GI Bleed - Rutland
1/41
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
42 Terms
bleeding proximal to ampulla of vater is considered what type of bleed
upper gi bleed
GI bleed distal to terminal ileum is considered
lower gi bleed
four Qs in GI bleed
is there GI bleeding?
what is the magnitude of the bleeding?
is the bleeding, upper, mid or lower GI
is there a spec therapy?
what is the most important aspect in the care of gi bleeding
estimation and replacement of blood loss
don’t tilt if pulse
>120
varices
arterial spurting
visible vessel
ulcers >2cm
posterior duodenal bulb ulcers
endoscopic prognostic indicators
is bleeding UGI
hematemesis
melena
BUN >40
NG lavage showing UGI bleeding
if pt has portal HTN, start
octreotide asap rocky
when is the best time to scope a pat
stable
clear stomach debris
painless upper GI bleed
mucosal tear near GEJ, usually on gastric side
most stop bleeding on its own
Mallory-Weiss tear
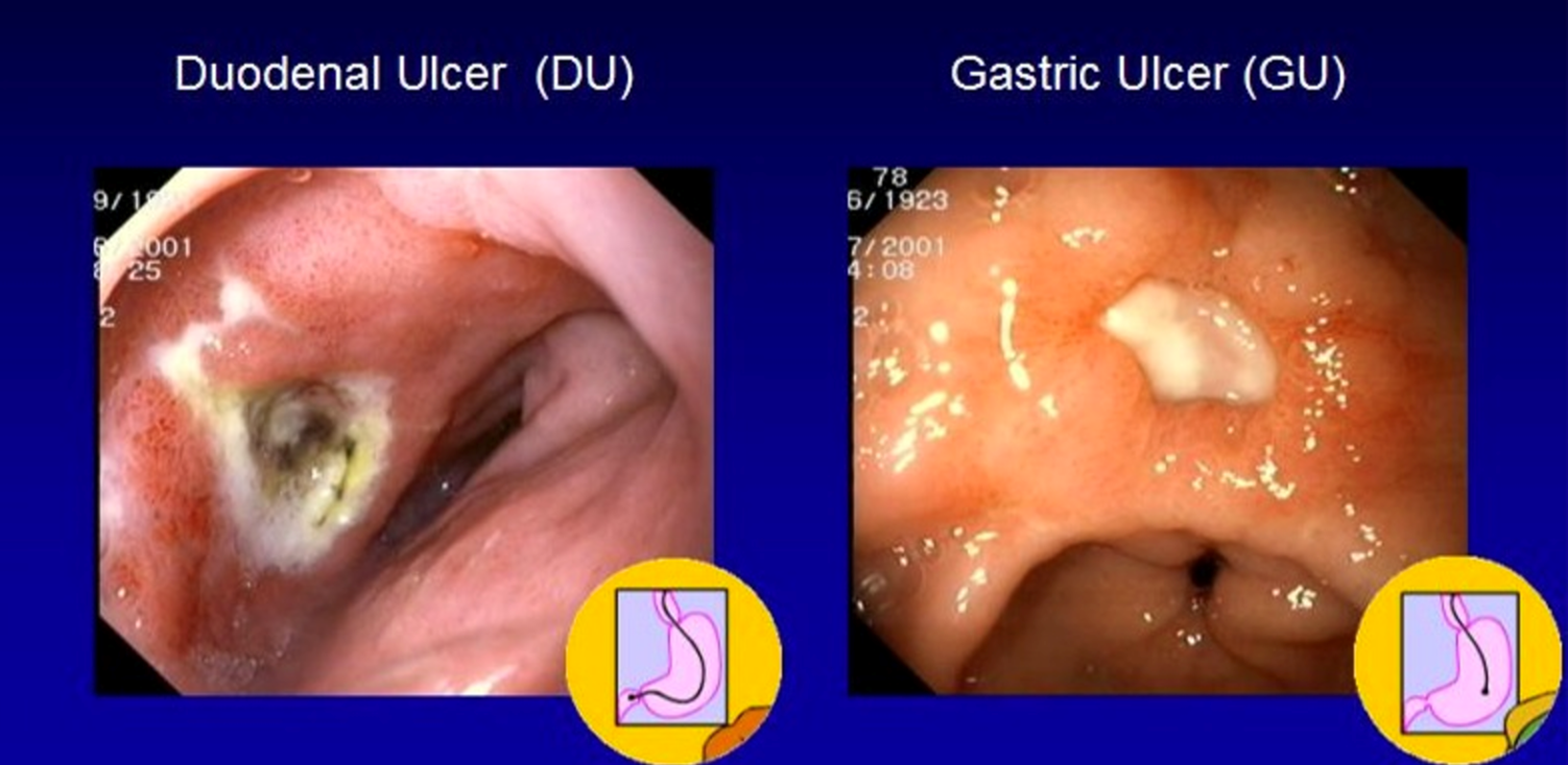
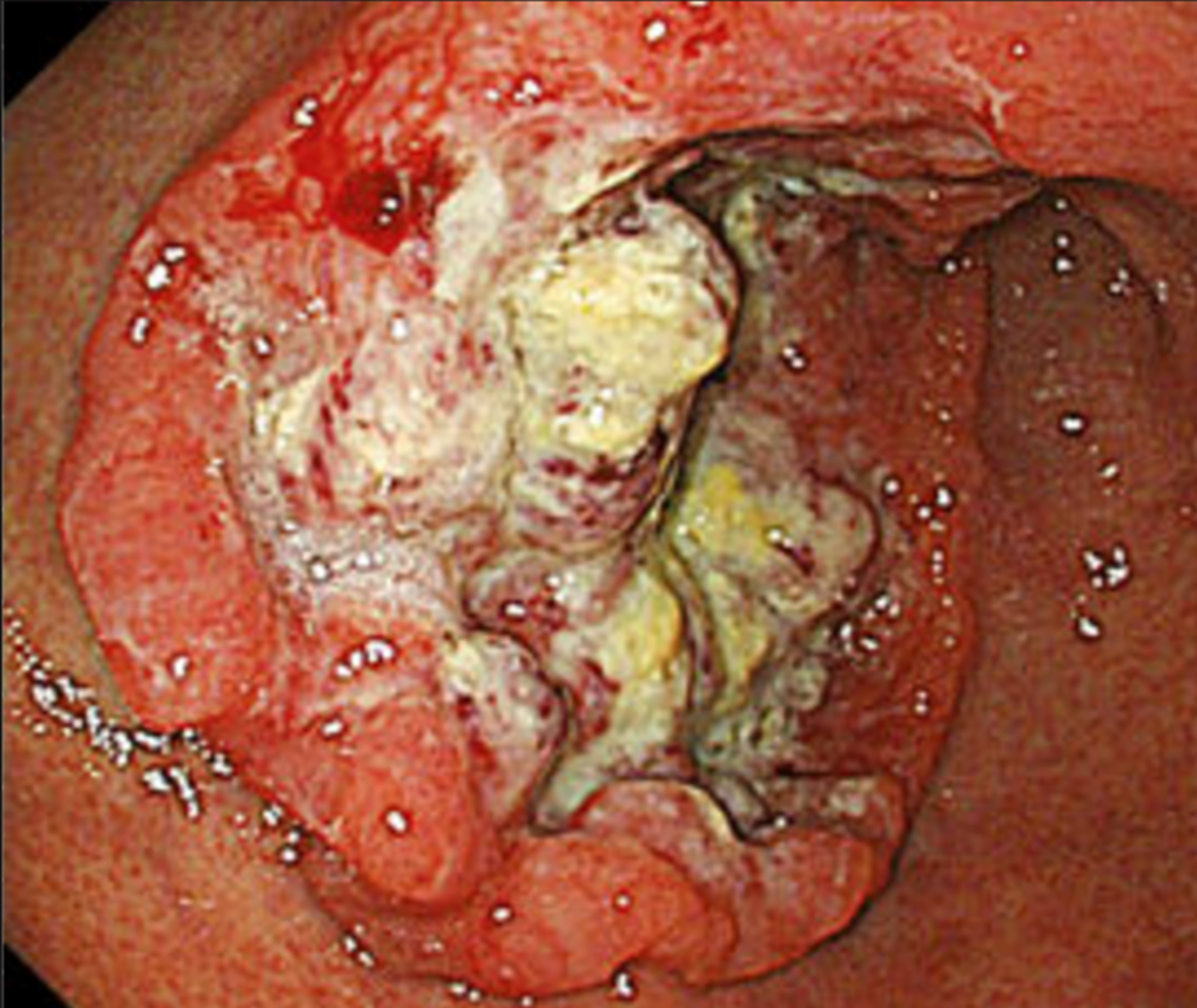
ulcers
5mm or larger break in GI mucosa
most H Pylori and NSAIDS
peptic ulcers
90% of duodenal ulcers
h pylori
how does h pylori damage mucosa
production of ammonia, proteases, lipases, phospholipases, mucinases
local immune response
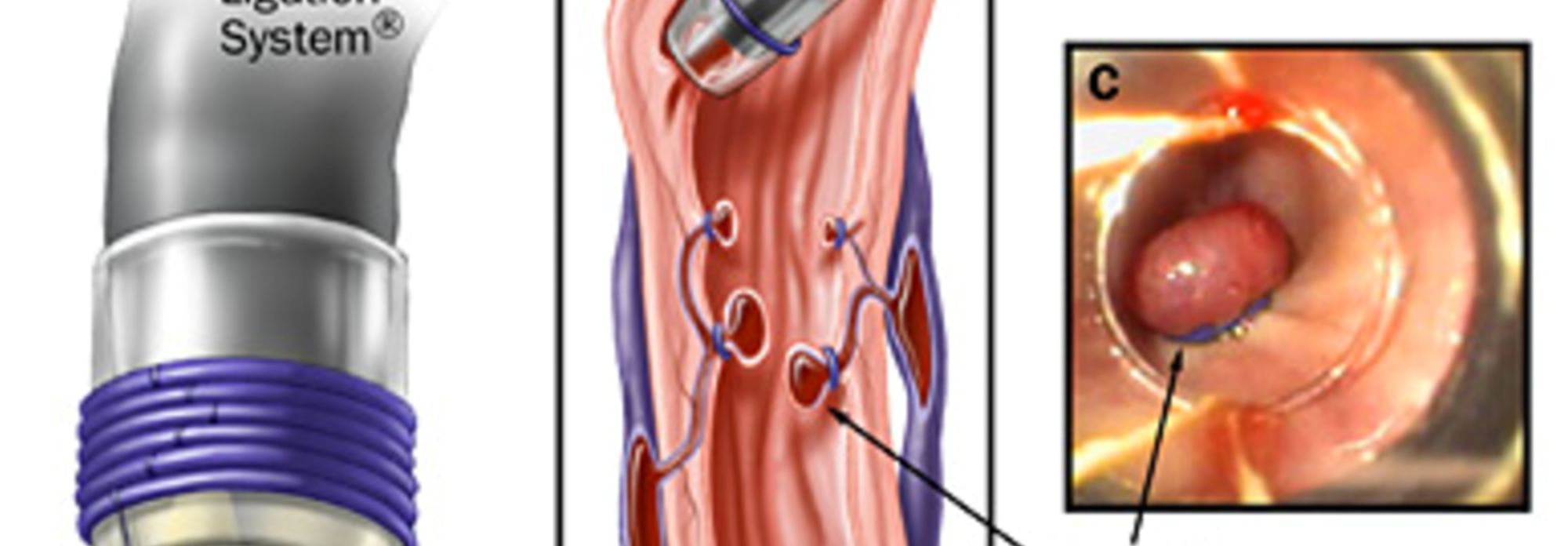
mechanical hemostasis
hemostatic clips
ligation bands
tamponade
develop to decompress portal vein
varices
varices
pharm for variceal bleeding
OCTREOTIDE
inhibits release of glucagon’decreases portal venous pressure and direct vasoconstrictive effect on splanchnic arteriolar smooth muscle
somatostatin analogues
controls bleeding
lowre mortality
fewer complications
fewer sessions
variceal band ligation
last resort bleeding
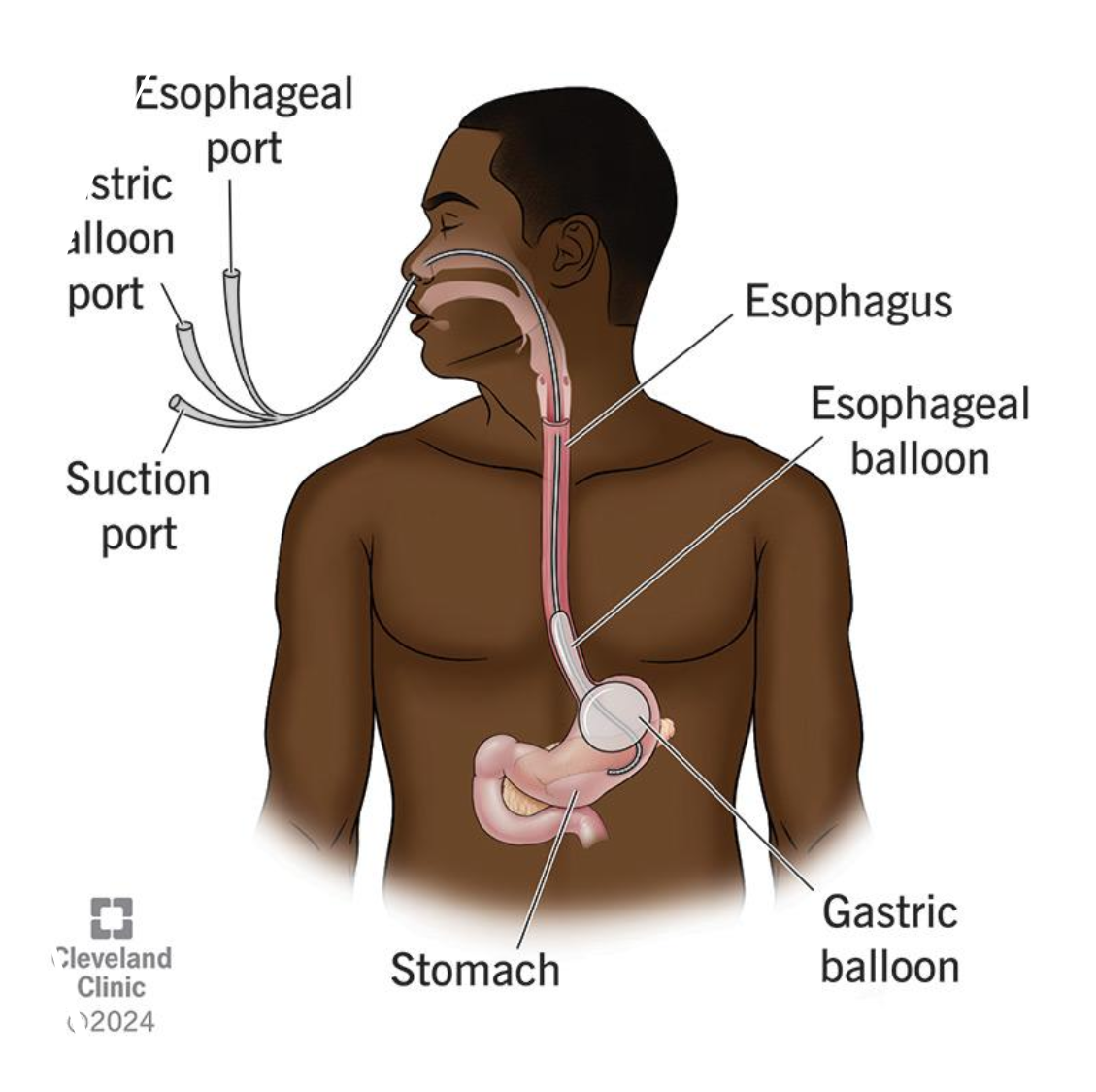
balloon tamponade
arrest bleeding, buys time
SO much complications, doesn’t prolong survival

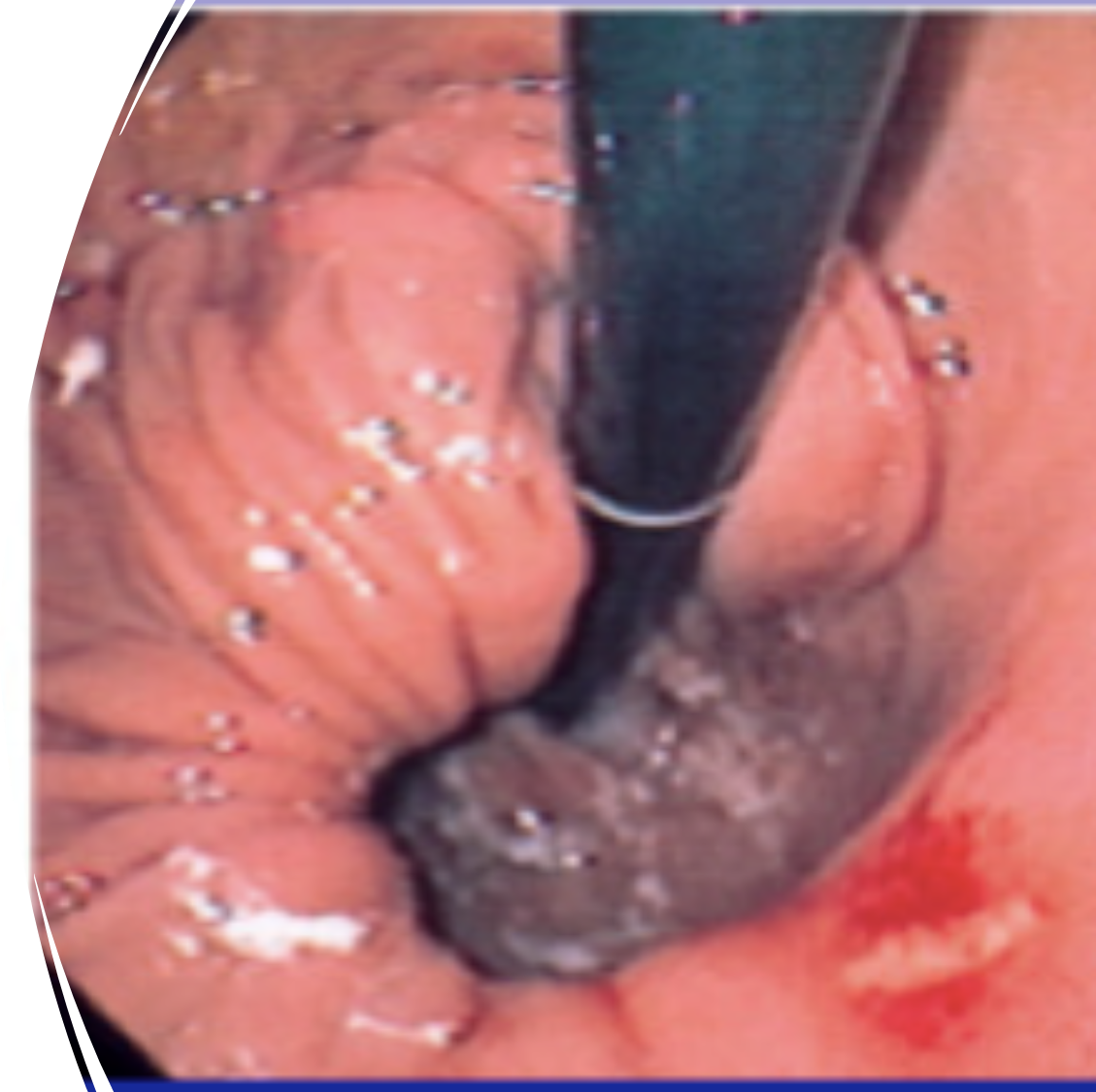
large submucosal artery
proximal stomach
intermittent painless massive bleeding
hard to ID
dieulafoy lesion
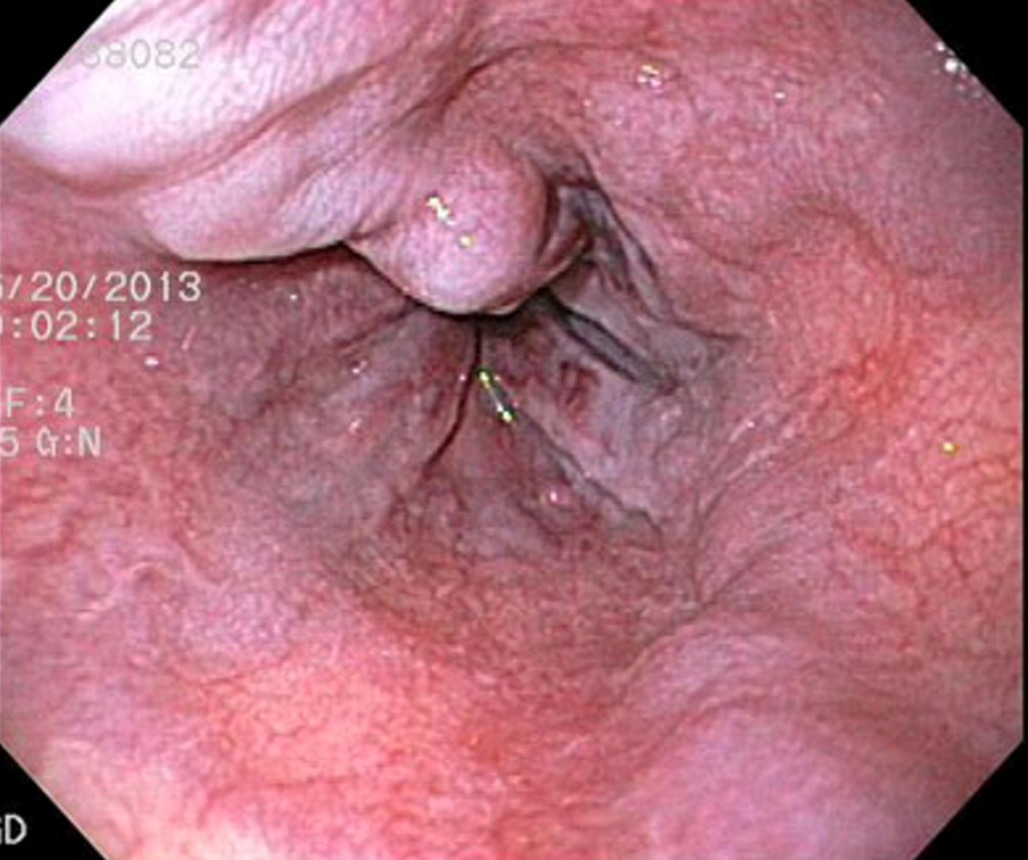
linear erosion in a hiatal hernia
chronic or acute bleeding
painless
cameron’s lesions

AV malformation
osler weber rendu
ehlers danlos
CREST
AVMs can be assoc with
AVMs most common where
stomach and duodenum
gastric cancer
high risk timing of endoscopy (UGIB)
within 12 hours
hemodynamic instability
ongoing bleed
sus varices
timing of endoscopy for standard UGIB
within 24 hours
low risk UGIB
early discharge
hematochezia most commonly indicates
colonic source
hemorrhoids
diverticular bleeding
vascular ectasia
neoplasm
ischemic colitis
IBD
infxn
radiaiton proctitis
lower GI bleed
acute blood loss
right sided diverticular more likely to bleed bc why
ostia wide
thinner colonic wall
pain
low vol hematochezia
h/o ab vasc surg
estrogen therapy, smoking
hypercoag
large vessel disease rarely found
spont resolution
ischemic colitis
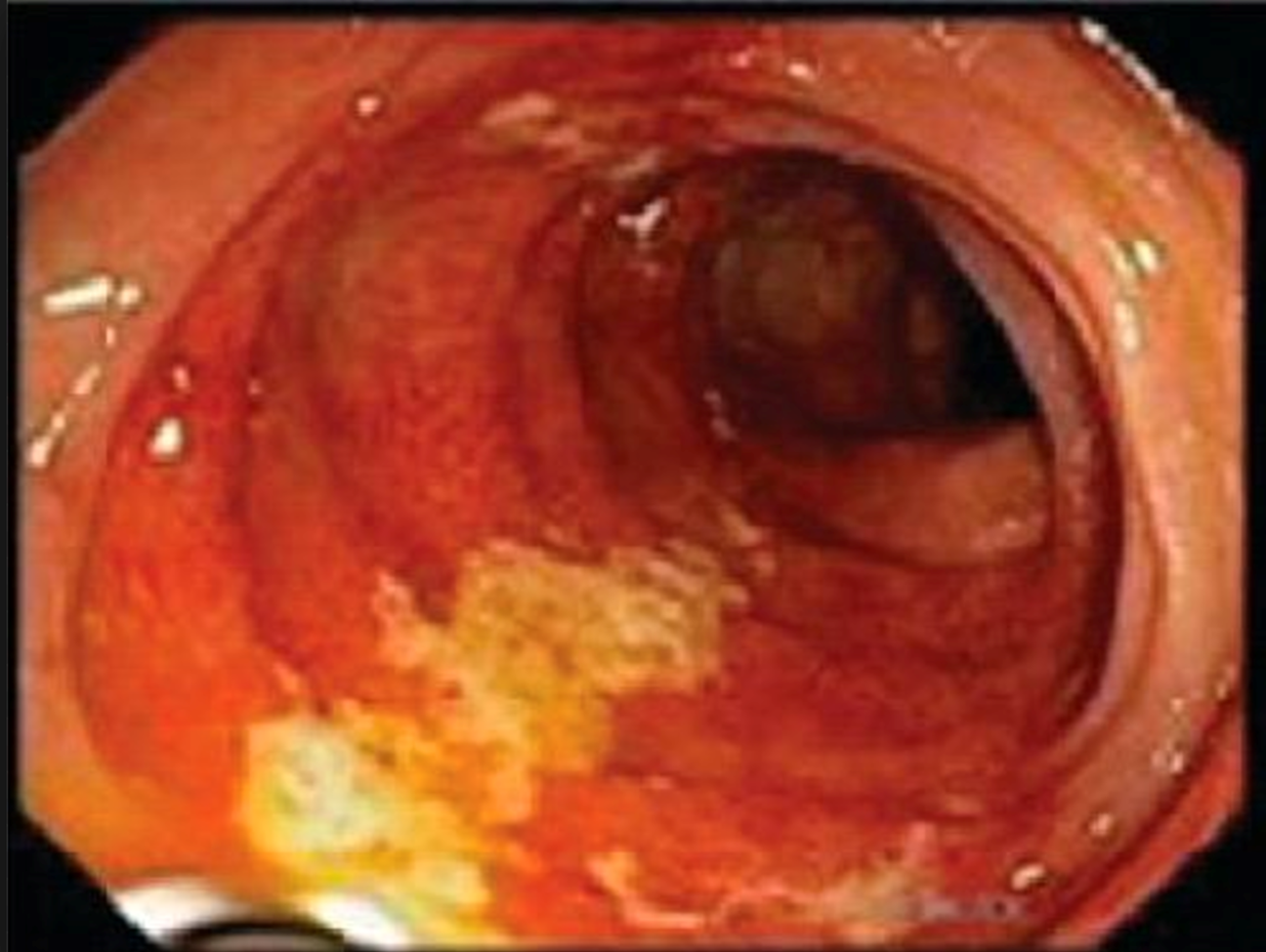
white stripe sign
ischemic colitis
grossly bloody diarrhea
IBD
benign rectoanal disease
hemorrhoids
anal fissures
stercoral ulcers
solitary rectal ulcer syndrome
after EGD and colonscopy, 5% bleeds unexplained still
MIDGI bleed
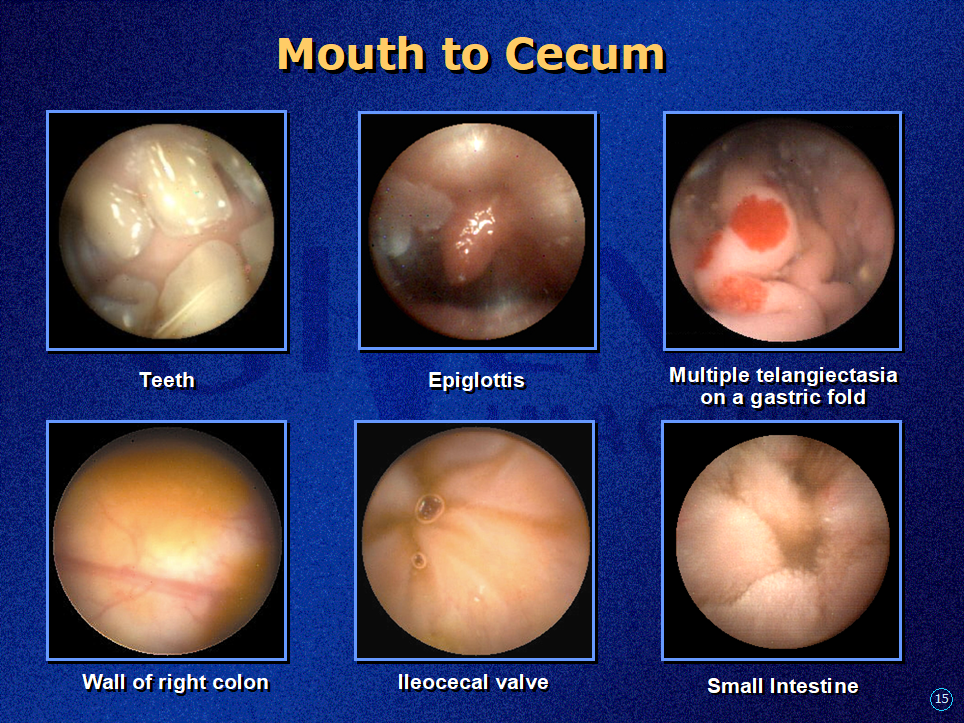
pillcam view
if they said they bled …
they bled
when in doubt
CALL GASTROENTEROLOGY
primary job in GI bleeds
prevent or treat consequences of blood loss