Travel Medicine
1/22
Earn XP
Description and Tags
PEBC
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
23 Terms
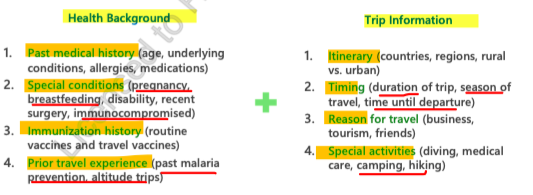
pre travel consultation
see travel specialist at least 6 weeks before travel
clinicians review patients medical and immunization history
trip specific health concerns based on pt medical hx and area of travel
prevention strategies
high altitude illness
insect protection
sun safety
water and food safety
thrombosis prevention
jet lag
vaccinations
high altitude illness
travelling to high elevations = these areas have lower partial pressure and can lead to hypoxia (inadequate oxygen supply at the tissue level)
ask pts if travelling to regions higher than 2000 meters above sea level
leads to Acute Mountain Sickness (AMS)
High altitude mountain sickness (AMS)
symptoms (w/in 48 hr of new altitude):
CNS = HA, lightheadedness
GI = Anorexia/ loss of appetite
MSK = weakness, fatigue
can progress to more serious forms:
High altitude cerebral edema (HACE) = end stage of AMS
High altitude pulmonary edema (HAPE) = not necessarily a progression form! it can occur on its own
prevention:
Ascend slowly and avoid direct transport to altitudes >3000 meters
spend 1-2 nights at 2500-3000m to acclimatize
>2500-3000m, sleeping altitude should not be increased by more than 300-500m/night (rest 2 nights at the same altitude every 2-3 days)
avoid alcohol/sedatives/hypnotics
high carb diet decreases AMS sx by 30%
avoid overexertion
treatment of AMS
Acetazolamide 250mg Q12H - initiated soon after AMS sx and continue until sx cleared (to a max of 4 days)
s/e = Diarrhea, upset stomach, or throwing up, Change in taste, Decreased appetite, Blurred eyesight, Feeling dizzy, sleepy, tired, or weak, Headache, Flushing, Feeling nervous and excitable
take with food to decrease stomach upset
rest and acclimatization at 1 altitude
dexamethasone 4mg q6H until 24hr after symptoms resolve or descent (limited to 48-72 hrs)
simple analgesics = ibuprofen or acetaminophen for HA
HA = cardinal smx of AMS
prophylaxis for rapid ascents
<24hr and >3000m or prior Hx of AMS/HAPE/HACE
Acetazolamide 125mg Q12H beginning day before ascent until 48hr after highest altitude reached or descent initiated
s/e = Diarrhea, upset stomach, or throwing up, Change in taste, Decreased appetite, Blurred eyesight, Feeling dizzy, sleepy, tired, or weak, Headache, Flushing, Feeling nervous and excitable
take with food to decrease stomach upset
Dexamethasone 4mg Q12H
high altitude cerebral edema (HACE)
uncommon
is an end stage of AMS and normally occurs within 3 days
most often associated with HAPE
Symptoms = same as AMS (HA, lightheadednes, Anorexia/ loss of appetite, weakness, fatigue) and with what seems like alcohol intoxication (neurological sx):
Ataxia = degenerative disease of NS —> death can occur w/in 24 hrs of development is person fails to descend
changes in mental status
severe headache
high altitude pulmonary edema (HAPE)
not really a progression of AMS! Symptoms can occur on its own
Sx:
Respiratory = dyspnea, cough, congestion
Pulmonary sounds = crackles, wheezing
CV = tachycardia, chest tightness, cyanosis
can be MORE RAPIDLY FATAL THAN HACE!
insect protection
consult public health agency of Canada (PHAC) to evaluate risk of insect-borne illness that are endemic to area
methods of prevention:
Avoidance - 2 types of insects
Aedes = mosquitos active during daytime = dengue fever, zika
Anopheles = mosquitos active during night = malaria
Physical Barriers
use screens around beds and room (permetherin-treated recommended)
screens (<1.5mm) over windows
wear shoes, socks and full clothing during Peak hours
Chemical Barriers
DEET = 30% TID for ADULTS >12y
DEET = 10% TID for children 2-12 yr
DEET = 10% daily for Children 6months - 2yrs
Icaridin = 20% BID for children >6 months
Mosquito net <6 months
malaria
caused by protozoan parasite: Plasmodium genus —> transmitted by mosquitos
5 different species:
P. falciparum - more serious
P. malariae
P. Ovale
P. vivax —> use Primaquine
P. knowlesi
clinical presentation:
flu-like sx = fever, chills, sweating, HA, myalgia
GI sx = Nausea/ vomiting
severe sx of P. falciparum = Jaundice, abnormal bleeding, convulsions (leading to shock, kidney failure, even death)
Risk = endemic to specific regions —> check CDC
prophylaxis:
patient factors:
Pt Hx of malaria prevention
area of travel
other risk factors = Pregnancy, extremes of age and immunocompromised
medication efficacy:
no medication is 100% effective
need to use medications + insect protection measures
resistance patterns:
always check local resistance patterns and patients medications
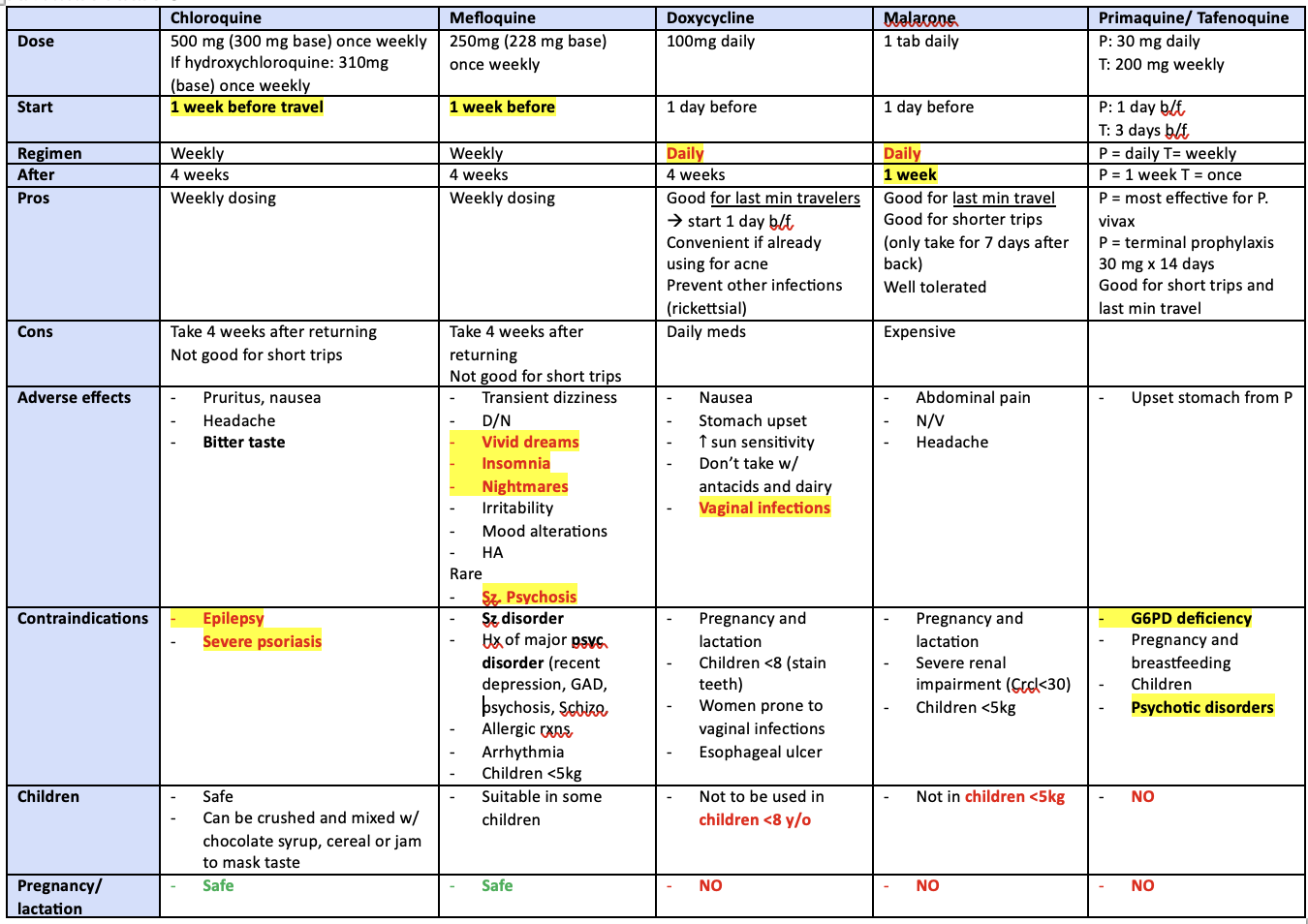
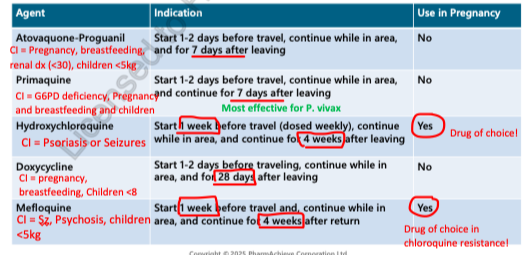
atovaquone proguanil (malarone)
adults = 250/100mg daily
children >5kg = 62.5/25mg —> dosed by weight
take with fatty food (or milk)
directions:
1-2 days BEFORE TRAVEL
DAILY while in risk area and
continue for 7 DAYS after leaving malaria risk area
well tolerated (mild abdominal pain, HA, N/V, insomnia)
Pros:
good for last minute travellers (b/c only need to take 1-2 days before)
good for short trips (only need to take 7 days after travel)
pediatric formulations available
Cons:
More expensive than others
AVOID IN PREGNANCY/ BREASTFEEDING, Children <5kg
AVOID IN RENAL IMPAIRMENT (CrCl<30 ml/min)
primaquine
use in P. vivax endemic areas, PART (presumptive anti-relapse tx) or alternative agent in chloroquine resistant areas
30 mg tab daily
begin 1-2 days BEFORE travel and
continue 7 days after end of trip
s/e = well tolerated (GI upset), methemoglobinemia (Rare), hemolysis with G6PD deficiency
Pros:
good for last min travellers (only need to start 1-2 days before travel)
good for short trips (only require 7 days of post travel treatment)
most effective for P. vivax (drug of choice for this strain)
Cons:
CONTRAINDICATION in severe G6PD deficiency (cost and delays to being tested for this)
AVOID IN PREGNANCY/ BREASTFEEDING and children
gastrointestinal s/e often leads to d/c of therapy —> best taken with food
hydroxychloroquine
useful when heading to area without chloroquine resistance
directions:
start 1 week before entering malaria risk area
take 1 tablet weekly throughout travel and
continue for 4 weeks after leaving malaria risk area
Adults = 400mg weekly
Children = 6.5/kg weekly
s/e = GI upset (nausea, vomiting, abdominal pain), HA, blurred vision, pruritus, dizziness
Administer with food
C/I:
psoriasis
seizures
Pros:
good for long trips (patients only require weekly dose)
safe in pregnancy/ breastfeeding = drug of choice
Cons:
Many endemic areas are known to be chloroquine-resistant
must take medication for 4 weeks post-travel
not good for last min travellers (must be started 1 week before travel)
AVOID IN PT WITH PSORIASIS OR SEIZURES!
Potential caution in those with G6PD deficiency due to risk of hemolytic anemia
doxycycline
100mg
directions:
begin 1-2 days before travelling and
continue for 28 days (4 weeks) after leaving malaria risk area
s/e = photosensitivity, N/V, GI upset, staining of teeth in children and fetuses, candida vaginitis (use fluconazole for self-treatment)
take with food and LOTS OF WATER while remaining upright position to avoid esophageal ulceration
Pros:
good for last minute travellers (only need to start 1-2 days before travel)
least expensive option
Cons:
risks of photosensitivity - use sunscreens to block UV radiation
contraindicated in PREGNANCY, BREASTFEEDING or CHILDREN <8
Must take for 28 days after malaria risk area
Mefloquine
use in areas sensitive to this!
directions:
250mg tab weekly
begin 1 week before travel and
continue for 4 weeks after return
Administer with food and with at least 240 mL of water
1st time users = recommended to start 2-3 weeks before leaving if time permits to assess for s/e
s/e = dizziness, nausea, vomiting, diarrhea, headaches, sinus bradycardia, nightmares, insomnia, mood alteration, anxiety, irritability, Vivid dreams/ nightmares
rare = psychosis and seizures
CI in many Psychiatric disorders (depression, seizures, anxiety)
Pros:
Good for long trips (only need weekly dosing)
can be initiated within 1 week of travel
SAFE in pregnancy (Drug of choice in chloroquine resistant areas)
weight based dosing for pediatrics
Cons:
areas of mefloquine resistance
Avoid in Hx of seizures and psychosis
Must take for 4 weeks after travel
known to have severe side effects leading to discontinuation
malaria prophylaxis summary
dengue fever
acute febrile illness caused by virus transmitted by Aedes mosquitos
prevention is key = use insect repellent and wear tight clothing
most common symptom = fever with GI sx, rash (2 days after fever) or aches/pains (joint pain)
sx begins 4-7 days after exposure
can develop severe dengue
supportive care
chikungunya
spread by Aedes mosquito
vaccine available
prevention is key = use insect repellents and wear tight clothing
most common sx = fever and joint pain
clinical presentation = HA, rash, Joint pain (can persist for years causing chronic disability), sx begin 3-12 days after exposure
mimics dengue fever
supportive care = acetaminophen for fever and muscle pain, rest and fluids
zika virus
caused by Aedes mosquito
no specific treatment or vaccine
can be passed from pregnant woman to fetus
pregnant women should avoid areas endemic to this
Avoid conception x 2 months (woman traveled to high risk/ outbreak areas) after leaving affected area
clinical presentation = fever, rash, joint pain, can cause microencephalopathy and congenital brain abnormalities in fetus
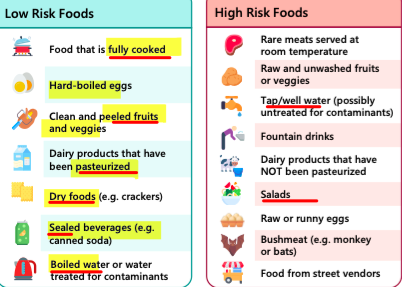
water and food safety
risk of neglecting recommendations = travelers diarrhea
education is important —> esp in Pregnant, young, old and immunocompromised
always boil, cook and peel food
drinking unsafe or untreated water —> exposure to harmful pathogens (cholera, E. coli, Typhoid) —> high risk of disease (cholera, typhoid fever) and symptoms (diarrhea, fever)
Boiling water = MOST RELIABLE and preferred method!
Iodination = recommended only for short term (< 2 weeks) if unable to boil
CI in pregnant women and children or thyroid disease patients
tincture of 2% iodine (5 drops/L) then let stand for 30 mins
chorine bleach = LEAST RELIABLE —> 2 drops chorine household bleach to 1 L water and let sit for 30 mins
thrombosis prevention
risk during long flights and following the flight
anyone travelling >4 hrs by air, car or bus = at risk of blood clot
Patients with Hx of DVT/PE due to flying will need an evaluation by physician regarding anticoagulant therapy for flights >2 hrs
risk factors:
duration of travel (8 hrs has strongest association)
previous patient risks (VTE, cancer, pregnancy, age, surgery, injury, clotting)
meds = oral contraceptives, HRT
immobility on fight
greatest risk first 2 weeks after travel, then slowly back to baseline by 8 weeks
non-pharm:
Avoid alcohol
contract muscles in calves regularly or get up often to walk around (every 1-2 hrs)
below knee compression stockings = not routinely recommended for those with no risk factors (recommended for long distance travellers at increased risk of VTE)
avoid constrictive clothing
thrombosis prevention medications
ASA does NOT reduce risk of travel related blood clots
LMWH or DOACs = recommended after physician assessment for long distance travel with baseline risk factors for VTE
if no increased risk for VTE: prophylactic anticoagulants not recommended
if already on prophylactic or treatment anticoagulant or antiplatelet = no additional treatment needed
jet lag
clinical presentation:
Malaise
Fatigue
Disruption of sleep-wake cycles
Irritability and impaired cognitive abilities
travelling eastward = more severe than westward
takes 1 day for every hr of time difference to acclimatize
Non-pharm:
adjust sleep patterns to destination prior to departure
stay well hydrated during flight —> avoid alcohol, large meals
remain active during flight by stretching, walking )also helps to stay awake to adjust to new time zone)
Pharm:
Melatonin = made by the body at nighttime by pineal gland to assist body with sleep
effective in reducing symptoms
dosing = 3-5 mg QHS —> IR formulation is most effective
take at first night after arrival (before nocturnal sleep in new time zone)
s/e = abdominal cramps, dizziness, HA, irritability, drowsiness