Venous thromboembolism
1/20
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
21 Terms
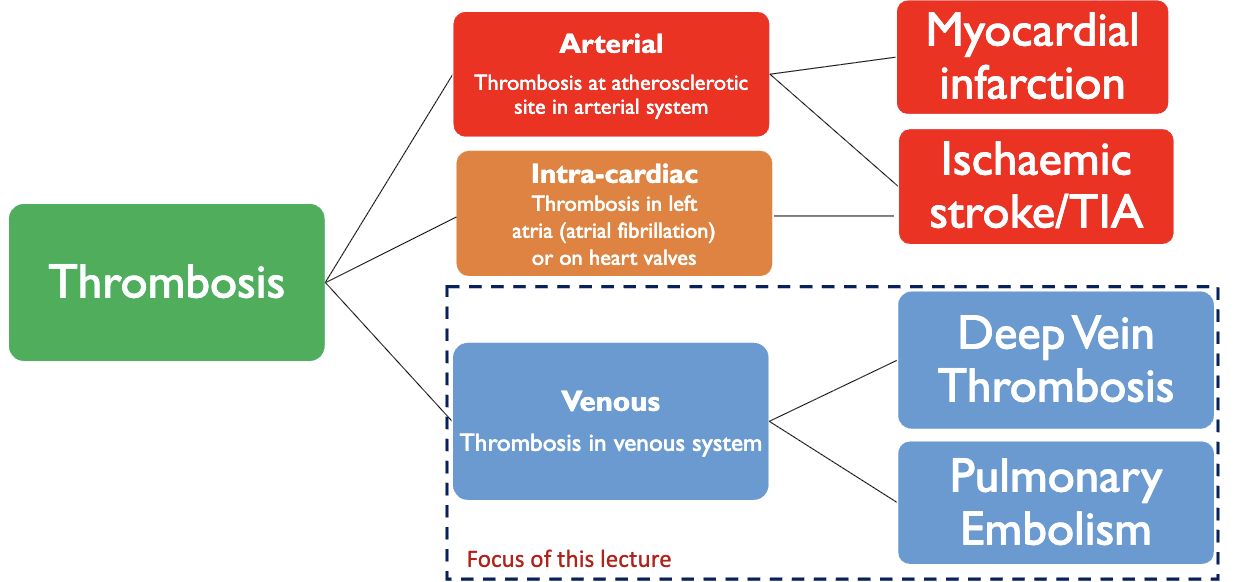
what is thrombosis
unwanted formation of a blood clot (thrombus), which can be arterial (in arterial system) or venous (in venous system)
management approaches will differ depending on the location of the thrombus
what is arterial thrombus and venous thrombus
arterial: composed of white thrombus, rich in platelets, leukocytes and fibrin
venous: composed of red thrombus, has a small head and jelly-like tail
what is an embolism
when a blood clot (thrombus) breaks away from its original site and travels elsewhere in the body
travelling blood clot = embolus
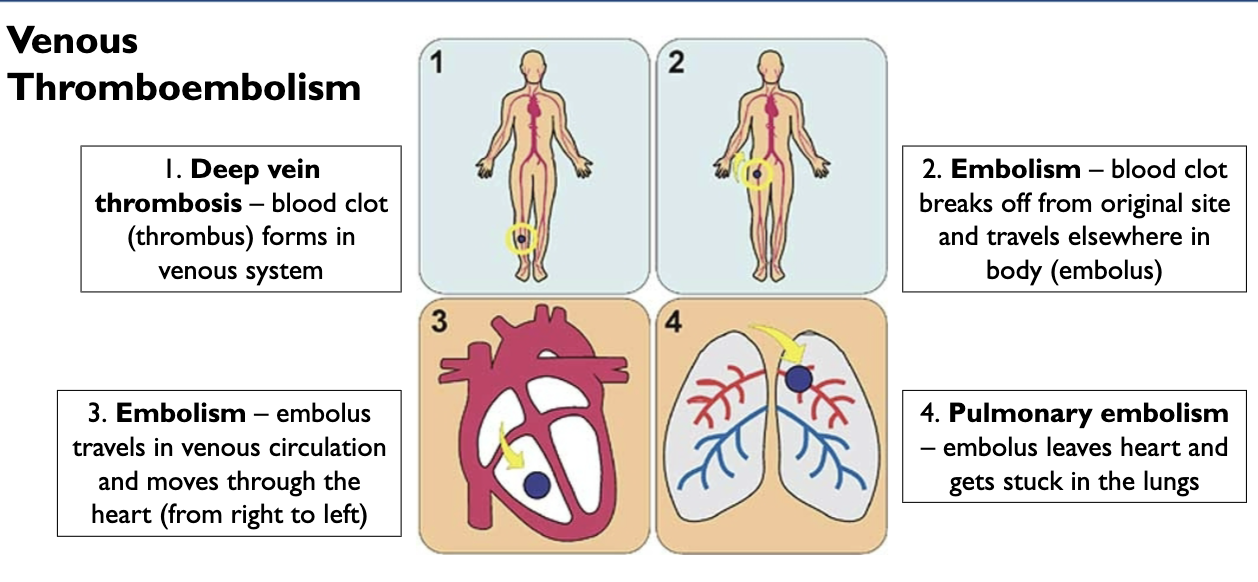
what is a venous thromboembolism
a blood clot (thrombus) that forms in the vein
if the thrombus breaks off, the embolus can travel to the lungs → pulmonary embolism
what is arterial thrombosis
thrombosis that occurs in arteries with fatty plaque → atherosclerotic site in the arterial system
compromised blood flow and oxygen in the artery → myocardial infarction or ischaemic stroke/TIA
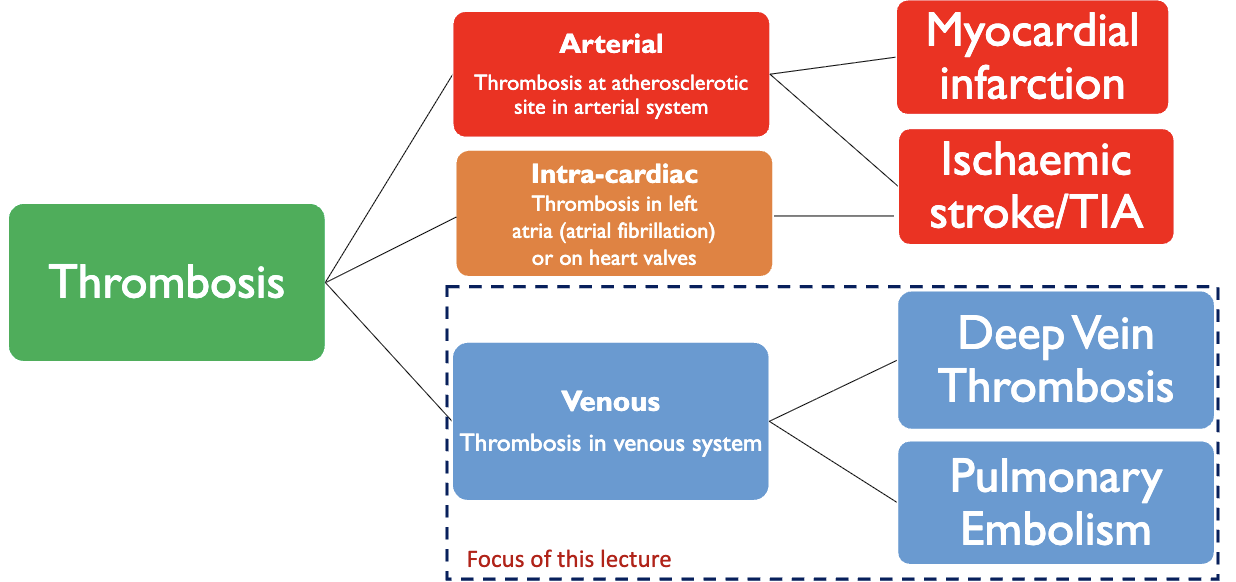
what is intra-cardiac thrombosis
thrombosis in the left atria or the heart valves
thrombus in heart can break off and move to other parts of the body, often to the brain, → ischaemic stroke/TIA
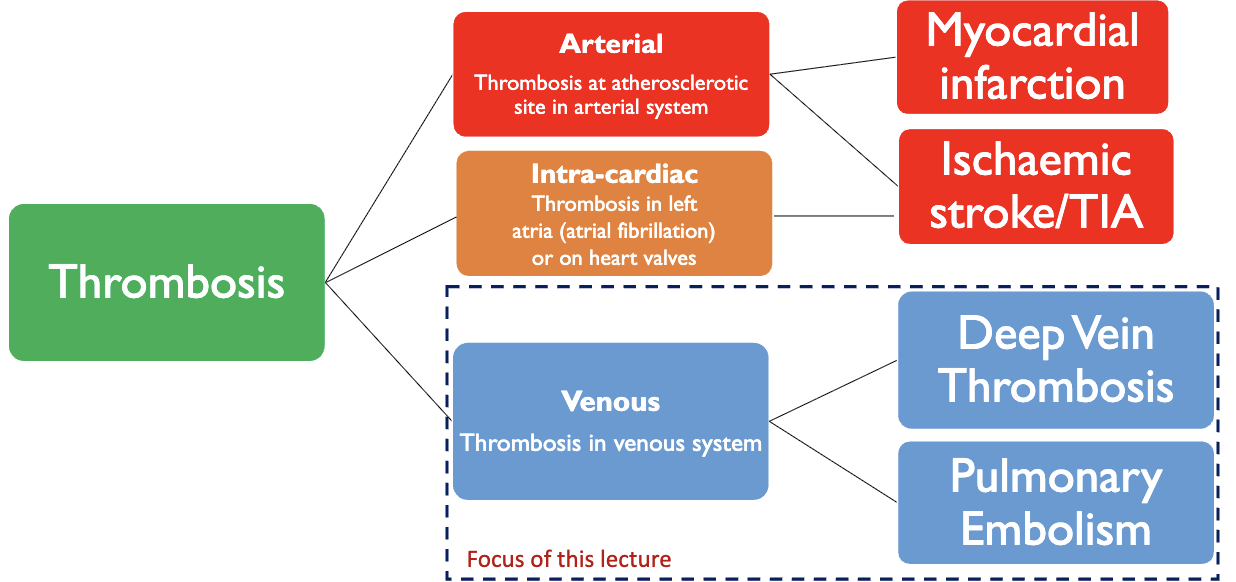
what is venous thrombosis
thrombosis in the venous system
original site is normally a vein in a leg → deep vein thrombosis
can break off and travel (embolus), normally to the lungs → pulmonary embolism
summary of venous thromboembolism
what is arterial thrombosis treated with and why
antiplatelets
thrombus in atherosclerotic site of an artery (in either one of the coronary arteries or in the brain) → fatty plaque rupture → platelet activation and aggregation
what is venous thrombosis treated with and why
anticoagulants
thrombus in venous site → inappropriate activation of the clotting cascade (platelets aren’t as involved)
the thrombus that is formed have high fibrin and low platelet content
what is Virchow’s triad
the factors that he said contribute to thrombosis
venous stasis (slow bood flow )
hypercoagulability (blood has an increased tendency to clot inappropriately)
vessel-wall injury
what are the risk factors for VTE
previous history of DVT or PE
previous myocardial infarction
previous stroke
cancer
thrombophilia (blood has increased tendency to clot)
immobility
recent surgery (specifically pelvic region or legs)
obesity
pregnancy
hormone replacement therapy
what are the signs and symptoms of DVT
unilateral leg pain (only one leg)
swelling
tenderness
increased pressure
pitting oedema (swelling where pressure leaves a visible dent)
how is DVT diagnosed
Doppler ultrasound → looks at blood flow abnormalities in the leg
D-Dimer blood test → detects D-Dimer, which suggests a blood clot
how are D-Dimer fragments caused
the blood clot is comprised mainly of fibrin, which holds it together
an enzyme called plasmin breaks the fibrin strands at both ends of the strand to produce two D units (D-Dimer fragments)
presence of D-Dimer fragments not only suggest presence of a blood clot, as well as breakdown of the blood clot
what are the signs and symptoms of PE
dyspnoea (shortness of breath)
chest pain
dizziness, light-headedness
tachycardia (HR more than 100bpm)
tachypnoea (rapid breathing)
haemoptysis (coughing blood)
what are the diagnostic tests for PE
computed tomography pulmonary angiogram (CTPA) → taking a picture of the vessels between the heart and lungs)
D-Dimer blood test
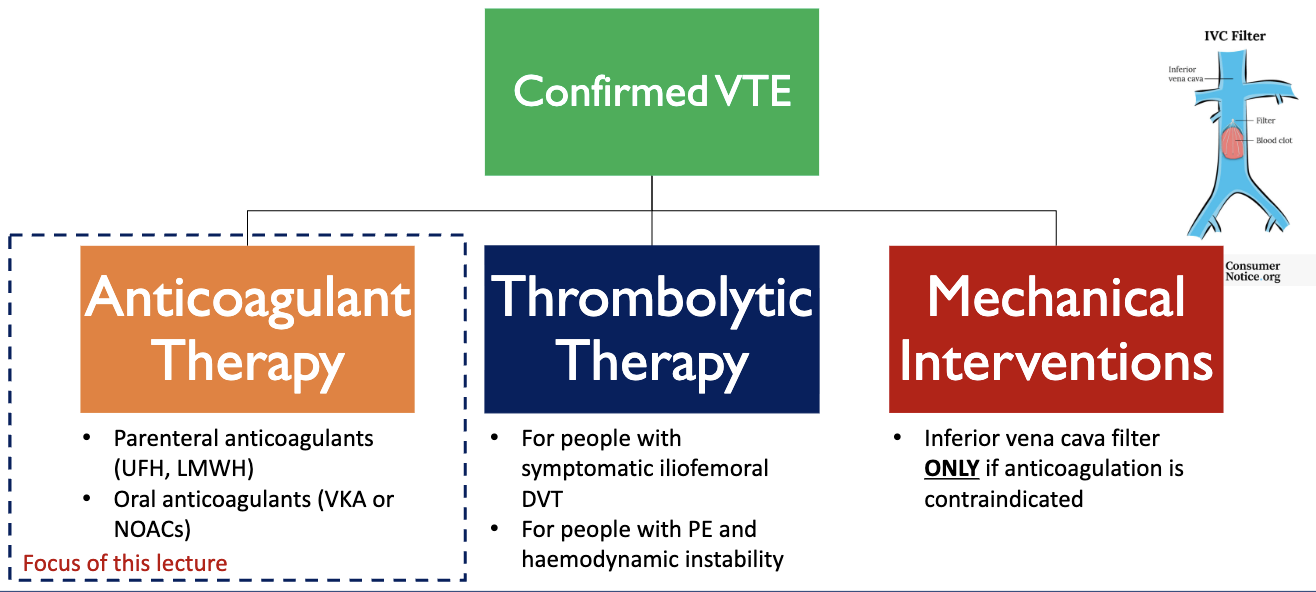
what are the different treatment options for confirmed VTE
anticoagulant therapy
parenteral anticoagulants → unfractionated heparin (UFH) or low-molecular weight heparin (LMWH)
oral anticoagulants → vitamin K antagonists (VKA) or non-vitamin K oral anticoagulants (NOAC/DOAC)
thrombolytic therapy
for people with symptomatic iliofemoral DVT → clot formed in the iliac femoral vein
for people with PE and haemodynamic instability (concerning changes in BP or HR → higher risk of tissue perfusion issues)
mechanical interventions
insert inferior vena cava filter if anticoagulation is contraindicated
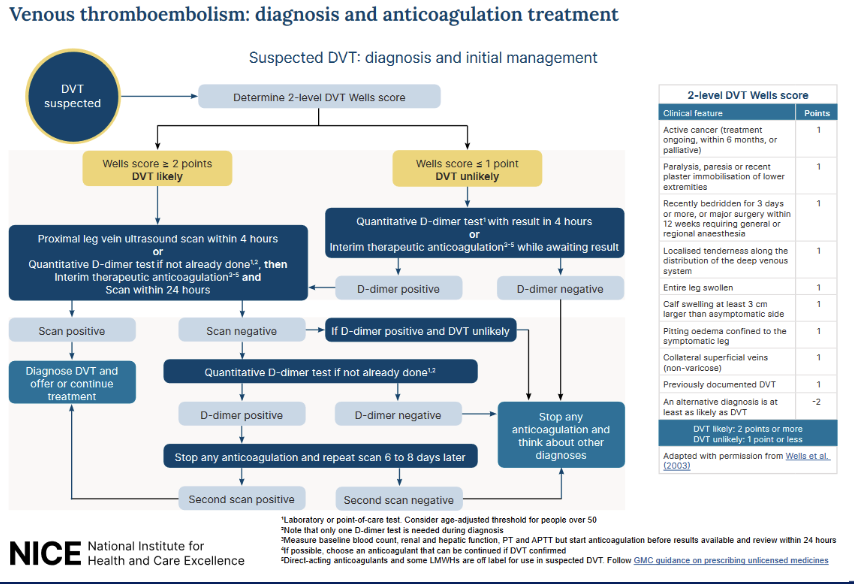
NICE guidelines for diagnosing DVT
when person presents with symptoms, we take a clinical history and examination → start parenteral coagulation (LMWH) as it can get out of the system quickly if diagnosis is wrong
2-level DVT well score is then calculated to confirm a diagnosis
a well score of 1 or less means DVT is unlikely → D-Dimer test done
negative test rules out a DVT and anticoagulation therapy is stopped
positive test → doppler ultrasound scan will be needed
a well score of 2 or more means DVT is likely → doppler ultrasound is done within 4 hours
if it can’t be within 4 hours, D-Dimer test is done → scan is still done but within 24 hrs
positive scan → confirmed diagnosis
negative scan → look at D-Dimer test results
if D-Dimer result is positive but the scan is negative → possibility of a DVT, but can’t be ruled out completely → stop anticoagulation + repeat the scan 6-8 days later
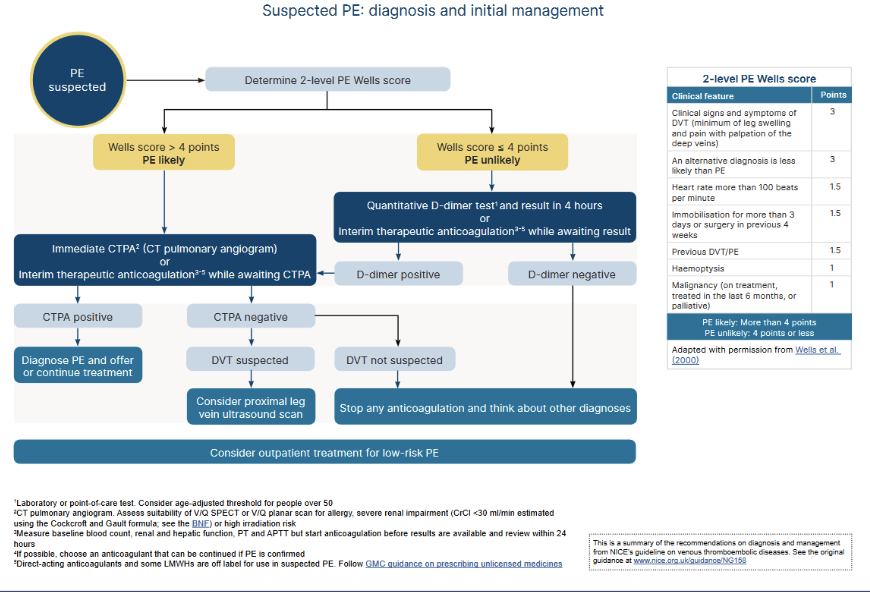
NICE guidelines for diagnosing PE
when person presents with symptoms → start parenteral coagulation
2-level PE well score is then calculated to confirm a diagnosis
a well score of 4 or less → means PE is unlikely → D-Dimer test
negative test rules out PE and anticoagulation therapy is stopped
positive test → CT pulmonary angiogram will be needed
a well score of 4 or more means PE is likely → CT pulmonary angiogram is done immediately
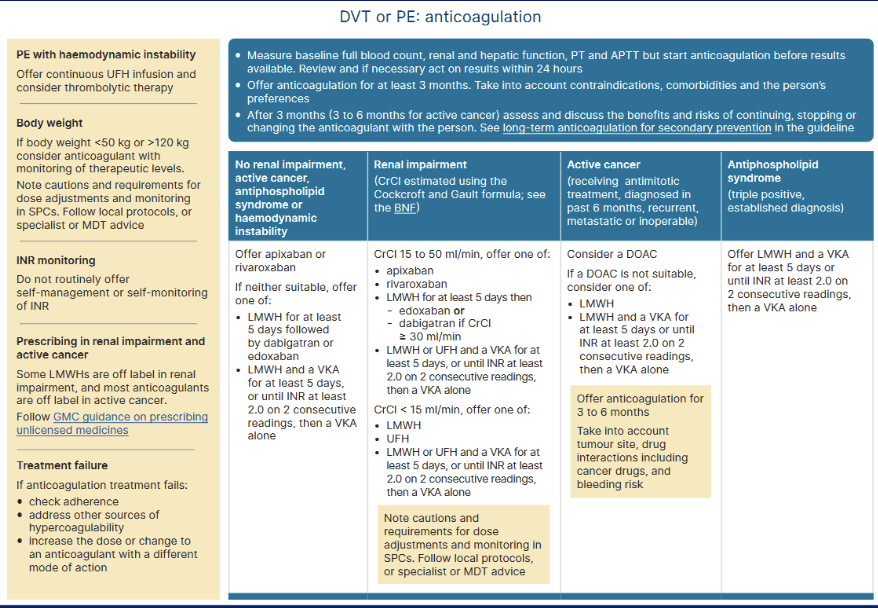
VTE management in different patient groups where long-term oral anticoagulation is needed after being discharged from hospital
assess whether they show any signs of high bleeding risk e.g. anaemia, blood clotting disorders
full blood count
renal function and hepatic function
Prothrombin Time and Activated Partial Thromboplastin Time
first line treatment are usually DOACs e.g. apixaban
they have greater acceptability with people
don’t require monitoring of INR
less interactions with other medicines and food
only one blood test is needed
monitoring is done annually
DOACs are contraindicated in people with antiphospholipid syndrome as it leads to a higher occurrence of thrombotic events → use parenteral anticoagulant or VKA with warfarin
DOACs have different requirements e.g. to adjust dose depending on weight/renal function/age, to take at meal times etc