Acid Secretion and Peptic Ulcer Disease
1/31
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
32 Terms
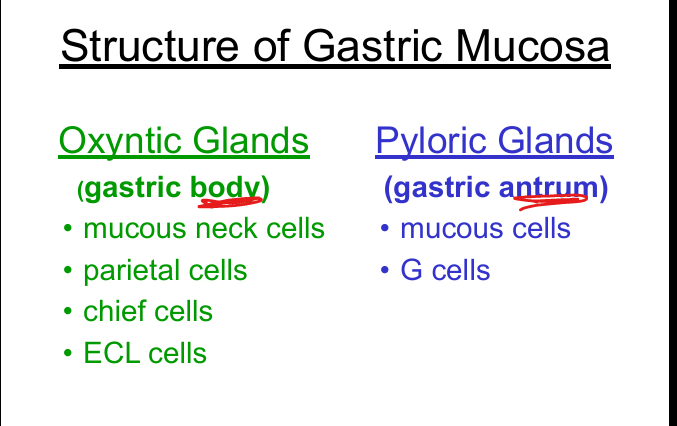
Gastric regions and major cell types
Fundus/Body: mucous neck cells, parietal cells, chief cells, ECL cells; Gastric Antrum: mucous cells, G cells.
Function of parietal cells
Secrete HCl (kills microbes, activates pepsin) and intrinsic factor (B12 absorption).
Function of chief cells
Secrete pepsinogen → activated to pepsin by HCl; proteolysis.
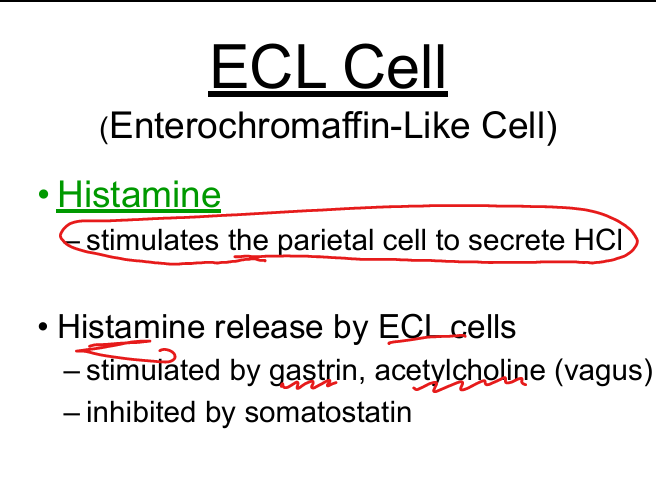
Function of ECL cells
Release histamine → stimulates parietal cells to secrete HCl.
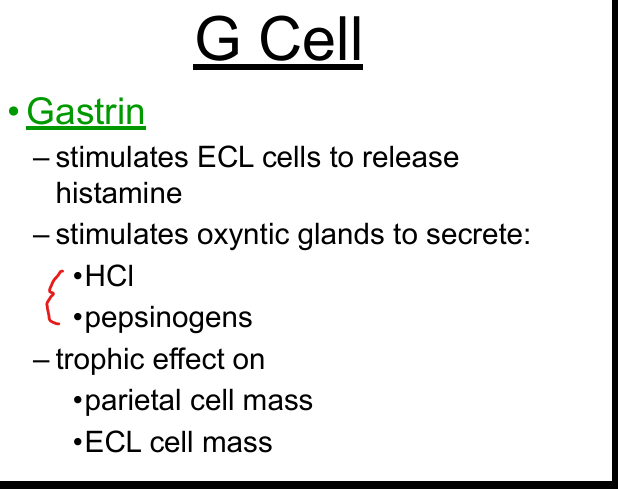
Function of G cells
Release gastrin → ↑ acid, ↑ pepsinogen, ↑ ECL histamine, trophic effect on parietal/ECL cells.
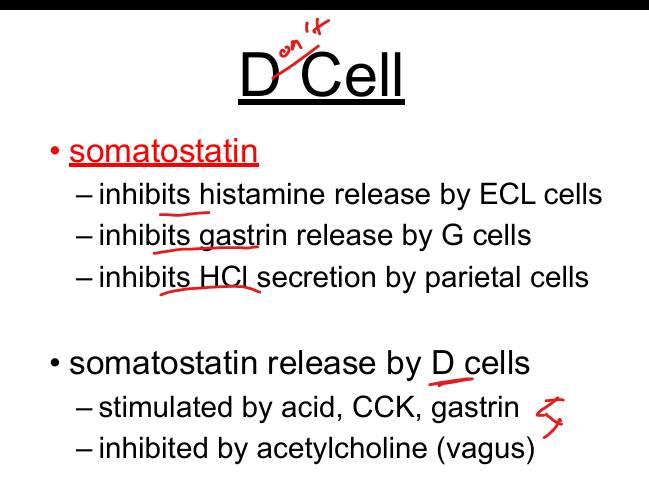
Function of D cells
Release somatostatin → inhibits gastrin, histamine, and parietal cell acid secretion.
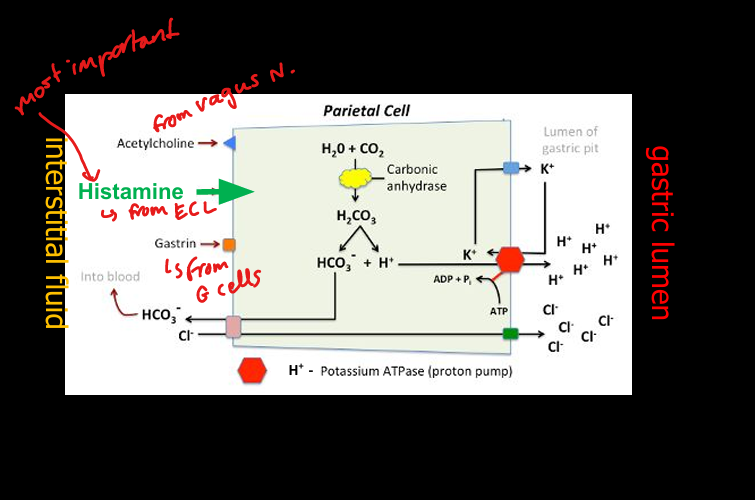
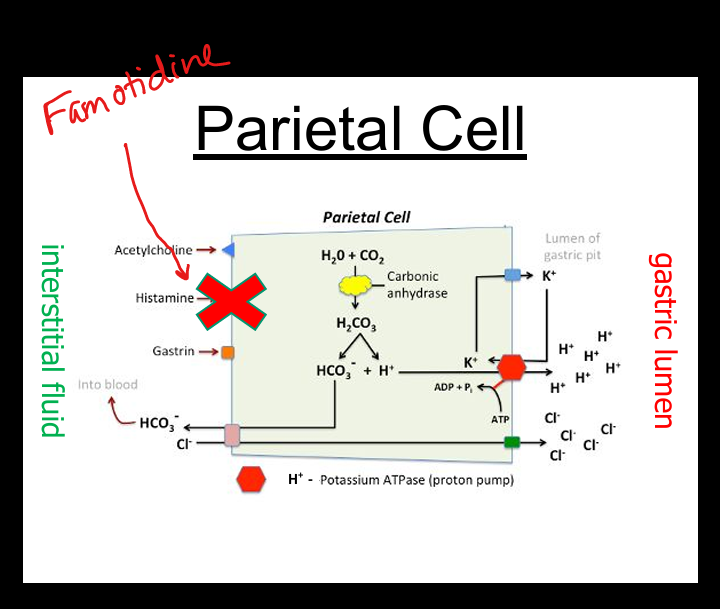
Mechanism of acid secretion (parietal cell)
Carbonic anhydrase forms H+; H+/K+ ATPase pumps H+ into lumen; Cl– follows; HCO3– enters blood (“alkaline tide”).
Stimulators of acid secretion
Histamine (H2 receptor), gastrin, acetylcholine (vagus).
Inhibitors of acid secretion
Somatostatin, prostaglandins, secretin, low gastric pH.
Cephalic phase of acid secretion
Sight/smell/taste → vagus → ↑ ACh, ↑ gastrin, ↑ histamine; inhibits D cells.
Gastric phase of acid secretion
Gastric distention (vagovagal reflex) + peptides → ↑ gastrin.
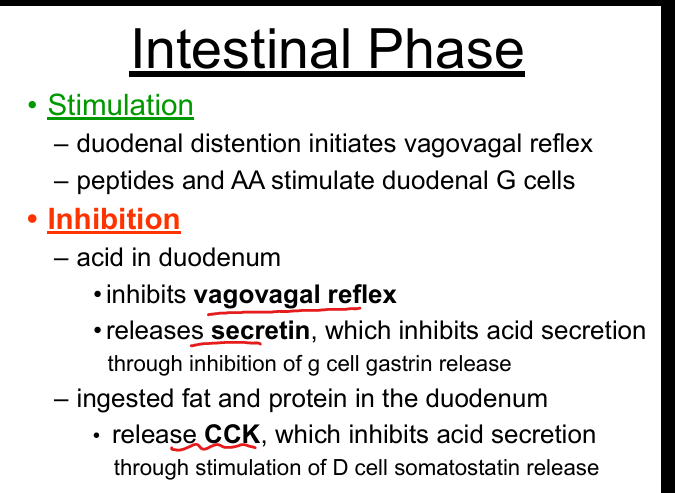
Intestinal phase of acid secretion
Peptides stimulate duodenal G cells; acid/fat inhibit via secretin + CCK → ↑ somatostatin.
Mucosal protective factors
Mucus, bicarbonate, epithelial barrier, prostaglandins, mucosal blood flow.
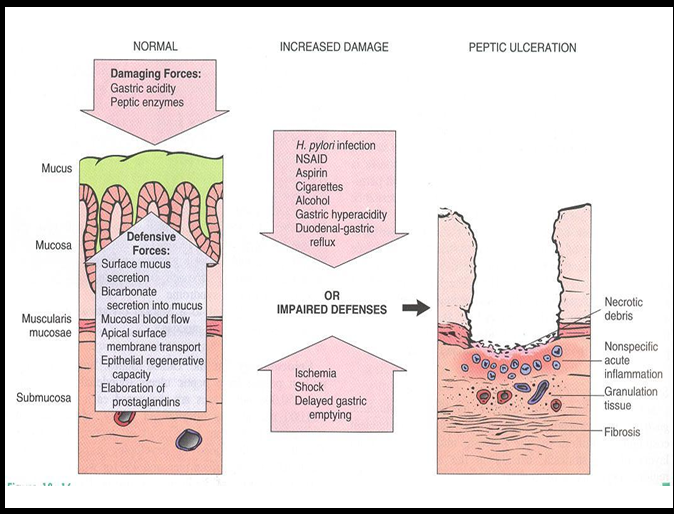
Damaging factors of mucosal lining
Acid, pepsin, H. pylori, NSAIDs, smoking, alcohol, stress, bile reflux.
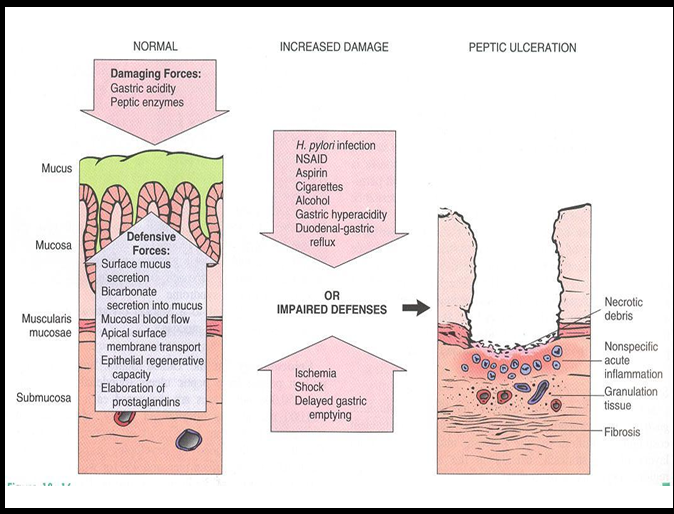
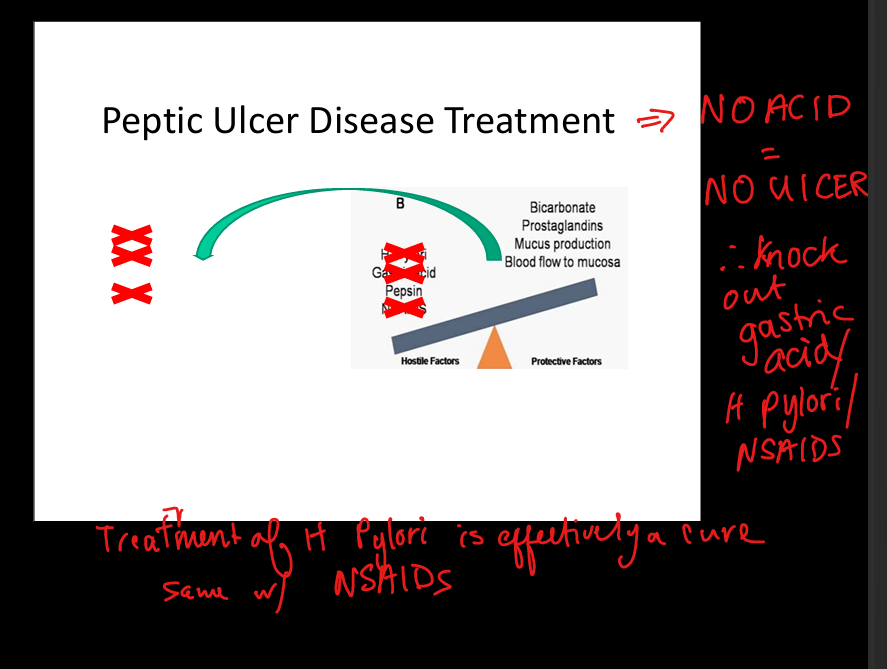
Pathogenesis of Peptic Ulcer Disease
Imbalance between acid/pepsin and mucosal defenses → ulceration.
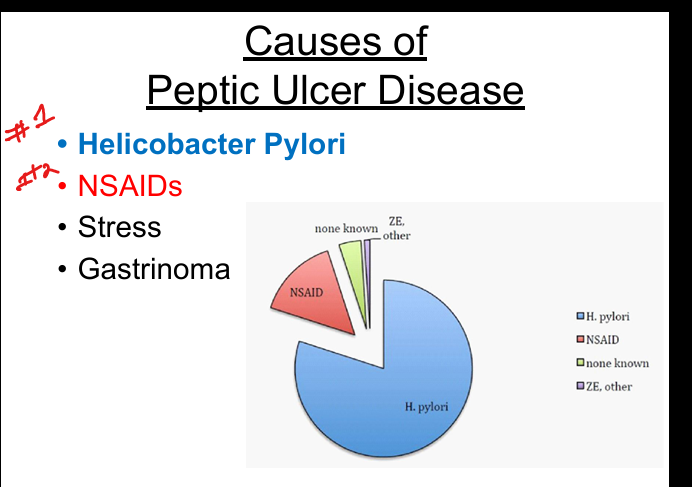
Major causes of Peptic Ulcer Disease
H. pylori (#1), NSAIDs, stress (critical illness), gastrinoma (ZE syndrome).
H. pylori characteristics
Gram‑negative rod; urease‑producing(produces ammonia which neutralizes acid); lives in mucus layer; causes chronic gastritis.
H. pylori complications
Peptic ulcers, gastric adenocarcinoma, MALT lymphoma.
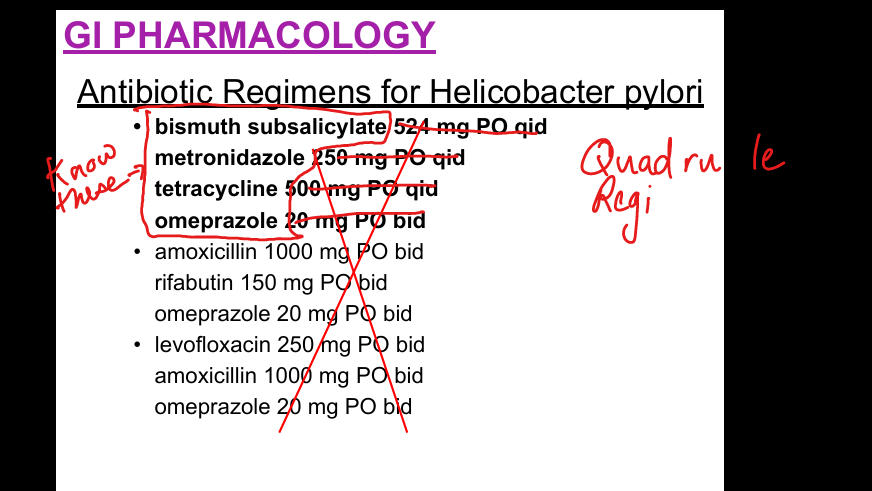
Meds to treat H Pylori
Bismuth Subsalicylate, Metronidazole, Tetracycline, Omepraziole = Quadrupule regimen
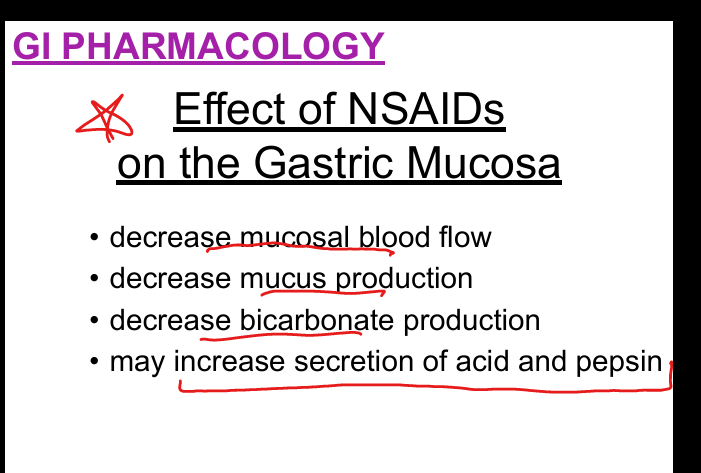
NSAID mechanism of injury in Peptic Ulcer Disease
COX‑1 inhibition → ↓ prostaglandins → ↓ mucus, ↓ bicarbonate, ↓ blood flow → ↑ acid injury.
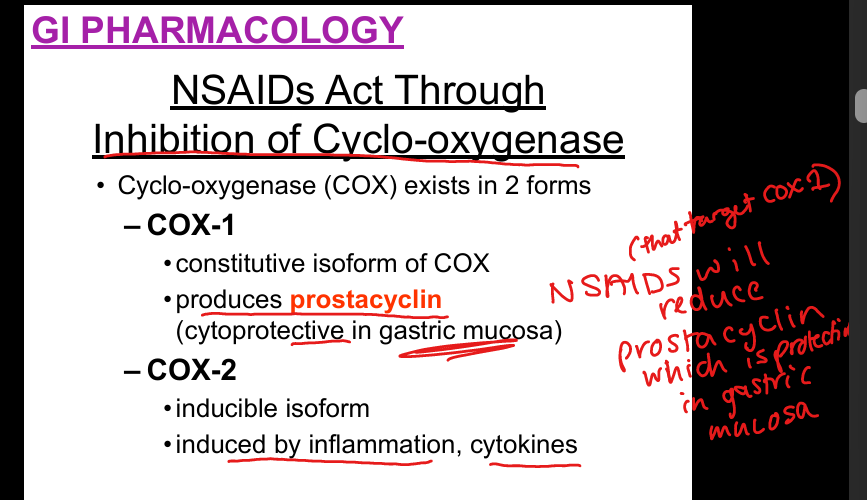
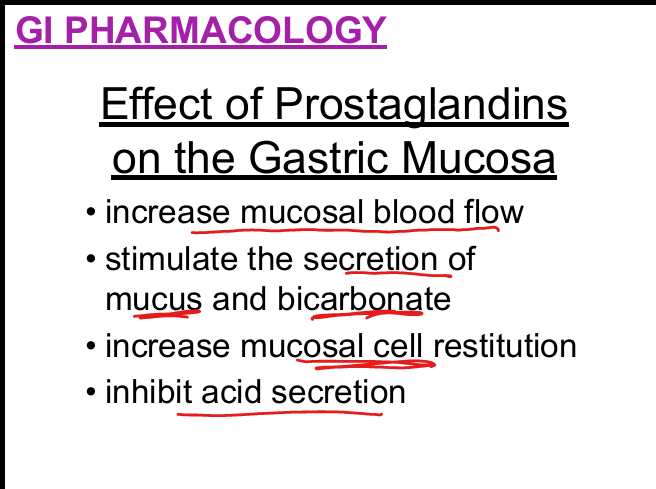
Prostaglandin protective effects
↑ mucus, ↑ bicarbonate, ↑ blood flow, ↑ epithelial repair, ↓ acid secretion.
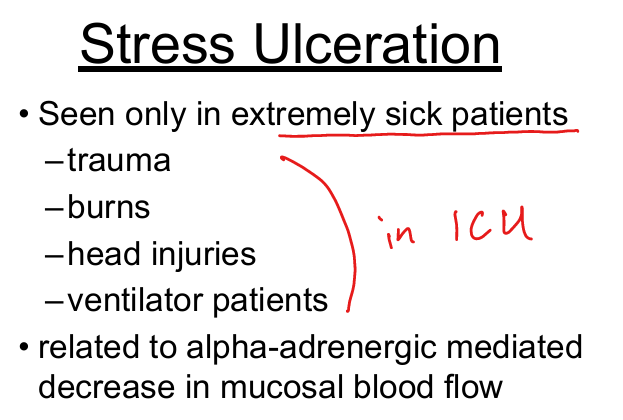
Stress ulcers
Seen in critically ill (trauma, burns, head injury, ventilated); due to ↓ mucosal blood flow.
Complications of Peptic Ulcer Disease
Bleeding, perforation, gastric outlet obstruction, pain.
Treatment principle for Peptic Ulcer Disease
NO ACID = NO ULCER; eliminate H. pylori; stop NSAIDs; reduce acid; enhance mucosal protection.
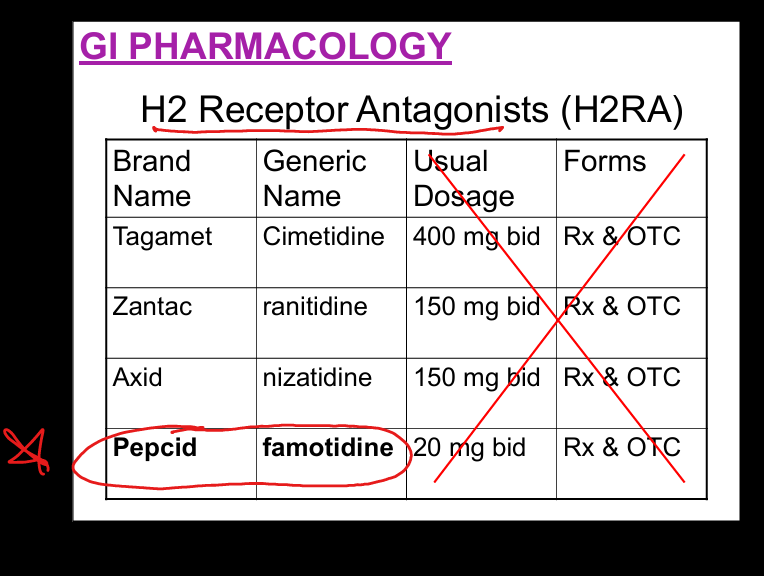
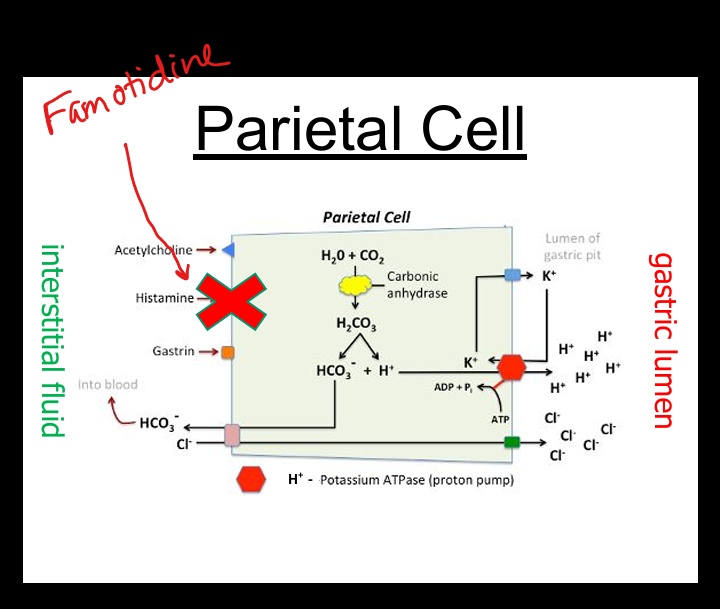
H2 blockers mechanism + Example
Block H2 receptors on parietal cells → ↓ histamine‑stimulated acid secretion. Famotidine(Pepcid)
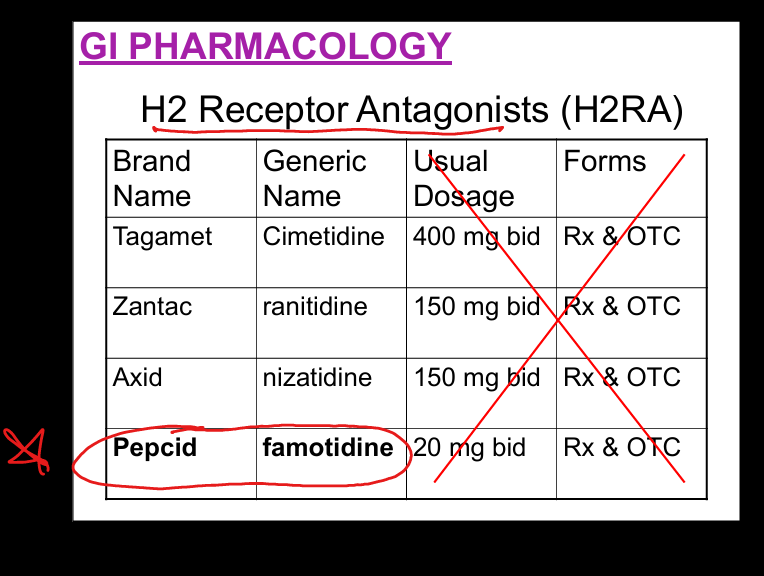
Famotidine (Pepcid) moa
H2 Receptor Antagonist on parietal cells»decreases histamine stimulated acid secretion
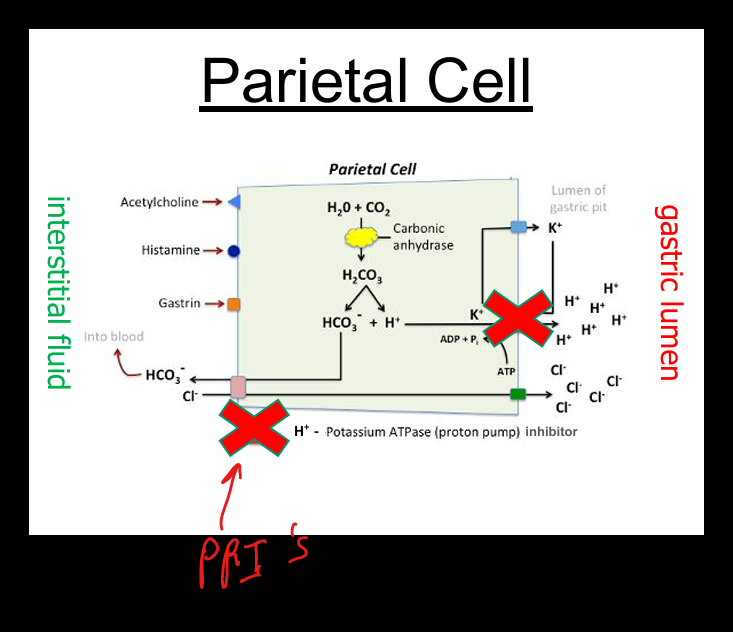
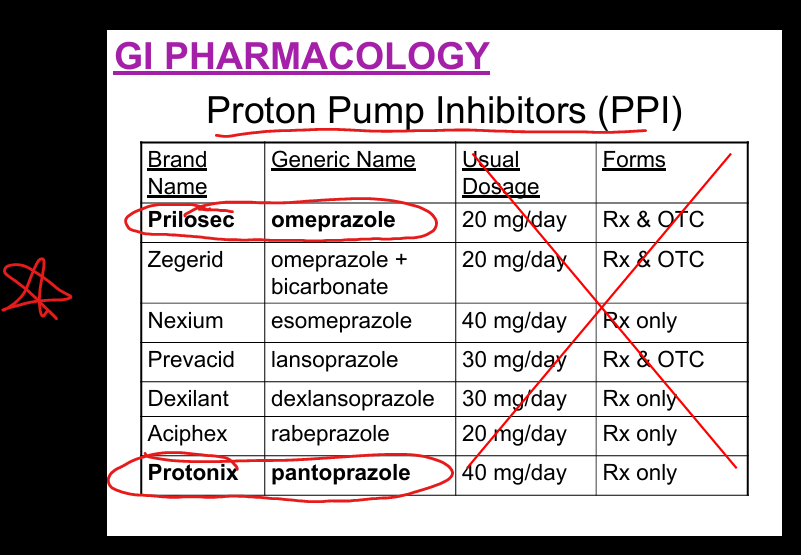
PPI mechanism
Irreversibly inhibit H+/K+ ATPase → block final step of acid secretion.
Examples of PPIs
Omeprazole(Prilosec), esomeprazole, pantoprazole(Protonix), lansoprazole, rabeprazole, dexlansoprazole.
Long‑term PPI risks
Low‑quality evidence: kidney disease, fractures, infections, B12 deficiency; absolute risk very low.
Mucosal protectants: sucralfate (Carafate)
Forms protective coating on ulcers; binds proteins; inhibits pepsin.
Mucosal protectants: misoprostol (Cytotec)
prostaglandin analog → ↑ mucus/bicarbonate, ↓ acid; contraindicated in pregnancy (abortifacient).
Acid reduction interventions
Anticholinergics, vagotomy, H2 blockers, antrectomy, PPIs.