Endocrine: DM Types 1 & 2, Hypoglycemia, DKA, & Diabetic Emergencies (HHS, DI, SIADH )
1/101
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
102 Terms
normal glucose fasting
70-99 mg/dL
glucose intolerance
100-125 mg/dL
what BG level indicates diabetes
> or equal to 126 mg/dL
insulin is the
key
it opens the door to let glucose into the cells
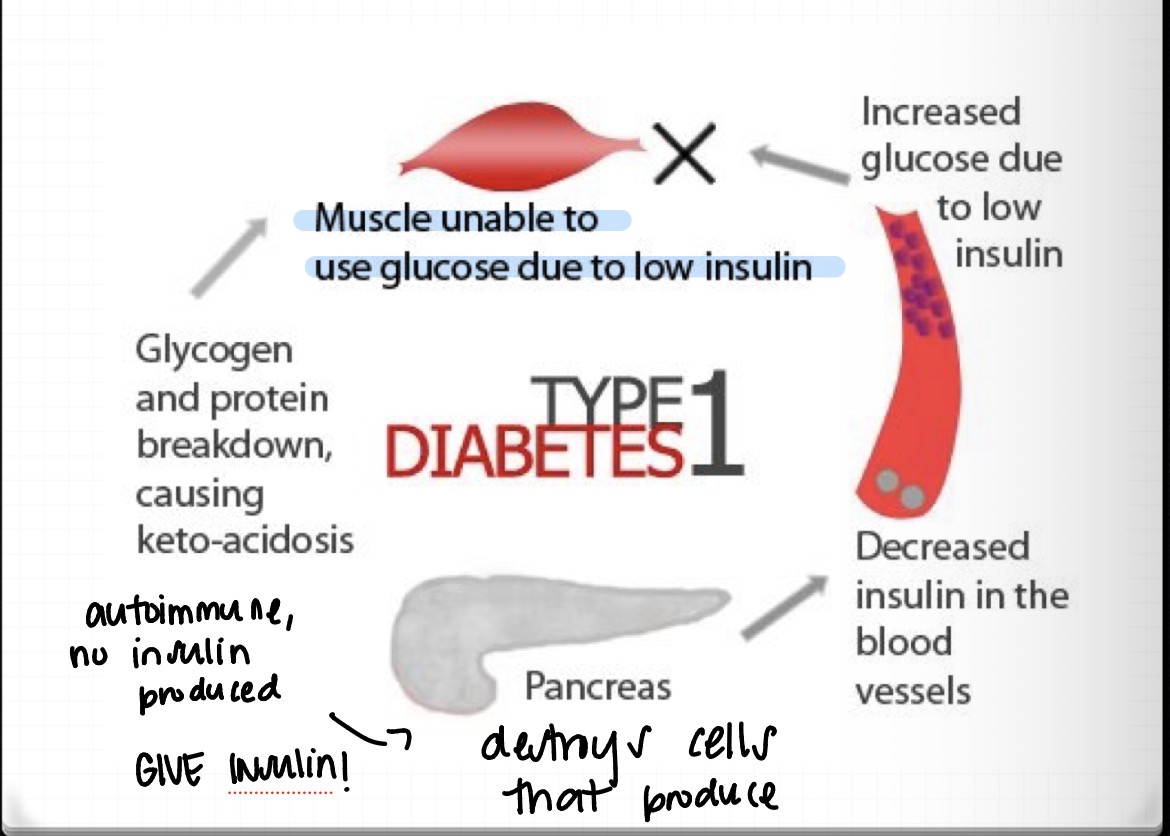
type 1 DM
autoimmune disease
no insulin is produced
the pancreas destroys cells that produce it
WE WILL GIVE INSULIN
type 1 DM continued
muscle unable to use glucose due to low insulin
increased glucose due to low insulin
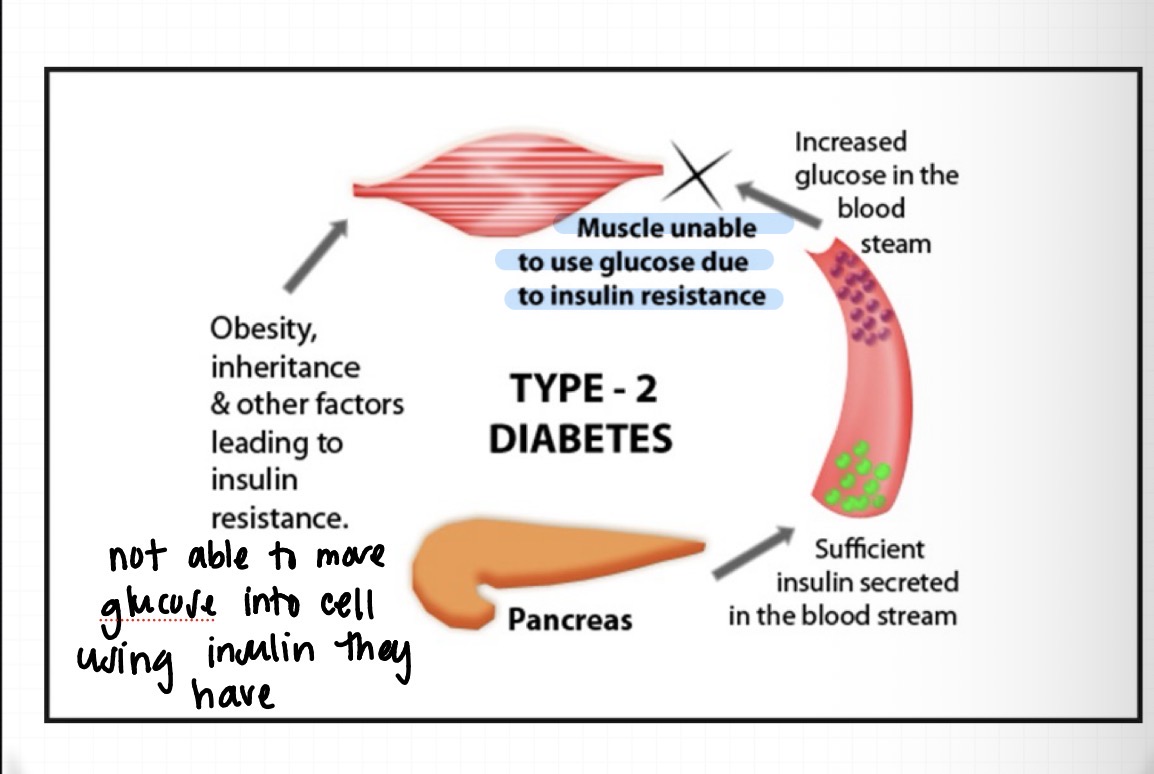
type 2 DM
not able to move glucose into the cell using the insulin they have
obesity and other factors that lead to insulin resistance
DM symptomology
3 p’s (usually seen more with >200 BG, glucose pulls water with it and glucose spills into the urine)
polyuria
polydipsia (thirsty)
polyphagia ( eat more since cells are starved)
fatigue
muscle cramps
nausea
headache
GLUCOSE CANT MOVE INTO THE CELLS
treatment for type 1 DM
must HAVE INSULIN
combo of short and long acting
diet, exercise, infection vigilance !!!!!
glucose is a
chemical irritant
—> causes vascular damage to the eyes, kidney, brain
type 2 DM treatment
weight loss/control
diet, exercise
oral agents + insulin
Metformin (decreases how much glucose is is absorbed from food)
type “1.5” DM (mix of both symptoms)
combo meds, diet, exercise, and weight control
SICK DAYS
foot care
cardiac care
kidneys
rapid acting insulins are
Lispro (humalog)
aspart (novolog)
glulisine (apidara)
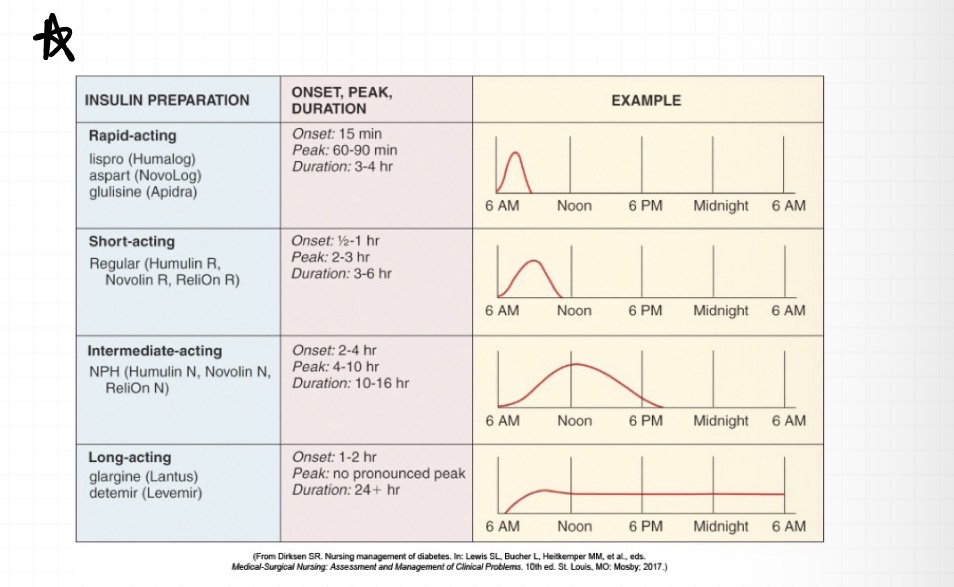
rapid acting insulins onset
15 minutes
rapid acting insulin peak
60-90 minutes
short acting insulin’s are
regular (humilin, novolin)
short acting insulin onset
30 min-1hr
intermediate acting insulin are
NPH (humulin N, Novolin N)
intermediate acting insulin onset
2-4 hrs
long acting insulin are
glargine (lantus)
determir (levemir)
long acting insulin onset
1-2 hrs
patient education for DM
Disease process
which type they have
lifestyle changes
activity, diet, need for care
Meds
importance
actions, dosing, how to
foot care
cardiac consideration
patient education continued
SICK DAYS
Ideally, instructions from health care provider
Often mistakenly think less insulin / meds needed
Need closer monitoring
Fingersticks more frequent
Insulin
Use rapid / short acting, no long acting
Pump – ensure proper functioning
Oral agents
If tolerant, per instructions from HCP
Consider calling primary when become ill
Continued nausea / emesis – seek medical care
pancreatic disorders in the critically ill patient
Stress-induced hyperglycemia
Diabetic ketoacidosis (DKA)
Hyperosmolar hyperglycemic state (HHS)
Hypoglycemia
stress induced hypoglycemia risk factors
Diabetes (diagnosed or undiagnosed)
Advancing age
Administration of exogenous catecholamines (epi/noepi)
Glucocorticoid therapy
Enteral or parenteral nutrition therapy
Medications
Obesity
Pancreatitis, cirrhosis
adverse effects of DM
Immune suppression
Cerebral ischemia/stroke
Dehydration/osmotic diuresis
Impaired wound healing
Endothelial dysfunction/thrombosis (stroke, clot, DVT)
Decreased erythropoiesis
Impaired gastric motility
clinical managment
Establish euglycemia
Target glucoses of 140 to 180 mg/dL
Insulin protocol (SUBQ or Drip)
stress and critical illness
Hyperglycemia
Excessive hepatic glucose production
Relative hypoinsulinemia
Adrenal insufficiency
Primary and/or secondary dysfunction
Thyroid dysfunction
hyperglycemia crises
Reduction in circulating insulin with concurrent elevation of counterregulatory hormones
Occurrence
DKA: Type 1 diabetes
HHS: Type 2 diabetes
Increasing incidence of both DKA and HHS in
same patient
type 2 DM can also get DKA
DKA
Bottom line issue:
absolute or relative insulin deficiency
Far more frequent v HHS, BUT HHS has higher mortality
Triggers – more frequent:
New onset diabetes
Infection / acute illness
Medication non – compliance
Increase in counterregulatory hormones: glucagon,
cortisol, catecholamines, and growth hormone
what is DKA
glucose is really high, can’t move glucose into cells , can’t burn glucose since theres not enough insulin —> burn fat
DKA s/s
exacerbated s/s of DM
ABD pain
hypotension
altered LOC
shock
coma
METABOLIC ACIDOSIS = CNS depression & CV collapse
burn fat—> ketones (acidotic)
Kussmual breathing (big deep and rapid breaths) to try and blow CO2 off
fruity breath
flushed dry skin
3 P’s
BG usually >250 mg/dL
HIGH ANION GAP acidosis (inadequate bicarb
SEVERELY DEHYDRATED
how is DKA treated
insulin drip and fluids
three biochemical problems in DKA
hyperglycemia
ketonemia
high anion gap metabolic acidosis
once pts BG is >200 will have glycosuria (glucose in urine) and will pull fluid pts become SEVERLY DEHYDRATED
DKA treatment
regular insulin drip
fluids
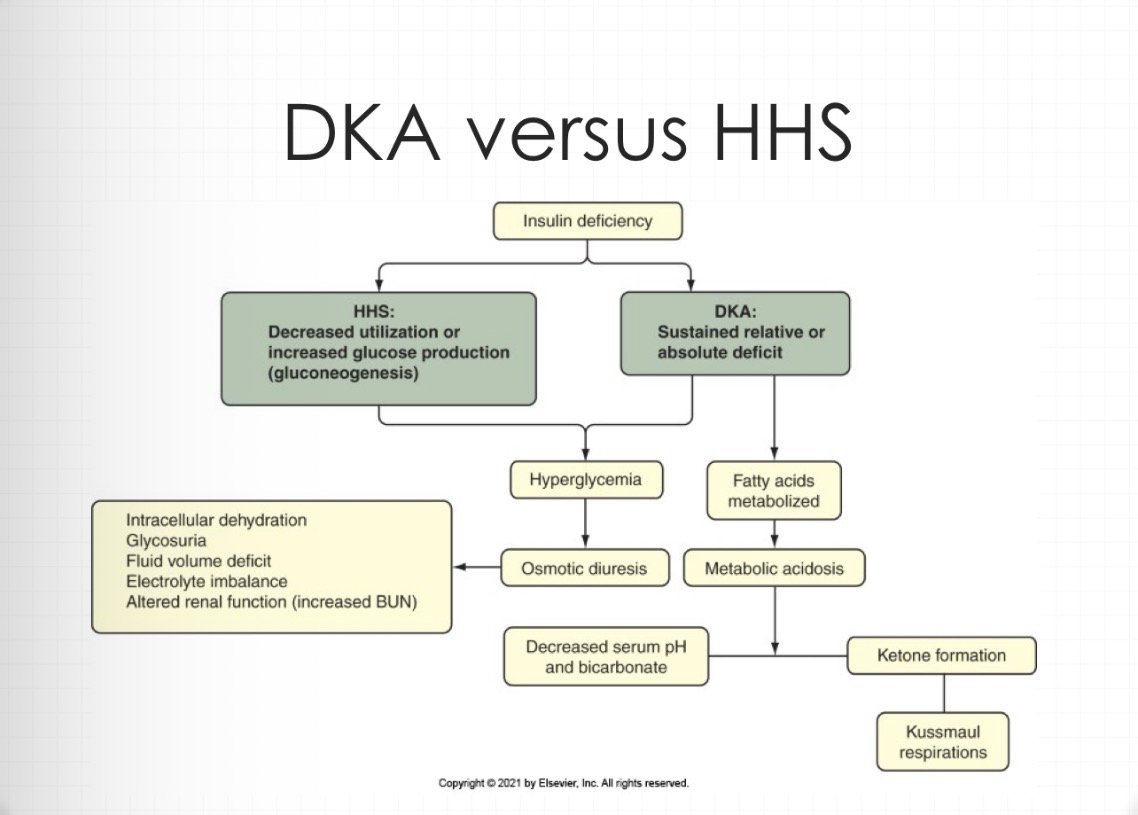
physiological changes in DKA
Hyperglycemia due to increased glucose production and decreased utilization
Osmotic diuresis and dehydration
Hyperlipidemia due to increased lipolysis
Metabolic acidosis/ketosis
Altered potassium balance (increased from acidosis, will actually be LOW, from K+ shifting in cells, replace)
Excess acids result in increased anion gap
Altered consciousness related to acidosis and
dehydration
fluid and electrolytes changes in hyperglycemia emergencies (DKA and HHS)
The clinical presentation of hyperglycemic
emergencies (DKA and HHS) is a product of
fluid volume losses related to osmotic diuresis
caused by hyperglycemia, ketosis (DKA), and
respiratory losses (DKA).
Sodium, potassium, and phosphate losses may accompany fluid losses.
K+ will initially be high, actually low need to correct and replace
BUN and Cr elevated (secondary to dehydration)
phosphate depletion (by insulin)
mild hyponatremia
hyperglycemia is
greater than 250
causes:
↑ gluconeogenesis
↑ glycogenolysis
↓ glucose use by cells
Glycogenolysis → 0 glycogen catabolized to lactic acid
ketonemia
elevated ketones= ketosis
Decreased insulin availability →
Decreased glucose transport into cells →
Cellular “starvation” →
Body uses other sources for energy
Fat breakdown produces fatty acids →
FA oxidized to ketones → ketonemia / ketosis
Ketones: β– hydroxybutyrate & acetoacetate
anion gap
evaluates bicarb
Difference of positive and negative ions
Cations (+) and anions (-)
Na+ ‒ (HCO3 ‒ + Cl ‒)
Normal £ 12
Elevated = metabolic acidosis
sodium and chloride will stay about the same
bicarb will be low
anion is high
an anion gap that’s >12 is considered what
open
DKA BG
usually >200 can reach up to 600 mg/dL
Serum β– hydroxybutyric acid, acetone (ketones)
DKA ABG’s
Mild: pH £ 7.3, HCO3‒ £ 15
Severe: pH £ 7.0, HCO3‒ £ 10
DKA electrolytes
K+: usually high, BUT NOT ALWAYS!
Na+ and Cl‒ : low / normal
CO2: low (normal 22 – 26)
DKA anion gap
Mild: high end normal, 10 – 12
Severe: above normal, > 12 (open)
why would we get a CBC with WBC and diff, UA, cultures in DKA
looking for infection
DKA diagnostics
Cardiac monitoring, 12 lead EKG
Chest x-ray
Pneumonia
Atelectasis
KUB
Free air
Obstruction
CT, MRI – possible,depending on initial findings
complications of DKA
Hypoglycemia
Hypokalemia
Alkalosis
Hypotension (dehydration)
Aspiration / pneumonia
Cerebral edema ( if corrected to fast)
Sepsis / septic shock
difference with DKA and HHS
NO KETONES ARE PRODUCED
can still move some glucose in the cells
in nclex world more seen in Type 2 DM
HHS
Hyperglycemia
Dehydration
Hyperosmolarity
Incidence
Less than 1% of diabetic related hospitalizations
More common with Type II DM
BUT…mortality upwards of 15%
More common in elderly, possible AMS
Often develops over several days to weeks
May have ketosis…if so, usually mild
sugar can get well over 600 mg/dL
HHS patho
Decreased use of glucose and/or increased
production
Hyperglycemia; increased extracellular
osmolality
Osmotic diuresis
Profound dehydration
No ketoacidosis—hyperglycemia with
hyperosmolarity blocks lipolysis (this is the difference with DKA)
HHS etiology
Inadequate insulin secretion, usually with type 2 diabetes
Often in geriatric patients with decreased
compensatory mechanisms
Stress response
meds
Affect blood glucose levels
Thiazides
Phenytoin (seizures)
Glucocorticoids
Beta blockers
Calcium channel blockers
Enteral and parenteral nutrition
HHS triggers
infection
new onset DM
med noncompliance
HHS s/s
early profound polyuria and polydipsia
profound dehydration
AMS
comorbidities: HTN, thyroid, PSH
HHS glucose
can be around 800 mg/dL
HHS osmolarity
>320 mOsm/kg
blood has no water but LOTS of sugar
HHS electrolytes
increased Na+
increased glucose
increased BUN
increased Cr
anion gap <12, wont be as acidic like DKA
HHS ABG
pH >7.3
HCO3- normal or slight elevation
HHS potential complications
Hypoglycemia
Ensure glucose added to IV fluid appropriately
Hypokalemia
Follow labs, replace as needed
Hypervolemia
Clinical assessment, may need CVP monitoring
Vomiting – aspiration
May need Salem sump to suction
Cerebral edema
Avoid rapid drop in serum glucose
HHS
blood sugar > DKA
more “normal” ABG , no changes or little ones
More electrolyte imbalances and renal
dysfunction
Higher serum osmolarity than DKA
Ketosis absent or mild
DKA & HHS interventions
Manage airway (DKA and HHS)
Fluid replacement (DKA and HHS)
First use 0.9% NS, then 0.45% NS (1/2 NS)
Dextrose added when glucose approaches 200 mg/dL
Monitor closely for signs of fluid volume overload and cerebral edema
DKA & HHS interventions
Insulin therapy (DKA and HHS)
Fluid replacement initiate first; monitor K+
Loading dose (not in children)
Continuous infusion
Hourly glucose monitoring
Decrease glucose by 50 to 75 mg/dL/hr
When glucose is less than 200 mg/dL, adjust infusion to maintain values of 150 to 200mg/dL (add dextrose)
DKA & HHS interventions continued
Insulin therapy – transitioning to subcutaneous therapy
Blood glucose < 200 mg/dL
two of the following criteria met to transition to SQ insulin
Blood glucose < 200 mg/dL
Two of the following criteria met (DKA):
pH > 7.30
HCO3 > 15 mEq/L
Anion gap ≤ 12 mEq/L (closed)
Ketosis must be resolved before transition (check urine and anion gap <12)
when do you give bicarb for DKA
ONLY if pH is <7.0 (less than)
changing to SQ therapy
Basal/bolus insulin regimen preferred
Long-acting/short- or rapid-acting insulin
Insulin pump
Administer subcutaneous insulin prior to
discontinuing IV insulin with attention to insulin
action profile
Monitor at least every 6 to 8 hours
Determined by meal schedule
If NPO, then every 6 hours
what do we want to keep the K+ at for DHA & HHS
4-5 mEq/L
establish renal function first
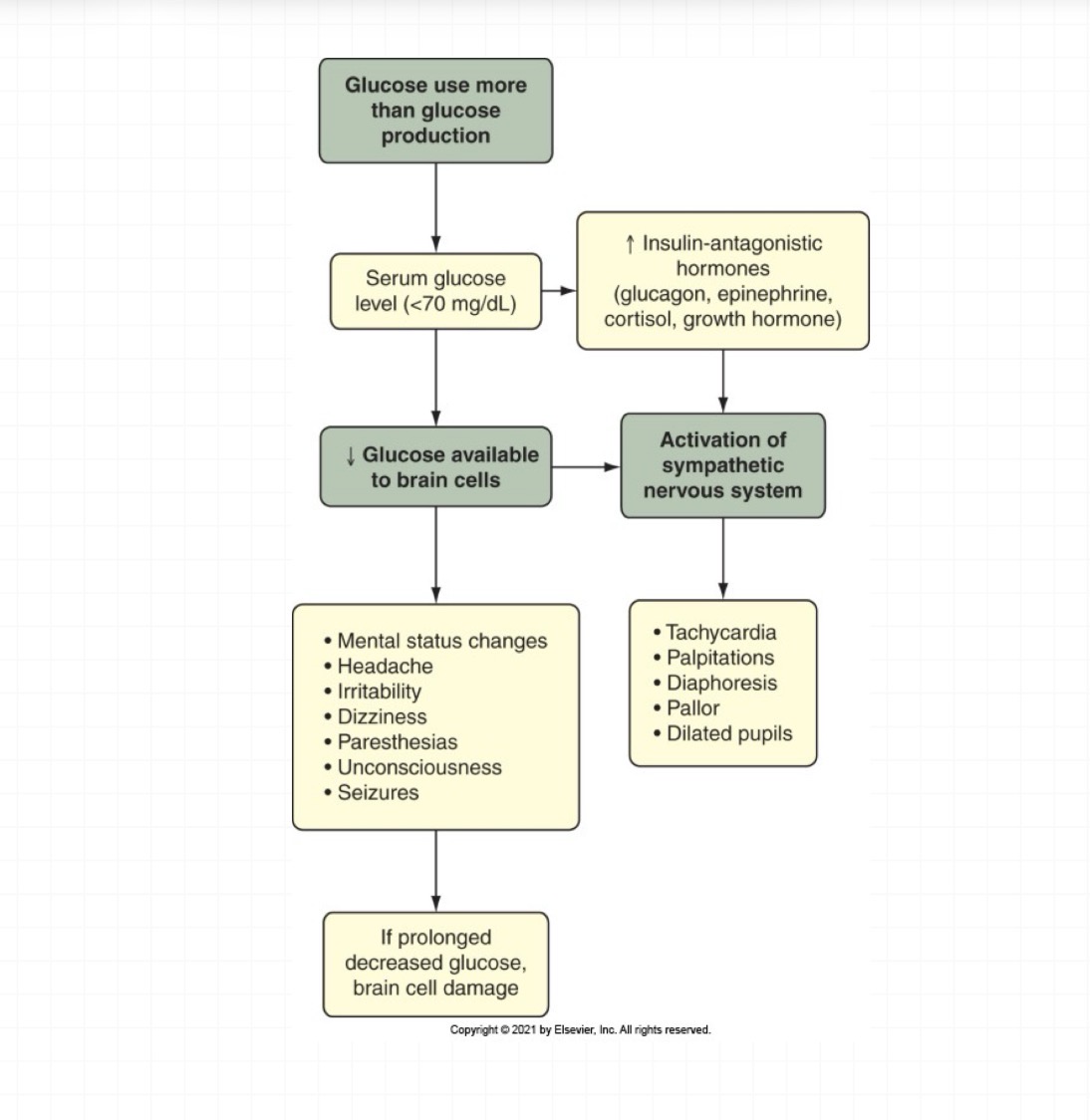
HYPOglycemia lab level
less than 70 mg/dL
hypoglycemia etiology
Excess insulin/oral agents
Alcohol potentiates hypoglycemic effects
Insufficient nutrition intake
Excess exercise
Medications (e.g., beta blockers)
Renal impairment
Diabetic neuropathy
Hypoglycemia unawareness
gastroparesis
hypoglycemia assessment
Rapid decrease in serum glucose levels
Activation of sympathetic nervous system
(epinephrine release)
Tachycardia
Diaphoresis
Pallor
Dilated pupils!!!!!
lightheaded
Hypoglycemia unawareness
neuro affects with low BG
Restlessness
Difficulty thinking and speaking
Visual disturbances
Paresthesias
Change in LOC
hypoglycemia interventions
15 g carbohydrate orally (carbs + protein,like pb&j, cheese )
50% dextrose (EMS, ED, ICU settings)
Glucagon
Oral glucose
Assess response: should improve rapidly
Adjust insulin regimen temporarily
Prevention and teaching
Diabetes Insipidus (DI)
not releasing adequate ADH —> PEE TOO MUCH—> CAN DIE FROM DEHYDRATION
DI patho
deficiency in synthesis or release of ADH
excessive WATER LOSS
dehydrated and hypotensive —> HYPOVOLEMIC SHOCK
what are the types of DI
neurogenic (central)
nephrogenic (kidney)
neurogenic DI
more common
ADH deficiency
brain not producing ADH —> pituitary swelling, tumor, trauma)
nephrogenic DI
kidneys are insensitive to ADH
dont respond
ADH disorders
DI
SIADH (TOO MUCH ADH)
DI neurogenic etiology
genetically predisposed
head trauma
neurological abnormalities
increased ICP
pituitary surgery
DI nephrogenic etiology
genetically predisposed
chronic renal disease
multisystem disorders affecting the kidneys
multiple myeloma
sickle cell
cystic fibrosis
DI nephrogenic etiology drugs
ethanol
phenytoin (dilantin)
lithium
demeclocycline
amphotericin
methoxyflurane (inhaled anesthetic)
DI assessment
PEE A LOT, high urine output
Thirst and polydipsia
Hypotension
Decreased skin turgor
Dry mucous membranes
Tachycardia
Weight loss
Low right atrial pressure/central venous pressure (RAP/CVP) and pulmonary artery (PA) pressure
Neurological changes
Hypernatremia and hypovolemia (DRY IS HIGH )
DI= dry inside
DI dx
urine sample
Dilute urine with low specific gravity (OVERLOADED, LOTS OF FLUID)
Increased serum osmolality (blood concentrated)
Increased blood urea nitrogen (BUN) and
creatinine
Hypokalemia or hypercalcemia
Water deprivation test
Vasopressin test (to differentiate)
what does the vasopressin test do
to differentiate betweeen neurogenic and nephrogenic
will give vasopressin, if they STOP PEEING, it is central/NEUROGENIC—> the body finally gets ADH which is vasopressin and they stop peeing as much and and urine becomes more concentrated —> increased specific gravity
if we give ADH and the pt doesn’t respond and keeps peeing, no change in UO, urine stays diluted
how does the sodium look in DI
WILL BE HIGH
HIGH and DRY
>145 mEq/L
Free water loss due to
absent or diminished
release of ADH or lack of
response by the kidneys
results in
hemoconcentration of
sodium DRY IS HIGHHHHHH
osmolality in DI
>295
Free water loss due to
absent or diminished
release of ADH or lack of
response by the kidneys
increases serum osmolality;
will be normal in secondary
DI
urine osmolality in DI
<100
Free water loss into urine
decreases urine osmolality
DI interventions
VOLUME REPLACEMENT
Monitor for fluid overload and water intoxication once therapy has been initiated
Hormone replacement
Vasopressin (desmopressin)
Thiazide diuretics (nephrogenic)
pt education of DI
Pathogenesis of DI
Dose, side effects, and rationale for prescribed medications
Parameters for notifying the physician
Importance of adherence to medication regimen
Importance of recording daily weight measurements to identify weight gain
Importance of wearing a Medic-Alert identification bracelet
Importance of drinking according to thirst and
avoiding excess drinking
SIADH- syndrome of inappropriate antidiuretic hormone
THEY ARE NOT PEEING ENOUGH
EXCESS ADH (withholding water)
plasma hypotonicity (hold onto fluid, become overloaded)
SIADH can be from
CNS disease
trauma
tumor
Malignancy (tumors produce, decreased ADH)
small lung cell carcinoma
hodgkin’s lymphoma
pancreatic and duodenal carcinoma
Pulmonary disorders
TB, lung abscess, PNA, COPD
what meds can cause SIADH
SSRI
TCA
Antiepileptics—> carbamazepine, valporic acid
Chemo —> cyclophosphamide
SIADH CNS s/s
low Na+
confusion
headache
seizures
weakness
SIADH pulmonary system
increased RR
dyspnea
adventitious lung sounds
SIADH CV s/s
HTN
elevated CVP and PA pressure (overloaded)
edema
SIADH GI system s/s
anorexia
N/V
muscle cramps
decreased bowel sounds
SIADH labs
hyponatremia (overloaded, hemodilutional)
decreased serum osmolality (overloaded)
high urine sodium
concentrated urine
decreased BUN and CR (overloaded)
decreased albumin
sodium in SIADH
<135 mEq/L (diluted)
free water retention due to over secretion of ADH —> dilutes Na+ , holding onto water/urine and the remaining Na+ gets diluted
osmolality serum in SIADH
<280
free water RETENTION due to over secretion of ADH , decreases osmolality from overload