MED CHEM LEC 30-31
5.0(2)
Studied by 2 peopleCard Sorting
1/52
There's no tags or description
Looks like no tags are added yet.
Last updated 8:17 PM on 4/17/23
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
53 Terms
1
New cards
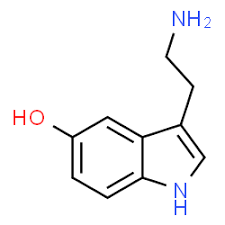
Structure of Serotonin
2
New cards
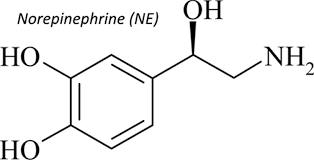
Structure of Norepinephrine
3
New cards
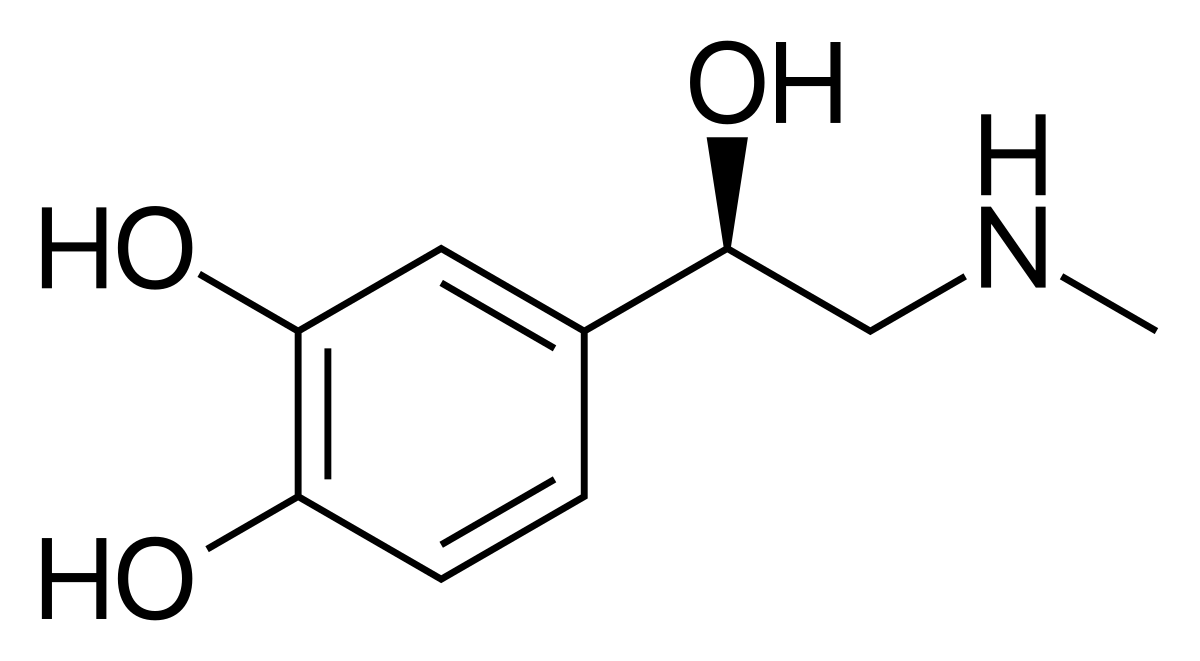
Structure of Epinephrine
4
New cards
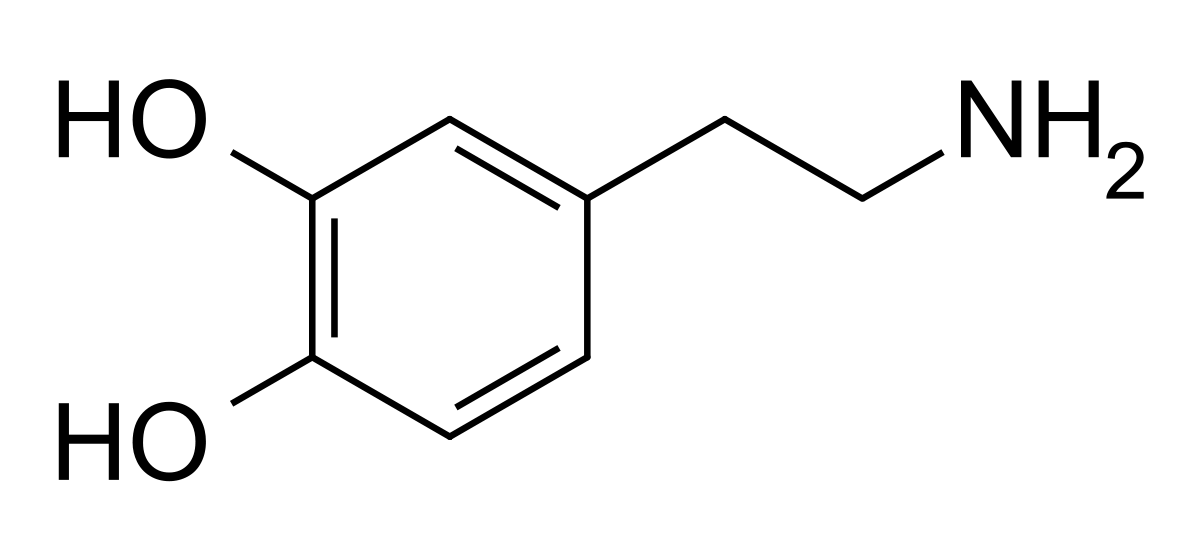
Structure of Dopamine
5
New cards
Biogenic Amine Hypothesis
Depression is coincident with diminished NT of naturally occurring amine NT )dopamine, NE, and serotonin = monoamines)
\
Binding of antidepressants to monoamine transporter occurs immediately, tho therapeutic effects take 3-6 weeks, and chronic administration is necessary, suggesting physiological changes are necessary.
\
Binding of antidepressants to monoamine transporter occurs immediately, tho therapeutic effects take 3-6 weeks, and chronic administration is necessary, suggesting physiological changes are necessary.
6
New cards
Receptor Sensitivity Hypothesis
\
1. There is an increased sensitivity and number of postsynaptic NE and serotonin receptors that lead to depression
1. Hypersensitive receptors keep NE and serotonin levels low → signals to upregulate the number of neuronal receptors
2. Receptor down-regulation and desensitization take → Consistent with observed delayed onset of drug effect
3. Through a study, it was found that increased NE and/or serotonin concentrations did not desensitize the postsynaptic receptors
1. There is an increased sensitivity and number of postsynaptic NE and serotonin receptors that lead to depression
1. Hypersensitive receptors keep NE and serotonin levels low → signals to upregulate the number of neuronal receptors
2. Receptor down-regulation and desensitization take → Consistent with observed delayed onset of drug effect
3. Through a study, it was found that increased NE and/or serotonin concentrations did not desensitize the postsynaptic receptors
7
New cards
The Permissive Hypothesis
\
1. Emphasize the balance between serotonin and NE is critical to regulate mood - not just their absolute concentraitons or their receptors
2. If serotonin elvels are too low:
1. NE levels are unchecked by serotonin and NE concentrations can go too **high→** leads to mania
2. NE levels are unchecked by serotonin and NE cocnentrations can get too **low→** leads to depression
3. Agents affecting dopamine levels are also effective and neuropeptides might also be involved
1. Emphasize the balance between serotonin and NE is critical to regulate mood - not just their absolute concentraitons or their receptors
2. If serotonin elvels are too low:
1. NE levels are unchecked by serotonin and NE concentrations can go too **high→** leads to mania
2. NE levels are unchecked by serotonin and NE cocnentrations can get too **low→** leads to depression
3. Agents affecting dopamine levels are also effective and neuropeptides might also be involved
8
New cards
What are the generally complications of DDI in terms of how the metabolism of a theoretical drug is altered and what the effect of that might be?
\
1. Appropriate choice of drug depends on many factors
1. Other medications the patient is on (including herbal/supplements)
2. Diet
3. Genetic variance
4. non-responsiveness to a particular therapy
5. Other disease
6. Tolerable SE/compliance
7. Routes of metabolism for chosen drug
2. If another drug (drug B) you are taking is able to inhibit the enzymes, there can be a buildup of drug A which can lead to toxic concentration
1. Appropriate choice of drug depends on many factors
1. Other medications the patient is on (including herbal/supplements)
2. Diet
3. Genetic variance
4. non-responsiveness to a particular therapy
5. Other disease
6. Tolerable SE/compliance
7. Routes of metabolism for chosen drug
2. If another drug (drug B) you are taking is able to inhibit the enzymes, there can be a buildup of drug A which can lead to toxic concentration
9
New cards
Which cytochrome P450 enzymes are most often involved with drug metabolism and how does the number of CYPs involved translate to the likelihood of drug-drug interactions?
\
1. CYP3A4 and CYP2D6 are the most involved
2. If an antidepressant is metabolized by more than one CYP450 isoform in parallel, genetic variance or drug interacts are less likely to be an issue due to CYP isoform inhibition
3. If the drug is metabolized by one CYP450 isoform, the potential for DDI increases
1. CYP3A4 and CYP2D6 are the most involved
2. If an antidepressant is metabolized by more than one CYP450 isoform in parallel, genetic variance or drug interacts are less likely to be an issue due to CYP isoform inhibition
3. If the drug is metabolized by one CYP450 isoform, the potential for DDI increases
10
New cards
Know how P-glycoproteins affect drug concentrations in various areas of the body and how this relates to the effect a drug has
\
1. P-glycoprotein transporters are membrane transport protein responsible for effux of many drugs
2. They are expressed in the liver, pancreas, kidney, colon, and brain capillary endothelial cells and placenta
3. Limits penetration/retneion of drugs into thse compartments which modulates durg effectiveness nad localized toxicity (CNS)
4. Inhibition of Pgp can significantly increase drug concentrations in the CNS = leads to toxicity
5. Inhibition of Pgp can significantly increase drug concentrations in intestinal cells = increased bioavailbility
6. Ex: grapefruit
1. Compounds within the fruit can inhibit CYP3A4 and Pgp to increases drug concentration
1. P-glycoprotein transporters are membrane transport protein responsible for effux of many drugs
2. They are expressed in the liver, pancreas, kidney, colon, and brain capillary endothelial cells and placenta
3. Limits penetration/retneion of drugs into thse compartments which modulates durg effectiveness nad localized toxicity (CNS)
4. Inhibition of Pgp can significantly increase drug concentrations in the CNS = leads to toxicity
5. Inhibition of Pgp can significantly increase drug concentrations in intestinal cells = increased bioavailbility
6. Ex: grapefruit
1. Compounds within the fruit can inhibit CYP3A4 and Pgp to increases drug concentration
11
New cards
What monoamines do monoamine oxidase inhibitors metabolize and how? In other words, what intermediates and metabolites do MAO enzymes generate from serotonin?
From serotonin, MAO can convert it into 5-HIAL
\
ALDH can then convert it into 5-HAA
\
ALDH can then convert it into 5-HAA
12
New cards
Know how monoamine oxidase inhibitors are used to treat depression.
\
1. Serotonin, melatonin, noradrenaline, adrenaline → mainly broken down by MAO-A
2. Phenethylamine and benzylamine are mainly broken down by MAO B
3. Both forms can break down dopamine, tyramine, and tryptamine equally
4. By inhibiting MAOs, we increase concentrations of these monoamines (cause not breaking them down)
1. Serotonin, melatonin, noradrenaline, adrenaline → mainly broken down by MAO-A
2. Phenethylamine and benzylamine are mainly broken down by MAO B
3. Both forms can break down dopamine, tyramine, and tryptamine equally
4. By inhibiting MAOs, we increase concentrations of these monoamines (cause not breaking them down)
13
New cards
14
New cards
Two subtypes of MAO
* MAO A
* MAO B
* MAO B
15
New cards
Name the 1st generation MAOIs
* Pargyline
* Tranylcypromine/Parnate
* Isocarboxazid/Marplan
* Phenelzine/Nardil
* Tranylcypromine/Parnate
* Isocarboxazid/Marplan
* Phenelzine/Nardil
16
New cards
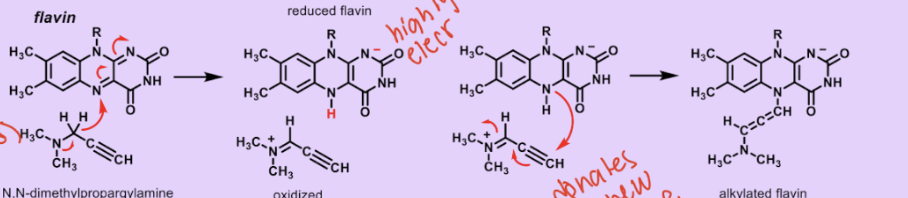
First gen MAOIs are irreversible/reversible?
Irreversible - they bind covalently to the MAO enzymes (usually with the flavin int he active site)
17
New cards
First gen MAOIs are selective/non-selective?
Nonselective - binds covalently to both MAO-A and MAO-B (all future a reactive functional group
18
New cards
Name hte 2nd gen MAOIs
* chlorgyline
* deprenyl/selegiline
* deprenyl/selegiline
19
New cards
2nd gen MAOIs are irreversible/reversible?
Irreversible
20
New cards
2nd gen MAOIs are selective/non-selective?
Selective (\* think because they are irreversible, they don’t want to bind onto an MAO until they know its the right one because they can come off later)
21
New cards
What is the mechanism of action of irreversible MAOIs and what distinct reactive functional groups do they have?
22
New cards
Selegiline/Deprenyl
* 2nd gen MAOI
* irreversible
* MAO-B selective
* early stages of Parkinsons disease - reduces symptoms (therefore) affecting dopaminergic neurons
* transdermal patch (Esam) is used to treat depression
* irreversible
* MAO-B selective
* early stages of Parkinsons disease - reduces symptoms (therefore) affecting dopaminergic neurons
* transdermal patch (Esam) is used to treat depression
23
New cards
Recognize the advantages of using a reversible, selective MAOI such as moclobemide over non-selective and/or irreversible MAOIs.
24
New cards
3rd gen MAOIs are irreversible/reversible?
reversible - binds non-covalently to the MAO enzymes
25
New cards
3rd gen MAOIs are selective/non-selective?
selective
26
New cards
Moclobemide/ clobemix
* 3rd gen MAOI
* Reversible
* MAO-A selective
* not approved in the US
* shorter duration of action than other MAOIs
* It is claimed that no significant rise in BP occurs when combined with amine such as tyramine- containing foods but patients are warned to avoid large amounts of tyramine containing foods
* Reversible
* MAO-A selective
* not approved in the US
* shorter duration of action than other MAOIs
* It is claimed that no significant rise in BP occurs when combined with amine such as tyramine- containing foods but patients are warned to avoid large amounts of tyramine containing foods
27
New cards
Side effects of MAOIs, the mechanisms by which these occur, and when MAOIs are contraindicated with other drugs.
\
1. Hypertensive crisis (tyramine pressor response)
1. Inhibitor of MAO-A and MAO-B in the liver and GI leads to dietary tyramine accumulation and displacement of NE from neuronal storage vesicles
2. Hypertensive crisis - Cheese reactions!
3. A paid and severe rise in BP
2. DDI - drug A affects the metabolism and therefore circulating concentration of drug B
1. Serotonin syndrome (CNS toxicity) - acute, potentially fatal when co-administered with TCAs
2. Effects of too much serotonin present at the receptor: mild symptoms: shivering, diarrhea; severe symptoms: muscle rigidity, fever, and seizures
3. TCAs block monoamine reuptake → increase serotonin
4. MAOIs block monoamine degradation → increased serotonin
3. Wight gain
4. Liver damage (hydrazines)
5. Longer term use leads to downregulation of adrenergic beta receptors → orthostatic hypotension
1. Hypertensive crisis (tyramine pressor response)
1. Inhibitor of MAO-A and MAO-B in the liver and GI leads to dietary tyramine accumulation and displacement of NE from neuronal storage vesicles
2. Hypertensive crisis - Cheese reactions!
3. A paid and severe rise in BP
2. DDI - drug A affects the metabolism and therefore circulating concentration of drug B
1. Serotonin syndrome (CNS toxicity) - acute, potentially fatal when co-administered with TCAs
2. Effects of too much serotonin present at the receptor: mild symptoms: shivering, diarrhea; severe symptoms: muscle rigidity, fever, and seizures
3. TCAs block monoamine reuptake → increase serotonin
4. MAOIs block monoamine degradation → increased serotonin
3. Wight gain
4. Liver damage (hydrazines)
5. Longer term use leads to downregulation of adrenergic beta receptors → orthostatic hypotension
28
New cards
Name the secondary amines of the tricyclic amine antidepressants (TCAs) - SNRIs
\
1. Desipramine/Norpramin
2. Nortriptyline/Pamelor
1. Desipramine/Norpramin
2. Nortriptyline/Pamelor
29
New cards
How do SNRIs affect NE vs serotonin levels
\
1. They are more selective for inhibiting NE uptake over serotonin uptake
2. Reduced SE compared to tertiary amines
1. They are more selective for inhibiting NE uptake over serotonin uptake
2. Reduced SE compared to tertiary amines
30
New cards
Desipramine/Norpramin
* Secondary amines - SNRIs
* The active metabolite of imipramine (N-demethylation)
* Tends to be less sedating than other TCAs and tends to produce fewer anticholinergic effects
* The active metabolite of imipramine (N-demethylation)
* Tends to be less sedating than other TCAs and tends to produce fewer anticholinergic effects
31
New cards
Nortriptyline/Pamelor
* Secondary amines - SNRIs
* Active metabolite of amitryptyline (N-demethylation)
* Active metabolite of amitryptyline (N-demethylation)
32
New cards
Reboxetine/edronax
* The first SNRI
* **Nontricylic SNRI** (-**xetine**)
* Used for treatment of major depressive disorders
* Available in many countries - FDA concluded it is not better than others
* Weak CYP3A4/CYP2D6 metabolism; moderate P-gp inhibitor
* Still being questioned about efficacy in humans through animal models show exceptional activity
* **Nontricylic SNRI** (-**xetine**)
* Used for treatment of major depressive disorders
* Available in many countries - FDA concluded it is not better than others
* Weak CYP3A4/CYP2D6 metabolism; moderate P-gp inhibitor
* Still being questioned about efficacy in humans through animal models show exceptional activity
33
New cards
Atomoxetine/Strattera
\
1. Secondary amines - SNRIs
2. **Non-tricyclic SNRI (-xetine)**
3. Developed as an antidepressant but was not efficacious as a monotherapy in large studies
4. Prescribed for ADHD >6 yo
5. Can help some patients with combined depression and ADHD
6. >1 million prescriptions in the US alone in 2020
1. Secondary amines - SNRIs
2. **Non-tricyclic SNRI (-xetine)**
3. Developed as an antidepressant but was not efficacious as a monotherapy in large studies
4. Prescribed for ADHD >6 yo
5. Can help some patients with combined depression and ADHD
6. >1 million prescriptions in the US alone in 2020
34
New cards
Imipramine
* tertiary amine TCA - NSRIs (NE and serotonin reuptake inhibitors)
* first TCA antidepressant to be developed
* serotonin inhibition> NE
* Demethylation to desipramine (SNRI) gives net results of non-selectivity
* first TCA antidepressant to be developed
* serotonin inhibition> NE
* Demethylation to desipramine (SNRI) gives net results of non-selectivity
35
New cards
Amitriptyline
* Tertiary amine TCA - SNRIs (NE and Serotonin reuptake inhibitors)
* conformationally restricted
* (\*i-ma - trip over because I have no room- I am restricted)
* Equal affinity towards NE and serotonin (for uptake, not receptor binding)
* Sensitive to photo-oxidation (HCL solutions need to be protected from light to avoid ketone formation and precipitation)
* conformationally restricted
* (\*i-ma - trip over because I have no room- I am restricted)
* Equal affinity towards NE and serotonin (for uptake, not receptor binding)
* Sensitive to photo-oxidation (HCL solutions need to be protected from light to avoid ketone formation and precipitation)
36
New cards
Why are TCAs used less frequently compared to some of the newer antidepressant agents now available?
\
1. Secondary TCA antidepressants were once first line therapy for depresison due to the range of depressive and CNS disorders that could be treated with them.
2. Now, they are second line treatment because of narrow therapeutic window (efficacy to toxicity ratio) and ADE and the development of new drugs that are better tolerated andhave different/fewer ADE.
1. Secondary TCA antidepressants were once first line therapy for depresison due to the range of depressive and CNS disorders that could be treated with them.
2. Now, they are second line treatment because of narrow therapeutic window (efficacy to toxicity ratio) and ADE and the development of new drugs that are better tolerated andhave different/fewer ADE.
37
New cards
Venlafaxine/ Effexor
\
1. Nontricyclic NSRIs
2. Preferential affinity for Serotonin reuptake (30x more potent for SERT over NET)
3. The increasing dose can inhibit both SERT (serotonin transporters and NET
4. Dose-dependent ADE profile
5. Key concern: prolonged QT interval (cardiotoxicity) at normal dose
6. Distributed in breast milk
7. Metabolized by CYP2D6 to Desvenlafaxine
1. Nontricyclic NSRIs
2. Preferential affinity for Serotonin reuptake (30x more potent for SERT over NET)
3. The increasing dose can inhibit both SERT (serotonin transporters and NET
4. Dose-dependent ADE profile
5. Key concern: prolonged QT interval (cardiotoxicity) at normal dose
6. Distributed in breast milk
7. Metabolized by CYP2D6 to Desvenlafaxine
38
New cards
Desvenlafaxine/ODV
\
1. Nontricyclic NSRIs
2. Approved in US and Canada
3. 10 x more potent at 5- HT uptake inhibits over NE uptake
4. Most common side effects: is nausea
5. Metabolized by CYP3A4 ( N-demethylation) and O-glucuronidation
1. Nontricyclic NSRIs
2. Approved in US and Canada
3. 10 x more potent at 5- HT uptake inhibits over NE uptake
4. Most common side effects: is nausea
5. Metabolized by CYP3A4 ( N-demethylation) and O-glucuronidation
39
New cards
Duloxetine
\
1. Nontricyclic NSRIs
2. One of the most prescribed medications
3. Depression, diabetic peripheral neuropathic pain, fibromyalgia, osteroarthritiis pain
4. Inhibits both SERT and NET (5-fold preference for SERT)
5. Low affinity for other neuroreceptors → low incidence of ADE
1. Nontricyclic NSRIs
2. One of the most prescribed medications
3. Depression, diabetic peripheral neuropathic pain, fibromyalgia, osteroarthritiis pain
4. Inhibits both SERT and NET (5-fold preference for SERT)
5. Low affinity for other neuroreceptors → low incidence of ADE
40
New cards
Understand how SSRIs are proposed to work and that they are the most widely prescribed antidepressants and why.
\
1. Working hypothesis on the SSRI MOA
1. SSRIs block the 5-HT transporter so 5-HT is not reabsorbed
1. Increases the concentration of 5-HT in the synaptic cleft
2. Excess 5-HT overstimulates the post-synaptic receptors
2. After \~2 weeks, pre-post synaptic receptors are significantly down-regulated in CNS and the number of 5-HT transporters is reduced
3. Consistent with delayed onset of action of SSRIs
2. Selective for inhibiting 5-HT reuptake transporter
1. Because of this selectivity and potency, inhibition of 80% of SERT leads to antidepressant effects
1. Working hypothesis on the SSRI MOA
1. SSRIs block the 5-HT transporter so 5-HT is not reabsorbed
1. Increases the concentration of 5-HT in the synaptic cleft
2. Excess 5-HT overstimulates the post-synaptic receptors
2. After \~2 weeks, pre-post synaptic receptors are significantly down-regulated in CNS and the number of 5-HT transporters is reduced
3. Consistent with delayed onset of action of SSRIs
2. Selective for inhibiting 5-HT reuptake transporter
1. Because of this selectivity and potency, inhibition of 80% of SERT leads to antidepressant effects
41
New cards
Know the general side effect profile of the SSRI class
\
1. Compared to TCA, SSRIs cause more nausea, diarrhea, agitation, insomnia, sexual dysfunction, and anorexia
2. Compared to TCA, SSRIs cause less cardiotoxicity, dizziness, sweating, and blurred vision
3. Increased risk of suicide in children
4. Fatigue, anxiety, nausea, insomnia, sexual dysfunction
5. Potential to cause serotonin syndrome
1. Compared to TCA, SSRIs cause more nausea, diarrhea, agitation, insomnia, sexual dysfunction, and anorexia
2. Compared to TCA, SSRIs cause less cardiotoxicity, dizziness, sweating, and blurred vision
3. Increased risk of suicide in children
4. Fatigue, anxiety, nausea, insomnia, sexual dysfunction
5. Potential to cause serotonin syndrome
42
New cards
Name SSRIs (3)
\
1. Fluoxetine
2. Sertraline
3. Paroxetine
4. CItalopram
5. Escitalopram
1. Fluoxetine
2. Sertraline
3. Paroxetine
4. CItalopram
5. Escitalopram
43
New cards
Fluoxetine
\
1. Chiral, but sold as racemate
2. Several P450-related DDI due to CYP2D6 metabolism inhibition
3. Extensively N-demethylation (long-lived, active metabolite)
4. Inhibits CYP2D6 isoform→ clinical drug interactions
1. Chiral, but sold as racemate
2. Several P450-related DDI due to CYP2D6 metabolism inhibition
3. Extensively N-demethylation (long-lived, active metabolite)
4. Inhibits CYP2D6 isoform→ clinical drug interactions
44
New cards
Sertraline
\
1. SSRI
2. Extensively N-demethylated (long-lived, active metabolite)
3. T ½ : Sertraline : 26 hr, desmethylsertraline : 66hrs
4. Inhibits CYP2D6 isoform→ clinical drug interactions
1. SSRI
2. Extensively N-demethylated (long-lived, active metabolite)
3. T ½ : Sertraline : 26 hr, desmethylsertraline : 66hrs
4. Inhibits CYP2D6 isoform→ clinical drug interactions
45
New cards
Paroxetine
\
1. SSRI
2. Several studies have associated paroxetine with suicidal thinking and behavior in children and adolescents
1. (\* paro = parrot = kids like parrots as pets)
3. Inhibits CYP2D6 isoform→ clinical drug interactions
1. SSRI
2. Several studies have associated paroxetine with suicidal thinking and behavior in children and adolescents
1. (\* paro = parrot = kids like parrots as pets)
3. Inhibits CYP2D6 isoform→ clinical drug interactions
46
New cards
Citalopram
\
1. SSRIs
2. Racemix
3. Not approved in pediatric patients (black box warning)
4. Increased risk of suicide in children/adolescents
5. Dosage >40 mg once daily is no longer recommended due the to risk of QT interval prolongation
6. Maintenance dosage: 20-60 mg
7. Does not inhibits an major P450 enzymes
1. SSRIs
2. Racemix
3. Not approved in pediatric patients (black box warning)
4. Increased risk of suicide in children/adolescents
5. Dosage >40 mg once daily is no longer recommended due the to risk of QT interval prolongation
6. Maintenance dosage: 20-60 mg
7. Does not inhibits an major P450 enzymes
47
New cards
Escitalopram
\
1. SSRI
2. S-enantiomer of citalopram
3. Modestly better tolerated
4. More costly than racemic citalopram
1. (\*adding extra letters to the work = cost more to add)
5. Example of a chiral switch or “evergreening” to extend patent life
1. SSRI
2. S-enantiomer of citalopram
3. Modestly better tolerated
4. More costly than racemic citalopram
1. (\*adding extra letters to the work = cost more to add)
5. Example of a chiral switch or “evergreening” to extend patent life
48
New cards
Know what is meant by “evergreening” or a chiral switch
\
1. Ex: escitalopram
2. A method to extend patent life by switching to using another enantiomer of a racemic drug
1. Ex: escitalopram
2. A method to extend patent life by switching to using another enantiomer of a racemic drug
49
New cards
Mirtazepine/Remeron
\
1. NaSSA (alpha2-noradrengergic antagonist/selective serotonin antagonist)
2. Atypical antidepressant
3. Alpha 2- receptor antagonist → increases extracellular NE because usually alpha 2 -agonist suppresses release of NE)
4. Antagonizes 5-HT receptors (allowing the release of NE and DA in reward areas of brain)
5. Does not inhibit the reuptake of serotonin
6. Tetracyclic antidepressant
7. Racemic
8. No SSRI-like ADE
9. Binds at histamine h1 (sedative properties)
10. Unlike TCAs, shows no significant cardiovascular ADE
11. More rapid onset and long-term efficacy
12. Used as an adjunct therapy to SSRIs and SNRIs
1. NaSSA (alpha2-noradrengergic antagonist/selective serotonin antagonist)
2. Atypical antidepressant
3. Alpha 2- receptor antagonist → increases extracellular NE because usually alpha 2 -agonist suppresses release of NE)
4. Antagonizes 5-HT receptors (allowing the release of NE and DA in reward areas of brain)
5. Does not inhibit the reuptake of serotonin
6. Tetracyclic antidepressant
7. Racemic
8. No SSRI-like ADE
9. Binds at histamine h1 (sedative properties)
10. Unlike TCAs, shows no significant cardiovascular ADE
11. More rapid onset and long-term efficacy
12. Used as an adjunct therapy to SSRIs and SNRIs
50
New cards
Trazodone/Olepro/Desyrel
\
1. SARI (serotonin- 2 antagonist/ reuptake inhibitor)
2. Anxiety and depression, insomnia
3. First atypical antideprssant
4. 5-HT recepotr antagonist, 5-HT reuptake inhibitor, particle agonist at 5-HT 1A receptors
5. Low anticholinergic activity and virturally devoid of cardiovascular arrhythmia effects
6. Idiosyncratic hepatotoxicity ( due to iminoquinone)
7. Grapefruit juice interaction (CYP3A4)
1. SARI (serotonin- 2 antagonist/ reuptake inhibitor)
2. Anxiety and depression, insomnia
3. First atypical antideprssant
4. 5-HT recepotr antagonist, 5-HT reuptake inhibitor, particle agonist at 5-HT 1A receptors
5. Low anticholinergic activity and virturally devoid of cardiovascular arrhythmia effects
6. Idiosyncratic hepatotoxicity ( due to iminoquinone)
7. Grapefruit juice interaction (CYP3A4)
51
New cards
Vortioxetine/Brintellix
\
1. SARI (Serotonin 2- antagonist/reuptake inhibitor)
2. first-line treatment for major depressive disorder and what major neurotransmitter it is affecting
3. Serotonin reuptake inhibitor with several other activities, including 5-HT3 receptor antagonism and 5-HT1A receptor agonism
1. SARI (Serotonin 2- antagonist/reuptake inhibitor)
2. first-line treatment for major depressive disorder and what major neurotransmitter it is affecting
3. Serotonin reuptake inhibitor with several other activities, including 5-HT3 receptor antagonism and 5-HT1A receptor agonism
52
New cards
Bupropion/Wellbutrin/Zyban
\
1. DNRI (dopamine and NE reuptake inhibitor)
2. Antidepressant and 2nd line smoking cessation aid
3. Atypical antidepressant
4. Potent DA reuptake inhibitor (weak 5-HT/NE uptake inhibition)
5. Induces release of DA and NE
6. Risk of seizure as a SE
1. DNRI (dopamine and NE reuptake inhibitor)
2. Antidepressant and 2nd line smoking cessation aid
3. Atypical antidepressant
4. Potent DA reuptake inhibitor (weak 5-HT/NE uptake inhibition)
5. Induces release of DA and NE
6. Risk of seizure as a SE
53
New cards
Esketamine
\
1. Non-competitive N-methyl-d-aspartate (NMDA) receptor antagonist
2. Most recently approved drug for depression
3. Ketanest - IV
4. Spravato - nasal spray for treatment-resistant depression
5. Must be administered in a clinical setting, patients must remain on site for at least two hours after administration
1. This is because, during drug trials, patients experience sedation, difficulty speaking, confusion, numbness, and feelings of dizziness
6. MOA: NMDA receptors are inhibited by esketamine, this prevents ca2+ flux that would otherwise limit glutamate release. Glutamate release into synapse. Glutamate signaling and cascade re-established receptor responsiveness and receptor distribution
1. Non-competitive N-methyl-d-aspartate (NMDA) receptor antagonist
2. Most recently approved drug for depression
3. Ketanest - IV
4. Spravato - nasal spray for treatment-resistant depression
5. Must be administered in a clinical setting, patients must remain on site for at least two hours after administration
1. This is because, during drug trials, patients experience sedation, difficulty speaking, confusion, numbness, and feelings of dizziness
6. MOA: NMDA receptors are inhibited by esketamine, this prevents ca2+ flux that would otherwise limit glutamate release. Glutamate release into synapse. Glutamate signaling and cascade re-established receptor responsiveness and receptor distribution