Pharm II Week 8 (Antiretroviral Agents)
1/69
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
70 Terms
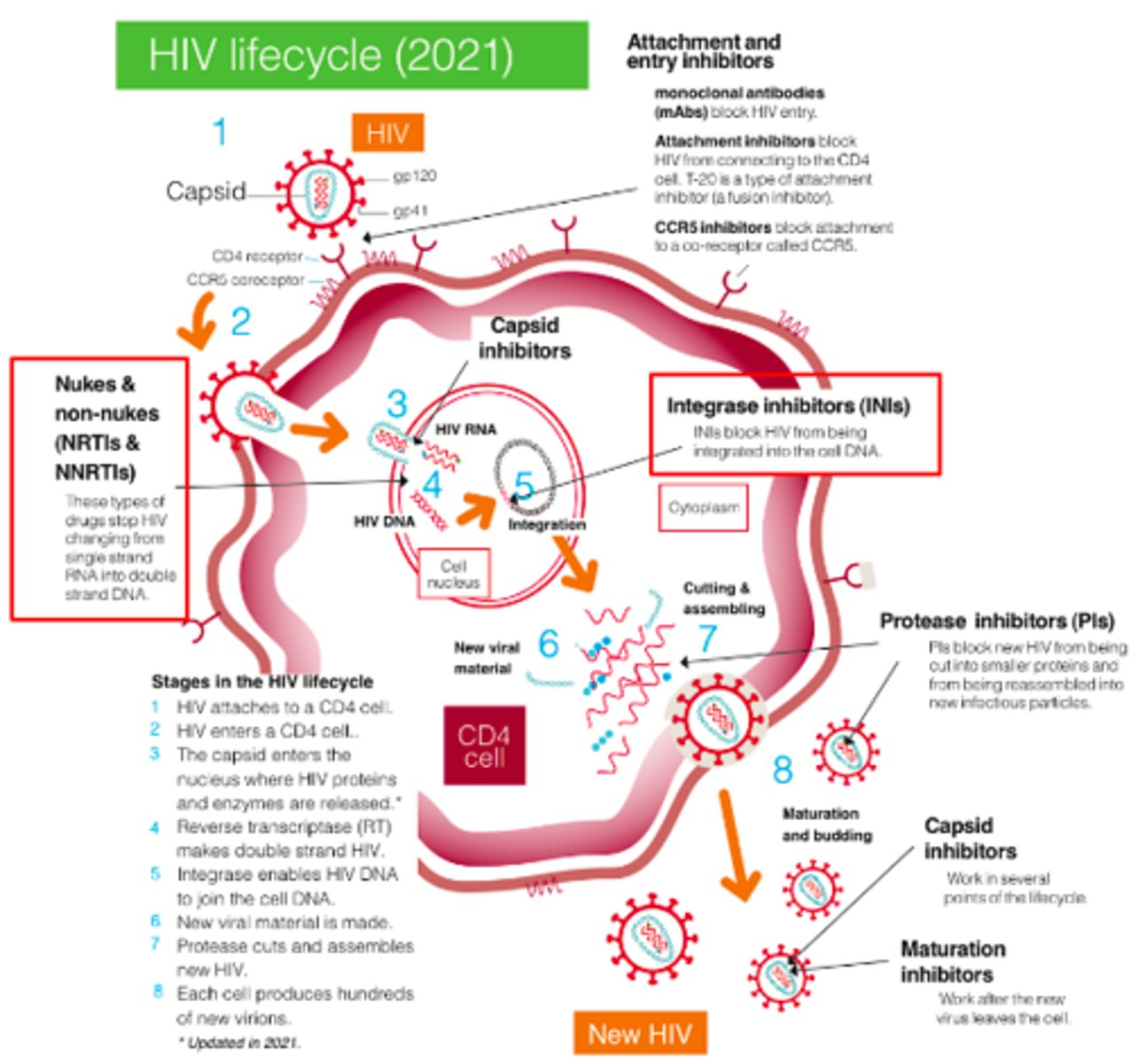
HIV Replication CYCLE
HIV = Retrovirus
•Cellular integration in CD4 cells
•Uses reverse transcriptase to transcribe viral RNA into dsDNA
Most antivirals aim to reduce/prevent replication
Pathophysiology: HIV Infection
Typical CD4 count vs AIDS
•Typical CD4 count: 500-1200 cells/mm3
•Acquired immunodeficiency syndrome (AIDS): CD4 <200 cells/mm3
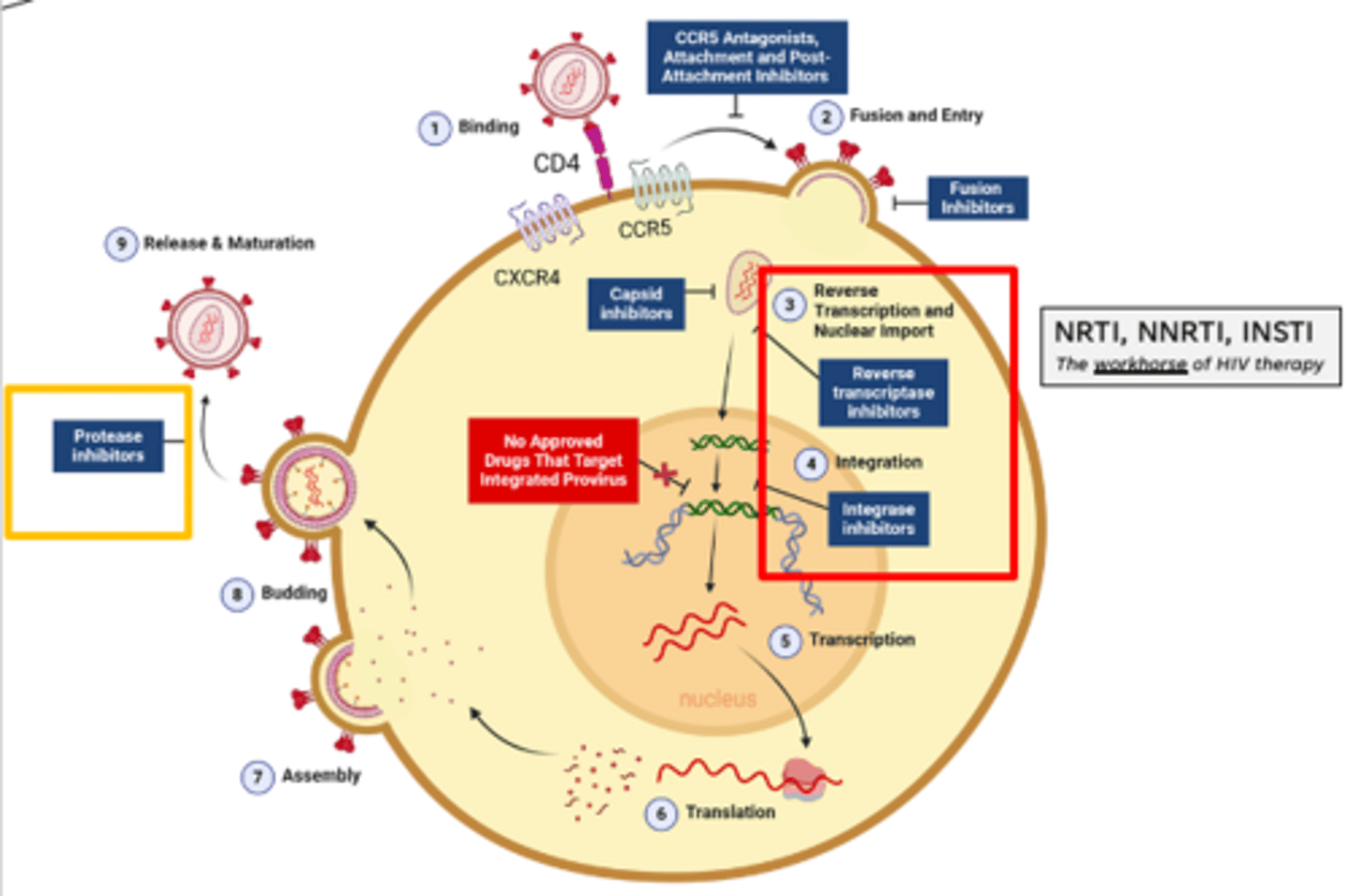
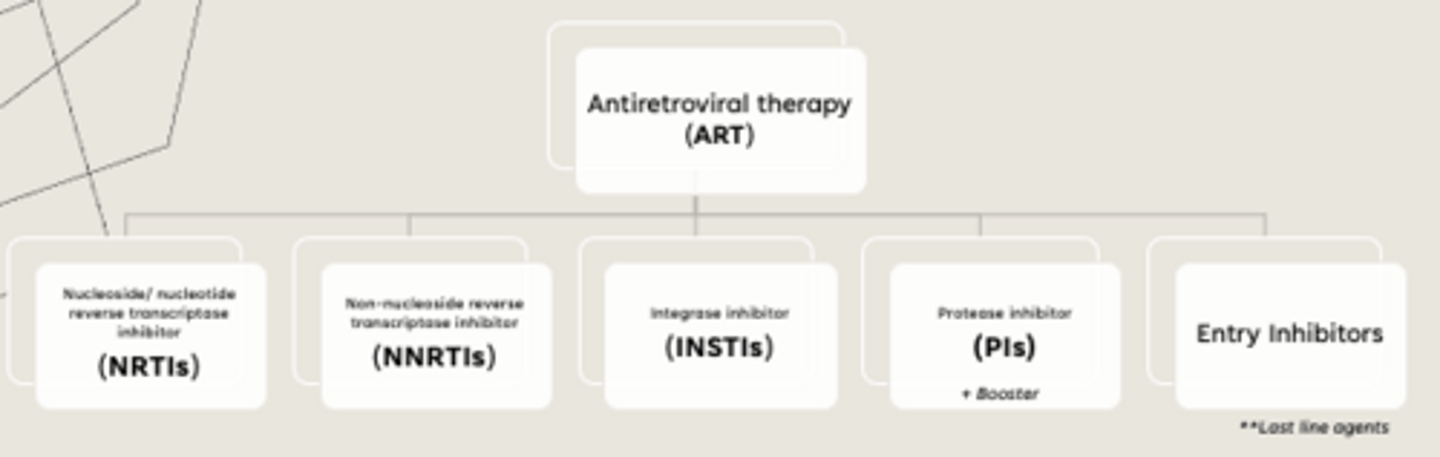
Antiretroviral therapy (ART) - drug classes
•Nucleoside/ nucleotide reverse transcriptase inhibitor (NRTIs)
•Non-nucleoside reverse transcriptase inhibitor (NNRTIs)
•Integrase inhibitor (INSTIs)
•Protease inhibitor (PIs)
•Entry Inhibitors
Treating HIV (Generally speaking)
know this very well
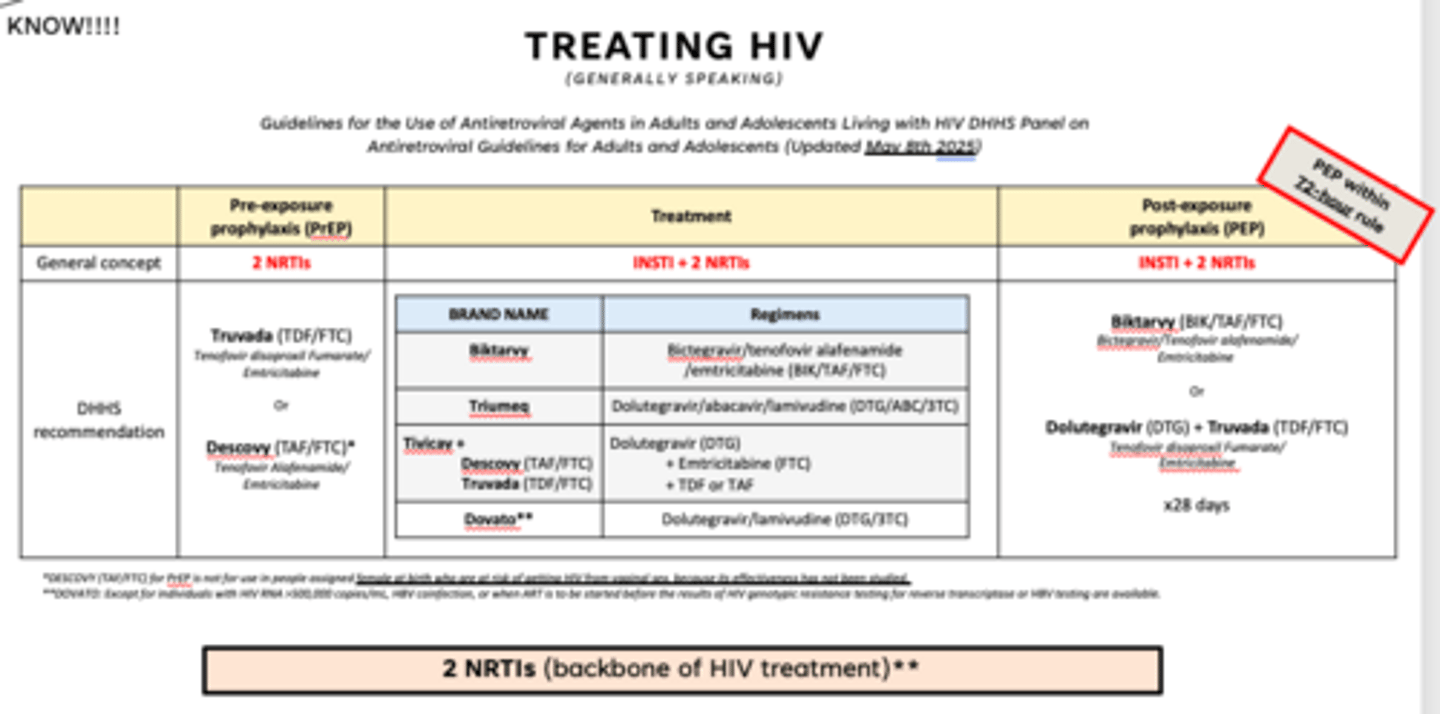
Treating HIV (Generally speaking)
Pre-exposure prophylaxis (PrEP)
2 NRTIs
Truvada (TDF/FTC)
Tenofovir disoproxil Fumarate/ Emtricitabine
Or
Descovy (TAF/FTC)**
Tenofovir Alafenamide/ Emtricitabine
Descovy (TAF/FTC)** Tenofovir Alafenamide/ Emtricitabine
NOT used in what pts??
**DESCOVY (TAF/FTC) for PrEP is not for use in people assigned female at birth who are at risk of getting HIV from vaginal sex, because its effectiveness has not been studied.
Treatment of HIV (know this well)
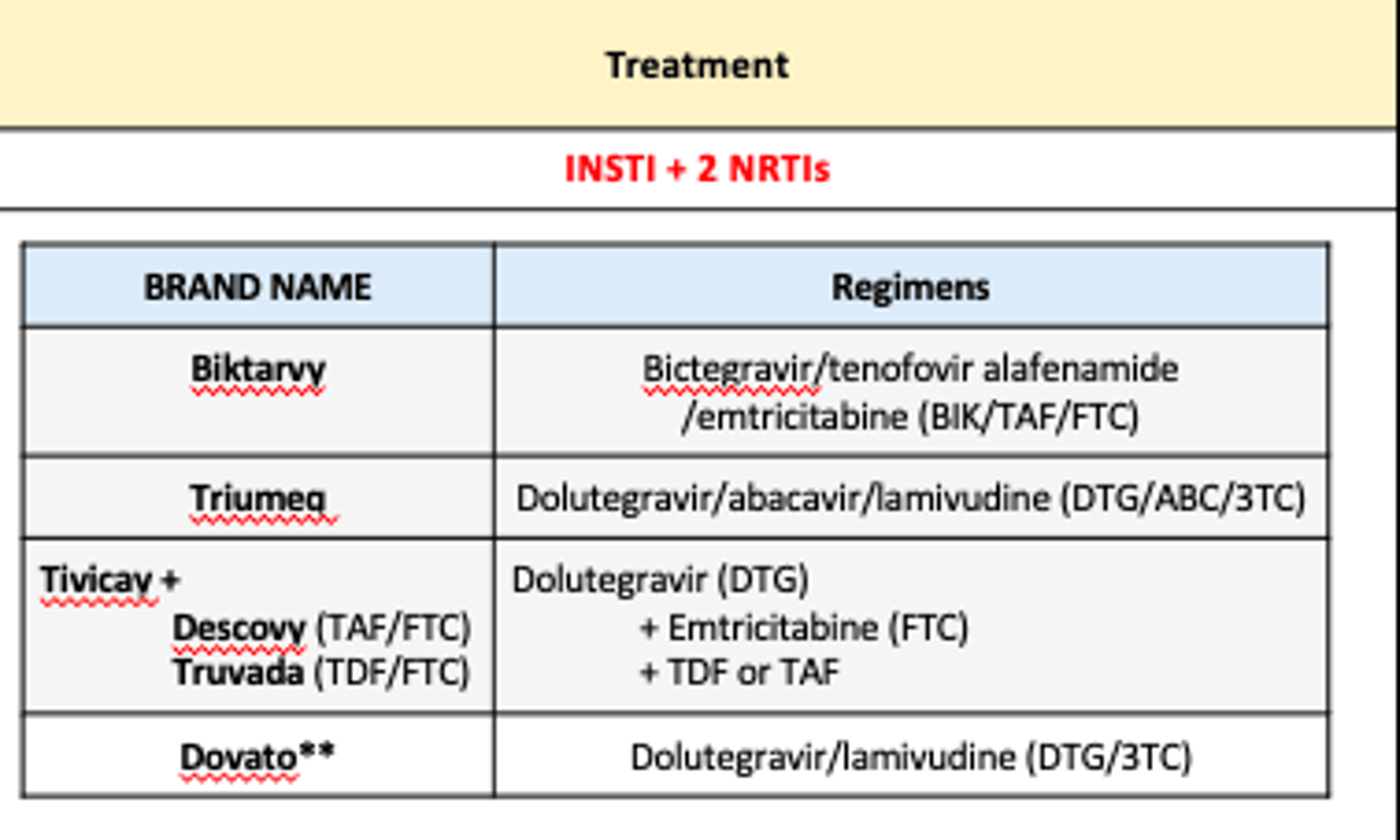
INSTI + 2 NRTIs (2 NRTIs is backbone of HIV treatment)
Biktarvy: Bictegravir INSTI + Tenofovir alafenamide (TAF) NRTI + Emtricitabine (FTC) NRTI
Triumeq: Dolutegravir (DTG) = INSTI, Abacavir (ABC) = NRTI, Lamivudine (3TC) = NRTI
**Before using abacavir test for HLA-B*5701
Tivicay + Descovy/Truvada
• Dolutegravir (DTG) = INSTI
• Emtricitabine (FTC) NRTI + TAF/TDF = 2 NRTIs
Dovato: Dolutegravir (DTG) = INSTI, Lamivudine (3TC) = NRTI. This one is weird bc its only 1 INSTI + 1 NRTI.
Post-exposure prophylaxis (PEP)
INSTI + 2 NRTIs PEP within 72-hour rule
Biktarvy (BIK/TAF/FTC)
Bictegravir/Tenofovir alafenamide/
Emtricitabine
Or
Dolutegravir (DTG) + Truvada (TDF/FTC)
Tenofovir disoproxil Fumarate/
Emtricitabine
length of post-exposure prophylaxis (PEP)
x28 days
Nucleoside/ nucleotide reverse transcriptase inhibitors (NRTIs)
drugs
•Tenofovir disoproxil fumarate/TDF (Viread)
•Tenofovir alafenamide/TAF (Vemlidy)
•Emtricitabine/FTC (Emtriva)
•Abacavir/ABC (Ziagen)
•Lamivudine/3TC (Epivir)
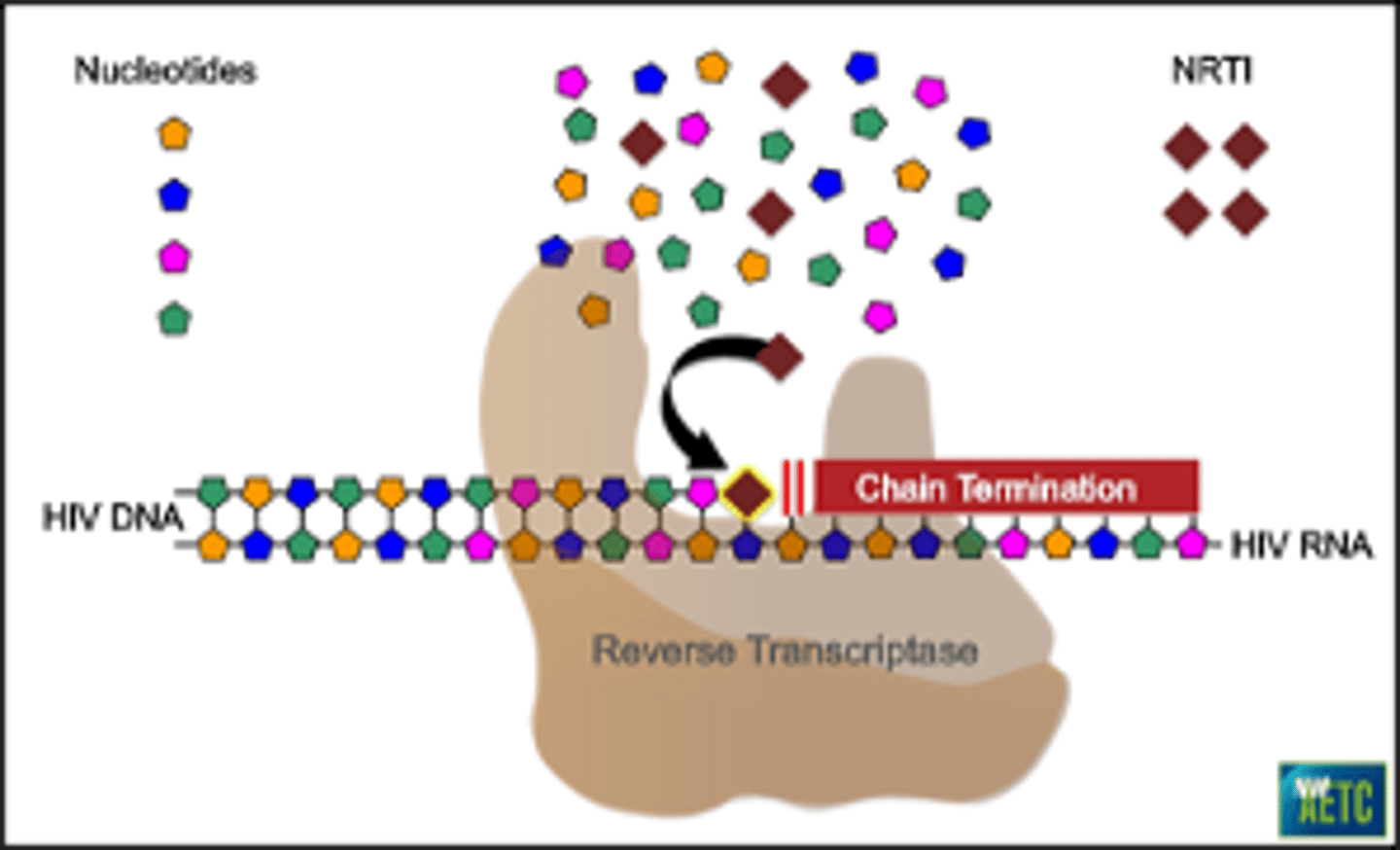
NRTIs MOA
MOA: Competes for binding to cause incorrect DNA strands = leading to termination
•Blocking reverse transcriptase (converts RNA --> DNA)
•NRTIs work by competing w/ natural nucleosides (dTTP, dCTP, dGTP, and dATP) and incorporate into viral DNA
•Causes chain termination --> prevents replication of virus.
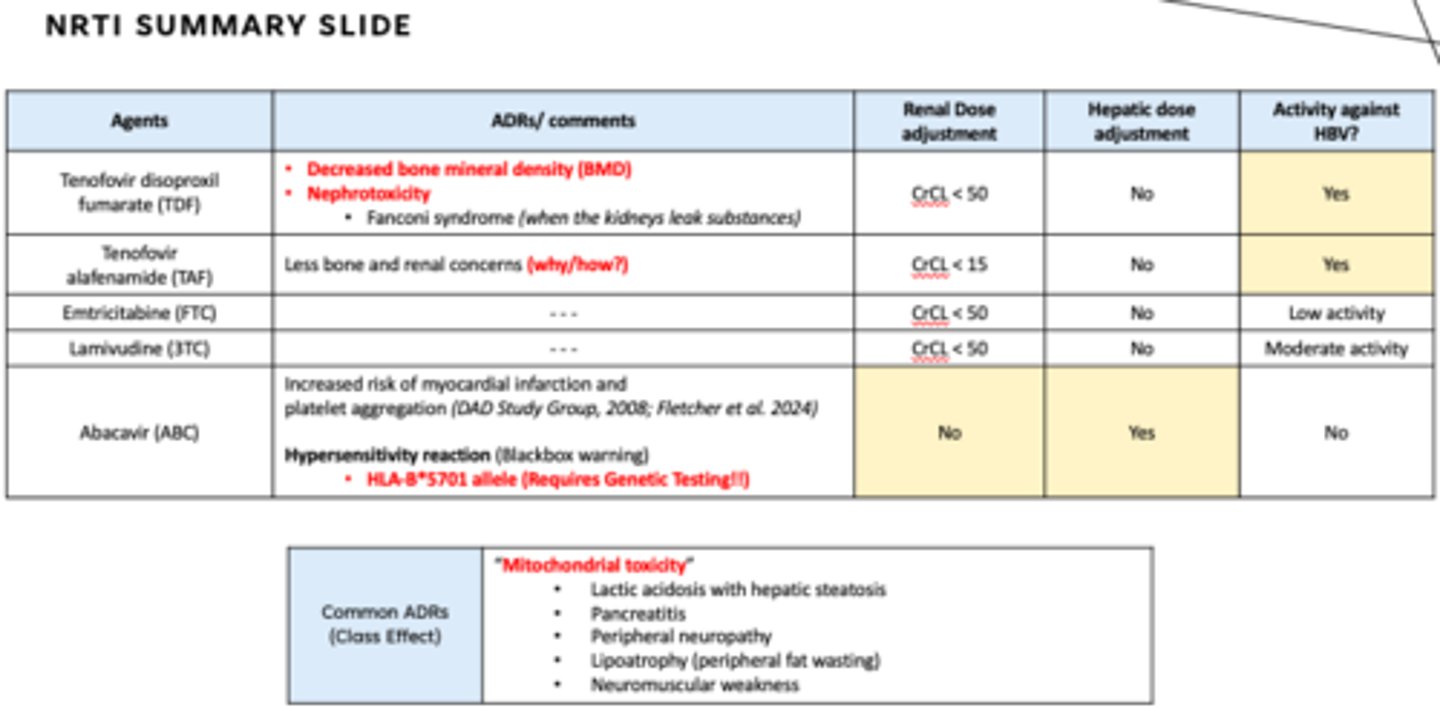
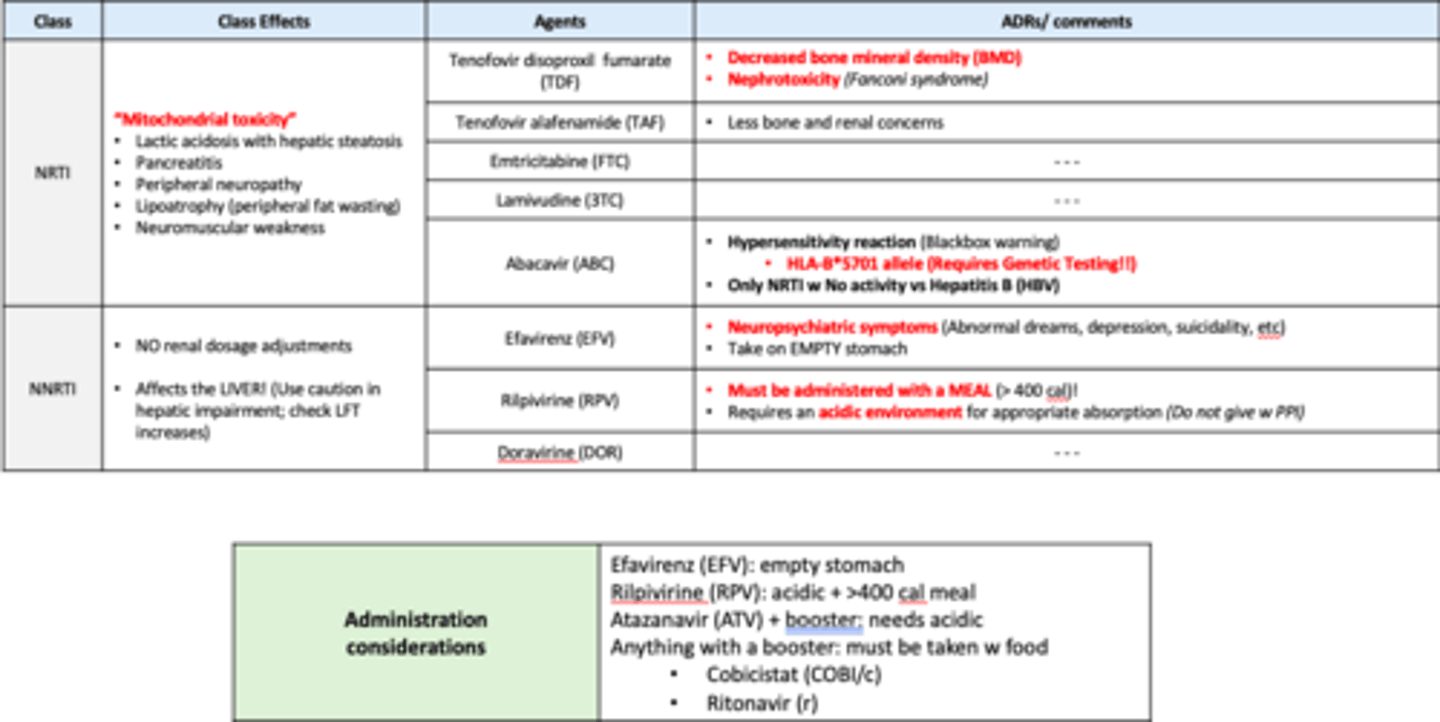
NRTIs ADRs (know all of these well)
Mitochondrial toxicity
•Lactic acidosis with hepatic steatosis
•Pancreatitis
•Peripheral neuropathy
•Lipoatrophy (peripheral fat wasting)
•Neuromuscular weakness
NRTIs: Tenofovir disoproxil fumarate (TDF)
ADRs
•Decreased bone mineral density (BMD)
•Nephrotoxicity
•Fanconi syndrome (when the kidneys leak substances)
•CrCL < 50
NRTIs: Tenofovir alafenamide (TAF)
ADRs
Less bone and renal concerns - why/how: bc a prodrug!
CrCL < 15
NRTIs: Emtricitabine (FTC)
ADRs
CrCL < 50
Tenofovir disoproxil fumarate (TDF), Tenofovir alafenamide (TAF), Emtricitabine (FTC)
Hepatic dose adjustment?
Activity against HBV?
Hepatic dose adjustment? NO
Activity against HBV? YES!!
Truvada and Descovy are commonly used in?
PrEP, PEP, and HVI treatment
NRTIs: Lamivudine (3TC) ADRs
CrCL < 50
Lamivudine (3TC) Hepatic dose adjustment? Activity against HBV?
Hepatic dose adjustment? NO
Activity against HBV? Moderate
Abacavir (ABC)
ADRs/comments
Increased risk of myocardial infarction and
platelet aggregation (DAD Study Group, 2008; Fletcher et al. 2024)
Hypersensitivity reaction (Blackbox warning)
•HLA-B*5701 allele (Requires Genetic Testing!!)
Abacavir (ABC)
Renal Dose adjustment?
Hepatic dose adjustment?
Activity against HBV?
Hepatic dose adjustment? YES
Activity against HBV? No
Need to test for _______ in patients starting Abacavir
HLA-B* 5701 allele
(requires genetic testing)
NRTI Summary SLIDE
Non-nucleoside reverse transcriptase inhibitor (NNRTIs)
agents
•Efavirenz/EFV (Sustiva)
•Rilpivirine/RPV (Edurant)
•Doravirine/DOR (Pifeltro)
•Etravirine/ETR (Intelence)
•Nevirapine/NVP (Viramune)
•Delavirdine/DLV (Rescriptor)
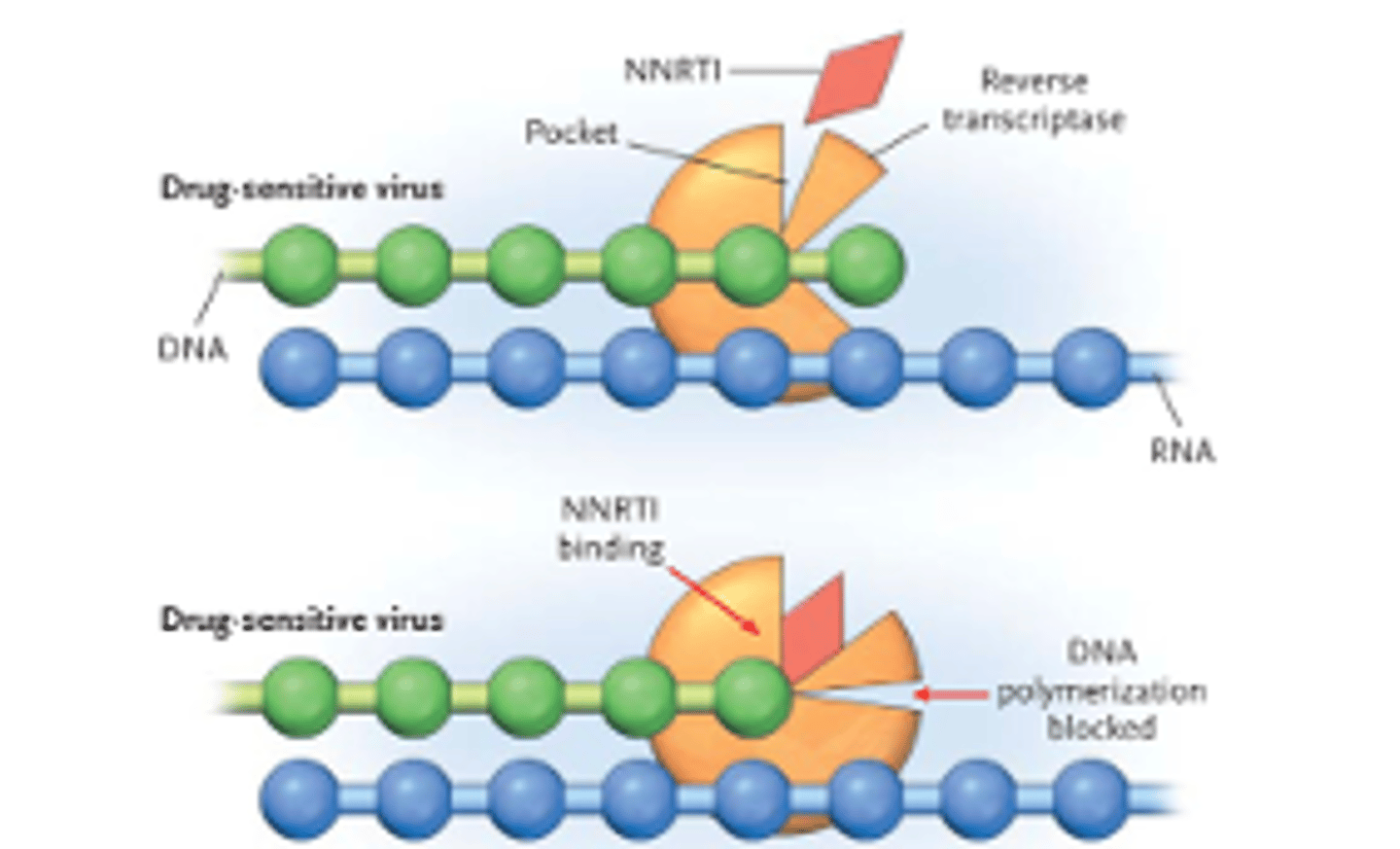
Non-nucleoside reverse transcriptase inhibitor (NNRTIs)
MOA
Allosterically blocking the reverse transcriptase, which converts RNA into DNA; causing termination
MOA: Allosteric inhibitor binds to an enzyme at a site other than the active site, causing change in the confirmation of the enzyme
Non-nucleoside reverse transcriptase inhibitor (NNRTIs)
Common ADRs
•Increased LFTs
•Rash (including Stevens-Johnson Syndrome)
•NO renal dosage adjustments
•Affects the LIVER! (Use caution in hepatic impairment)
Non-nucleoside reverse transcriptase inhibitor (NNRTIs)
CI
Severe hepatic dysfunction (Child-Pugh class B or C)
NNRTIs: Efavirenz (EFV)
ADRS
Neuropsychiatric symptoms (may resolve in 2-4 weeks)
•Abnormal dreams, dizziness, morning confusion, depression, suicidality
QTc prolongation
NNRTIs: Efavirenz (EFV) Administration
Take on empty stomach at bedtime to decrease CNS effects
Use with caution in the 1st trimester of pregnancy; birth defects seen in primate studies
NNRTIs: Rilpivirine (RPV) ADRs
Do not co-administer Rilpivirine w:
•Proton pump inhibitors
•Certain anticonvulsants
•Phenytoin, phenobarbital, oxcarbazepine
•Rifabutin, rifampin, rifapentine
•St. John’s Wort
Depression is observed in cases
NNRTIs: Rilpivirine (RPV) Administration
Must be administered with a MEAL (> 400 cal)!
Requires an acidic environment for appropriate absorption (Do not give w PPI)
CANNOT be started in patients with VL <100,000 copies/mL and CD4 >200 cells/mm3
NNRTIs: Doravirine (DOR) ADRs
Well tolerated
Treatment-emergent DOR resistance mutations may confer resistance to certain NNRTIs
NNRTIs: Efavirenz (EFV) tx study
•Acute psychosis as a side effect of efavirenz therapy (seen in > 40%)
•High-fat meals can increase lvl +60% concentrations
•Dizziness, abnormal dreams, headache, depression, suicidality, insomnia, somnolence
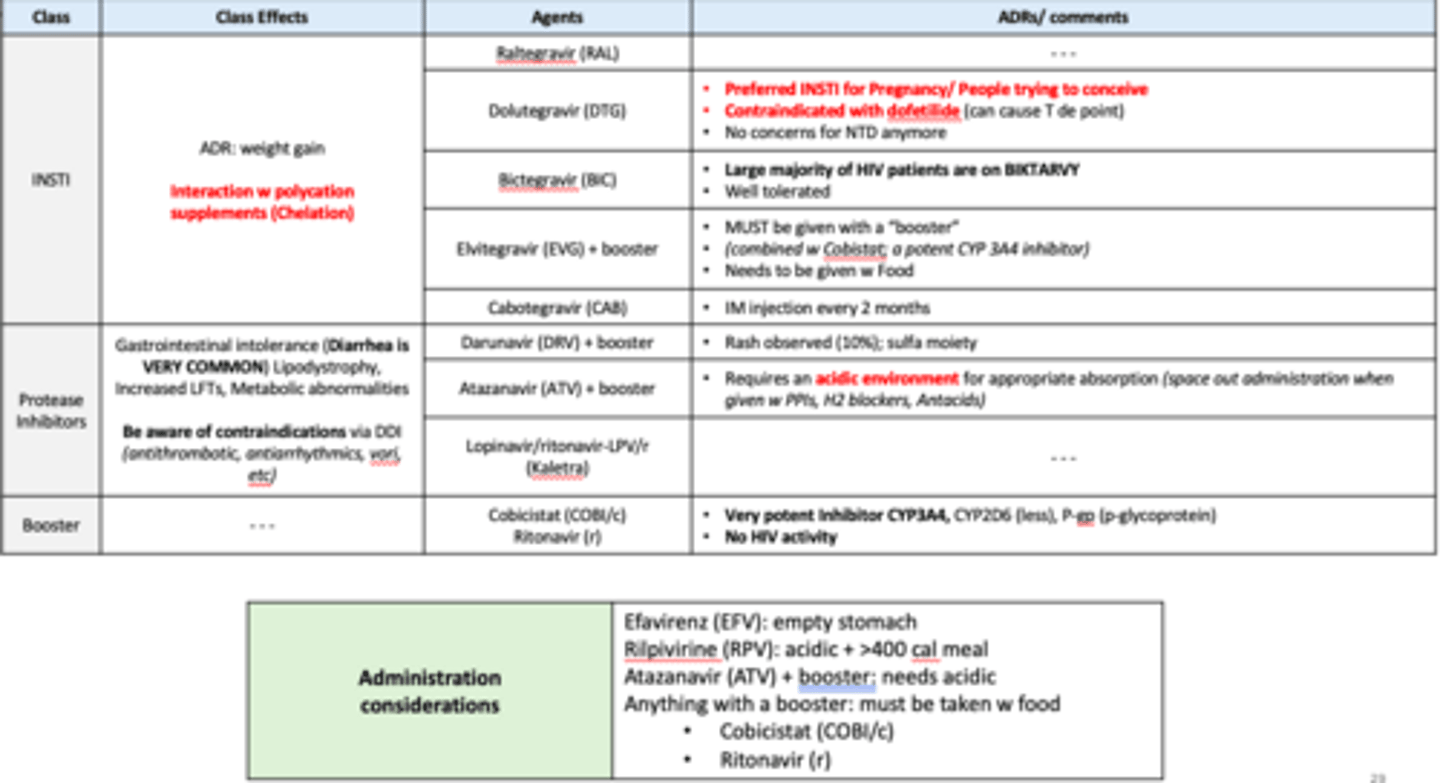
Integrase strand transfer inhibitors (INSTis)
agents
•Dolutegravir/DTG (Tivicay)
•Raltegravir/RAL (Isentress)
•Elvitegravir/EVG (coformulated as Genvoya/Stribild)
•Bictegravir/BIC (coformulated as Biktarvy)
Cabotegravir/ CAB (coformulated as Cabenuva)
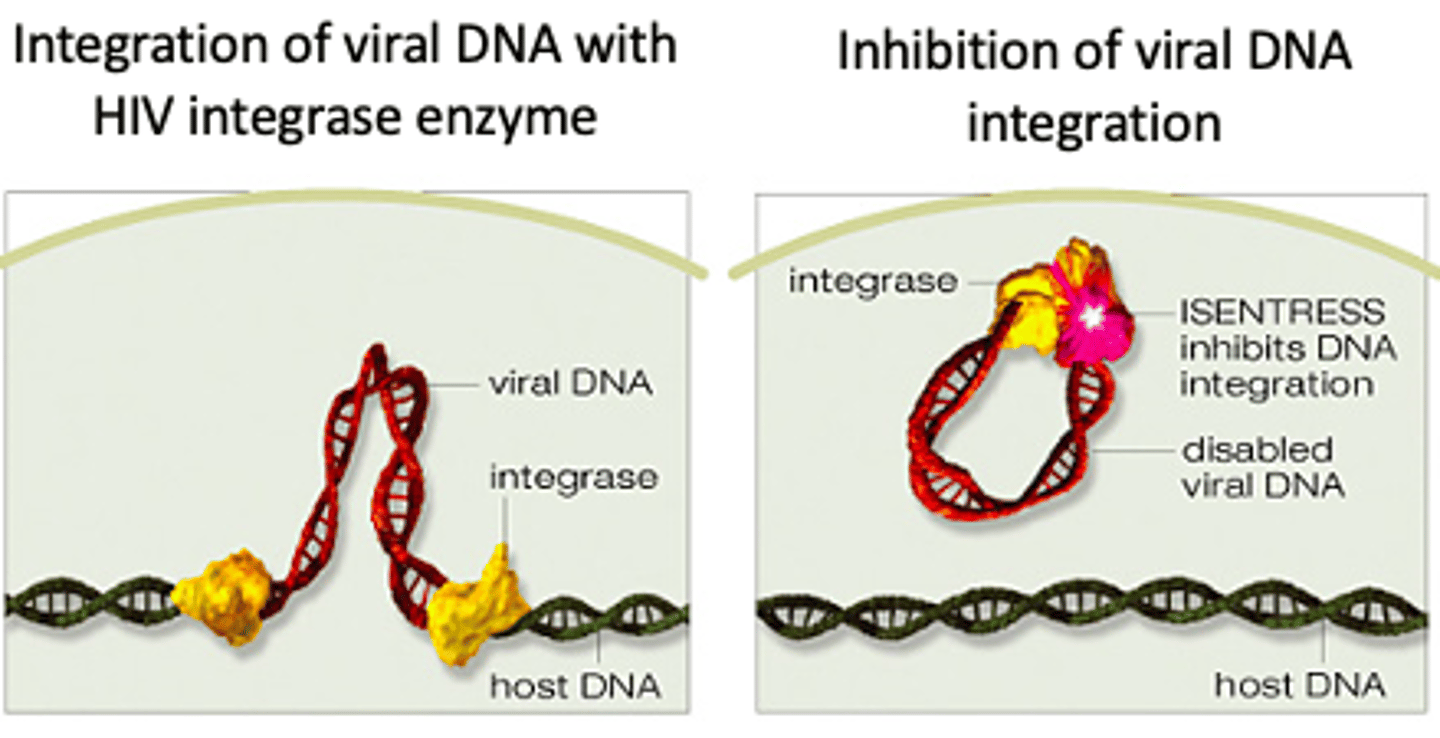
Integrase strand transfer inhibitors (INSTis) MOA
Prevent HIV integrase from incorporating proviral DNA into human host cells, which inhibits the HIV-catalyzed strand transfer step. This step is essential in the viral lifecycle and has no human homolog, making it a specific and effective HIV drug target
Integrase strand transfer inhibitors (INSTis)
ADRs
•Well tolerated (N/V/D)
•Weight gain
Weight gain-related issues w/ INSTI: all showing some metric of increased weight gain/ BMI in pts taking INSTI
Biggest issue w INSTIs??
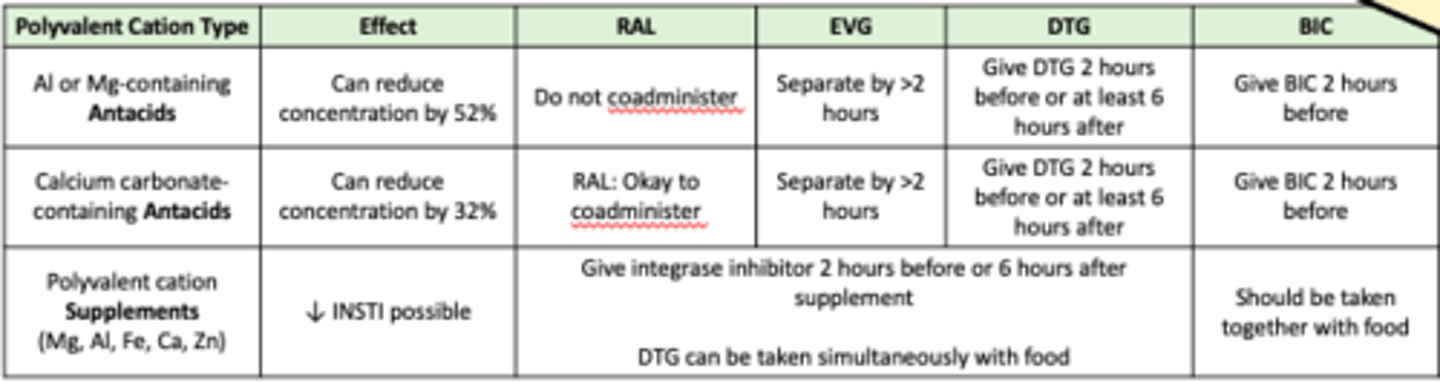
Class drug interaction with polycation supplements (Chelation) + Weight Gain
Integrase Inhibitors: Class Drug Interaction (FYI SLIDE)
Chelation concerns!! INSTIs have 2 binding sites for metals that can be chelated by polycation
INSTis: Raltegravir (RAL) ADRs
Increases in creatine kinase, myopathy, and rhabdomyolysis have been reported
INSTis: Dolutegravir (DTG) ADRs
Preferred INSTI for Pregnancy/ People trying to conceive
Contraindicated with dofetilide (can cause T de point)
Neural Tube Defect (NTD) considerations... study results DO NOT show an increased risk of NTDs in exposed infants
INSTis: Bictegravir (BIC) ADRs
Large majority of HIV patients are on BIKTARVY
Well tolerated
Recently approved for use in pregnancy!
INSTis: Elvitegravir (EVG) + Cobicistat
ADRs
MUST be given with a “booster”
(combined w Cobicistat; a potent CYP 3A4 inhibitor)
Needs to be given w Food
INSTis: Cabotegravir (CAB) vs CAB/RPV
"Future of HIV"
CAB Singular component - PrEP
CAB/RPV = HIV treatment

Cabotegravir (CAB) and Cabotegravir/ Rilpivirine (CAB/RPV)
ADRs
IM infection is given every 2 months
Used in patients w controlled HIV
ADR: painful IM injection
General questions during eligibility check for CAB and CAB/RPV
•Hep B history
•Pregnancy/ trying to conceive?
•History of depression? May incr
•HIV resistance history? Get injection regularly
•Travel plans - will have to switch agents
•Appointment adherence
HIV and missing a dose
Missing HIV medication doses can cause drug levels to fall too low --> allows virus to replicate & develop resistance
Once resistance develops to one med, HIV can become resistant to other drugs in the same class, limiting future tx options and forcing patients to use alternative or later-line regimens.
List of Protease inhibitors (PIs)
•Darunavir/DRV (Prezista)
•Atazanavir/ATV (Reyataz)
•Lopinavir/ritonavir-LPV/r (Kaletra)
•Tipranavir/TPV (Aptivus)
•Indinavir/IDV (Crixivan)
•Saquinavir/SQV (Invirase)
•Fosamprenavir/FPV (Lexiva)
•Nelfinavir/NFV (Viracept)
List of “Boosters” (Pharmacokinetic Enhancers)
•Cobicistat (Tybost)
•Ritonavir (Norvir)
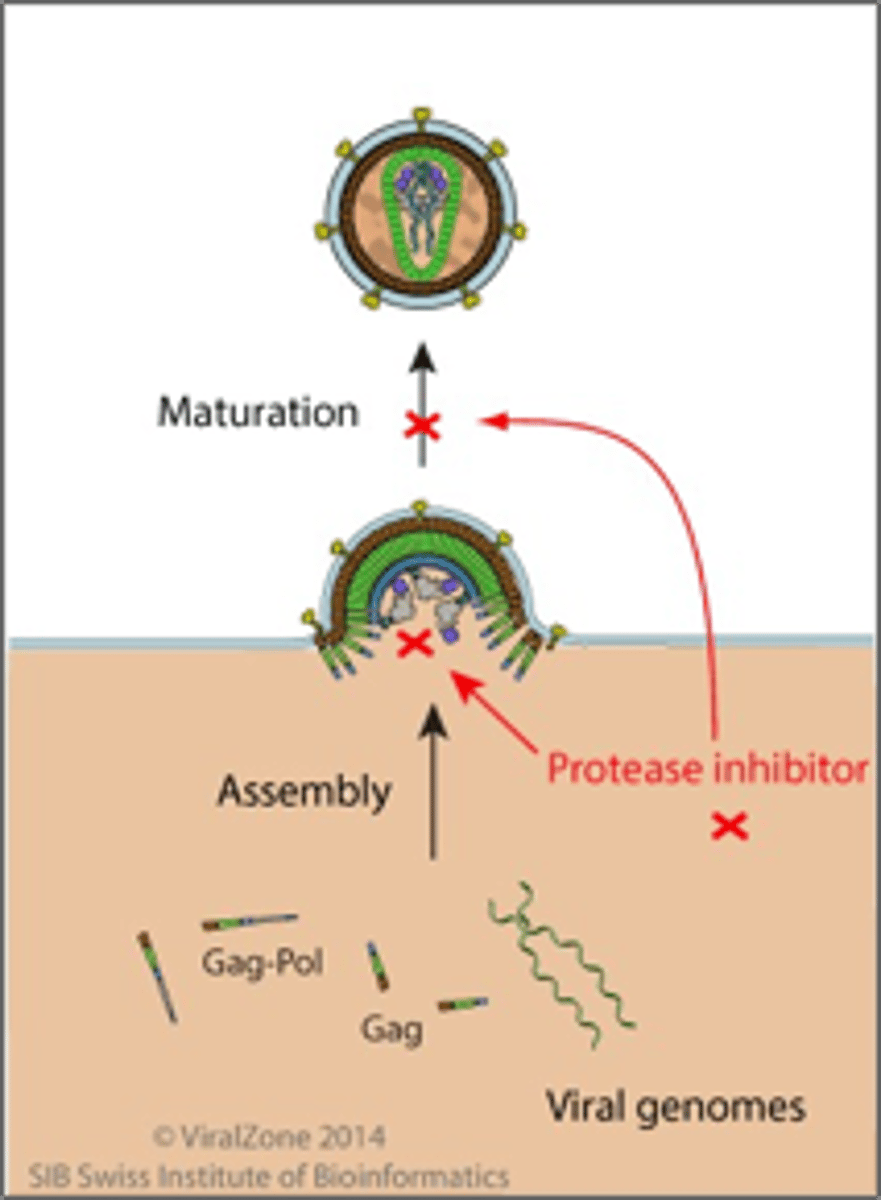
PROTEASE INHIBITORS (Pis) + BOOSTER
MOA
•Prevent viral replication by selectively binding to viral proteases (e.g. HIV-1 protease) and blocking proteolytic cleavage of protein precursors that are necessary for the production
PROTEASE INHIBITORS (Pis) + BOOSTER
Common ADRs
•Lipodystrophy (via buffalo hump)
•Increased transaminases (affect LFTs)
•Gastrointestinal intolerance (Diarrhea is VERY COMMON)
Metabolic abnormalities
•Hyperlipidemia
•Insulin resistance
PROTEASE INHIBITORS (Pis) + BOOSTER
Contraindications
Severe hepatic dysfunction (Child-Pugh class C)
See list in later slides (DDI)
General comments - PROTEASE INHIBITORS (Pis)
•Protease Inhibitor and Boosters – STRONG 3A4 Inhibitor
•High genetic barrier to resistance
•Use with caution in hepatic impairment
•Must take w food
Pis: Darunavir (DRV)
ADRs
Rash observed (10%); sulfa moiety
Pis: Atazanavir (ATV)
ADRs/comments
•Reversible indirect hyperbilirubinemia (35-47% patients)
•Requires an acidic environment for appropriate absorption (space out administration when given w PPIs, H2 blockers, Antacids)
Pis: Lopinavir (LPV)
comments
Always taken w Ritonavir
PROTEASE INHIBITORS (Pis) + BOOSTER
what are the boosters
Cobicistat (COBI/c)
Ritonavir (r)
Cobicistat (COBI/c) and Ritonavir (r) are both? (think DDI)
Extremely strong CYP 450 inhibitors!
Cobicistat (COBI/c) - ADRs/Comments
•No HIV activity
•Not recommended when CrCL < 70 mL/min
•Approved for use only with darunavir and atazanavir
Ritonavir (r) - ADRs/Comments
•Minimal HIV activity
Summary Slide 1
Summary Slide 2
Which HIV ARV also has anti-hepatitis B activity?
A.Abacavir
B.Tenofovir alafenamide
C.Efavirenz
D.Rilpivirine
B. Tenofovir alafenamide
Which of the following NRTIs requires dose adjustments in patients with hepatic impairment?
A.Tenofovir alafenamide
B.Lamivudine
C.Abacavir
D.Emtricitabine
C. Abacavir
Which of the following NNRTIs must be taken on an empty stomach?
A.Efavirenz
B.Rilpivirine
C.Doravirine
A. Efavirenz
Which of the following NNRTIs is contraindicated with omeprazole?
A.Efavirenz
B.Rilpivirine
C.Doravirine
B. Rilpivirine
Opportunistic Infections in HIV(in 1 slide)
If CD4 is >200, usually don’t treat!!!
<200 always use bactrim
<50 = use bactrim AND azithromycin
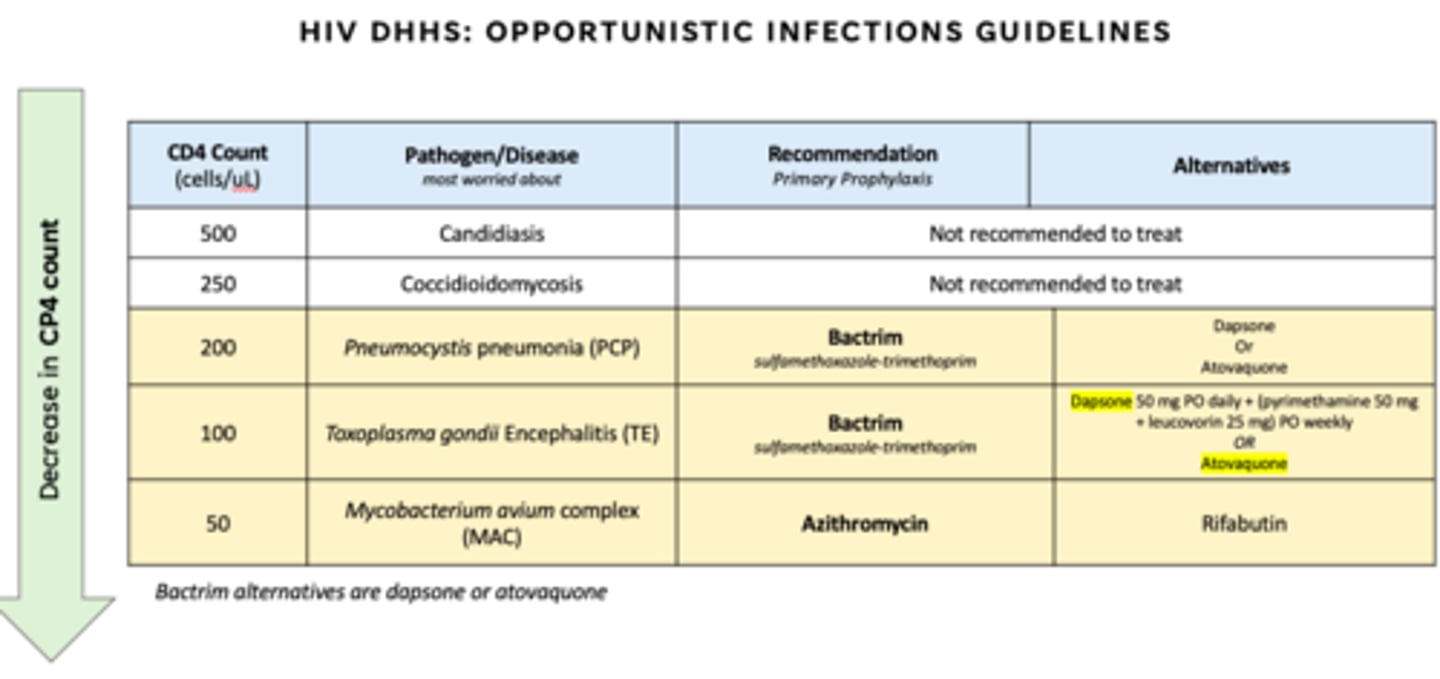
what pathogens for:
CD4 < 200
CD4 < 100
CD4 < 50
200 - Pneumocystis pneumonia (PCP)
100 - Toxoplasma gondii Encephalitis (TE)
50 - Mycobacterium avium complex (MAC)
Bactrim alternatives are?
Azithromycin alternative?
Bactrim alternatives = dapsone or atovaquone
Azithromycin alternative = Rifabutin
bactrim and azithro adrs
Bactrim:
- SJS
- Rash
- Sulfa allergy/hypersensitivity
- Hyperkalemia
Azithromycin:
- Allergy/rash
- QTc prolongation → risk of arrhythmias
Dapsone requires
G6PD testing
If they have it = increased risk hemolytic anemia.