, short-term anorexia.
What are the different types of feeding tubes?
Naso-oesophageal tubes
Pharyngostomy tubes (no longer used due to delicate BVs & nerves → complications)
Oesophagostomy tubes
Gastrostomy/ PEG tubes
Enterostomy tubes

What type of tube should you use to provide feed from short to medium term (days to a couple weeks)?
Naso-oesophageal
(tube enters oesophagus only)
What are the advantages of the naso-oesophageal tube
No anaesthesia / sedation needed = cheap
Quick & easy to place
What are the contraindications to using a naso-oesophageal tube?
Patient needs gag reflex (able to swallow) to use
If patients have dx of head, pharynx & below
What are key limitations of naso-oesophageal tubing?
Tube is very narrow so can only provide liquid feed through it
Often bothers the patient as it has to be adhered to the face → to incidental removal
What type of tube should you use to provide feed from medium to long term?
Oesophagostomy tube (placed via small incision into oesophagus)
What are the contraindications of oesophagostomy tubing?
Diseases of the oesophagus or below.
What are the indications of oesophagostomy tubing?
Oral, nasal or pharyngeal disease.
What are the limitations of oesophagostomy tubing?
Requires GA to administer —> risk if you think patient will not survive anaesthesia
What are the benefits of oesophagostomy tubing?
Well tolerated c.f. other tubing methods
What tubing method is generally used of long term nutritional support?
Gastrostomy tubes (inserted directly into fundus of stomach)
What are the indications for gastrostomy tubing?
All but gastric, intestinal and pancreatic dx
What are the limitations of gastrostomy tubing?
Requires minimum 7 days placement —> takes time for body to seal off where site entry is & entry into fundus of stomach otherwise risk of leakage
GA required
What are the benefits of gastrostomy tubing?
Well tolerated generally
Wider indications compared to all other tubes
What tubing method is good to use if a patient has pancreatitis?
Enterostomy tube (inserted direct to SI)
What are the limitations of enterostomy tubing?
GA required
Contraindicated in diffuse intestinal disease
Need constant rate of infusion (as stomach as reservoir lost)
Costly & problematic
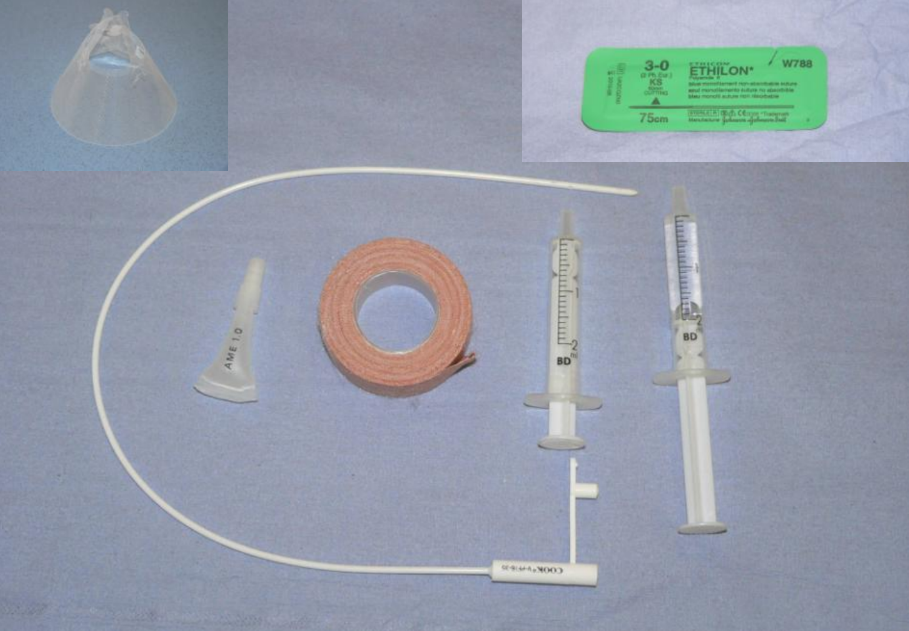
What equipment is needed for a naso-oesophageal tube placement?
Topical LA —> placed in nares before placement
numb nasal passages
give ~ 10-15mins to work
Silicone tube —> less traumatic, but can be pulled out by patient (slippery)
Suture material
Tape
Empty syringe + water syringe
Buster collar
How long should a naso-oesophageal tube be?
Measure before placing:
Nose to 9-10th rib or 3/4 of nose to caudal rib.
Mark with pen how far in

Where should the tube be directed when placing a naso-oesophageal tube in cats?
Ventromedially (aiming for the ventral meatus).
Steady head (hand on top of head & under chin)

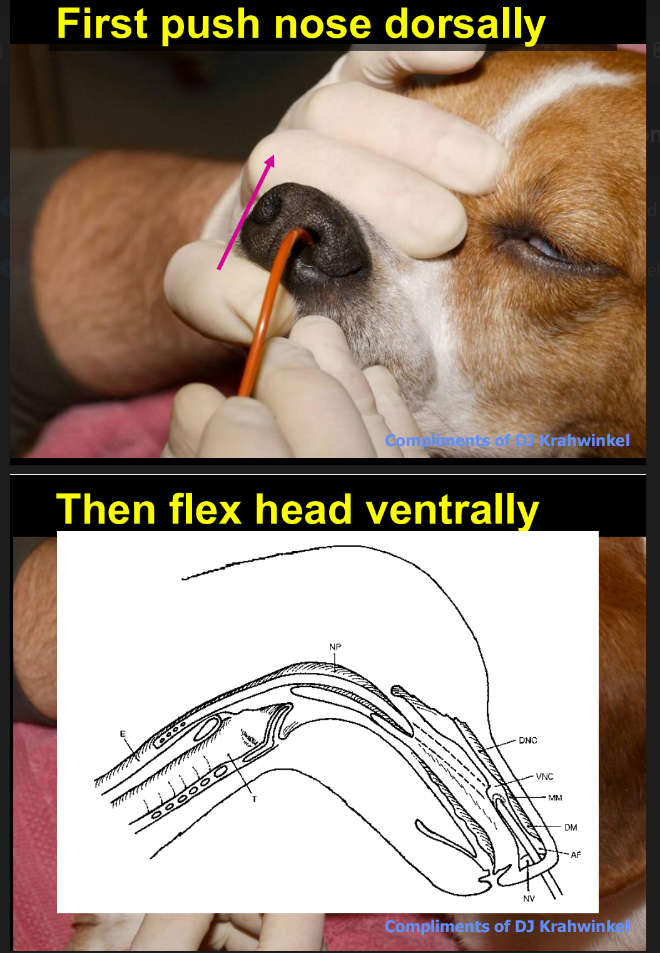
Where should the tube be directed when placing a naso-oesophageal tube in dogs?
Push nose dorsally to align outer & inner passages (alar cartilages) before placing tube
Then flex head ventrally
Then direct ventromedially (as in cat)
should be no resistance & pass smoothly
What signs would indicate that you have placed the naso-oesophageal tube correctly i.e. in oesophagus & not trachea?
Administer water → should have no cough reflex
Vaccum created in empty syringe (due to no air) —> -ve pressure
(Radiographic confirmation only if unsure)
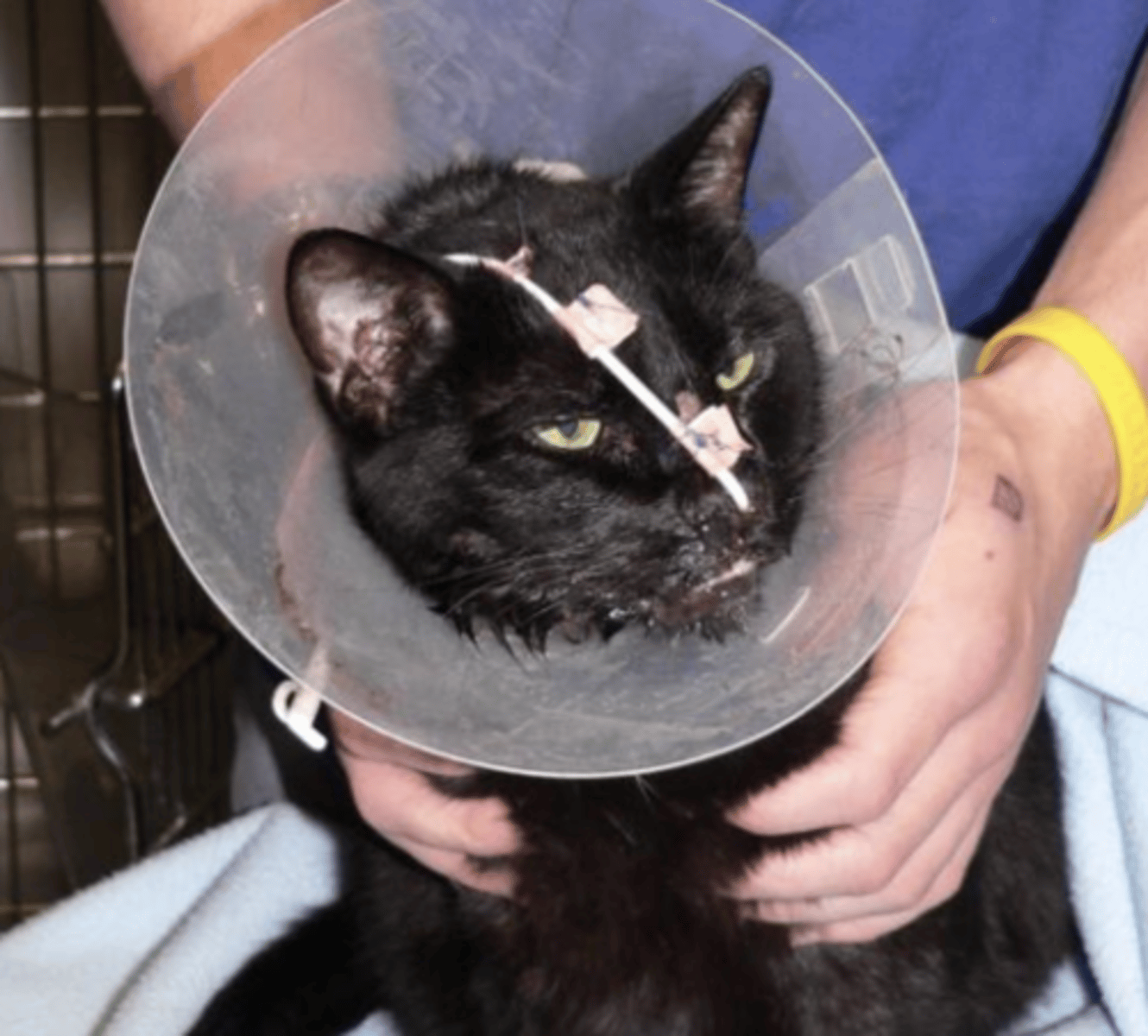
What can we use to secure a naso-oesophageal tube? How?
Use butterfly clips + suture the tube as close to the nares as possible and then one to the forehead —> limits amount of slack before entering nose —> harder for patient to dislodge
(do not use super glue —> will remove part of skin & hair)
(can use staple gun as alternative)
(can use suture material passed through needle)
What side of the body should an oesophagostomy tube be placed in?
Right or left lateral neck.
(preferrably left —> oesophagus closer to skin on L)
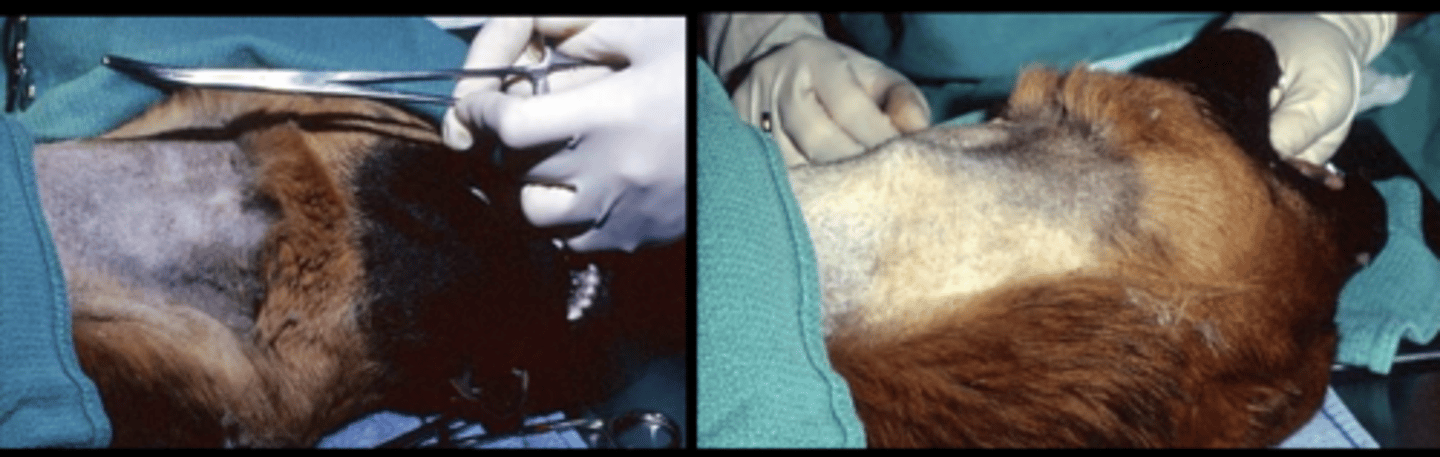
How should you place an oesophagostomy tube?
GA, clip & prep patient
Use carmalt forceps to measure length
(use longest carmalt forceps possible)
Insert forceps & push out laterally
direct tips outwards so shows up under skin
Incise skin over forceps, force tip through —> not too big a hole (risk of infection / leakage)
Advance out through mouth
Reverse tube & pull slack of tube out through skin end then advance downwards as far into oesophagus as poss

How is oesophagostomy tube placement confirmed?
Use radiography to confirm placement in oesophagus and NOT trachea —> under GA so won’t cough if fluid put down tube + air presence
What does an oesophagostomy tube have that may be problematic?
Solid bung —> shows up on radiograph
Risk of blockage so can be cut off


When applying an oesophagostomy tube, what is an important structure to avoid?
Jugular vein.

How do we secure an oesophagostomy tube to the skin?
Use fingertrap pattern and suture to skin
Apply dressing and bandage to neck with tube entrance pointing dorsally

How is a PEG (Percutaneous Endoscopic Gastrostomy) tube placed?
Find fundus
Hypodermic needle pushed through skin
Wire / suture material placed through, pulled on by forceps through mouth (endoscope guided)
endoscope confirmation of placement

What is the resting energy requirement (RER) equation for dogs?
30 x BW + 70
What is the energy resting requirement equation (RER) for cats?
40 x BW
What energy doesn't the RER accompany for?
Thermoregulation, activity.
How do you adjust the RER regularly?
Weigh patient regularly & adjust accordingly based on change in weight
How do we work out caloric density of food?
(3.5 x % protein) + (8.5 x % fat) + (3.5 x % carbohydrates)
How do we work out amount of food needed for a patient?
Energy required by patient divided by caloric density of food
(introduce food gradually over 3-5days)
Which tubes can we not start feeding straight away (must wait 24 hours)?
Gastrostomy tube
Enterostomy tube
give time to seal tube off at entry points
Which tubes can we begin feeding immediately?
Oeosphagostomy tube
Naso-oesophageal tube
How much feed should be given on day 1?
1/3 of feed required.
How much feed should be given on day 2?
2/3 of feed required.
How much feed should be given on day 3?
3/3 of feed required.
How many times a day should a meal given via a feeding tube be administered over?
4-6 times per day
Describe the basic principles of how you should tube feed animals
Always aspirate first (w/ empty syringe to ensure nothing is in stomach/oesophagus —> if so, minus amount left in tube from prev. meal from meal about to feed)
Warm food
Administer over several mins
Flush tube w/ warm water —> otherwise could dry out & block tube
When do we stop tube feeding?
With voluntary intake of at least 85% basal energy requirement
or longer if patient likely to suffer relapse
What nutrients need to be considered?
Fluid & electrolytes
Energy requirements
Protein ± specific amino acids
Micronutrients
What are some complications with feeding tubes?
Mechanical blockage
carbonated beverage can help clear
GI upset
Hypophosphataemia —> re-feeding syndrome if deprived from food for significant amount of time —> INTRO FEED SLOWLY + GRADUALLY
Tube dislodgement → peritonitis
Stoma infection
Tube removal by patient