Preterm birth, post-partum, sepsis
1/55
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
56 Terms
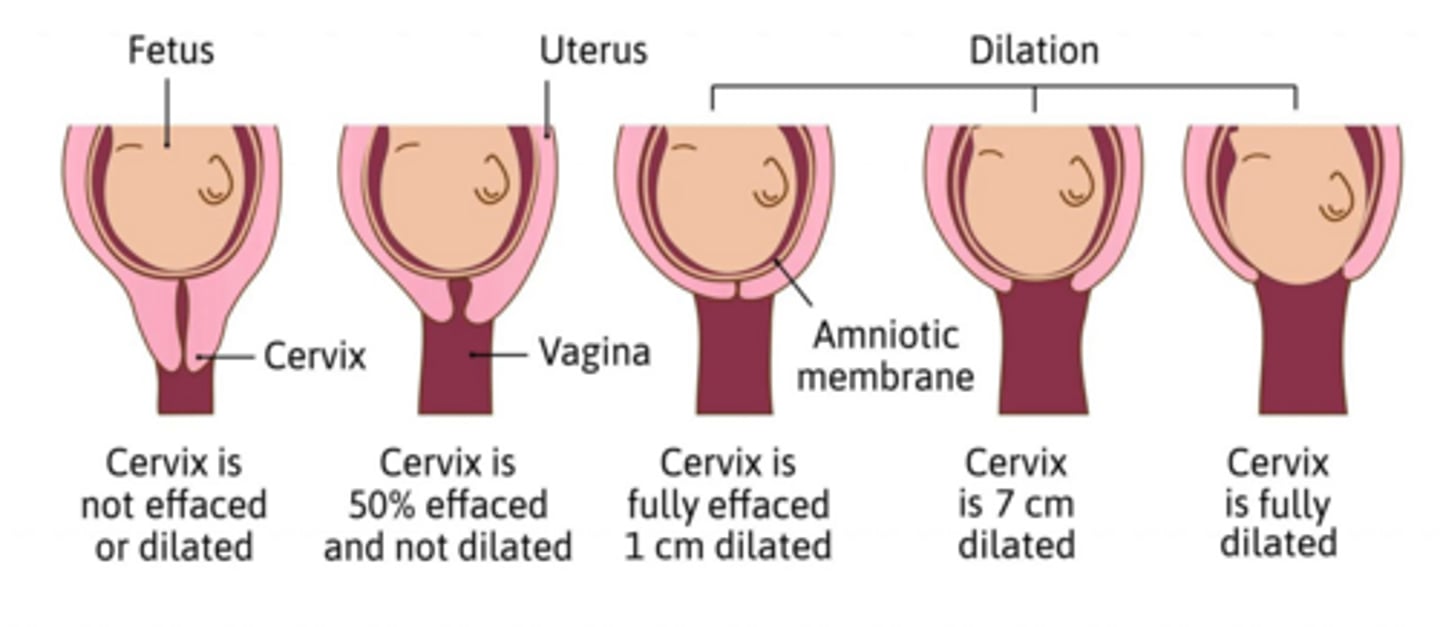
What is the definition of preterm labor?
Uterine contractions occurring between 20-37 weeks of gestation, leading to cervical changes.
What are the criteria for diagnosing preterm labor?
Uterine contractions of 4 per 20 minutes or 8 per 60 minutes, with cervical effacement of 80% or cervical dilation of 2 cm or more.
What is the leading cause of infant mortality related to gestation?
Prematurity.
What are some causes of preterm labor?
Spontaneous preterm labor, multiple gestations, preterm premature rupture of membranes (PPROM), pregnancy-associated hypertension, and cervical incompetence.
What are some risk factors for preterm labor?
Placental-uterine vascular dysregulation, smoking, stress, assisted reproductive technologies, genetic thrombophilias, and previous preterm birth.
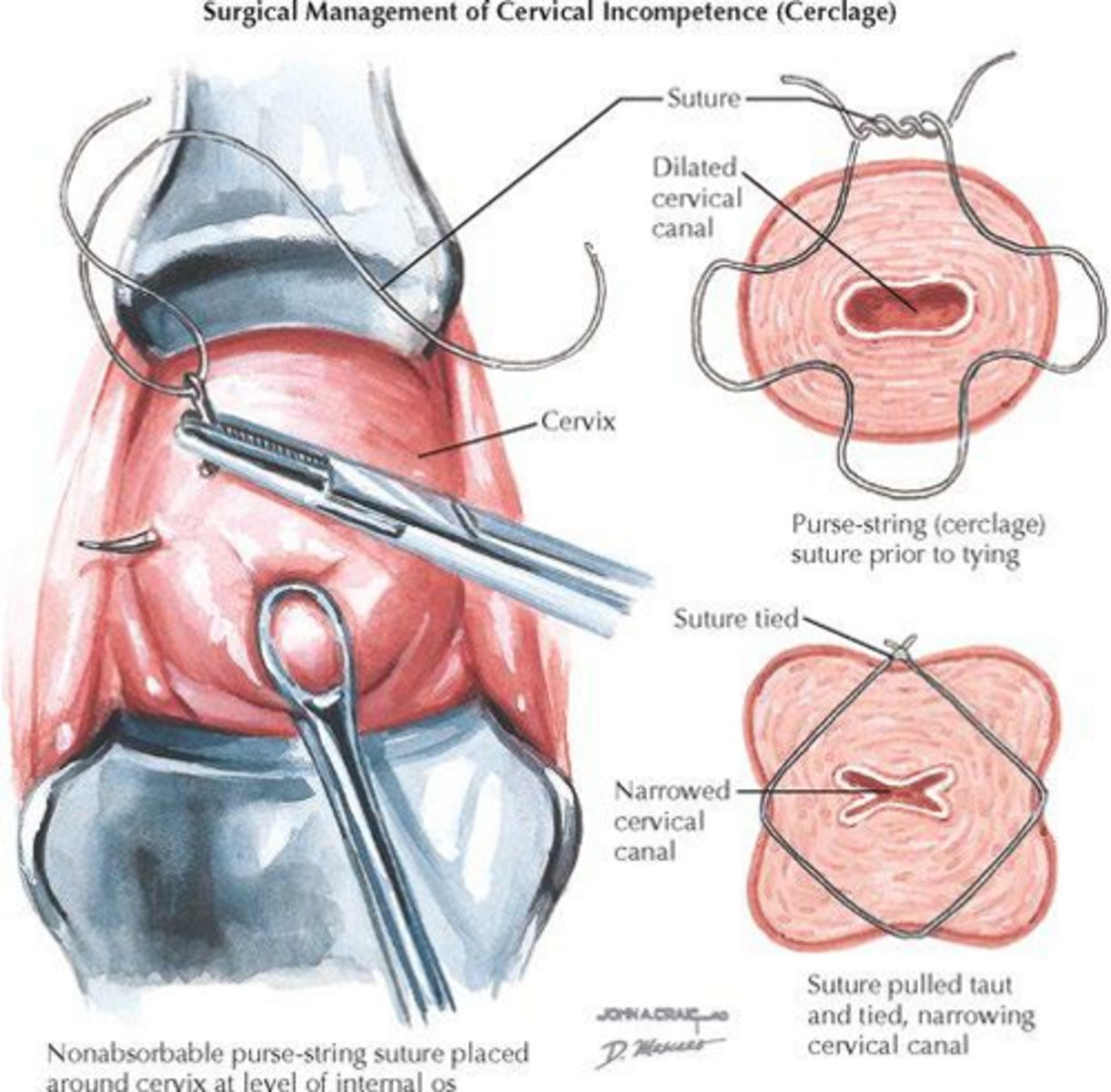
What is cervical incompetence?
The inability to retain a pregnancy in the absence of contractions or labor.
What diagnostic tools are helpful for cervical incompetence?
Patient history, transvaginal ultrasound, and physical examination.
What is the first-line management for cervical incompetence?
Transvaginal cerclage
When is the transabdominal approach reserved?
For those contraindicated for transvaginal
What should be done with sutures prior to labor?
They should be removed.
What is the implication of a transabdominal approach?
It results in lifelong cesarean deliveries.
What does a positive fetal fibronectin test at 22-24 weeks predict?
More than half of spontaneous preterm births before 28 weeks.
What is the definition of premature rupture of membranes (PROM)?
Rupture of the fetal membranes before the onset of labor.
What is the management approach for patients with premature rupture of membranes?
Monitoring for infection, assessing fetal well-being, and considering delivery based on gestational age and maternal/fetal status.
What defines post-term pregnancy?
Pregnancy that extends beyond 42 weeks of gestation.
What is a key week for respiratory development in fetuses?
24 weeks.
What levels give ratio that help to predict RDS risk?
Lecithin/sphingomyelin.
What does an L/S ratio <2 indicate?
Pulmonary immaturity.
What is included in the initial management of preterm labor/delivery?
Observation/serial exams, UA/vaginal swabs, hydrate, 5% dextrose.
What is the management for preterm labor if hydration is ineffective?
Initiate tocolytic therapy.
What are the contraindications to tocolytics?
Severe preeclampsia, severe placental bleeding, chorioamnionitis, IUGR, and fetal anomalies incompatible with life.
What is the purpose of glucocorticoid therapy in preterm delivery?
To facilitate fetal pulmonary maturation and reduce mortality.
What is the significance of the 7-day IM injections of betamethasone?
It is optimal for facilitating fetal pulmonary maturation.
What is the potential viability lower limit for preterm delivery?
24 weeks or 500 g.
What is defined as PROM?
Vaginal loss of amniotic fluid before the onset of labor.
What are the risk factors of PROM?
Vaginal/cervical infections, abnormal membrane physiology, incompetent cervix, nutritional deficiencies.
What tests confirm PROM?
Nitrazine paper test, fern test, and Amnisure test.
What is the management of PROM?
CBC, POC blood glucose, pulmonary maturation studies from vaginal pool, gram stain of amniotic fluid. MUST CONSIDER QUANTITY OF AMNIOTIC FLUID!
What does oligohydramnios associated with PROM <24 weeks lead to?
Pulmonary complications
What is the management for PROM at 36 weeks or more?
Labor may be induced if the cervix is favorable.
What is the risk associated with PPROM?
High risk of infection increases with time.
What is done if chorioamnionitis is diagnosed in either PROM or PPROM?
Ampicillin/gentamicin are mainstay pending sensitivity.
What makes someone eligible to be discharge with PROM?
Reliable, understanding of risks, fetus in vertex position, and cervix must be closed.
What is postterm pregnancy?
Pregnancy beyond 42 weeks from onset of last "normal" menstrual period.
What are the risks associated with post-term pregnancy?
Increased risk of stillbirth, macrosomia, and need for cesarean delivery. Perinatal mortality 2-3x higher
What is the management strategy for postterm pregnancy?
Induction when possible; monitoring with NSTs and biophysical profiles, if not a candidate for induction.
What is the definition of postpartum hemorrhage?
Blood loss >500 ml vaginal delivery or >1000 ml C-section. Leading cause of maternal mortality.
What is the leading cause of postpartum hemorrhage?
Uterine atony.
What are common causes of postpartum hemorrhage?
Uterine atony, lacerations, retained placenta, and coagulopathy.
What are the risk factors for postpartum hemorrhage?
Clotting disorders, prolonged labor, grand multiparity, and uterine overdistention.
What is the management for postpartum hemorrhage?
Early high risk identification, give oxytocin infusion for high risk pp patients, volume repletion, pharm treatment, bimanual compression, uterine packing, hysterectomy (LAST RESORT)
What is the management for postpartum hemorrhage due to lacerations?
Suture above the apex and manage conservatively for cervical lacerations.
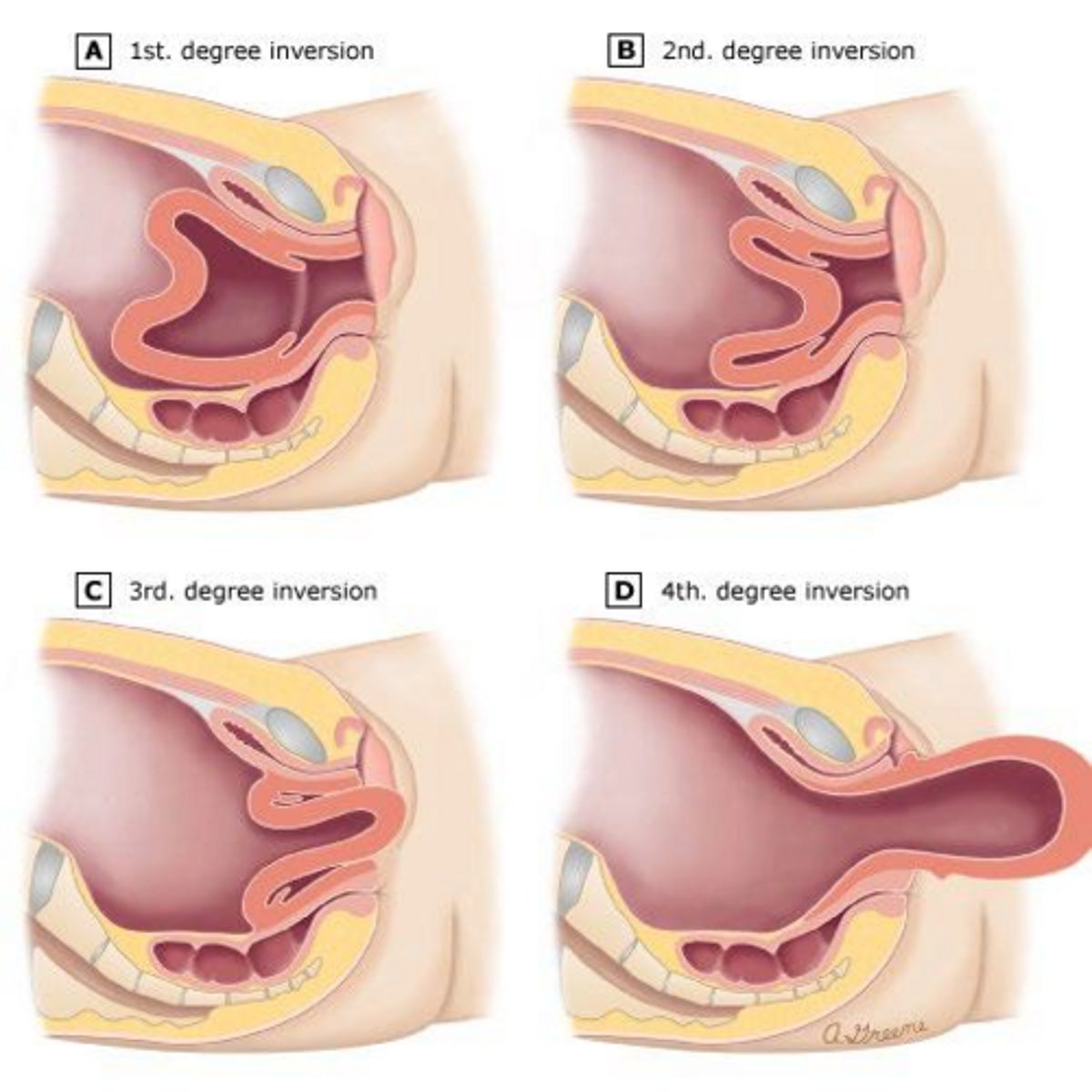
What is the management for uterine inversion?
IV fluids and manual replacement of the inverted fundus.
What is the role of amniotic fluid embolism in postpartum complications?
It can cause rapid decompensation requiring respiratory support.
What is the differential etiologies for postpartum infection?
Endometritis, chorioamnionitis and postabortal infection.
What are the risk factors for chorioamnionitis?
Prolonged labor/rupture of membranes, multiple vaginal exams, young age, low socioeconomic class, pre-existing BV.
What are the signs of chorioamnionitis?
Fever, maternal or fetal tachycardia, leukocytosis, uterine tenderness, foul smelling amniotic fluid.
What is the role of antibiotic prophylaxis in postpartum infection?
To prevent infections in high-risk patients during and after delivery.
What is the most common cause of puerperal fever?
Post partum endometritis.
What are the risk factors fo PPE?
C-section (higher risk if after labor or rupture of membranes), prolonged labor, rupture of membranes, BV, frequent vaginal exams, internal fetal monitoring.
What are common bacterial causes of PPE?
GBS, G vaginalis.
What is the typical presentation of postpartum endometritis?
Fever on POD ½, abdominal pain, uterine tenderness, leukocytosis.
What is the recommended antibiotic regimen for postpartum endometritis?
Clindamycin + gentamicin.
What are the risks of postabortal infection?
Greater duration of pregnancy, procedure technically difficult and STI/BV.
What are the PE findings of postabortal infection?
Elevated temp, tachycardia, tachypnea, abdominal tenderness.
What is the management for retained products of conception post-abortion?
Hospitalization, IV antibiotics, and evacuation of POC if febrile.