GW BGZ2026 Case 2 - How do drugs act on molecular level?
1/32
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
33 Terms
What is the function of the heart and what are the main structures?
The heart is a muscular pump that maintains continuous blood circulation by generating pressure to drive blood through two connected systems:
Systemic circulation → left heart → body → right heart
Pulmonary circulation → right heart → lungs → left heart
Its main role is to ensure oxygen and nutrient delivery and waste removal.
The heart consists of:
Right heart
Pumps deoxygenated blood to the lungs
Left heart
Pumps oxygenated blood to the systemic circulation
Valves (tricuspid, pulmonary, mitral, aortic)
Ensure one-way blood flow
Prevent backflow during contraction
What are the main types of blood vessels and their functions?
Blood vessels are specialized for different roles:
Arteries
Carry blood away from the heart
High pressure, thick muscular walls
Arterioles
Main resistance vessels
Major regulators of blood pressure
Capillaries
Site of exchange (O₂, CO₂, nutrients, waste)
Very thin walls for diffusion
Veins
Return blood to the heart
Low pressure, act as blood reservoir
Blood vessels are not passive tubes:
They actively regulate blood pressure
They control regional blood flow distribution
Especially arterioles determine total peripheral resistance
What are catecholamines?
Catecholamines are stress hormones released during “fight or flight”:
Adrenaline (epinephrine)
Noradrenaline (norepinephrine)
They are released from the adrenal medulla in response to stress or sympathetic activation.
How do catecholamines affect the heart?
Mainly via β₁-adrenergic receptors:
↑ Heart rate (chronotropy)
↑ Contractility (inotropy)
↑ Cardiac output
Result:
The heart pumps faster and stronger
More oxygenated blood is delivered to tissues
How do catecholamines affect blood vessels?
Effects depend on receptor type:
α₁ receptors (most vessels)
→ vasoconstriction
→ ↑ systemic blood pressure
β₂ receptors (skeletal muscle, lungs)
→ vasodilation
→ increased blood flow to muscles
What is the net effect of catecholamines?
Combined effects lead to:
Increased blood pressure
Redistribution of blood flow
more to muscles and heart
less to digestive system
Preparation for rapid physical activity
How is blood vessel tone regulated?
By GPCR-mediated signaling pathways in smooth muscle cells:
Balance between contraction and relaxation signals
Controlled by intracellular messengers:
Ca²⁺ → contraction
cAMP → relaxation
How does vasoconstriction and vasodiliation occur?
Vasoconstriction
Mainly via α₁ receptors (Gq pathway):
Activation → IP₃ increases intracellular Ca²⁺
Ca²⁺ → smooth muscle contraction
Vessel diameter decreases
→ increased blood pressure
Vasodilation
Mainly via β₂ receptors (Gs pathway):
Activation → ↑ cAMP
cAMP inhibits contraction machinery
Smooth muscle relaxes
Vessel diameter increases
→ decreased resistance / BP or redistribution
What is the baroreflex?
A fast neural feedback system that stabilizes blood pressure:
Sensors in carotid sinus & aortic arch
Detect changes in pressure
Adjust:
heart rate
vascular tone
If BP drops:
↑ sympathetic activity
↑ heart rate
↑ vasoconstriction
What is RAAS?
A slow hormonal system activated by low blood pressure:
Kidney releases renin
→ angiotensin II formation
Effects:
vasoconstriction
stimulates aldosterone
Aldosterone:
↑ Na⁺ and water retention
↑ blood volume → ↑ BP
What is ADH?
Antidiuretic hormone:
Increases water reabsorption in kidneys
Increases blood volume
→ raises blood pressure
What is ANP?
A hormone released when BP is too high:
Causes vasodilation
Promotes salt and water excretion
Opposes RAAS
How do drugs lower blood pressure?
By targeting heart, vessels, or fluid volume:
β-blockers
↓ heart rate and contractility
ACE inhibitors
↓ angiotensin II → vasodilation
Diuretics
↓ blood volume
Calcium channel blockers
relax vascular smooth muscle
How do drugs increase blood pressure?
By increasing vascular tone or cardiac output:
α₁ agonists
vasoconstriction
Adrenaline (emergency use)
↑ heart rate + vasoconstriction
How does stress affect blood pressure?
Stress activates catecholamines leading to:
↑ cardiac output (β₁)
↑ vasoconstriction (α₁)
blood redistribution
Result:
Rapid increase in blood pressure (“fight or flight response”)
What is log₁₀(x)?
It is the power to which 10 must be raised to obtain x:
log₁₀(x) = y → 10ʸ = x
Examples:
log₁₀(1) = 0
log₁₀(10) = 1
log₁₀(100) = 2
How do you convert number → log?
Take log base 10
Example: log₁₀(50) ≈ 1.7
→ because 10¹·⁷ ≈ 50
How do you convert log → number?
Raise 10 to the power of the log value
Example: log₁₀(x) = 3
→ x = 10³ = 1000
What are the 5 main biologic drug target categories?
1. Receptors
Bind signaling molecules (hormones, neurotransmitters)
Example: β-adrenoceptors
2. Enzymes
Catalyze biochemical reactions
Inhibition alters pathways
Example drugs:
ACE inhibitors
Aspirin
Statins
3. Transporters
Move molecules across membranes
Example:
Fluoxetine blocks SERT
→ more serotonin in synapse
4. Ion channels
Control ion flow and excitability
Example:
Amlodipine blocks Ca²⁺ channels
→ vasodilation
5. Structural proteins / nucleic acids
Affect cell structure or DNA function
Example:
Paclitaxel → tubulin stabilization
What 5 different receptors are there?
1. GPCRs (7TMRs)
Largest receptor family (>800 genes)
Span the membrane 7 times
Activate G proteins
Produce second messengers such as:
cAMP
IP₃
DAG
Second messengers activate proteins like protein kinase A (PKA).
2. Ligand-gated ion channels
The receptor is the ion channel.
Ligand binding opens the channel within milliseconds.
Allows ions such as:
Na⁺
K⁺
Cl⁻
Ca²⁺
3. Kinase-linked receptors
Usually activated by:
Growth factors
Insulin
Ligand binding causes receptor dimerization.
Intracellular kinase phosphorylates proteins.
Leads to changes in cell growth, metabolism, or survival.
4. Nuclear receptors
Located inside the cell (cytoplasm or nucleus).
Ligands are lipid-soluble and cross the cell membrane.
Ligand–receptor complex binds DNA and changes gene expression.
Slow onset (hours to days), but effects last longer.
5. Cytokine receptors
Bind cytokines involved in immune regulation.
Lack intrinsic kinase activity.
Signal mainly through the JAK–STAT pathway.
Important in inflammation and immune responses.
What is propranolol, how does it work and what is the effect?
Non-selective β-adrenoceptor antagonist
Target: Blocks β₁ and β₂ adrenergic receptors
Competitively blocks β1 receptors in the heart:
Decreases heart rate (negative chronotropy)
Decreases force of contraction (negative inotropy)
Slows conduction through the AV node
Blocks β2 receptors in the lungs and blood vessels:
Can cause bronchoconstriction
May reduce glycogen breakdown and mask signs of low blood sugar
Normal β-receptor signaling
Adrenaline or noradrenaline binds β receptors:
β receptor → Gs protein → adenylyl cyclase → ↑ cAMP → ↑ PKA activity
Results:
Increased heart rate
Increased contractility
Increased renin release
What is amlodipine, how does it work and what is the effect?
Dihydropyridine calcium channel blocker.
Blocks L-type calcium channels in smooth muscle
Reduces calcium entry into cells
With amlodipine
↓ Ca²⁺ entry → ↓ contraction → smooth muscle relaxation
Leads to:
Vasodilation (especially arteries)
Lower peripheral resistance
Reduced blood pressure
Normal calcium channel function Calcium enters smooth muscle cells through L-type channels.
Calcium binds calmodulin.
This activates myosin light-chain kinase.
Result:
Smooth muscle contraction.
What is salbutamol, how does it work and what is the effect?
Salbutamol is a selective β₂-adrenoceptor agonist
It is a drug mainly used as a bronchodilator in respiratory disease
Target type: G protein-coupled receptor (GPCR)
Binds to β₂ receptors on smooth muscle (especially in the lungs)
Activates the Gs protein pathway
Leads to:
↑ Adenylyl cyclase activity
↑ cAMP
↑ Protein kinase A (PKA) activation
This causes:
↓ intracellular calcium
Relaxation of smooth muscle
Key idea:
β₂ activation → smooth muscle relaxation
What blood pressure medications are there and how do they work?
β-blockers (e.g. propranolol, metoprolol)
Block β₁ receptors (heart + kidney)
Effects:
↓ heart rate
↓ contractility
↓ renin release
↓ blood pressure
ACE inhibitors (e.g. enalapril, lisinopril)
Block ACE enzyme
Effects:
↓ angiotensin II
↑ vasodilation (also ↑ bradykinin)
↓ aldosterone
↓ blood pressure
ARBs (e.g. losartan, valsartan)
Block AT₁ receptor (angiotensin II receptor)
Effects:
Prevent vasoconstriction
↓ aldosterone release
↓ blood pressure
Renin inhibitors (e.g. aliskiren)
Block renin
Effects:
↓ angiotensin I → ↓ angiotensin II
↓ blood pressure
Calcium channel blockers (e.g. amlodipine)
Block L-type Ca²⁺ channels
Effects:
↓ vascular smooth muscle contraction
Vasodilation
↓ peripheral resistance → ↓ BP
Diuretics (e.g. hydrochlorothiazide, furosemide)
Increase Na⁺ and water excretion
Effects:
↓ blood volume
↓ blood pressure
What are affinity, potency, and efficacy?
1. Affinity
How strongly a drug binds to a receptor
Measured by KD
Lower KD = higher affinity
KD = is the concentration of a drug (ligand) at which 50% of the target receptors are bound by the drug at equilibrium.
KD= k off/k on
2. Potency
How much drug is needed for an effect
Measured by EC50
The concentration producing 50% maximal effect.
Lower EC50 = higher potency
3. Efficacy
Maximum effect a drug can produce
Measured by Emax
Emax most commonly refers to the maximum drug effect in pharmacology
Higher Emax = greater effect possible
Is a higher dose always better?
No
Dose–response is sigmoidal
After receptor saturation:
No extra benefit
More side effects
More toxicity
Key idea
Use lowest effective dose
What is dose margin (therapeutic window)?
Range between:
Effective dose (ED50)
Toxic dose (TD50)
Formula:
Therapeutic index = TD50 / ED50
Interpretation:
High TI → safer drug
Low TI → narrow safety margin
What is an agonist and what types are there?
An agonist:
Binds receptor
Activates receptor
Produces response
Full agonist
Binds to a receptor and produces the maximum possible response (Emax).
Has high efficacy.
Partial agonist
Binds to the receptor but produces less than the maximum response, even when all receptors are occupied.
Has lower efficacy than a full agonist.
Can act as an antagonist in the presence of a full agonist because it competes for the same receptor.
What is an antagonist and what types are there?
An antagonist:
Binds receptor
Does not activate receptor
Blocks agonist action
Competitive antagonist
Binds to the same (active) binding site as the agonist.
Binding is reversible.
Can be overcome by increasing the agonist concentration.
Effect on dose-response curve
Emax: unchanged
EC₅₀: increases (curve shifts to the right)
Non-competitive antagonist
Binds irreversibly to the active site or binds to an allosteric site.
Prevents receptor activation even if more agonist is added.
Cannot be overcome by increasing agonist concentration.
Effect on dose-response curve
Emax: decreases
EC₅₀: usually unchanged
Would you prefer an antagonist or an agonist for treating a disease?
Antagonists (usually preferred)
Block excessive signalling
Safer
Less receptor overstimulation
Agonists
Used when signalling is too low
Higher risk:
tolerance
receptor downregulation
Rule
Too much activity → antagonist
Too little activity → agonist
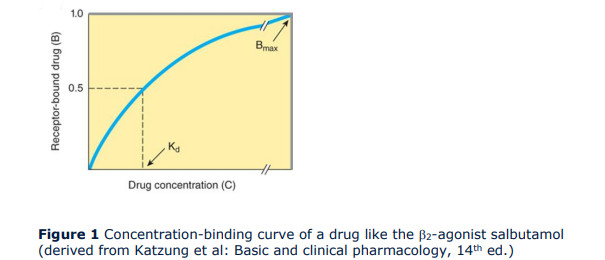
Describe what you see in the curves and what information can you get out of it?
This curve shows how much drug is bound to receptors as concentration increases.
What you see
Sigmoidal (saturable) curve
At low concentrations → little binding
At higher concentrations → binding increases
Eventually reaches a plateau = Bmax
Key information you get
KD (affinity)
Concentration where 50% of receptors are occupied
Low KD → high affinity (left shift)
Bmax
Maximum binding capacity
Reflects total number of receptors, not drug strength
Main concept
This is about binding, not effect
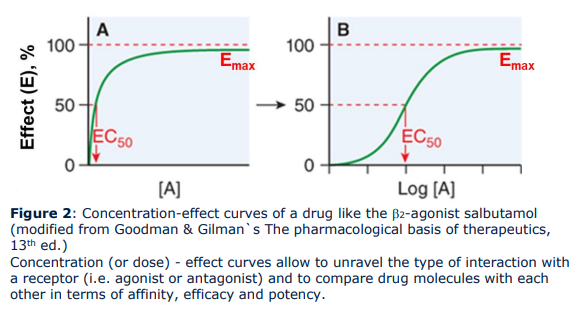
Describe what you see in the curves and what information can you get out of it?
This shows drug concentration vs biological response.
What you see
Sigmoidal curve (usually plotted on log scale)
Low dose → small effect
Middle range → steep increase
High dose → plateau (Emax)
Why log scale is used
Expands the middle (clinically relevant) part
Makes EC50 easier to compare between drugs
Key information you get
EC50 (potency)
Concentration that gives 50% of max effect
Low EC50 → high potency
Emax (efficacy)
Maximum achievable effect
Independent of dose once saturation is reached
Key concept
Effect ≠ binding
Full receptor binding does not always equal full effect (receptor reserve, signaling efficiency)
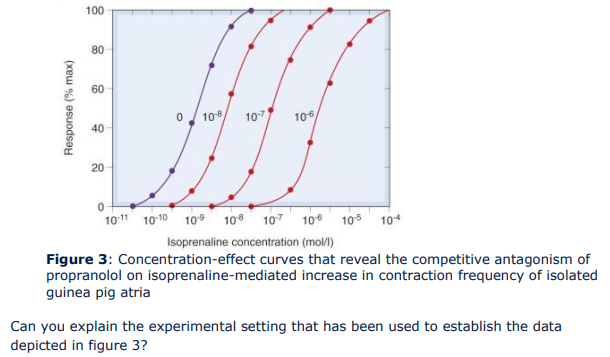
Describe what you see in the curves and what information can you get out of it?
This shows what happens when an antagonist competes with an agonist at the same receptor.
What you see
Multiple dose–response curves
With increasing antagonist:
Curve shifts to the right
Shape stays the same
Maximum height stays the same
What changes
EC50 increases → potency decreases
Need more agonist to get same effect
What does NOT change
Emax stays the same
Because high agonist concentration can outcompete antagonist
Mechanism
Reversible binding at the same receptor site
Competition depends on concentration
Key conclusion
Competitive antagonists reduce potency but do not reduce efficacy.