pain management - lecture 18
1/37
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
38 Terms
pain
An unpleasant sensory & emotional experience. Pain is a universal human experience and yet it is a very individual & subjective experience that only the patient can describe and feel. Pain is whatever the patient says it is, at any time they say pain is occurring, even when no specific cause of the pain can be found.
“Pain is the 5th vital sign”
Pain cannot be captured in the way that we capture quantitative data like blood pressure, blood glucose, or an ABG. We cant “see” pain. We rely on the patient to provide information about their pain. The patient’s experience of pain must be respected.
Consequences/Considerations:
Pain can limit daily activities and diminish quality of life; effects are physiologic, psychological, and social, and even financial. (Disability, loss of work; decrease in performing activities such as walking/exercise, etc., and can cause feelings of depression, anxiety, & stigmatization. (There is often a stigma associated with chronic pain clients). Pain can also limit a person’s ability to perform activities of self-care such as ADLs, shopping, and house cleaning. Acute pain can affect how a person performs at work or school (pain affects attendance at work and school; threat of job loss). Pain often restricts an individual’s leisure activities and social contacts. Social isolation is common.
REMEMBER: The only person who is the authority on their pain is the patient and we must rely on the patient’s description/report of pain to administer treatment. ALL pain is valid.

what are the four steps in the pain pathway
1. transduction
2. transmission
3. perception
4. modulation
transduction
activation of pain receptors, called nociceptors. They are selective to sensing pressure, temperature, and chemical stimuli. Nociception- the ability to feel painful stimuli.
In transduction, painful stimuli are converted into electrical impulses that travel from the periphery to the spinal cord.
Injured tissue releases chemicals (bradykinin, prostaglandins, and substance P) that stimulate pain receptors and are involves in histamine release, vasodilation, redness, swelling, and pain that occurs with inflammation
Mechanical stimuli- friction from bed linens, pressure from a cast
Thermal stimuli- sunburn, cold water on a tooth
Chemical stimuli- acid or other chemical burn
transmission
Electrochemical signals travel along the length of a nerve to the dorsal horn of the spinal cord.
Pain sensations are conducted along ascending pathways to the spinal cord and brain.
- Afferent fibers carry impulses from the pain receptors towards the brain with fast conducting A-delta fibers and slow conducting C –fibers
-A-delta-fibers (myelinated) are larger and transmit acute, well-localized pain; C-fibers (unmyelinated) are smaller and convey dull, achy, poorly localized pain
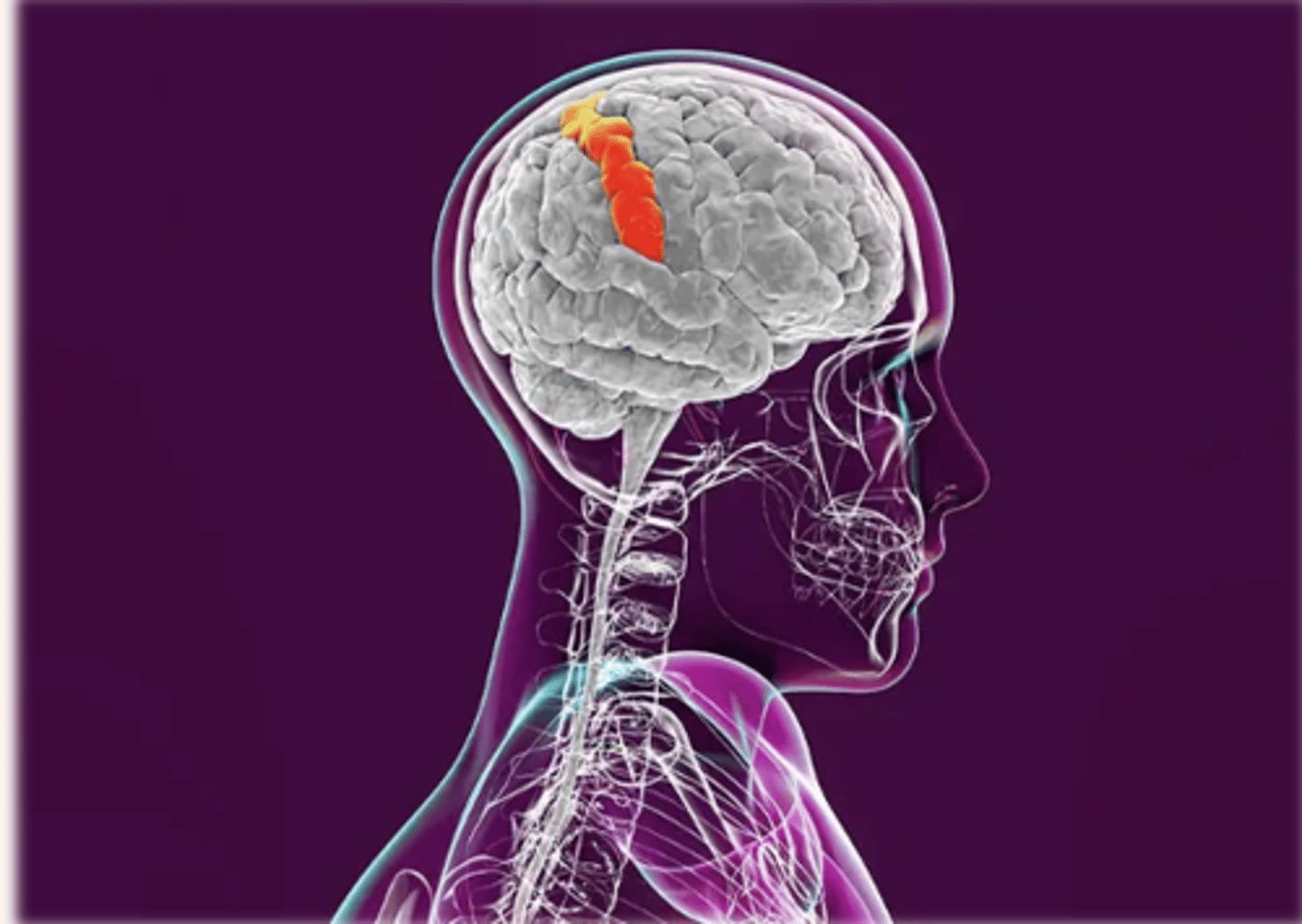
perception
The pain stimulus reaches the cerebral cortex, where the brain interprets the quality of the pain (sharp, dull, aching) and processes information from past experiences, knowledge, and cultural associations in the perception of the pain. Pain is perceived and understood.
The somatosensory cortex identifies the location and intensity of the pain. In this part of the pain pathway, triggers for anxiety, fear, and depression can occur with pain stimulus. Perception gives awareness to pain, resulting in a reaction that includes both physiological and behavioral responses.
modulation
Pain relief begins as a signal from the brain that descends by way of the spinal cord—in the dorsal horn, chemicals such as endorphins are released to diminish the pain message from the injured site. (other neuromodulators include serotonin, norepinephrine)
Modulation- the process by which the sensation of pain is inhibited or modified. The brain “modifies” the sensation of pain via neuromodulators.
Endorphins are endogenous, (naturally present in the body), opioid compounds that have an analgesic effect that alters pain perception. Analgesic-anything that relieves pain.
Protective pain reflex- responsible for withdrawal of an endangered tissue from a damaging stimulus. A-delta fibers send sensory impulses to the spinal cord, where they synapse with spinal motor neurons. The motor impulses travel by a reflex arc along efferent (motor) nerve fibers back to a peripheral muscle near the site of the pain stimulus where contraction of the muscle leads to a protective withdrawal from the source of the pain.
the gate control theory of pain (IMPORTANT)
Model used to describe how pain works
Painful stimuli can be blocked by non-painful stimuli (hitting elbow, and holding it to relieve pressure)
Neurological gates “decide” which pain signals can pass through and which are kept out
Theory explains how rubbing an injured area can reduce pain. Small diameter fibers activated by painful stimuli open the “gate” to pain transmission, and large diameter fibers have inhibitory effects to “shut” the gate.
Rubbing the injured area promotes large diameter fiber input and inhibits further transmission of pain signals from the small-diameter nerves to the brain, reducing pain.
Physiologic (autonomic) response to pain
The Autonomic Nervous system is activated with pain of low to moderate intensity and superficial pain eliciting the typical sympathetic (fight or flight) response including an increase in vital signs (HR, BP, RR,) along with pupil dilation, pallor, increased muscle tension, and increased blood glucose. Note: Patients in pain do not always have changes in their vital signs. Changes in VS more often indicate problems than pain. Changes in VS do not typically occur with chronic pain.
Behavioral response to pain
Complex and influenced by a person’s culture, pain experiences, perception of pain, and ability to manage stress. Clenching of the teeth, guarding, grimacing and restless, rocking in bed, pacing, protecting the painful area, sighing, crying and bent posture are common indications of acute pain.
With chronic pain, patients’ activities such as eating, sleeping, and socialization, thinking, emotions (anger, irritability, depression), quality of life, and productivity are impacted.
Lack of an obvious response to pain does not mean the patient is without pain. The nurse must perform a detailed pain assessment to understand the patient’s experience.
acute pain
pain that comes on rapidly, as with a cut, broken bone, sore throat, or surgery. It can range from mild to severe. Acute pain goes away once the underlying cause is resolved. It has limited tissue damage and emotional response. It resolves with or without treatment after the injured area heals. An increase in vital signs due to activation of the sympathetic nervous system can occur with acute pain.
chronic pain
pain that persists or is recurrent for more than 3-6 months. Chronic pain can also last for years. It is debilitating, both mentally and physically. Chronic pain can be unrelenting, persistent and severe or have periods of remissions and exacerbations.
Remission-disease is present, but person does not experience pain
Exacerbation- symptoms reappear

pain location
Pain can be also be classified based on its location and whether it is generalized or localized
Generalized pain- generalized pain is poorly localized (“My whole body aches.”)
Localized pain- location can be pinpointed, hurts in one area of the body (“My ankle hurts.”)
-Superficial- pain is of short duration and localized. Usually a sharp sensation (needlestick, paper cut)
-Somatic pain- pain that originates in bone, joint, muscle, skin, or connective tissue; usually aching or throbbing; well localized
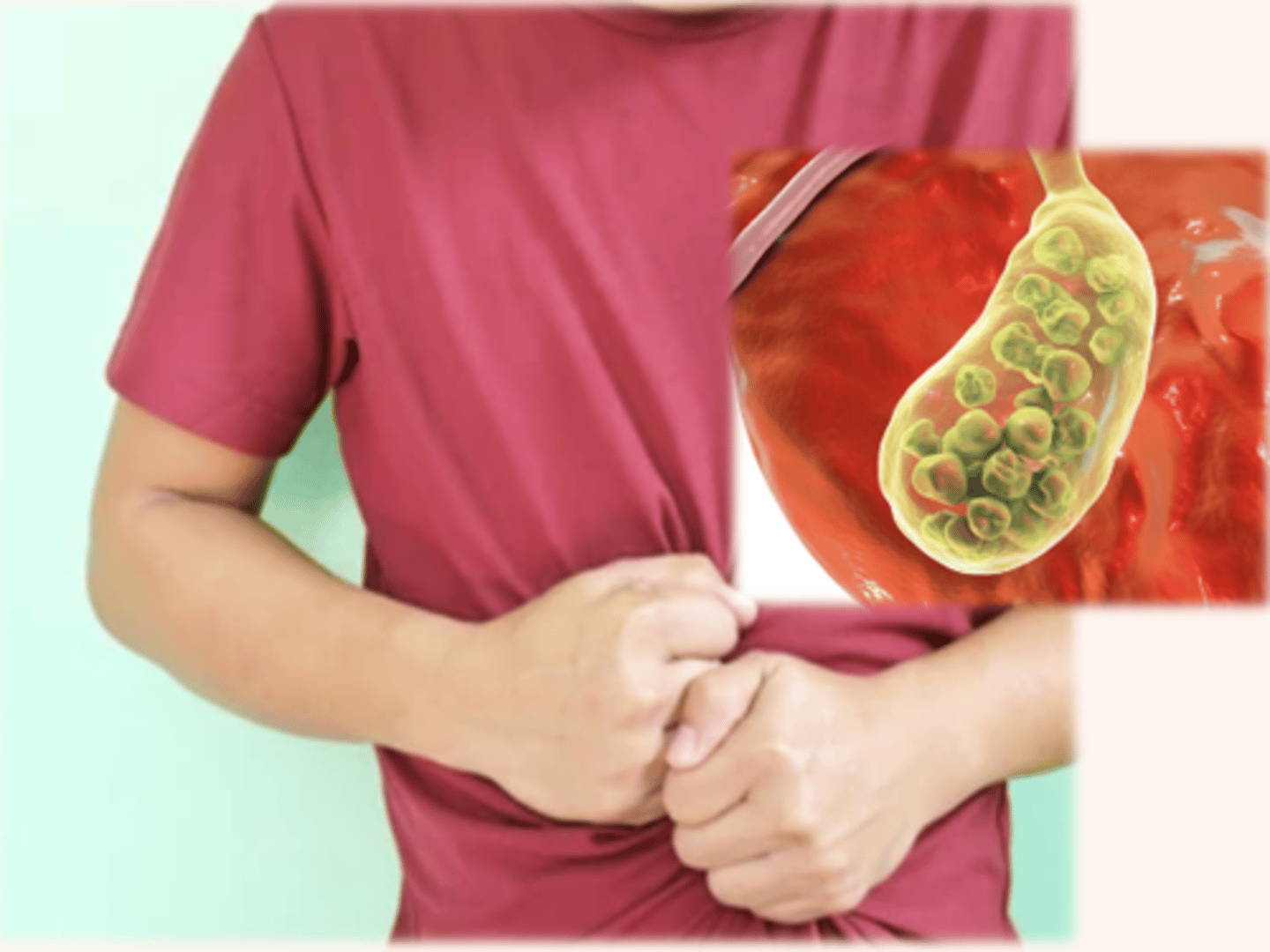
-Visceral pain- originates in visceral organs such as in the GI tract and pancreas. Visceral pain is often the result of a disease process that causes the organs to become distended, bloated, or ischemic. Pain can be aching, cramping, and is often poorly localized
Some examples of visceral pain are peritonitis, bowel obstruction, or cholecystitis
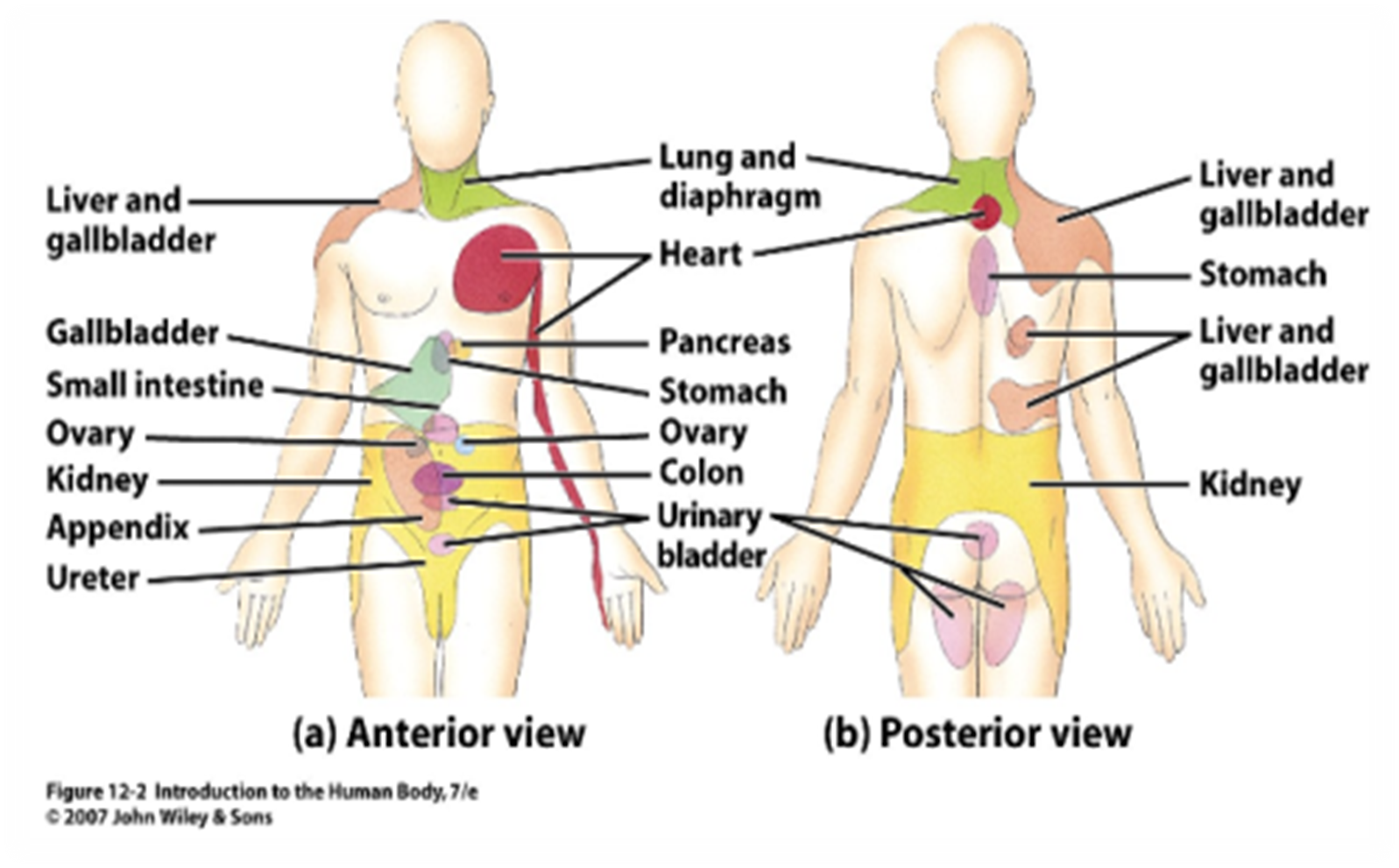
referred pain
Pain is in a part of the body that is different from the source of the pain and assumes any characteristic. Referred pain is common in visceral pain because many organs themselves have no pain receptors. This happens because pain referral sites are innervated by nerves in the same spinal segment as the original pain location.
Example: Patients with a myocardial infarction frequently experience referred pain to the left arm or jaw.
Nociceptive pain
activated by nociceptors in the peripheral tissue. This represents the normal pain process. This pain is usually responsive to nonopioids and/or opioids (acetaminophen, oxycodone)
Neuropathic pain
Occurs due to a disease process of the nerves, with the pain often following a nerve path. Often chronic but can occur in episodes. Pain is severe.
-Described as “burning, shooting, shock-like, tingling, or stabbing”
**Allodynia
Examples: Peripheral neuropathy, sciatica, phantom limb pain (severe nerve pain in a part of the body that has been amputated; described as burning, twisting, crushing or cramping or as if the limb is being pulled and twisted)
allodynia
(common feature of neuropathic pain) -patient experiences pain in response to a stimulus that isn’t normally painful. For example, a light feather touch, bedsheet on the legs, or a cotton swab can provoke pain.
diabetic peripheral neuropathy
COMMON complication of long-term diabetes mellitus. Metabolic and vascular changes cause damage to peripheral and autonomic nerves (feet, retina). Sensory loss can lead to foot injuries that progresses to infection and gangrene (see example below)
-Numbness, prickling, tingling, stabbing sensation that is worse at night. Allodynia is common.
Example: In a patient with severe diabetic neuropathy, if they step on thumbtack, are exposed to extreme temperatures, if a small rock/object becomes lodged in their shoe, or if dry skin becomes cracked and exposed, they may not feel it at all. These injuries can lead to breakdown and ulcerations (these patients also do not have good wound healing, which puts the patient at further risk for tissue damage). The nurse should teach the patient to do regular foot care and foot checks, podiatry is often part of the care team for patient’s with diabetic neuropathy. *

physiologic factors influencing the pain experience
Age
Misconceptions: (see Table 44.4 on page 1136)**
1)Infants do not feel and cannot express pain
2)Pain is a natural part of growing old, pain perception decreases with age
Facts:
1) Infants cannot verbalize pain, but respond with behavioral cues and physiological indicators that are observable
2) Older people often go undertreated for pain-because pain is viewed as a natural part of aging that should be accepted.
3) Older adults commonly underreport pain because they may expect to have pain with increasing age, do not want to alarm loved ones, are fearful of losing their independence, do not want to distract, anger, or bother caregivers.
4) Pts with Alzheimer’s disease and other cognitive impairments experience pain and their reports of pain are valid; many patients with dementia likely suffer significant unrelieved pain and discomfort. Accept a patient’s report of pain and use relevant pain assessment tools
social factors influencing the pain experience
Each person learns from painful experiences, but prior experience does not mean that a person accepts pain more easily in the future.
Past Pain Experience
*Past pain experiences affect new experiences with pain. If a person repeatedly experiences the same type of pain that was relieved in the past successfully, the person finds it easier to interpret the pain sensation
Some patients have no fear of pain, as they’ve never had severe pain. Their first perception of pain often impairs the ability to cope
Patients who have chronic pain or severe pain who did not get relief may experience feelings of fear, despair, hopelessness
*Anxiety can increase patient’s experience of pain
Family & Social Network
Presence or absence of caring, support people or family can influence pain experience and make it less stressful.
Spiritual Factors
Spiritual beliefs affect the way patients view or cope with pain. Pain has physical and emotional components; often patients can use positive spiritual coping practices such as looking to a higher being for strength and support and they can adjust better to pain. The nurse should provide support for patients to utilize their spiritual practices in managing pain.
psychological factors influencing the pain experience
-The degree to which a patient focuses on pain influences the patient’s perception of pain. Increased attention to pain is associate with increased pain, whereas distraction is associated with a diminished pain response
-The meaning of pain is influenced by the patient’s perception of the degree and quality of the pain; Anxiety and fear often increase pain perception, and pain causes feelings of anxiety and fear
-Patients who are critically ill or injured often perceive a lack of control over their environment and care, which can cause anxiety
cultural factors influencing the pain experience
*Cultural norms related to pain expression
(Example: stoicism vs. loud vocalizations or denial of pain)
*Be knowledgeable about cultural variations in pain expression, alternative methods of pain relief and practices, but never make assumptions or generalizations based on ethnicity
Language differences-communication is critical, as the pain assessment relies on the patient’s feedback. Language barriers can impede pain assessment
Low-income and minority patients are often undertreated for chronic pain, often do not seek treatment for pain for longer periods of time
*Culturally inappropriate pain assessment tools (not using an interpreter), prejudice, and misconceptions often lead to provider bias and undertreatment of pain
nursing process: assessment
Pain assessment should be a routine part of assessment; it is a subjective experience; the nurse must accept that pain exists when a patient reports it
-Set realistic goals for pain control with patient, and include your patient in the care plan; establish an “acceptable level of pain” or a “pain goal” with the patient
-Interprofessional team involvement (pharmacy, provider, nurse, physical and occupational therapy)
-There are multiple pain scales that can be used to accompany the nurse’s pain assessment (“0-10” scale commonly used)
Establish and maintain a trusting therapeutic relationship that fosters open communication and creates an environment that conveys respect. If a patient senses you doubt their pain exists, they may underreport pain or share little information about their pain experience.
ABCDE Approach to pain Assessment & Management:
ASK about pain regularly.
BELIEVE the patient in their report of pain and what relieves it
CHOOSE pain control options appropriate for the patient and setting
DELIVER interventions in a timely, logical, and coordinated fashion
EMPOWER patients and their families. Enable them to control their course to the greatest extent possible
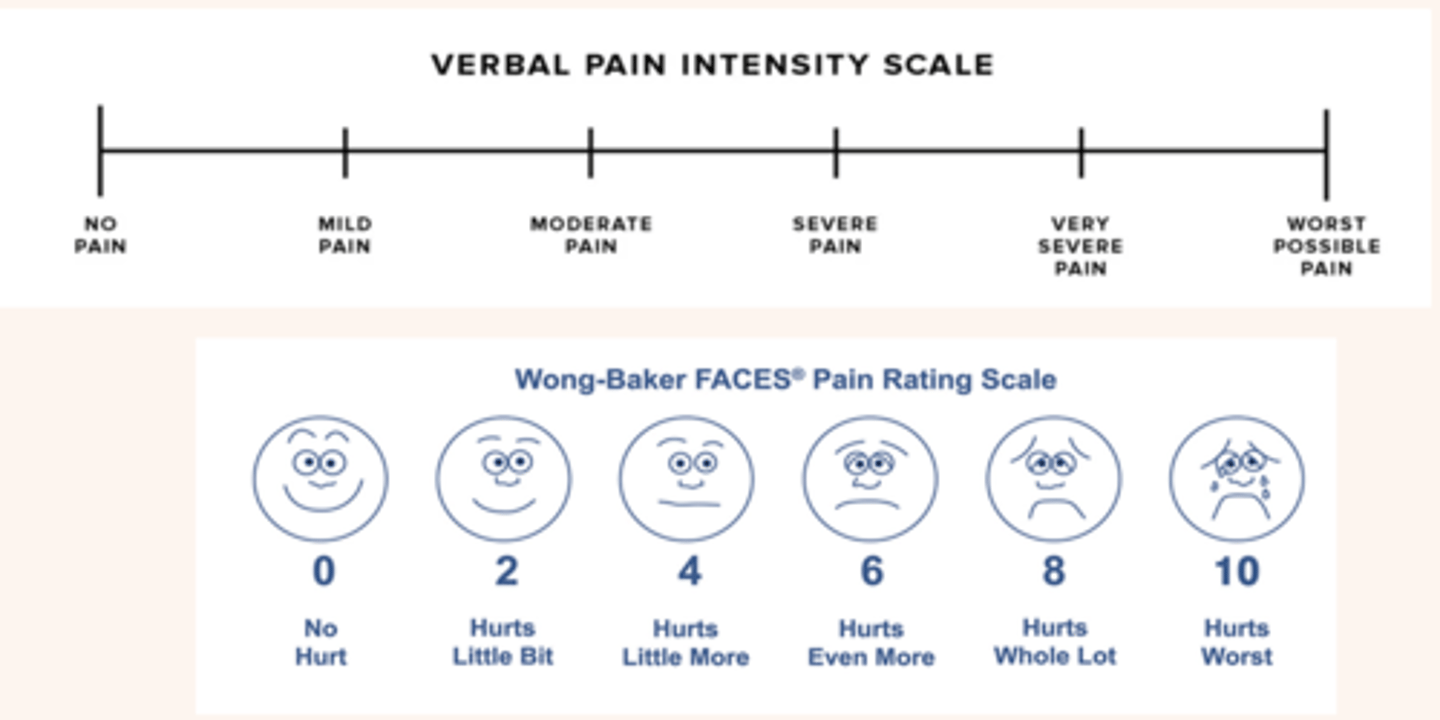
pain scales
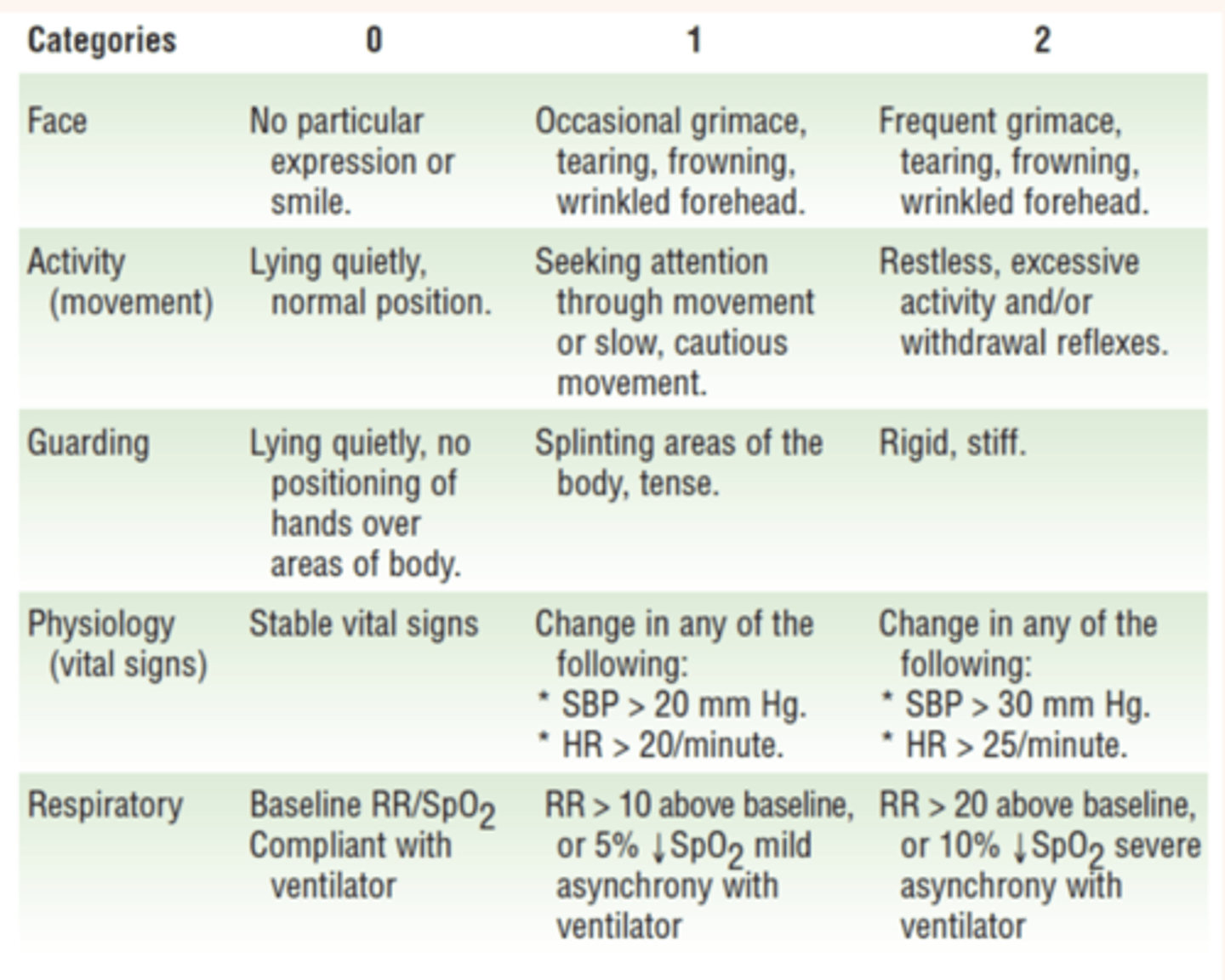
pain scales (2)
Nursing Process: Assessment: “COLD SPA”
Character : describe the pain (sharp, dull, aching, throbbing)
Onset: When did it begin?
Location: Where is it? Does it radiate?
Duration: How long does it last? Does it recur?
Severity: How bad is the pain? (Rate, use scale)
Pattern: What makes it better? What makes it worse? (Aggravating and Alleviating)
Associated factors: What other symptoms occur with your pain?
COLDSPA is a mnemonic to help guide you in your pain assessment.
Use a combination of open-ended and closed-ended communication to gather information about patients’ pain.
Ex. “Tell me more about your pain” elicits more valuable data than “Do you have pain?”

Nursing Process: Analysis & Nursing Diagnosis
Acute Pain related to recent surgery as evidenced by facial expression of pain, need for Acetaminophen 650mg q 4 hours, and patient's statement "I have sharp pain when I move" and a "7/10" pain rating on a scale from 0-10"
Risk for Injury related to decreased pain sensation
Hopelessness related to the belief that the present pain means imminent death
A nursing diagnosis focuses on the specific nature of a patient’s pain to identify the most relevant types of interventions for alleviating pain and improving function.
Nursing Process: Planning & Outcomes Identification
Nursing measures are directed towards achieving the established goals set by the patient and care team collaboratively. Determine relevant and realistic expectations for pain relief. Decide on a mutually acceptable level of pain that allows the patient to return to function.
Priorities change as a patient’s pain experience changes. Consider the type of pain the patient is experiencing and the effect it has on function and quality of life. Any episode of acute pain is a priority because of its potential effects on physical and psychological function. Acute pain can also delay other important therapies (physical therapy, ambulation, diagnostic procedures, wound care)
For chronic pain, work with patients to determine a plan that will decrease pain to a level that will allow the patient to participate in care, restore or improve function in performing ADLs, and prevent complications.
-Collaborate with other members of the care team (APRNs, PharmDs, PT, OT, social workers, psychologists, and clergy)
Nursing Process: Implementation
Pain therapy requires an individualized patient-centered approach. Partner with the patient and family and the entire health care team. Effective pain management requires patience and the ability to be flexible in choosing interventions that are both provider-ordered and that can independently provided.
-Establish trust and open communication with the patient where the patient’s pain experience is validated.
-Use different types of pain relief measures, use measures the patient believes are effective; keep an open mind about ways to relieve pain; when pain is not totally eliminated, focus on improvement in function
-Educate the patient - patients are often better prepared to handle pain when they understand it; adapt educational materials and approaches so that they are suited for patients for low health literacy
Basic Nursing Interventions – there are simple ways to control painful stimuli in a patient’s environment.
Tighten and smooth wrinkled bed linen
Reposition patient in bed to relieve any pressure points
Reposition patient to avoid lying on tubing or IV caps (chest tube, iv tubing)
Loosen constricting bandages (if appropriate)
Change wet dressings and linens
Position patient correctly on a bedpan
Avoid exposing skin or mucous membranes to irritants (urine, stool, wound drainage)
Keep patients clean, dry, and turned if needed
Prevent urinary retention by keeping Foley catheters patent and free flowing if in use
Prevent constipation with fluids, diet, exercise, and stimulant laxatives if needed
Nursing interventions can be pharmacologic or nonpharmacologic.
-Our priority goal for pain management is to find the most appropriate and safe methods to relieve pain
Nonpharmacologic Pain Relief Interventions
USED ALONE OR ALONG WITH PHARMACOLOGICAL THERAPIES
Distraction
TENs unit
Guided Imagery
Acupuncture
Massage
Heat & Ice therapy
Mindfulness, Meditation
Art, Games, TV, Music
Pet therapy
Nonpharmacological strategies can be effective in managing pain. They can be used alone or in combination with pharmacological measures. In the case of moderate to severe pain, nonpharmacological therapies should be used with pharmacological therapies.
The reticular activating system inhibits painful stimuli if a person receives sufficient or excessive sensory input. With sufficient sensory stimuli, the person ignores or becomes unaware of pain. Nonpharmacologic pain-relief interventions reduce patients’ awareness of pain.
-The effectiveness of nonpharmacological therapies often varies depending on the type of pain the patient is experiencing and the patient’s belief in the therapy.
-Cognitive-behavioral interventions change patients’ perceptions of pain, alter pain behavior and provide patients with a greater sense of control (distraction, prayer, mindfulness)
-Physical therapies (hot or cold compresses, massage, exercise, TENS) treat pain by improving physical function, altering physiological responses and reducing pain-related immobility
-Nonpharmacological interventions act on the physiological, emotional, and psychological aspects of pain
analgesic pharmacological intervention
A multimodal approach is recommended for acute and chronic pain relief. Use nursing judgment in the use and management of analgesics with out without other pain therapies to ensure the best pain relief possible.
Definitions:
Analgesic- any pharmacologic agent that relieves pain
There are 3 types of analgesics:
Nonopioid analgesics - acetaminophen and NSAIDs
Opioid analgesics - narcotics, controlled substances like morphine, codeine, oxycodone, Vicodin
Adjuvant drugs - are drugs in other classes that are typically used for other purposes, but that also relieve certain types of pain. They can be anticonvulsants, antidepressants; gabapentin is an example). These medications enhance analgesics or have analgesic properties
-Pharmacologic pain management is complex and requires a thorough and accurate assessment. It is the foundation of many pain medication plans.
-Drug safety, knowledge of medications, patient teaching, and an interprofessional approach required
-Know side effects, interactions
-Communicate with a provider regarding a patient who is undermedicated or who needs a different drug or route of administration (advocate for your patient)
-Challenges exist with provider/nurse lack of confidence in prescribing opioids safely and how to detect abuse of emerging addiction, leading to pain that is not appropriately managed
-KNOW YOUR DRUGS
nonopioid analgesics
Non-opioid Analgesics include acetaminophen and NSAIDS
-Simple dosage schedules
-Safe, well-tolerated
-Least invasive pain management modality
-Available OTC or prescribed
-Combining nonopioid analgesics and opioids provides more analgesia than either drug taken alone
Side effects:
Gastric upset (take with food or antacids)
GI bleeding, interference with platelet function (NSAIDs)
Hepatoxicity (at high doses and for long periods of time)
Opioid analgesics
also called narcotic analgesics, are the major class of drugs used to treat moderate to severe pain because of their effectiveness. They act on higher centers in the brain and spinal cord by binding with opioid receptors to modify perceptions of pain.
Examples include: morphine, codeine, hydromorphone, fentanyl, oxycodone, and hydrocodone
Follow provider orders- regarding dosing intervals, utilize the provider’s orders
Opioids commonly are ordered as “prn range orders” (example “morphine 2 to 6mg IV q 2hr prn for pain). Nurses base decisions about the administration of range orders on a thorough pain assessment and knowledge of the drug to be administered.
-Opioids relieve pain that is :
*peripheral/nociceptive
*acute pain due to injury
*Arthritis/chronic pain
*Cancer pain (often intractable and difficult to treat without opioids)
Opioid Analgesics: Side Effects
Most common side effects are:
- Sedation –monitor frequently
-Constipation –increase fluid and fiber intake*
-Nausea –administer antiemetics
-Respiratory depression –monitor closely, administer naloxone if necessary
-Respiratory depression is a common and serious adverse effect of opioids, but it is an uncommon occurrence in patients who have used opioids for a long time because of the tolerance they’ve developed. Patients most at risk include those who are opioid naïve (patients who have taken opioids around the clock less than 1 week), patients who have obstructive sleep disorders, patients who are on high-dose opioids, or who are taking opioids with other sedative medications.
-Sedation always occurs before a patient experiences respiratory depression; monitor patients closely for sedation when they are taking opioids.
Narcan (naloxone) is a medication that works to reverse respiratory depression patients by blocking the action of the opioid at receptor site
*Patient education is needed to reduce patient fears surrounding the use of opioids for pain relief:
Physical dependence - The body is physiologically used to opioid therapy and withdrawal symptoms occur if the opioid is suddenly withdrawn. Common symptoms include shaking, chills, abdominal cramps, excessive yawning, and joint pain
Tolerance - When the body becomes used to the opioid and needs a larger dose (up to 10x the original dose) for pain relief
Addiction - compulsive drug seeking and use, despite harmful consequences, drug craving
Physical dependence and tolerance (expected responses) are NOT the same as addiction. Patients who have a history of substance abuse should still be treated for pain. Treat patients with addiction and pain with the same amount of dignity and respect for all patients.
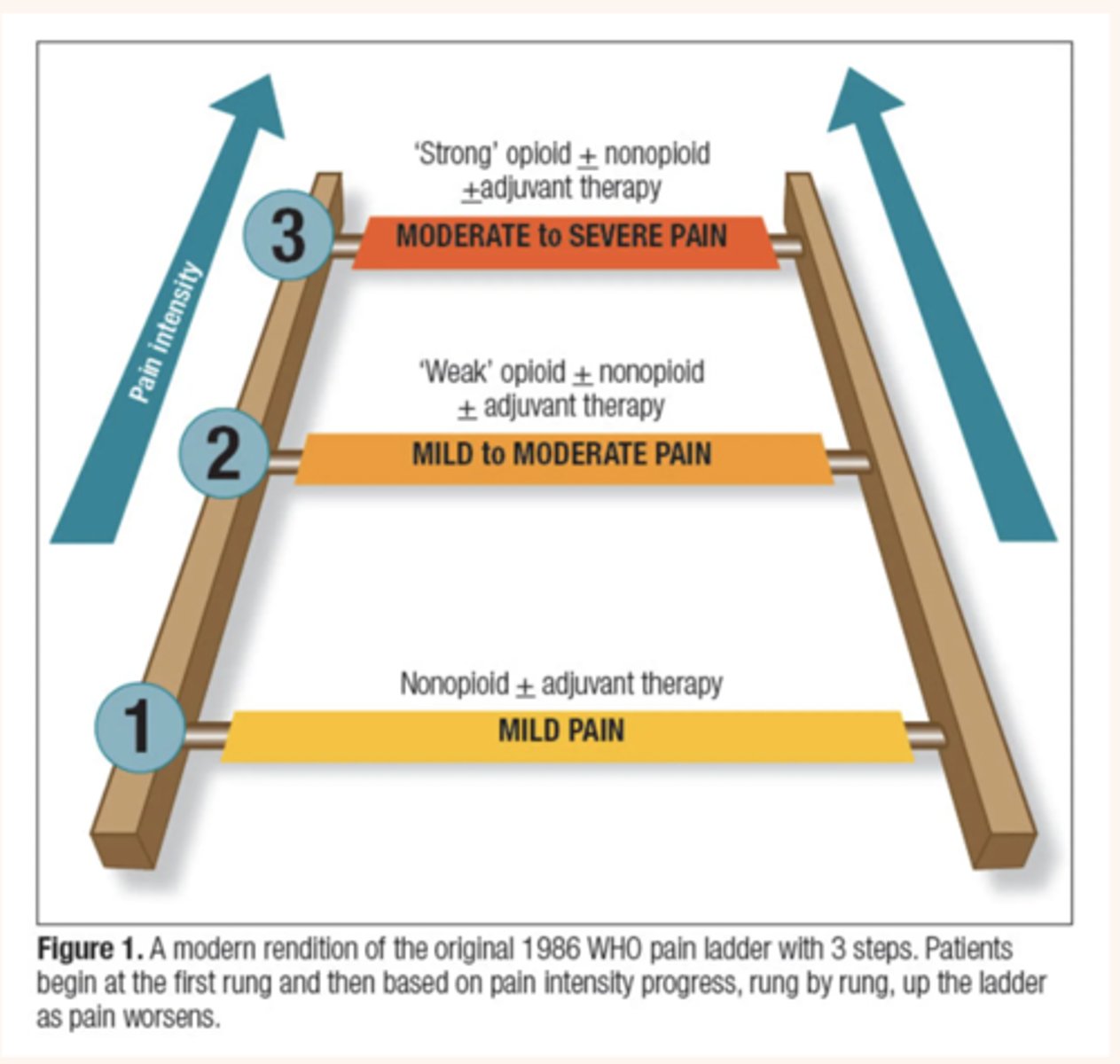
A depiction of the WHO (World Health Organization’s) pain management ladder that shows the progression of the medications that we use to treat mild, moderate and severe pain.
Often a multimodal approach is used, meaning that there is a combination of a nonopioid like acetaminophen with an opioid like oxycodone to make Percocet. These drugs are synergistic and work well to maximize pain relief with fewer adverse effects
1)MILD PAIN: Acetaminophen, NSAIDS (nonopioids)
2)MILD to MODERATE PAIN: “weak opioids” tramadol, codeine
3)MODERATE to SEVERE PAIN: “strong” opioids (morphine, oxycodone, hydromorphone)
Nursing Principles for Administering Analgesics
Know Patient’s Previous Response
-Patient allergies, sensitivities to drug
-At risk for using NSAIDs (hx of GI bleeding or renal insufficiency) or opioids (hx of obstructive sleep apnea, opioid naive)
-Identify previous doses and routes of analgesic administration to avoid undertreatment
-Determine whether patient obtained relief with previous doses
Select Proper Medications When More than One is Ordered
-Consult with HCP to use nonopioid analgesic or opioid combination drugs for mild to moderate pain
-Recommend opioids with nonopioids to provide multimodal analgesia (combining drugs with at least two different mechanisms of action to optimize pain control; multimodal regimens lower the risk of side effects while providing pain relief that is as good or even better than could be obtained from each of the medications alone)
-Avoid using multiple opioids with the same duration and mechanism of action
-IV medications act more quickly and usually relieve severe acute pain within 1 hour; oral medications take as long as 2 hours to relieve pain
-Avoid intramuscular analgesics, especially in older adults
-For chronic pain, give oral medications ATC
Know Accurate Dosage
-Adjust doses as appropriate for children and older patients
-Large doses of opioids are acceptable in opioid tolerant patients but not in opioid-naïve patients
-When titrating an opioid, titrate to effectiveness
Assess Right Time and Interval for Administration
-Administer analgesics as soon as pain occurs and before it increases in severity
-Give analgesics before pain-producing procedures or activities (PT, wound care)
-Know the average duration for a drug and the time of administration so that the peak effect occurs when the pain is most intense
Around the Clock (ATC) Dosing one way to maximize pain relief while potentially decreasing opioid use is to administer analgesics around the clock (ATC) or at schedule times rather than a prn basis. This approach ensures a more constant therapeutic blood level of an analgesic. An ATC medication lessens the severity of end-of-dose pain, allowing a patient to sleep through the night and reduce “clock watching” for the next dose of pain medication
Alternative Routes of Pharmacologic Delivery: Epidural
Epidural analgesia is effective in providing pain relief in certain situations like after abdominal and thoracic surgeries and during labor, and with chronic cancer pain.
-A catheter is inserted into the epidural space between the walls of the vertebral canal and dura mater and the opioid medication delivered acts directly on the opioid receptors in the spinal cord.
-Pain relief is able to be achieved with small doses.
-Medication delivered by continuous infusion pump or by PCEA pump
-Usually morphine or fentanyl
Nursing Care for Patients Receiving Epidural Opioids
Provide emotional support the patients receiving epidural by explaining the insertion technique and warning patients that they will temporarily lose sensory function within minutes of the injection. Motor and autonomic (bowel and bladder control) function may also be lost quickly. It is common for patients to fear paralysis because the epidural injection come close to the spinal cord. Explain to the patient that numbness, tingling and coldness are common.
*Verify provider order, drug prep, and infusion rate
Narcan should be available
Only use epidural tubing and label tubing as such***
*Assess and record sedation level, vital signs closely throughout infusion
Notify provider for : an increase in patient sedation, or decrease in respiratory rate**
*Monitor for side effects, hypotension, pruritis, n/v, bladder and bowel distention
Maintain catheter function, check external dressing around catheter site for dampness or discharge
Secure catheter carefully to outside skin to prevent displacement of the catheter
Patient Controlled Analgesia
a drug delivery system that allows patients to self-administer opioids with minimal risk of overdose**. The goal is to maintain a constant blood level of analgesic to avoid the problems of prn dosing
-Most commonly used to deliver analgesics intravenously or subcutaneously
-Patient is in charge of the pain management program, offers more autonomy, less anxiety about achieving pain relief
-Consistent analgesic blood level is maintained
-Can be used in the hospital or at home
PCA system consists of:
-Computerized portable infusion pump containing a chamber for a syringe that is prefilled with the prescribed opioid analgesic
-The machine is programmed to give a dose to the patient when they press a button that activates the device
-When the pain sensation occurs, they press the button to deliver a small bolus of medication
-There is a preset interval of time, usually where the patient won’t be able to receive additional medication if the button is pressed (lock out feature)
-The pump can also be programmed to deliver only a specific amount of analgesic per hour
Nursing Considerations:
-Only patients who are alert and who can use the unit (locate and press the button) should have a PCA
-Very young children, cognitively impaired adults, or patients who are at risk for over sedation/ respiratory depression (asthma, sleep apnea) are not candidates for PCA
-Teach the patient to press the button for their PCA pump when they have pain
-The button should NEVER be pressed by anyone other than the patient (this includes the family member and the nurse) (known as PCA by proxy)
key factors in managing pain
-Empower the patient to take charge of their own pain relief measures. Determine what works best for the patient and develop an individualized care plan.
-Review the pain scale, understand patient goals. What is an acceptable pain goal for the patient?
-Use pain control measures BEFORE pain gets severe
-Be open-minded about non-pharmacologic strategies
-Accurate documentation of pain and follow up documentation necessary to determine if pain relief is effective
-Time analgesics appropriately (example, offer an analgesic prior to ambulating a post-op patient with knee replacement)
-Use the lowest effective dose of an opioid needed