Unit 3: Implications in the Real World - Schizophrenia
1/81
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
82 Terms
What is Schizophrenia? AO1
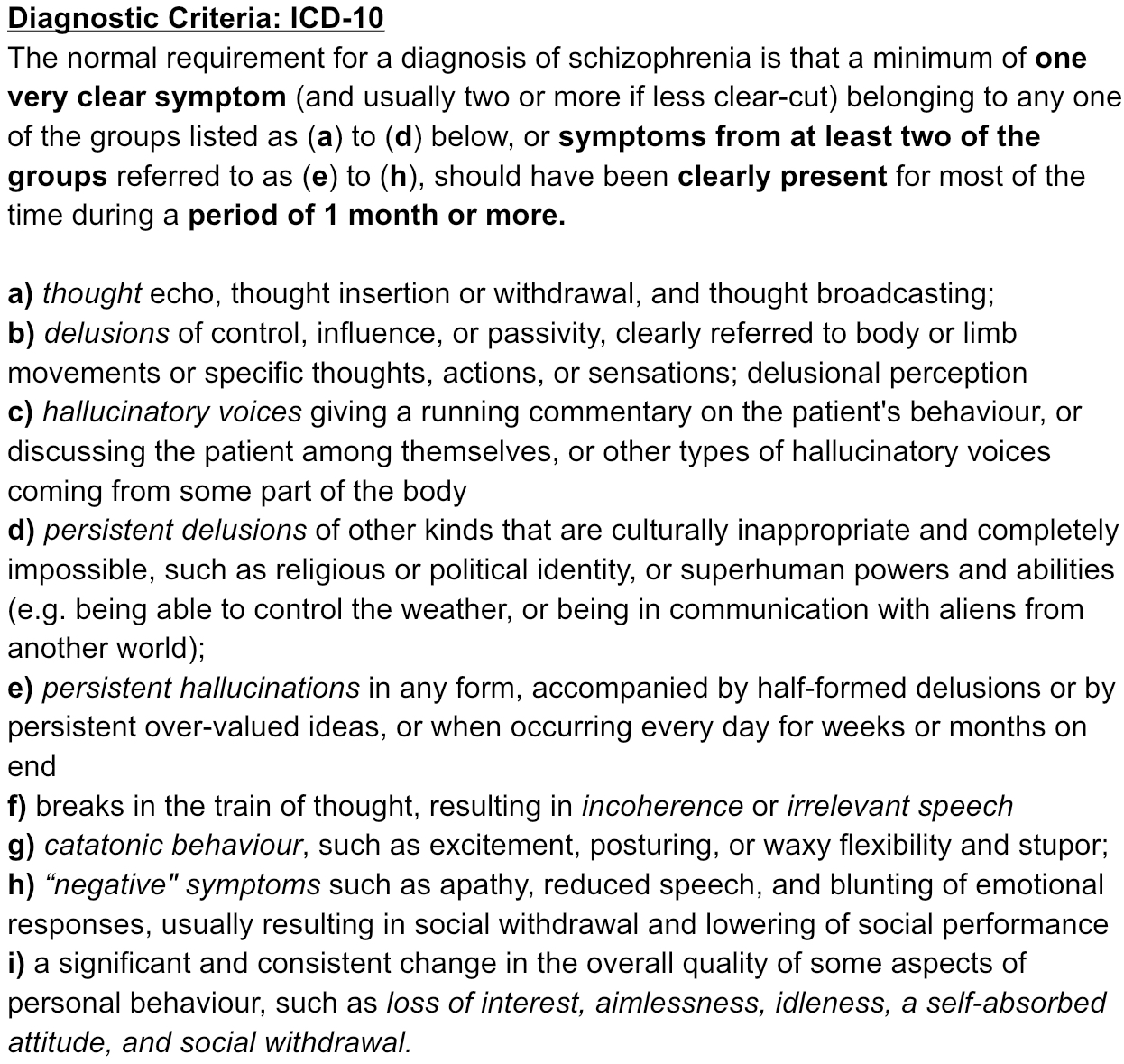
Schizophrenia (Scz.) is a lifelong illness that affects about 1% of the population. Schizophrenia is characterised by symptoms that cause a person to break contact with reality.
Common symptoms include delusions, hallucinations, problems with speech and behaviour, and often social and occupational dysfunction.
A person with schizophrenia will typically suffer “episodes” of the illness, where their symptoms become much more acute (severe) but also many periods of time that are symptom free.
Currently, there is no known single cause of schizophrenia, but there are many theories. Schizophrenia is a complicated disorder that presents in different ways in different people, and so is likely to be caused by a number of interacting factors.
Positive Symptoms of Schizophrenia - Hallucinations
Positive symptoms – behaviours and thoughts that the person with schizophrenia did not have before they became ill.
Hallucinations - perceptions which aren’t real; can be auditory, tactile or visual.
Positive Symptoms of Schizophrenia
Delusions - beliefs that aren’t real; persecution, grandiosity or reference.
Disorganised Thinking/ Speech - The sentences of someone suffering with schizophrenia may become mixed up and difficult to understand, referred to as a ‘word salad’.
Insertion - Someone suffering with schizophrenia may report having thoughts in their head which are not their own.
Disorganised Behaviour - Unpredictable behaviour, for example, they may behave inappropriately or shout/ swear for no reason.
Catatonic Behaviour - A person suffering with schizophrenia may display varied body movement. This could range from a stupor, to fast repetitive movement, to the mimicking of other behaviour around them (echopraxia).
Negative Symptoms of Schizophrenia
Negative symptoms – behaviours and thoughts that the person with schizophrenia used to have but have now lost or reduced due to the illness.
Avolition - A person suffering with schizophrenia may lose interest and motivation in life and activities e.g work, relationships and sex.
Anhedonia - A person suffering with schizophrenia may lose the ability to feel pleasure. This may result in the person not reacting appropriately to pleasurable experiences.
Alogia - A reduction in the amount of speech produced by someone suffering with schizophrenia, resulting from impairment in thinking that affects language abilities.
Flat affect - A person suffering with schizophrenia may appear to have diminished emotional expression. They may hold conversations without any indication of emotional tone and show little of no facial expressions.
Prodromal Symptoms
A prodrome is an early symptom indicating the onset of a disease or illness. For people who are about to experience their first episode of schizophrenia, they may show certain prodromal symptoms such in the weeks and months before showing full schizophrenic symptoms. Common prodromal symptoms may be:
a loss of interest in usual activities
avoiding the company of others
staying away from work or school
being irritable and oversensitive
lack of interest in personal appearance and hygiene
generalised anxiety
mild degrees of depression
These symptoms are not enough to diagnose schizophrenia, as they also occur in other illnesses.
Stages of Schizophrenia
Diagnosis of Schizophrenia
Patients are diagnosed against set criteria. Both systems clarify symptoms and allow diagnosis.
▶ Lots of overlap between the two systems - generally high level of agreement when it comes to diagnosis.
▶ However, there are some differences, meaning that someone may receive a diagnosis for schizophrenia with one criteria but not the other.
▶ DSM focuses exclusively on mental illness, while ICD also includes physical illnesses.
▶ Both based on most up to date research in psychology and are periodically revised and updated
Diagnostic Criteria: ICD-10/11
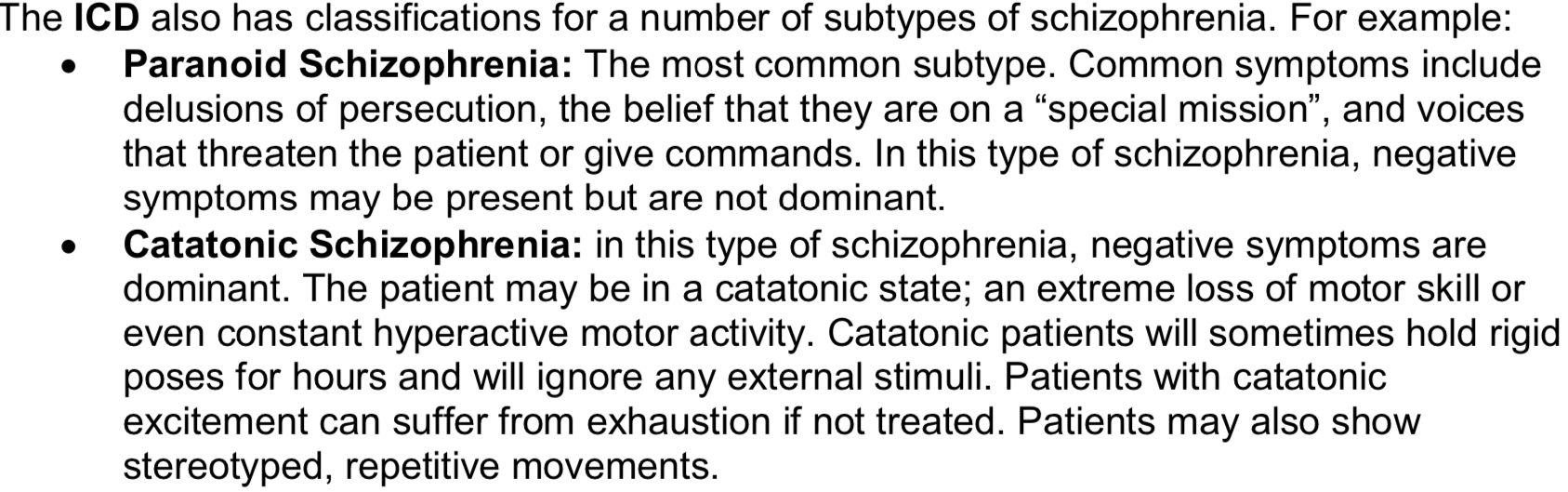
Subtypes of Schizophrenia - ICD
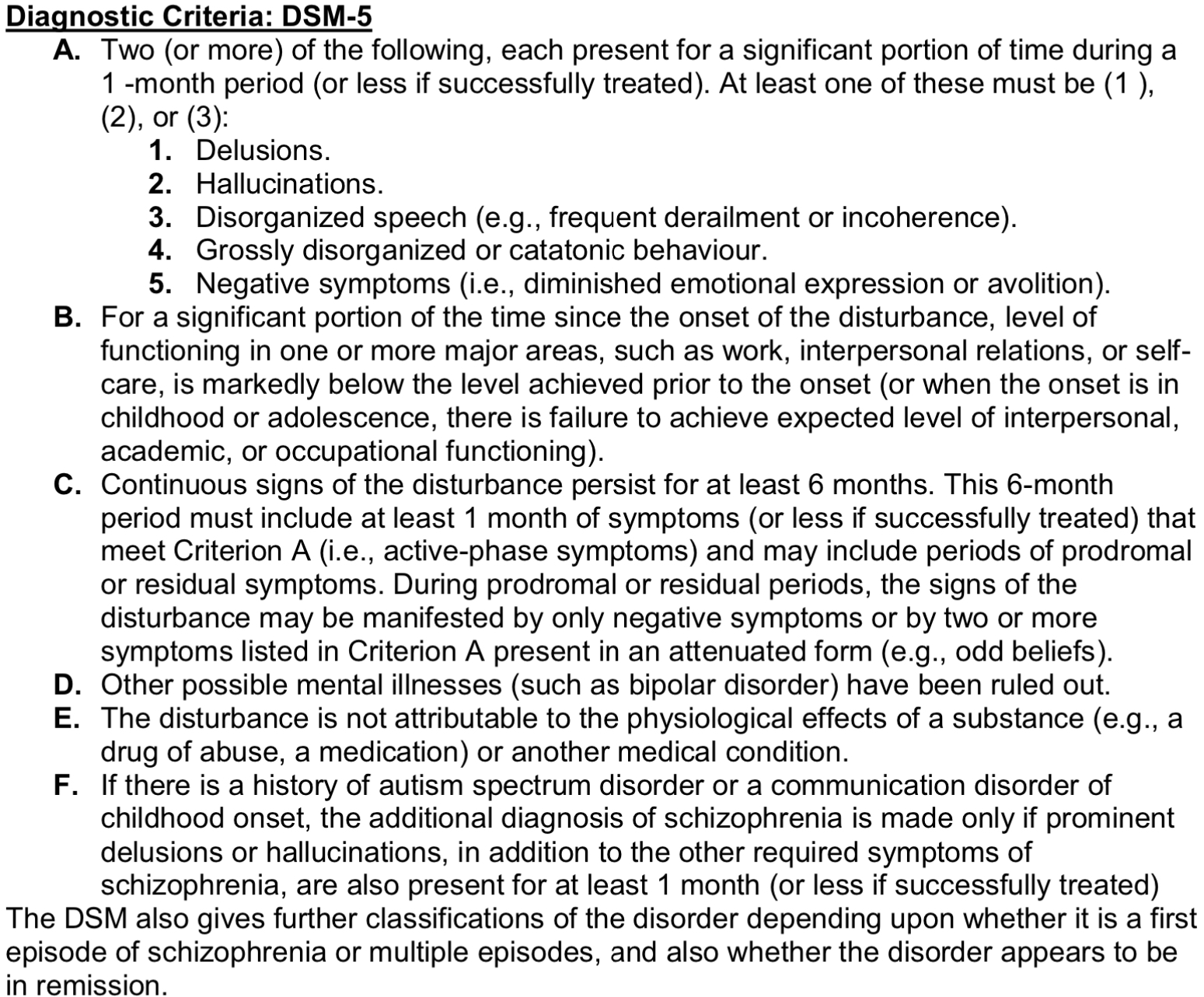
Diagnostic Criteria: DSM-5
Biological Explanations of Schizophrenia: Dopamine Hypothesis Version 1 (Superhero)
The original dopamine hypothesis (version I) claims that an excess of the neurotransmitter dopamine in certain regions of the brain is associated with the positive symptoms of schizophrenia.
Originally the dopamine receptor hypothesis (version I) emerged from the discovery of antipsychotic drugs and the work of Carlsson and Lindqvist (1957) who identified that these drugs reduced levels of dopamine uptake when administered to animals.
Further research has suggested that individuals with schizophrenia have abnormally high numbers of D2 receptors on receiving neurons, meaning that when dopamine is release into the synapse, it results in more dopamine binding to post synaptic receptor sites and therefore more neurons firing.
e.g. if there is an increase of activity in an area linked to your auditory cortex, it would result in too many neurons firing in that area of the brain which could then lead to the experience of auditory hallucinations (positive symptom of scz).
Biological Explanations of Schizophrenia: Dopamine Hypothesis Version 2
The original dopamine hypothesis was updated by Davis 1991 in the light of research incompatible with version I (e.g. clozapine proved effective in patients unresponsive to other antipsychotic drugs despite its low impact on D2 receptor activity) and evidence that dopamine receptors show different brain distribution.
Davis (1991) suggested that it is not just the excess levels of dopaminergic activity, rather it is an abnormal level of dopaminergic activity, whether that be too high OR too low. For example, too much dopamine in the mesolimbic pathway (reward pathway in the brain) can lead to positive symptoms.
However, a deficit of dopaminergic activity in the prefrontal cortex linked to thinking and decision making can lead to negative symptoms such as cognitive impairment or avolition.
Davis argued that the positive symptoms (hallucinations, delusions) are due to striatal hyperdopaminergia while negative symptoms of schizophrenia (e.g. withdrawal, cognitive effects) result from prefrontal hypodopaminergia.
Biological Explanations of Schizophrenia: Dopamine Hypothesis Version 3
Research has been used by Howes and Kapur 2009 to propose a version III which aims to provide a framework that links risk factors (including pregnancy and obstetric complications, stress trauma, drug use and genes) to increased presynaptic striatal dopaminergic function rather than D2 receptor activity.
They hypothesise that ‘multiple hits’ interact to result in dopamine dysregulation linked to psychosis rather than schizophrenia. This dopamine dysregulation is argued to alter the appraisal of stimuli.
Evaluation of The Dopamine Hypothesis - Determinist (Strength)
Schizophrenia can be explained by a number of biological explanations, for example, the dopamine hypothesis states that the brain of schizophrenic patients produces more dopamine than normal brains.
The biological explanation of schizophrenia is often supported because of its deterministic nature.
A strength of this explanation is that it provides a clear, scientific account of schizophrenia by linking the disorder to neurochemical imbalances rather than personal choice.
The dopamine hypothesis supports this view, suggesting that schizophrenia is caused by excessive dopamine activity in certain brain pathways, particularly the mesolimbic system, which is associated with hallucinations and delusions. For instance, research has shown that antipsychotic drugs, which block dopamine receptors, significantly reduce positive symptoms of Schizophrenia Carlsson and Lindqvist (1957).
This deterministic approach is beneficial as it frames schizophrenia as the result of uncontrollable biological processes, removing blame from individuals and allowing treatments to directly target the underlying cause.
Therefore, the deterministic nature of the biological explanation, supported by the dopamine hypothesis, strengthens its credibility while also reducing stigma by presenting schizophrenia as a medical condition rather than a personal weakness.
Evaluation
The Dopamine Hypothesis:
Deterministic - Carlsson and Lindqvist (1957) - antipsychotic drugs block dopamine - reduce positive symptoms
Reductionist - (Howes and Kapur 2009) - stress, trauma & cognitive processes
Scientific - Davis (1991) too much dopamine/ to little - led to treatment (atypical antipsychotics)
Cause & Effect - correlational - limits explanatory power
Evaluation of The Dopamine Hypothesis - Reductionist (Weakness)
The biological explanation of schizophrenia can be criticised for being reductionist.
A weakness is that it reduces a highly complex behaviours such as schizophrenia down to simple biological factors such as dopamine levels, ignoring the wider psychological and social influences.
For example, while the dopamine hypothesis has strong support, many patients do not respond to dopamine-blocking drugs, suggesting that other factors such as stress, trauma, or cognitive processes also play a role in the development of schizophrenia (Howes and Kapur 2009)
This reductionist approach may limit our understanding, as it oversimplifies the condition and risks neglecting other important factors such as family environment and social interaction.
Therefore, although the biological explanation provides valuable scientific insights, its reductionist nature weakens it as it fails to capture the full complexity of schizophrenia.
Evaluation of The Dopamine Hypothesis - Scientific (Strength & Weakness)
The dopamine hypothesis of schizophrenia can be evaluated as both a strength and a weakness due to its scientific basis.
On one hand, a strength is that it is grounded in empirical research, making it a credible and testable explanation of schizophrenia.
For example, studies have shown that drugs which block dopamine receptors, such as antipsychotics, often reduce positive symptoms like hallucinations and delusions, providing clear biological support for the role of dopamine.
This scientific approach increases the validity of the explanation and has led to practical applications in treatment, improving patients’ quality of life.
However, the same scientific focus can also be seen as a weakness of the dopamine hypothesis as most supporting evidence is correlational. This means we cannot establish cause and effect — it is unclear whether high dopamine activity causes schizophrenia, or whether the disorder itself leads to dopamine imbalances. Therefore, the hypothesis may not accurately explain the origins of schizophrenia.
Therefore, while the dopamine hypothesis is valuable for its scientific credibility and practical applications, its narrow biological focus limits its explanatory power.
PET Scans (Patel 2010) - Weakness
Evidence to support version III relies heavily on PET scan data to provide estimates of synaptic dopamine levels; the results are based on modelling rather than direct measurement and therefore subject to errors which may yet be identified; this would undermine version III
Research using PET scans hasn’t yet been able to detect differences in dopamine activity in the brain of individuals with schizophrenia and those without.
This suggests that it may be some time before we know for certain if dopamine imbalances cause schizophrenia, or the other way round.
Therefore, the dopamine hypothesis’ reliance on PET scan data would be seen as a weakness, due to errors and issues of causation.
(Conclusion)
Cannabis Influence on Brain Chemistry: Cannabis and the Brain (Sidekick)
The endocannabinoid system (ECS) plays a role in regulating a wide range of functions and processes, including mood, appetite, sleep, and memory. The ECS is made up of three core components: endocannabinoids, receptors, and enzymes.
Long term cannabis use leads to psychosis as THC (tetrahydrocannabinol) overstimulates the endocannabinoid system by quickly attaching to cannabinoid receptors throughout the brain and body, this alters dopamine & glutamate which affects perception, memory, and mood.
Cannabis Influence on Brain Chemistry: Adolescents
Studies show a strong link between cannabis use during adolescence and an increased risk of developing schizophrenia.
Adolescent brains are still developing, especially the prefrontal cortex. Cannabis use during this period disrupts brain maturation and increases the risk of psychosis. (Singh and Balhara, 2017)
Changes in endocannabinoid activity, might lead to subtle but lasting neurobiological changes that can affect brain functions and behaviour.
Cannabis Influence on Brain Chemistry: The COMT Gene & Val/Val Variant
Cannabis consumption interacts with genetic susceptibility to schizophrenia. There is an interaction between the COMT gene which some regard as a susceptibility gene for schizophrenia and cannabis consumption.
The COMT Val/Val variant clears dopamine too quickly in the prefrontal cortex. Combined with cannabis use in adolescence, this leads to greater dopamine dysregulation and higher risk of schizophrenia, due to abnormal dopamine activity.
Evaluation
Cannabis Influence:
Scientific - Di Forti (2009) - skunk (THC) increases risk of psychosis
Reductionist - Singh and Balhara (2017) cannabis use during adolescence disrupts brain maturation & increases risk of psychosis, only looks at biological effects of THC, ignores social & psychological - environmental stressors, peer pressure, learned behaviours
Evaluation of Cannabis Influence: Scientific (Strength)
A strength of explaining the influence of cannabis is that it is scientific.
Research into cannabis often uses objective methods such as brain imaging or controlled laboratory studies to measure the effect of THC on neurotransmitter activity.
Di Forti (2009) found that smoking higher potency cannabis (skunk) leads to an increase in the risk of developing psychosis, which supports the hypothesis that THC exposure increased the risk of psychosis.
This means findings are more reliable and can be replicated, which strengthens the validity of conclusions drawn about cannabis’ impact on behaviour.
Therefore, scientific explanations of cannabis are highly credible, as they are based on measurable and empirical evidence.
Evaluation of Cannabis Influence: Reductionist (Weakness)
A limitation of explaining the influence of cannabis is that it can be considered reductionist.
This is because such explanations often focus only on the biological effects of THC on neurotransmitters like dopamine, while ignoring other psychological and social influences.
By reducing cannabis’ impact to purely biological processes, this ignores the role of environmental stressors, peer pressure, or learned behaviours that may cause schizophrenia.
Therefore, while reductionist explanations provide scientific clarity, they lack a holistic understanding of cannabis’ influence on schizophrenia, as they oversimplify a complex issue.
(Conclusion)
Individual Differences Explanations of Schizophrenia: Thought Disorder (Superhero)
The argument that schizophrenia (scz.) is caused by disordered thinking is developed from the cognitive approach. This accepts the role of biological factors and argues that symptoms stem from people trying to make sense of the experiences that result from biological abnormalities.
The cognitive approach views behaviour and thoughts as being a product of internal mental processes. Mental illness is therefore explained by problems with these internal mental processes.
The symptoms of the disorder could be explained through problems with the processes that govern perception, language or attention.
Thought Disorder: Hallucinations - (Claiborn, 2009) + Frith (1992) Faulty ToM
Hallucinations are a common symptom of schizophrenia, and one of its defining characteristics. Hallucinations can be in any modality (e.g. sight, sound, touch etc).
It is estimated that around 2.5-4% of the general population have experienced hallucinations at least once in their life but are not diagnosed with a psychiatric illness (Claiborn, 2009).
A theory to explain why many schizophrenics hear voices comes from Frith (1992). He argues that some of the cognitive impairments shown by schizophrenics are due to a faulty Theory of Mind.
We all have an “inner voice” in our head. When a person hears voices, it is actually their own inner speech being misinterpreted. Frith argues that schizophrenics do not have a clear grasp of their own minds, and fail to monitor their own thoughts, misattributing them to the outside world.
According to Frith, these cognitive deficits are caused by abnormalities in the areas of the brain that use dopamine, especially the prefrontal cortex.
Thought Disorder: Lack of Preconscious Filters - Frith (1979)
Frith (1979) developed the “Attention Deficit Theory” of schizophrenia. In this theory, schizophrenia is seen as a result of the breakdown of the thought filtering process.
Schizophrenics have issues with attention, and are not able to effectively filter non-pertinent information out of consciousness.
This inability to properly focus causes schizophrenics to give the impression of disordered thought, and can possibly account for hallucinations, delusions and disorganised speech.
Thought Disorder: Negative Symptoms - Beck (2008)
Beck (2008) applied his cognitive triad to schizophrenia. He suggests that dysfunctional beliefs about their own performance leads to the schizophrenic developing a gloomy view of the future.
Their mental filters only allow the negative messages to process and leads to a pessimistic view resulting in negative symptoms of schizophrenia.
Evaluation of Thought Disorder: Deterministic (Strength) - Bowers (1966)
Schizophrenia can be explained by a number of individual differences explanations, for example, thought disorder argues that the mental illness can be explained by problems with internal mental processes.
A strength of the thought disorder explanation is that it is deterministic, suggesting schizophrenic symptoms are caused by underlying cognitive dysfunctions rather than personal choice.
For example, Bowers (1966) found that dopaminergic abnormalities cause symptoms of psychosis such as disorganised thinking in schizophrenia which is linked to difficulties in processing and integrating information.
This deterministic view promotes a scientific understanding of schizophrenia, supporting treatments like CBT that target specific cognitive deficits, and reduce negative symptoms.
It also reduces blame and stigma by framing symptoms as the result of uncontrollable mental processes rather than individual weakness and encourages individuals to seek help early and adhere to treatment plans, ultimately improving recovery outcomes.
Evaluation of Thought Disorder: Reductionist (Weakness) - Frith (1992)
A weakness of the thought disorder explanation is that it is reductionist, focusing mainly on cognitive processes while ignoring social factors.
For example, Frith (1992) suggested that disorganised thinking in schizophrenia results from impaired Theory of Mind, meaning schizophrenics do not have a clear grasp of their own minds, and that they misunderstand their own thought processes.
While this highlights cognitive mechanisms, it does not consider social influences such as family dynamics, stress, or cultural context.
This oversimplification limits its ability to fully explain individual differences and reduces its usefulness for developing holistic treatments.
Evaluation of Thought Disorder: Scientific (Strength) - Frith (1992)
A strength of the thought disorder explanation is that it is scientific, using lab-based tests to measure cognitive difficulties such as impaired ToM (Frith, 1992).
Laboratory studies provide controlled conditions, allowing researchers to replicate findings and make reliable comparisons between patients.
However, a limitation is that behaviour in an artificial lab setting may differ from real life. Participants may focus on completing tasks “correctly,” be less affected by everyday distractions, or feel anxious under observation, which can influence their responses.
Therefore, although the approach is highly reliable, it may not fully represent how disorganised thinking affects daily functioning.
Evaluation of Thought Disorder: Cause and Effect (Weakness) - Morrison
A limitation of the thought disorder explanation is the issue of cause and effect.
Morrison’s theory may explain how schizophrenia can result from hearing voices, however, it is difficult to determine whether these auditory hallucinations cause schizophrenic symptoms or are a result of the disorder itself.
This makes it hard to establish a clear causal relationship, limiting the explanation’s ability to fully account for how schizophrenia develops.
(Conclusion)
Individual Differences Explanations of Schizophrenia: Schizophrenogenic Mother (Sidekick)
Frieda Fromm-Reichman, believed that the mother-child relationship was crucial in the development of schizophrenia.
She suggested that the trigger for schizophrenia came from mothers who were overly dominant in the home, and dominant particularly towards the schizophrenic child. However, while being overbearing, controlling and overprotective, they were also cold and distant.
The overprotection stifles the child’s development, and their distance leaves the child feeling emotionally insecure. She called this type of mother Schizophrenogenic (schizophrenia causing).
Schizophrenogenic Mother: ‘Marital Schism and Marital Skew’
The central characteristics of maternal overprotection and maternal rejection were further developed by Lidz 1957 who introduced the terms marital schism and marital skew.
Marital schism referred to the failure of parents to adopt role reciprocity within the family and therefore left them emotionally ‘divorced’ from each other.
Marital skew referred to a situation where one of the marital partners seemed to dominate the family interaction. This was usually the mother. When skew was present, the mother was usually intrusive and the father distant and cold. Both contributed to the development of schizophrenia as they left the child feeling emotionally insecure.
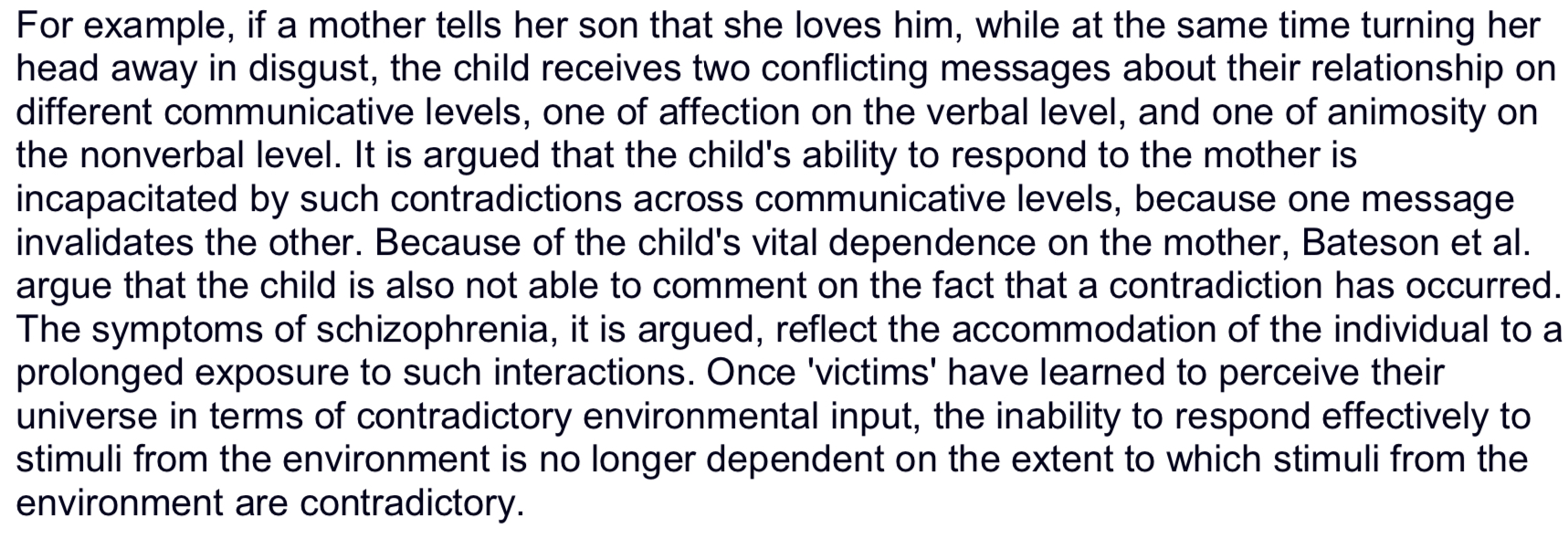
Schizophrenogenic Mother: ‘Double Bind Theory’ - Bateson 1956
Bateson 1956 introduced the ‘double bind’ theory of schizophrenia which also became associated with the schizophrenogenic mother.
He proposed that symptoms of schizophrenia are an expression of social interactions in which the individual is repeatedly exposed to conflicting communications, from the mother in particular, without having the opportunity to adequately respond to them, or to ignore them (i.e., to escape the field).
It was believed that this inconsistent communication created confusion and anxiety in the child, contributing to the development of psychotic symptoms later in life.
Evaluation of The Schizophrenogenic Mother: Deterministic (Strength) - Fromm-Reichmann (1948)
The schizophrenogenic mother explanation suggests that schizophrenia develops due to cold, controlling, and rejecting parenting.
A strength of this explanation is that it is deterministic, as it implies that children exposed to such maternal behaviour are likely to develop schizophrenia regardless of personal choice.
For example, Fromm-Reichmann (1948) described mothers of schizophrenic patients as aloof, domineering, and emotionally distant, suggesting these behaviours could contribute to the onset of the disorder.
By framing schizophrenia as influenced by identifiable environmental factors, this explanation encourages early intervention and support for families to reduce risk, through family intervention therapy.
Evaluation of The Schizophrenogenic Mother: Cause and Effect (Weakness) - Mischler (1968)
A weakness of this explanation is that its claims about cause and effect are unclear.
Mischler (1968) observed that mothers of children with schizophrenia were often aloof, unresponsive, and emotionally distant, however, it is unclear whether these maternal behaviours directly caused their child to develop schizophrenia, or whether they were a response to the child’s early symptoms.
This makes it impossible to establish a clear causal relationship, which limits the explanation’s reliability and usefulness in understanding how schizophrenia develops.
(Conclusion)
Social Psychological Explanation of Schizophrenia - Sociocultural Factors: Urbanicity
There are a number of sociocultural factors that could have an effect on how an individual experiences schizophrenia, as well as the likelihood of becoming schizophrenic in the first place.
These include urbanicity, social isolation, ethnicity and discrimination.
One key finding is that the rate of schizophrenia in urban areas is much higher than in rural areas.
Faris and Dunham (1939) found that there was a higher incidence of schizophrenia in the densely populated centre of Chicago rather than in the less densely populated suburbs; they also found that the highest levels of schizophrenia were in the areas that had a high level of ethnic conflict and a high degree of social mobility (i.e where people came and went with high frequency).
Sociocultural Factors: Urbanicity Factors affecting Pregnancy
Some of the potential factors associated by Krabbendam and van Os could link in with other explanations of schizophrenia:
Herman et al (2006) found that the stress of an unwanted pregnancy can lead to an increased chance of the child being schizophrenic. Unwanted pregnancy is related to poverty and lack of education, both associated with urbanicity.
Also, people in cities may be more prone to illness due to the cramped living conditions and poor sanitation. When mothers catch certain illnesses in pregnancy, it may cause structural abnormalities in the brain development of their baby, leading to schizophrenia.
Sociocultural Factors: Urbanicity Factors - Drug Use & Poverty
Urban areas have higher levels of drug and/or substance abuse. Zammit et al (2002) found that cannabis use doubled the risk of schizophrenia in 40,000 Swedish males.
Children who live in poverty may be more likely to suffer abuse. Bebbington et al (2004) found that sexual abuse led to a threefold increase in schizophrenia.
Sociocultural Factors: Social Isolation
The theory of social isolation links closely with the theory of urbanicity. It is often suggested that people living in cities experience greater social isolation and loneliness than those in close-knit rural communities.
Schizophrenics are frequently very socially isolated, with few friends, estranged family relationships, and a higher likelihood of living alone.
A simple explanation for this is that the illness itself and its associated behaviour lead to isolation from mainstream society.
Difficulties in communication and disturbing or confusing behaviour may hinder close relationships. However, there is also evidence that social isolation may contribute to the development of the illness or the worsening of symptoms.
Sociocultural Factors: Childhood Isolation
Research has shown a link between childhood isolation, poor early relationships, and an increased risk of schizophrenia.
Peter Jones’ (1994) longitudinal study found that those later diagnosed with schizophrenia preferred solitary play at ages 4 and 6, and by age 13 rated themselves as less socially confident, suggesting isolation begins early.
Social interaction is crucial for healthy emotional and psychological development, and a lack of positive interaction may prevent corrective feedback, allowing inappropriate thinking and behaviour to develop unchecked.
Evaluation of Sociocultural Factors: Deterministic (Strength) - Faris and Dunham (1939)
The sociocultural explanation suggests that factors such as urbanicity and social isolation increase the risk of developing schizophrenia.
A strength of this explanation is that it is deterministic, as it shows how consistent environmental pressures can cause schizophrenia regardless of individual choice.
Faris and Dunham (1939) found higher rates of schizophrenia in densely populated inner-city areas of Chicago, suggesting that social isolation and breakdown of community ties in urban environments can lead to the development of the disorder.
This deterministic view is useful because it highlights identifiable social causes, allowing for preventive measures such as improving social support and reducing urban stressors.
Evaluation of Sociocultural Factors: Cause and Effect (Weakness) - Jones et al. (1994)
A weakness of this explanation is that it struggles to establish cause and effect.
For example, Jones et al. (1994) found that individuals who later developed schizophrenia had fewer social contacts in childhood, suggesting a link between social isolation and the disorder.
However, it is unclear whether urban living and social isolation cause schizophrenia or, whether early signs of the disorder, such as unusual or withdrawn behaviour, lead individuals to be socially isolated or move to urban areas.
This uncertainty about the direction of the relationship reduces the explanation’s validity and limits its ability to clearly identify social factors as an explanation for the development of schizophrenia.
Evaluation of Sociocultural Factors: Interactionist (Strength) - Vassos et al. (2012)
The sociocultural explanation of schizophrenia considers multiple social and environmental factors, making it an Interactionist approach.
A strength is that it accounts for the complexity of schizophrenia rather than focusing on a single cause.
For example, Vassos et al. (2012) found that people living in urban areas had over twice the risk of developing schizophrenia, showing how urban stress and social isolation interact to increase risk.
By considering multiple interacting factors, this explanation provides a more complete understanding of schizophrenia and informs interventions such as improving social support and reducing urban stressors.
Evaluation of Sociocultural Factors: Not Scientific (Weakness) - Jones et al. (1994)
A weakness is that it is less scientific, as it relies on observational correlations rather than controlled experiments, making it harder to establish objective, measurable evidence.
For example, Jones et al. (1994) longitudinal study measuring the age at which social isolation begins to occur, does not show a direct causal relationship and could be influenced by many uncontrolled variables.
This reliance on correlational data reduces the explanation’s scientific credibility and makes it difficult to determine exactly how social factors contribute to schizophrenia.
(Conclusion)
Social Psychological Explanation of Schizophrenia - Expressed Emotion (EE)
Expressed Emotion (EE), introduced by George Brown, is a measure of the family environment, which includes the quality of interaction patterns and nature of family relationships.
It emphasises criticism, hostility and emotional over involvement as key features of high EE relatives (Amaresha 2012).
The stress-diathesis model suggests that the negative emotional climate caused by EE may be a major contributing factor to critical stress levels among people with schizophrenia.
There are a number of tools for measuring levels of EE. One is the Camberwell Family Interview (Brown and Rutter 1966) based on how the relatives of a psychiatric patient spontaneously talk about the individual in a taped interview.
Expressed Emotion (EE): Key Studies
High levels of EE are most likely to influence relapse rates. A patient returning to a family with high EE is about 4 times more likely to relapse that a patient whose family is low in EE (Linszen et al 1997).
Communication patterns in such families involve more intense and negative verbal exchanges which are oppositional or conflict ridden in nature (Wuerker 1994).
Research by Kuipers et al (1983) found that high EE relatives talk more and listen less.
Evaluation of Expressed Emotion (EE): Deterministic (Strength)
The Expressed Emotion (EE) explanation suggests that high levels of criticism, hostility, or over-involvement from family members can increase the risk of relapse in people with schizophrenia.
A strength of this explanation is that it is deterministic, as it shows how certain family environments can strongly influence someone’s recovery.
Linszen et al. (1997) found that patients returning to high-EE homes were about four times more likely to relapse than those in low-EE homes.
This shows that family behaviour can directly affect outcomes, making the explanation useful as it helps develop treatments like family therapy to reduce EE and prevent relapse.
Evaluation of Expressed Emotion (EE): Reductionist (Weakness)
A weakness is that it is reductionist, as it focuses only on family communication while ignoring biological or individual factors.
George Brown (1950s) studied 156 men with schizophrenia and found that relapse was more common in patients returning to live with parents or spouses than in those living in lodgings or with siblings, showing that family environment plays a key role.
However, this overlooks how factors like genetics, stress, or medication may also influence relapse, meaning the EE explanation oversimplifies a complex disorder, by reducing it to only environmental factors)
(Conclusion)
Methods of Modifying Schizophrenia: Antipsychotic Drugs
Antipsychotic drug treatments are based on the dopamine hypothesis as an explanation for schizophrenia and aim to address the associated chemical imbalance.
Antipsychotic medications allow the patient to function more effectively and appropriately.
Conventional antipsychotic drugs (e.g. chlorpromazine) are used primarily to combat the positive symptoms (e.g. hallucinations, delusions) of the disorder by reducing dopamine levels in the mesolimbic system, but also lowers dopamine in other areas causing cognitive, emotional, and motor side effects.
Carlsson and Lindqvist (1957) identified that these drugs reduced levels of dopamine uptake when administered to animals.
Atypical antipsychotic drugs are thought to combat both positive and negative symptoms of schizophrenia.
Atypical antipsychotics block D2 receptors but also block serotonin 5-HT2A receptors, which increases dopamine in the mesocortical and nigrostriatal systems.
This helps maintain balanced dopamine in these areas, reducing the side effects seen with conventional antipsychotics.
Antipsychotic Drugs: Effectiveness
(Kapur 2003) argues that the psychological effect of antipsychotic drugs is ‘dampening salience’ which requires the patient to then ‘work through’ their symptoms towards a psychological resolution.
Antipsychotics at first reduce the degree to which the symptoms occupy the mind, distress the patient and drive action.
It is only later that the fundamental content of the delusions and hallucinations may be deconstructed and (only for some) recedes entirely from awareness.
However, a significant proportion of patients show suboptimal treatment responses and poor tolerability of current antipsychotics. According to (Miller 1987) improvement in psychotic symptoms after taking antipsychotics is slow and cumulative.
Evaluation of Antipsychotic Drugs: Effectiveness - Symptom Reduction (Strength)
Antipsychotic drugs are effective because they reduce the symptoms of schizophrenia.
A strength is that they can significantly improve patients’ daily functioning by targeting the biological causes of symptoms.
For example, Littrell (2015) notes that antipsychotics, which block dopamine receptors, reduce the more dramatic positive symptoms of schizophrenia, such as hallucinations and delusions.
This shows that medication can directly decrease symptom severity and improve quality of life, making antipsychotics a practical and reliable treatment option for managing schizophrenia.
Evaluation of Antipsychotic Drugs: Effectiveness - Severe side effects (Weakness)
A weakness of antipsychotic drugs is that they can cause severe side effects, reducing their overall effectiveness.
While they may reduce positive symptoms, Hill (1986) found that patients often experienced serious motor problems, such as tardive dyskinesia, due to dopamine blockade in the nigrostriatal system.
In addition, antipsychotics can cause weight gain, which increases the risk of other health problems such as diabetes and high blood pressure.
These side effects can make patients stop taking their medication, meaning symptoms may return or worsen.
Therefore, although antipsychotics can modify behaviour, their severe side effects limit their practical usefulness and long-term effectiveness.
Evaluation of Antipsychotic Drugs: Effectiveness - Atypical Advantage (Strength)
A strength of antipsychotic drugs is that atypical antipsychotics are effective while causing fewer side effects than conventional drugs.
This makes them more tolerable, improving adherence and overall treatment success. Kapur and Remington (2001) note that atypical antipsychotics block D2 dopamine receptors but also act on serotonin receptors, which helps maintain dopamine balance in areas responsible for motor control.
As a result, patients experience fewer movement-related side effects, such as tardive dyskinesia, compared to conventional antipsychotics.
This shows that atypical antipsychotics can reduce symptoms of schizophrenia while minimizing negative impacts on health, increasing their effectiveness, as patients will be more likely to continue with their medication reaping long lasting benefits.
Evaluation of Antipsychotic Drugs: Effectiveness - Weakness
A weakness of antipsychotic drugs is that they can reduce motivation and the ability to experience pleasure, limiting overall effectiveness.
Lewander (1994) found that patients on antipsychotics show ‘dampened salience’ or reduced motivational drive for objects and ideas that were previously highly rewarding.
Kapur (2003) suggests this may explain why patients with schizophrenia have a higher incidence of drug abuse, self-medication, and other attempts to overcome this dampening.
This can lead to high rates of medication discontinuation and difficulties with social integration.
Therefore, while antipsychotics reduce hallucinations and delusions, these side effects can negatively impact quality of life and limit long-term effectiveness.
(Conclusion)
Evaluation of Antipsychotic Drugs: Ethical Issues - Informed Consent & Right to Withdraw
A weakness of antipsychotic drug treatment is that it raises ethical issues around informed consent and the right to withdraw.
Patients with schizophrenia may not be in the right frame of mind to fully understand the risks and benefits of their medication.
Lobos (2010) found that many patients discontinue antipsychotics due to side effects, showing that even when prescribed, patients may feel unable to continue or make fully informed decisions.
This highlights concerns about autonomy, as patients may be pressured into treatment or unable to make voluntary choices, potentially compromising both their rights and their wellbeing.
Evaluation of Antipsychotic Drugs: Ethical Strength - Benefits of Medication
A strength of antipsychotic drugs is that they provide clear ethical benefits by improving patients’ quality of life.
By reducing positive symptoms, patients can regain control over their thoughts and behaviour, enhancing daily functioning and safety. For example, Littrell (2015) notes that antipsychotics block dopamine receptors and decrease dramatic symptoms like hallucinations and delusions, allowing patients to engage more fully in social and occupational activities.
This means that, ethically, prescribing antipsychotics can be justified because the benefits to patients’ wellbeing outweigh the risks, making treatment a valuable intervention.
Evaluation of Antipsychotic Drugs: Ethical Issue - Weight gain
A weakness of antipsychotic drugs is that their severe side effects raise ethical concerns.
Weight gain caused by some antipsychotics can lead to high blood pressure, diabetes, and in rare cases, fatal agranulocytosis, creating significant health risks.
These side effects also contribute to high rates of medication discontinuation and difficulties with social integration.
For example, Lobos (2010) found that patients often stopped taking their medication due to side effects, which not only reduced treatment effectiveness but also increased long-term healthcare costs.
This shows that, although antipsychotics can control symptoms, their serious side effects make their use ethically challenging.
Evaluation of Antipsychotic Drugs: Social Implications - Economic Burden (Strength & Weakness)
A social implication of antipsychotic drugs is their economic impact on healthcare systems.
On the positive side, providing antipsychotics can reduce long-term costs by preventing relapse and the need for extended hospitalisation. Eisenberg (2010) argues that deinstitutionalisation as a result of antipsychotics, has been an overall benefit for most psychiatric patients.
Furthermore, chlorpromazine is cheap to produce and is still widely used in developing countries, making treatment accessible where resources are limited.
However, in wealthier countries, modern antipsychotics are more expensive, and side effects such as weight gain can increase healthcare costs due to additional treatments.
This shows that while antipsychotics can save money and improve social outcomes in the long term, their cost and side effects also create a significant economic burden.
Evaluation of Antipsychotic Drugs: Social Implications - Social Stigma & Labelling
A social implication of antipsychotic drugs is their effect on social stigma and labelling.
A positive is that using medication based on the medical model and Kraeplin’s view of schizophrenia as a disease, helps patients understand that schizophrenia is a biological illness, which can reduce blame and social stigma while giving access to professional treatment.
However, a downside is that this medical perspective can justify coercive treatment, since individuals may be seen as less responsible for their behaviour.
Therefore, while antipsychotics can help reduce stigma, they may also reduce independence and raise social implications about forcing treatment on patients.
(Conclusion)
Methods of Modifying Schizophrenia: Cognitive Behavioural Therapy (CBT)
Cognitive Behavioural Therapy (CBT) is often used in conjunction with antipsychotics and it works by replacing maladaptive thoughts with more rational ones.
CBT aims to enable the patient to acknowledge their thinking is maladaptive, and accept this rather than merely change the thinking.
CBT is used to help individuals who are suffering with schizophrenia to think about and organise their disorganised thoughts (a common positive symptom). One of its purposes is to make the individual aware of the connections between their disorganised thinking and their illness.
The therapist will try to make these disorganised thoughts conscious, and then by challenging them, the patient will see that there is no basis for these thoughts.
This is done during therapy in several ways such as :
Socratic questioning
Dysfunctional thought diary
Behavioural Experiments
During CBT the therapist lets the patient develop their own alternatives to previous maladaptive beliefs.
Cognitive Behavioural Therapy (CBT): Murray 2005 & Effects
Murray 2005 argues that CBT helps patients to reassess whether they were interpreting the world in a paranoid way, and consider that perhaps they may have been mistaken; this involves examining the evidence that led them to the delusional conclusion.
Cognitive therapy can only be successful if the psychologist accepts the client’s perception of reality and determines how to use this ‘misperception’ to assist the client in managing life problems.
CBT can be used mainly to reduce the positive symptoms of schizophrenia (delusions, disordered thinking etc).
However, when armed with the right cognitive skills, the schizophrenic may be empowered to be more independent, and may have more confidence.
This may have the knock-on effect that negative symptoms (particularly avolition and asociality) may also be reduced.
Evaluation of Cognitive Behavioural Therapy (CBT): Effective - Drury et al. (1996) + Kuipers et al. (1997)
The aim of CBT is to challenge maladaptive thoughts and replace them with constructive thinking that will lead to healthy behaviour.
A strength of CBT for schizophrenia is that it has been shown to be effective in reducing positive symptoms and improving recovery.
Research suggests that patients who receive CBT experience fewer hallucinations and delusions compared to those treated with medication alone.
Drury et al. (1996) found that combining CBT with antipsychotic medication led to faster recovery, while Kuipers et al. (1997) also reported lower dropout rates and higher patient satisfaction with combined treatment.
This suggests that CBT is an effective method of modifying behaviour, particularly when used alongside medication, as it helps patients better understand and manage their symptoms.
Evaluation of Cognitive Behavioural Therapy (CBT): Ineffective - Not suitable for all (Kingdon and Kirschen (2006)
A weakness of CBT for schizophrenia is that it is not suitable for all patients.
Those with severe symptoms or who deny their illness may struggle to engage with the cognitive and behavioural tasks required, limiting its effectiveness.
Kingdon and Kirschen (2006) found that many patients were judged unsuitable for CBT, as psychiatrists believed they would not fully engage with therapy—particularly older patients.
This suggests that CBT may only benefit those with less severe symptoms or who are more willing to work to overcome their illness, meaning study results could be biased towards patients already more likely to recover.
Therefore, CBT cannot be seen as an effective treatment for all individuals with schizophrenia.
Evaluation of Cognitive Behavioural Therapy (CBT): Effective - Bradshaw (1997)
A strength of CBT for schizophrenia is that it provides patients with skills to cope with schizophrenia, reducing reliance on antipsychotic medication.
Bradshaw (1997) found that clients in a four-year outpatient CBT programme experienced significant reductions in symptoms and rehospitalisation, along with improved psychosocial functioning at a one-year follow-up.
These lasting benefits may occur because CBT teaches patients coping strategies and ways to challenge unhelpful thoughts, which they can continue to use after therapy ends.
This shows that CBT can provide enduring improvements in both symptoms and daily functioning, making it a valuable treatment for schizophrenia.
Evaluation of Cognitive Behavioural Therapy (CBT): Ineffective - Unskilled Therapists (Wykes et al. (2008)
A weakness of CBT for schizophrenia is that its effectiveness depends on the skill of the therapist.
Wykes et al. (2008) note that most studies involve CBT delivered by highly trained experts, so the results may not reflect what happens in real-world settings.
CBT provided by less skilled or briefly trained staff may be less effective, meaning patients may not receive the full benefits of the therapy.
This limits how widely CBT can be recommended and reduces its overall practical effectiveness in everyday mental health services.
(Conclusion)
Evaluation of Cognitive Behavioural Therapy (CBT): Ethical Strength/Weakness - Lack of side effects
An ethical strength of CBT is that it does not cause physical side effects.
Unlike antipsychotic medication, which can lead to weight gain, tardive dyskinesia, or even fatal agranulocytosis, CBT is a psychological treatment free from such risks.
However, a weakness is that CBT may be less effective without antipsychotic medication, as patients often need medication to gain enough control over their thinking and behaviour to benefit fully from therapy.
This means that while CBT avoids harmful side effects, its ethical advantage may be reduced if symptom reduction is limited when used alone.
Evaluation of Cognitive Behavioural Therapy (CBT): Ethical Issue - Only treats symptoms not causes Bentall et al. (1994)
A weakness of CBT is that it may raise ethical concerns by focusing on symptom control rather than understanding underlying causes.
Bentall et al. (1994) argue that CBT targets current thought processes, such as paranoid delusions, without exploring their deeper origins, which may lie in early life experiences.
This means therapy may only treat the symptoms rather than addressing the root causes of distress.
Ethically, this could be limiting because patients are not given the opportunity to fully understand or resolve the deeper factors contributing to their schizophrenia, potentially restricting long-term personal growth.
Evaluation of Cognitive Behavioural Therapy (CBT): Ethical Strength - Consent
A strength of CBT is that it is an ethical form of therapy because it is entered into voluntarily.
Unlike antipsychotic medication, which may be given against a patient’s will, CBT requires informed consent and can be withdrawn at any time.
This allows patients to maintain control over their treatment and increases their independence in managing symptoms.
CBT also provides strategies to support self-management, enabling patients to participate more fully in society.
This makes CBT a more ethically favourable treatment option compared to coercive drug therapy.
Evaluation of Cognitive Behavioural Therapy (CBT): Positive & Negative Social Implication - Society
A positive social implication of CBT is that it provides patients with skills to cope with schizophrenia, reducing reliance on antipsychotic medication.
Without access to psychological treatments, patients may remain dependent on drugs for the rest of their lives, limiting their ability to manage symptoms independently.
CBT allows individuals to develop coping strategies, improving daily functioning and social participation.
However, a weakness is that access to CBT is unequal across the UK, with a “postcode lottery” meaning some patients cannot receive this therapy depending on where they live.
This limits the social benefits of CBT and creates inequalities in treatment availability.
Evaluation of Cognitive Behavioural Therapy (CBT): Negative Social Implication - Cost
A weakness of CBT is that it can be expensive, limiting its availability to patients.
The long-term cost of providing a full course of CBT is often higher than the cost of prescribing antipsychotic medication alone.
Since most patients receiving CBT are also on medication, it may be seen as more cost-effective by health services to rely solely on drugs.
This financial barrier means that many patients do not have access to CBT, reducing the social benefits of therapy and creating inequalities in treatment.
Evaluation of Cognitive Behavioural Therapy (CBT): Positive Social Implication - Use with medication & Cost Kuipers (1998)
A strength of CBT is that, when combined with antipsychotic medication, it can improve outcomes and reduce long-term costs.
Kuipers (1998) argues that medication alone often leads to non-adherence and relapse, resulting in repeated hospitalisations.
Adding CBT can help patients manage symptoms more effectively, reducing the likelihood of rehospitalisation. While the initial cost may be higher, long-term savings occur as fewer patients require institutional care.
This benefits society by freeing up resources and allowing more funding for other patients in need, while also reducing the social impact of having large numbers of individuals confined in psychiatric hospitals.
(Conclusion)
Applying The Dopamine Hypothesis (Biological Explanation) to Methods of Modifying Behaviour
The biological explanation of the dopamine hypothesis suggests that schizophrenia is caused by abnormal dopamine activity in the brain.
Individuals with schizophrenia have an excess of dopamine and a higher number of D2 receptors, causing overactivity in certain brain areas and leading to positive symptoms such as hallucinations.
Davis (1991) updated this explanation, showing that dopamine levels vary across brain regions — with too much dopamine in the mesolimbic pathway causing positive symptoms and too little dopamine in the prefrontal cortex leads to negative symptoms like avolition.
Applying The Dopamine Hypothesis to Antipsychotic Drugs
The method of modifying should therefore work by reducing dopamine activity in the limbic system to reduce positive symptoms of schizophrenia while also increasing dopamine reuptake in the mesocortical regions such as the frontal cortex that result in negative symptoms, through the use of:
Antipsychotic Drugs
Antipsychotic drug treatments are based on the dopamine hypothesis as an explanation for schizophrenia and aim to address the associated chemical imbalance. Antipsychotic medications allow the patient to function more effectively and appropriately.
Applying The Dopamine Hypothesis to Antipsychotic Drugs - Outline of method of modifying
Conventional antipsychotic drugs (e.g. chlorpromazine) are used primarily to combat the positive symptoms (e.g. hallucinations, delusions) of the disorder by reducing dopamine levels in the mesolimbic system, but also lower dopamine in other areas causing cognitive, emotional, and motor side effects.
Atypical antipsychotic drugs are thought to combat both positive and negative symptoms of schizophrenia.
Atypical antipsychotics block D2 receptors but also block serotonin 5-HT2A receptors, which increases dopamine in the mesocortical and nigrostriatal systems.
This helps maintain balanced dopamine in these areas, reducing the side effects seen with conventional antipsychotics.
Applying Thought Disorder (Individual Differences Explanation) to Methods of Modifying Behaviour
The argument that schizophrenia is caused by disordered thinking is developed from the cognitive approach.
This accepts the role of biological factors and argues that symptoms stem from people trying to make sense of the experiences that result from biological abnormalities.
Frith (1979) developed the “Attention Deficit Theory” of schizophrenia. In this theory, schizophrenia is seen as a result of the breakdown of the thought filtering process.
Schizophrenics have issues with attention, and are not able to effectively filter non-pertinent information out of consciousness.
This inability to properly focus causes schizophrenics to give the impression of disordered thought, and can possibly account for hallucinations, delusions and disorganised speech.
Applying Thought Disorder to Cognitive Behavioural Therapy
The method of modifying should therefore work by replacing maladaptive thoughts with more rational ones, by acknowledging that the schizophrenic's inability to process information normally leads to disorganised thinking.
This method of modifying aims to enable the patient to acknowledge their thinking is maladaptive, and accept this rather than merely change the thinking through:
Cognitive Behavioural Therapy (CBT)
CBT is used to help individuals who are suffering with schizophrenia to think about and organise their disorganised thoughts (a common positive symptom). One of its purposes is to make the individual aware of the connections between their disorganised thinking and their illness.
Applying Thought Disorder to Cognitive Behavioural Therapy - Outline of Method of Modifying
The therapist will try to make these disorganised thoughts conscious, and then by challenging them, the patient will see that there is no basis for these thoughts.
During CBT the therapist lets the patient develop their own alternatives to previous maladaptive beliefs.
Murray 2005 argues that CBT helps patients to reassess whether they were interpreting the world in a paranoid way, and consider that perhaps they may have been mistaken; this involves examining the evidence that led them to the delusional conclusion.
Cognitive therapy can only be successful if the psychologist accepts the client’s perception of reality and determines how to use this ‘misperception’ to assist the client in managing life problems.
Applying Expressed Emotion (Social Psychological Explanation) to Methods of Modifying Behaviour
EE is a measure of the family environment, which includes the quality of interaction patterns and nature of family relationships.
It emphasises criticism, hostility and emotional over involvement as key features of high EE relatives (Amaresha 2012).
The stress-diathesis model combines both biological and environmental factors to explain mental disorders. Research suggests that the negative emotional climate caused by EE may be a major contributing factor to critical stress levels among people with schizophrenia.
There are a number of tools for measuring levels of EE. One is the Camberwell Family Interview (Brown and Rutter 1966) based on how the relatives of a psychiatric patient spontaneously talk about the individual in a taped interview.
Applying Expressed Emotion to Family Intervention Therapy
The method of modifying should therefore work by changing the behaviour of the family: Treating the family rather than just the schizophrenic through:
Family Intervention therapy
With the increasing deinstitutionalization of patients, family has assumed the role of care performed by psychiatric hospitals, with a high emotional cost for caregivers as well as the recognition of burden experiences.
Applying Expressed Emotion to Family Intervention Therapy - Outline of method of modifying
Family intervention involves working with the relatives of people with psychosis to build a collaborative relationship with mental health professionals and support recovery.
It typically includes psychoeducation, stress reduction, emotional processing, cognitive reappraisal, and problem solving.
Psychoeducation reduces recurrence and improves adherence to medication received by the patient and also allows the family to increase their knowledge and coping strategies.
These coping skills reduce family stress and expressed emotion (EE), improving outcomes and quality of life for both patients and relatives.
Modern family therapy therefore focuses on promoting empathy, support, and healthier communication within the family.