Chapter 7 - Understanding & Managing Pain
1/58
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
59 Terms
Physiology of Pain
What parts of the body are involved in experiencing pain? (BSS)
Brain
Spinal Cord
Somatosensory System
Somatosensory System
What it does?
Contains…
Conveys sensory info from the body to brain
Contains
Afferent neurons
Efferent neurons
Interneurons
Afferent Neurons
Sensory neurons — relay info from sense organs → brain
Efferent neurons
Motor neurons — result in the movement of muscles / stimulation of organs or glands
Interneurons
Connect sensory to motor neurons
Nociception
What is it?
What are nociceptors?
Nociception—process of perceiving pain
Nociceptors—receptors in skin + organs; responds to stimulation that may cause tissue damage
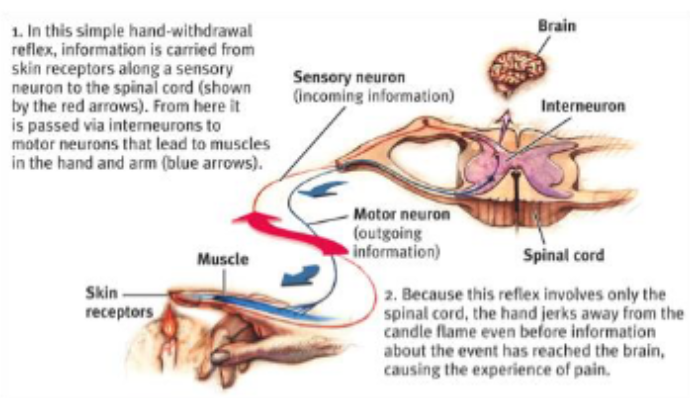
Spinal Cord
Avenue for sensory info—travels toward brain & motor info comes from it
Provides spinal reflexes—react w/o processing it
Process
Somatosensory Cortex
slide 8
Motor cortex
Sensory cortex
The Experience of Pain
Pain is a s— experience & e— experience
Sensory experience—-somatosensory cortex tells you where it is + how strong it is
Emotional experience—insula cortex & anterior cingulate cortex tell you how much it bothers, annoys, or disturbs you
Main Theories of Pain
Specificity Theory
Gate Control Theory
Neuromatrix Theory
Specificity Theory
What?
Pain is the result of — — — —
Experience of pain is approximately = to amount of tissue damage/bodily injury
Pain is the result of transmission of specific signals
Henry Beecher
Who?
Found what?
Anesthesiologist for soldiers in WWII
Found that despite serious battle injuries, many of men reported very little pain
Henry Beecher found that
Phantom Limb Pain
What is it?
Reported by…
Why does it occur?
What: Sensation of pain from a limb that has been lost; person no longer receives physical signals
Who: Reported from amputees / quadriplegics
Why? Even when limb is amputated → brain represents limb in somatosensory cortex
Bottom-up processes vs. Top-down processes
Bottom-up—afferent neurons send messages to spinal cord + brain
Top-down—brain & spinal cord decides how messages from the afferent neurons affect the brain
Gate Control Theory
Psychological influences are manifested in the brain may influence the experience of pain
During a war or sports victory, the brain sends messages closing the gate
Gate Control Theory
What controls the gate?
The amount of activity in the pain fibers
Messages from the brain
Gate control theory
What opens the gate?
Physical
Cognitive
Emotional
Physical
Extent of injury
Inappropriate activity level
Cognitive
Focus on the pain
Boredom
Emotional
Anxiety, worry
Depression; anger
Gate control theory
What closes the gate?
Physical
Cognitive
Emotional
Physical
Meds
Heat, massage
Pressure
Cognitive
Distraction
Concentration
Emotional
Relaxation
Positive emotions
Affect influences chronic pain by…
Ex: arthiritis
People with arthirits who’s more depressed &/or anxious → more pain
Neuromatrix Theory
An extension of — theory
What?
Melzack’s extension of gate control theory
How different parts of the brain are involved in the increasing / decreasing experience of pain
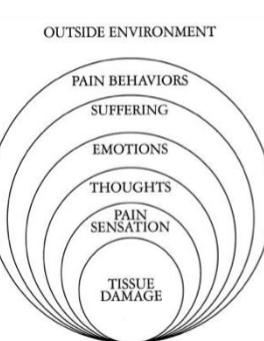
What can affect experience of pain?
Unpleasantness
Multiple people with the same pain stimulus → all would rate it differently in terms of unpleasantness
What can affect experience of pain?
Context of Pain
Same person had same stimulus (pos/neg) at different times → pain experience ↗ when you find out something about negative stimulus vs positive stimulus
What can affect experience of pain?
Influences on Pain
Classifying Pain
Acute Pain
Adaptive; lasts short
Ex: pain from cuts, burns, & other physical trauma
Typically soft tissue damage, infection, and/or inflammation among other causes
slide 28
Chronic Pain
Longer than normal healing; constant
Often reinforced by other people + becomes self-perpetuating
Typically w/ capable older adults
slide 29
Can trigger psychological problems
Defined as “disease of pain”
Features of Chronic Pain
Persists long after healing
May spread + increase in intensity
May become stronger than initial pain from injury
Chronic Pain Conditions
Arthritis
Migraine headaches
Lower back pain
Fibromyalgia
Arthritis
Pain caused by inflammation in the joints
Migraine
Recurrent, throbbing, very painful headaches
Lower back pain
Chronic low back
Pre-chronic Pain
Experienced B/T acute & chronic pain; critical
Pain can either go away or turn into chronic pain
Lower Back Pain
What contributes to it?
Lead to…
Only —% have identified cause
What:
Infections
Degenerative disease
Cancer (rare)
Injury / physical stress
Lead to
Musculoskeletal
Ligament
Neurological problems
Only 20% have identified cause
Fibromyalgia
slide 33
Cancer Pain
slide 34
Measurement of Pain
Types of Measures
Self-report
Behavioral assessment
Physiological measures
Self-report
Visual Analogue Scale
Pain intensity—from somatosensory
Pain unpleasantness—from insula; anterior cingulate cortex
Visual Analogue Scale—place mark on line to indicate how much pain you are feeling
Distance from left is measured for pain score
Behavioral assessment
What do you do?
What to look for?
Good for..
Watch to see if they exhibit pain behaviors
Guarded movement
Bracing
Position shifts
Partial movement
Grimacing
Limitation statements
Emitting pain sounds
Good for kids + older adults
Physiological measurement
Tried to do muscle tension + autonomic NS response
But, don’t show sufficient reliability / validity
Medical Professionals typically…
Underestimate pain of patients
May prescribe / administer too little pain meds
Why may doctors prescribe / administer too little pain meds?
Fear of addiction to opiate drugs
Treatment of Pain
— drugs are the most common treatment for acute pain
Drugs fall into 2 groups:
Analgesic drugs are most common treatment for acute pain
2 groups:
Opiates
Nonnarcotic analgesics
Opiates
Powerful analgesic effects, but also produce tolerance & dependence
Fear of addiction typically under-prescribed → may harm pain recovery
Why has there been an increase in prescription of analgesic drugs?
Would oxycontin lead to less / more active coping w/ pain?
Demand of oxycodone (oxycontin) & hydrocodone
More active coping
NSAIDS
Useful for..
Examples:
Useful for managing minor pain, especially pain due to injury
Ex:
Ibuprofen (Advil)
Naproxen (Aleve)
Aspirin
Too much ibuprofen causes..
Organ damage
ibuprofen → kidneys
Tylenol → liver
Surgical Intervention
slide 48
Treatment of Pain
slide 49
Behavioral & Cognitive Interventions
Slide 50
Progressive Muscle Relaxation
Why do some people still experience pain
slide 52 reinforcement of pain
Behavior Modification
slide 53
Progression
slide 54