MLS 320L
1/41
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
42 Terms
Where is CSF primarily produced?
a. Arachnoid villi
b. Choroid plexus
c. Ependymal lining of spinal cord only
d. Dural sinuses
b. Choroid plexus
What is a major function of CSF?
a. Cushioning the brain and spinal cord against mechanical injury
b. Regulation of systemic blood pressure
c. Production of immune cells
d. Filtration of plasma proteins
a. Cushioning the brain and spinal cord against mechanical injury
What is the normal appearance of CSF?
a. Slightly haze due to protein content
b. Pale yellow
c. Slightly opalescent
d. Clear and colorless
d. Clear and colorless
Which tube is used for microbiology testing?
a. Tube 1 due to highest protein content
b. Tube 2 to minimize contamination and preserve organisms
c. Tube 3 due to lowest cell count
d. Any tube if processed immediately
b. Tube 2 to minimize contamination and preserve organisms
Why is Tube 3 preferred for hematology?
a. It contains the highest concentration of leukocytes
b. It preserves RBC morphology
c. It has the lowest protein concentration
d. It is least affected by peripheral blood contamination during collection
d. It is least affected by peripheral blood contamination during collection
Why is Tube 1 used for chemistry testing in CSF analysis?
a. Best for cell count accuracy
b. Preserves organism viability
c. Less affected by RBC contamination for chemical tests
d. Lowest protein concentration
c. Less affected by RBC contamination for chemical tests
If only one CSF tube is collected, which department tests it first?
a. Hematology to prevent cell lysis
b. Chemistry for protein analysis
c. Microbiology to preserve organism viability
d. Cytology for malignancy screening
c. Microbiology to preserve organism viability
Which condition makes CSF results uninterpretable?
a. Slight turbidity
b. Presence of a clot interfering with cell counts
c. Mild xanthochromia
d. Slightly elevated protein
b. Presence of a clot interfering with cell counts
CSF should be processed how quickly?
a. Within 2 hours
b. Within 24 hours
c. STAT/ASAP
d. Anytime after refrigeration
c. STAT/ASAP
What is xanthochromia?
a. Increased turbidity
b. Yellow-orange discoloration
c. Elevated protein concentration
d. Presence of bacteria in CSF
b. Yellow-orange discoloration
What is the primary cause of xanthochromia in CSF?
a. Increased protein permeability across the blood-brain barrier
b. Bacterial metabolism producing pigments
c. Elevated WBC count causing turbidity
d. Breakdown of RBCs releasing hemoglobin degradation products
d. Breakdown of RBCs releasing hemoglobin degradation products
Which condition causes xanthochromia?
a. Traumatic tap
b. SAH
c. Visual infection
d. Dehydration
b. SAH
In a traumatic tap, RBC count across tubes
a. Remains consistent due to uniform bleeding
b. Increases due to clotting
c. Decreases progressively as collection continues
c. Decreases progressively as collection continues
In a true hemorrhage (SAH), RBC count across tubes
a. Remains consistent due to uniform bleeding
b. Increases due to clotting
c. Decreases progressively as collection continues
a. Remains consistent due to uniform bleeding
CSF clot formation is most associated with
a. SAH due to fibrin formation
b. Normal CSF
c. Viral meningitis
d. Traumatic tap introducing plasma proteins and clotting factors
d. Traumatic tap introducing plasma proteins and clotting factors
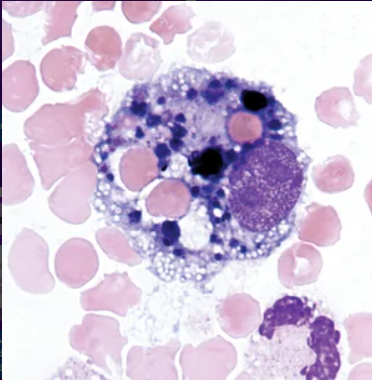
What are siderophages in CSF?
a. Macrophages containing hemosiderin from hemoglobin breakdown
b. Macrophages containing lipid droplets from cell membrane degradation
c. Macrophages containing nuclear debris from apoptotic cells
d. Monocytes accumulating ferritin due to increased serum iron levels
a. Macrophages containing hemosiderin from hemoglobin breakdown
Siderophages are seen in:
a. Traumatic tap
b. True hemorrhage
c. Normal CSF
d. Viral meningitis
b. True hemorrhage
What is normal WBC count for an adult?
a. 0-5 cells/uL
b. 5-15 cells/uL
c. 10-20 cells/uL
d. >100 cells/uL
a. 0-5 cells/uL
What is normal CSF RBC count
a. 0-1 cells/uL
b. 5-10 cells/uL
c. <50 cells/uL
d. >100 cells/uL
a. 0-1 cells/uL
Why is acetic acid used in WBC count?
a. To enhance staining of nuclei
b. To preserve WBC morphology
c. To lyse RBCs and improve visualization of nucleated cells
d. To prevent clotting
c. To lyse RBCs and improve visualization of nucleated cells
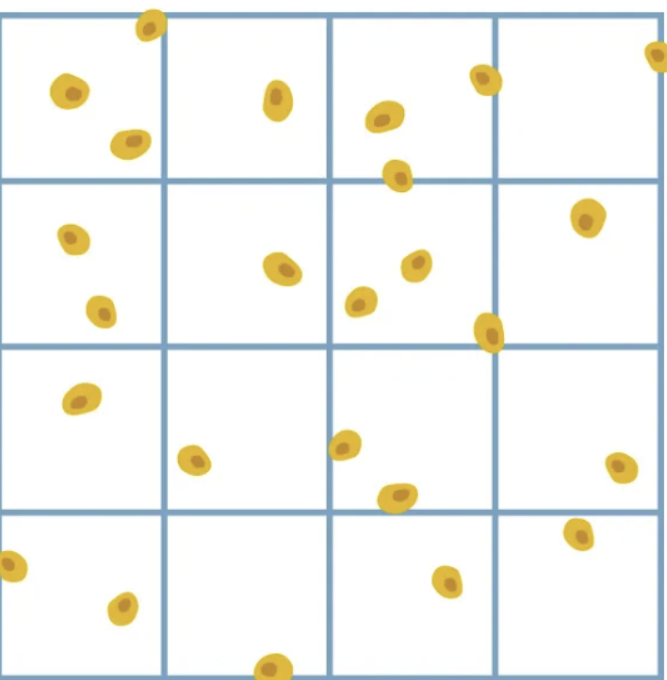
Cells touching which lines are counted?
a. Top and bottom
b. Right and bottom
c. Top and left lines
d. Right and left lines
c. Top and left lines
Purpose of cytocentrifuge
a. Separate plasma from cells
b. Increase sample volume
c. Concentrate cells into monolayer
d. Lyse unwanted cells
c. Concentrate cells into monolayer
Cytocentrifuge increases cell concentration by approximately
a. 5-fold
b. 10-fold
c. 20-fold
d. 50-fold
c. 20-fold
Why is albumin added in cytospin prep
a. To enhance cell adherences add preserve morphology
b. To lyse RBCs
c. To enhance stain cells
d. To reduce viscosity
a. To enhance cell adherences add preserve morphology
If fewer than 100 cells are present:
a. Estimate percentage out of 100 cells
b. Perform count of second slide to meet 100 cells counted
c. Report as less than 100 cells observed
d. Report actual number counted with cell types observed
d. Report actual number counted with cell types observed
Predominant normal CSF cells
a. Neutrophils
b. Lymphocytes and monocytes/macrophages
c. Macrophages only
d. Plasma cells
b. Lymphocytes and monocytes/macrophages
Neutrophils in CSF indicate
a. Viral infection
b. Bacterial infection, especially acute meningitis
c. Usually normal in CSF
d. Chronic inflammation only
b. Bacterial infection, especially acute meningitis
Reactive lymphocytes are associated with
a. Acute bacterial meningitis
b. Viral infections and immune response activation
c. Traumatic tap
d. SAH
b. Viral infections and immune response activation
Ependymal cells are
a. Macrophages that have migrated into CSF
b. Tissue lining cells of ventricles
c. Choroid plexus epithelial cells involved in CSF filtration
d. Reactive lymphocytes with irregular nuclear morphology
b. Tissue lining cells of ventricles
Bacterial meningitis predominant cells
a. Lymphocytes
b. Monocytes
c. Neutrophils
d. Eosinophils
c. Neutrophils
Fungal/TB meningitis predominant cells
a. Lymphocytes
b. Monocytes
c. Neutrophils
d. Eosinophils
a. Lymphocytes
Serous fluids include
a. CSF, synovial, urine
b. Plasma and lymph
c. Interstitial and intracellular fluids
d. Pleural, peritoneal, and pericardial fluids
d. Pleural, peritoneal, and pericardial fluids
Effusion is defined as
a. Accumulation of excess fluid in a body cavity
b. Infection of a cavity
c. Inflammation of a cavity
d. Hemorrhage
a. Accumulation of excess fluid in a body cavity
Thoracentesis removes fluid from
a. Peritoneal cavity
b. Pleural cavity
c. Pericardial sac
d. Joint cavity
b. Pleural cavity
Transudate is caused by
a. Inflammatory damage
b. Infection
c. Altered hydrostatic/oncotic pressures
d. Trauma
c. Altered hydrostatic/oncotic pressures
Exudate is associated with
a. Normal physiology
b. Inflammatory process
c. Low protein states
d. Dehydration
b. Inflammatory process
Exudate protein levels are
a. Low relative to serum
b. Equal to serum
c. Absent
d. Greater than 50% of serum protein levels
d. Greater than 50% of serum protein levels
Transudate appearance
a. Clear to pale yellow
b. Cloudy and cellular
c. Bloody
d. Green
a. Clear to pale yellow
Mesothelial cells are
a. Reactive macrophages in serous fluids
b. Epithelial-like cells lining serous membranes
c. Synovial lining cells of joint spaces
d. Malignant epithelial cells in effusions
b. Epithelial-like cells lining serous membranes
Key features of mesothelial cells
a. High nuclear to cytoplasmic ratio
b. Absence of cytoplasm
c. Single eccentric nucleoli
d. Low N:C ratio and possible multinucleation in clusters
d. Low N:C ratio and possible multinucleation in clusters
Monosodium urate crystals indicate
a. Rheumatoid arthritis
b. Septic arthritis
c. Gout with strong birefringent needle shaped crystals
d. Pseudogout with rhomboid crystals and weak birefringence
c. Gout with strong birefringent needle shaped crystals
CPPD crystals indicate
a. Rheumatoid arthritis
b. Septic arthritis
c. Gout with strong birefringent needle shaped crystals
d. Pseudogout with rhomboid crystals and weak birefringence
d. Pseudogout with rhomboid crystals and weak birefringence