Patho exam 1
1/52
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
53 Terms
genotype
the coding
phenotype
the expression
heterozygous alleles
when two DIFFERENT alleles are inherited
Homozygous allele
When two IDENTICAL alleles are inherited
Types of Chromosome aberrations
Euploidy
polyploidy
Aneyploidy
Euploidy
Cells with “NORMAL” amounts of cells
both gametes and diploid cells are present
Polyploidy
Presence of more than 2 complete sets of chromosomes
Aneuyploidy
Gain or loss of one or more individual chromosomes
Down Syndrome
Abnormality of chromosome number 21
trisomy 21
needs clinical diagnosis
manifestations
low nasal bridge, epicanthal folds, protruding tongue, low set ears
intellectual disability (Avg. IQ 20-70)
Incidence rises with increasing age
Turner Syndrome
Single X Chromosome (X) → Female
Characteristics:
short stature
wide chest
lymphedema
infertility
multiple moles
Klinefelter Syndrome
Extra X Chromosome (XXY) → male
Characteristics:
longer legs
broader hips
gynecomastia
reduced body hair
small testes
reduced muscle mass
infertility
Epigenetics
the study of changes in gene functions that are heritable and that are not attributed to alterations in the DNA sequence itself
→ explores how behavior and environmental factors can switch genes on or off—adjusting how cells read genetic coding
Can be affected by:
nutrition
toxins, pollutants, and radiation
lifestyle
DNA Methylation
Methyl groups attaches to DNA strand → cells are unable to read this portion of DNA
this can be a good AND bad thing
(ex. parts of the sheet music are blank)
Methylation of BRCA 1 and 2 can lead to breast, ovarian, and prostate cancer
Histone Modification
Chemical changed (Methyl groups) occur on histones, preventing unraveling
(ex. You can’t open the music book)
Innate Immunity
Defense mechanisms that are present at birth and provide the initial response to invasion and injury
first line of defense against actual or potential invaders
primary cellular components of innate immunity
mast cells
platelets
neutrophils
basophils
monocytes/macrophages
dendritic cells
Mast cells
Found in connective tissue and close to vessels in skin, GI, and respiratory tract linings
Release histamine
Platelets
Aggregates to help stop bleeding; degranulation releases serotonin to accelerate inflammation
Neutrophils
primary phagocyte in early inflammation which phagocytizes pathogens and removes cellular debris and dead cells from lesions
Basophils
least prevalent granulocyte
contains heparin
release histamine
particularly involved in adaptive immune response, esp. w/ asthma or allergies
monocyte/macrophage
largest WBC
migrates to inflammation and transforms into macrophage
responds to presence of chemical mediators
cleanup and repair crew
dendritic cells
consumes invaders
presents “remnants” to Helper T cells
promotes activation of adaptive immunity
immunity pathway
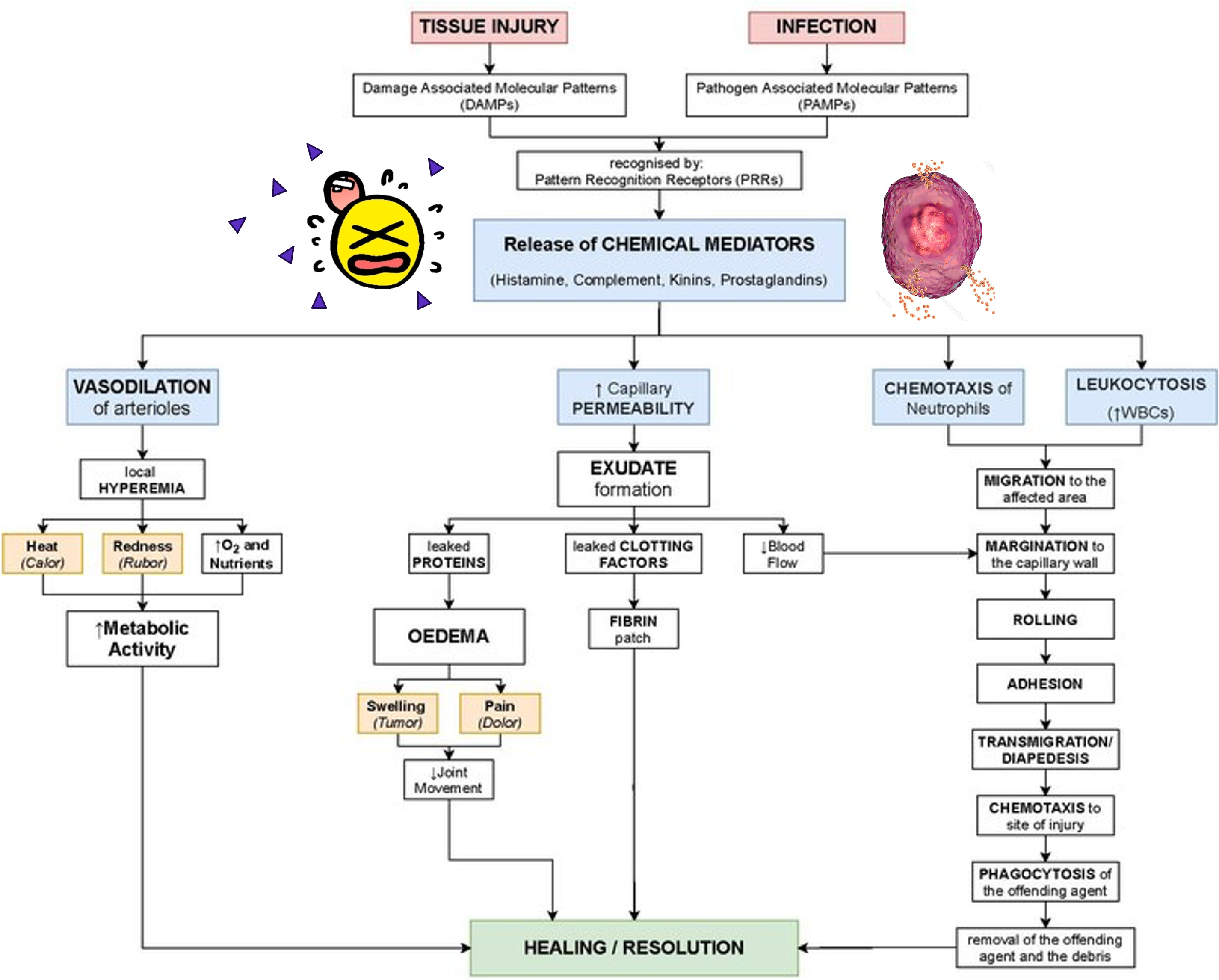
Symptoms of Local Inflammation
Rubor → Redness
Calor → Heat
Tumor → Swelling
Dolor → Pain
Functio Leasa → Loss of Function
Symptoms of Systemic Inflammation
Fever
Increased WBC count → Check CBC
Increased synthesis of plasma proteins → Check ESR and CPR
4 Phases of Wound Healing
Hemostasis
Inflammation
Proliferation and New Tissue Formation
Remodeling and Maturation
Hemostasis
Phase 1
Damage leads to vasoconstriction then vasodilation and clotting cascade
fibrin mesh of blood clot acts as a scaffold
*Primary goal is to keep blood in and invaders out
Inflammation
Phase 2
Begins in minutes
Involves macrophages, mast cells, neutrophils, and lymphocytes
Phagocytosis
*Primary goal is to catch and eliminate invaders present and clearing debris
Proliferation and New Tissue Formation
Phase 3
Begins 3-4 days after injury
Angiogenesis
Fibroblast activation
Granulation tissue formation
*Primary goal is to begin rebuilding what has been lost/damaged
Remodeling and Maturation
Phase 4
Begins weeks after injury
Re-epithelialization
Scar formation
Wound contraction
*Primary goal is to strengthen and reorganize the newly formed tissue
Swelling
results from increased capillary permeability and fluid movement into the tissues
histamine released → inc vasucular permeability
inc capillary hydrostatic pressure → pushes fluid into tissues
dec. oncotic pressure → proteins accumulate in tissues
Osmotic Forces
Pulling force → pulling of fluids and solutes from one side to the other
Na, K, Glucose
Oncotic Forces
Pulling force → pulling of proteins/maintaining levels in blood volume
plasma proteins
Hydrostatic forces
pushing force → pushes water out through semipermeable membrane
maintains fluid pressure (BP)
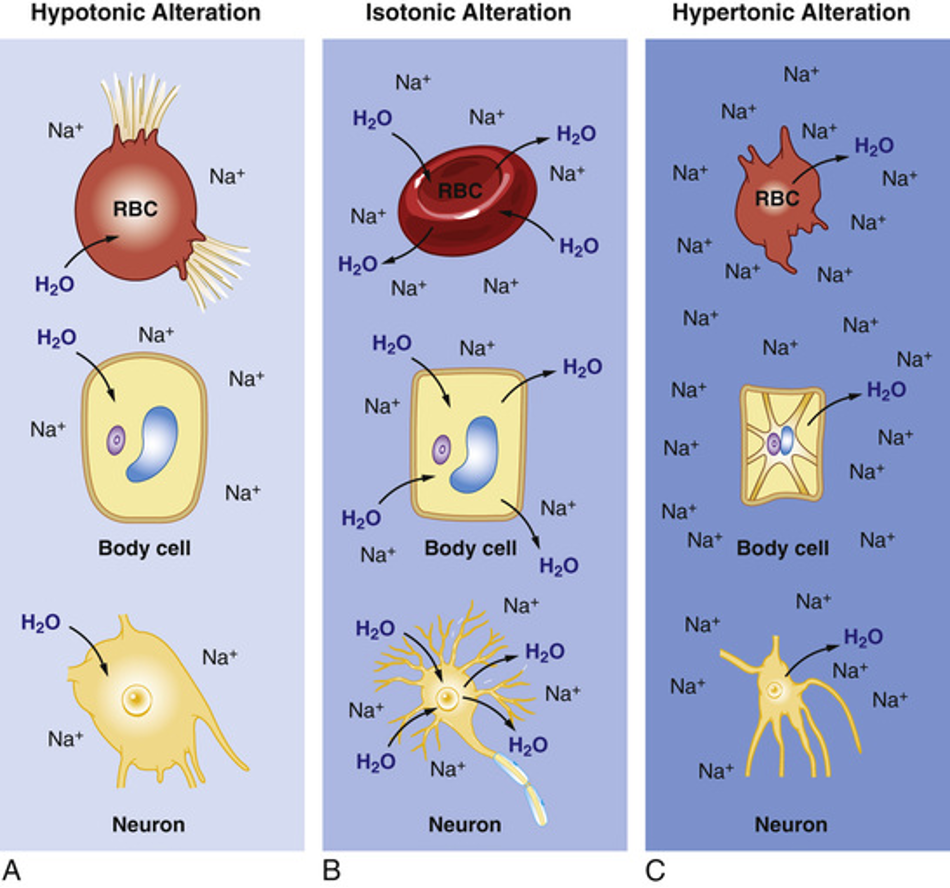
Fluid alterations
Isotonic alteration: fluid is shifting equally/everywhere → equal sodium everywhere
Hypotonic alteration: low sodium in bloodstream and increased water → lost osmotic pulling force
hypertonic alteration: too much sodium in bloodstream and water is leaving cells → massive osmotic pulling force
Isotonic imbalance
TBW loss equivalent to electrolyte loss
leads to hypovolemia (too little plasma volume)
Manifestations
dec. U/O
dec. BP, elevated HR
dry mucous membranes and skin
SEVERE loss = shock
elevated hematocrit
Isotonic fluid gains/excess (plasma volume increase)
Causes:
too much IV fluids
aldosterone hypersecretion
drug effect
Manifestations
hypertension
edema → hydrostatic forces altered
dyspnea (pulmonary edema)
hypertonic imbalance
Water loss or solute gain
osmolality is high
causes
isovolemic hypernatremia (only water lost)
severe diarrhea
inadaquate water intake
respiratory tract infections
Hypovolemic (lots of water lost, some sodium lost)
loop diuretics, mannitol
renal failure
Hypervolemic hypernatremia (lots of sodium and water lost)
rare → endocrine disfunction
inc. Na intake along with kidney disease
Cells shrink
hypotonic imbalances
water gain or solute loss
osmolality is low (diluted)
causes
isovolemic hyponatremia (only Na lost)
SIADH
hypothyroidism
hypovolemic hyponatremia (lots of Na lost, some water lost)
severe diarrhea
prolonged vomiting
hypervolemic hyponatermia (inc. Na leads to water retention)
CHF
cirrhosis of liver
significant edema
cells swell
Hypernatremia
Too much sodium (Na > 145 mEq/L )
Manifestations:
Flushed skin
Restless
Inc. BP and HR
Edema
Dec. U/O
Seizures
Anxious
Low-grade fever
Thirst
(FRIED SALT)
Hyponatremia
too little sodium (Na < 135 mEq/L)
Manifestations:
Stupor/coma
Anorexia
Lethargy
Tendon reflex dec.
Limp muscles
Orthostatic hypotension
Seizures
Stomach cramping
(SALT LOSS)
Hypokalemia
Too little potassium (K < 3.5 mEq/L)
Manifestations:
Lethargy
Leg cramps
Limp muscles
Low, shallow breaths
Lethal cardiac arrythmias
Lots of urine
(6 L’s)
Hyperkalemia
Too much potassium (K > 5.0 mEq/L)
Manifestations:
Muscle weakness
Urine abnormalities
Restless nerves
Diarrhea
EKG changes
Reflexes
(MURDER)
Hypocalcemia
Too little calcium (Ca < 5.5 mg/dL)
Manifestations
Chvostek’s sign
Arrhythmias
Trousseau’s sign
Spasms
(CATS)
Hypercalcemia
Too much calcium (Ca > 10.5 mg/dL)
Manifestations
Stones → kidney stones
Bones → bone pain, osteoporosis, fractures
Groans → abdominal pain, N/V, constipation
Psych Moans → depression, anxiety, confusion
Hypomagnesemia
Too little magnesium ( Mg < 1.8 Mg/dL)
Manifestations
Chvostek’s signs
Refractory hypokalemia
Arrhythmias
Muscle spasms
Paresthesias
Seizures
(CRAMPS)
Hypermagnesemia
too much magnesium (Mg > 2.8 mg/dL)
Manifestations
Sedation
Loss of reflexes
Unresponsiveness
General weakness
Gait problems
Impaired breathing
Slow heart rate
Hypotension
(SLUGGISH)
ABG
Arterial blood gases
Normal pH: Acidic ← 7.35-7.45 → Basic
—> typically 7.4
Normal CO2: Basic ← 35-45 → Acidic
Normal HCO3: Acidic ← 22-26 → Basic
Compensation
Is the pH in a normal range → compensated
Are either CO2 of HCO3 in normal range → uncompensated
Is the value that doesn’t match the pH in the opposite range → partially compensated
Control of serum pH
Resp system alters CO2 levels → fast
Kidneys alter HCO3 levels → slow
respiratory acidosis
lungs fail to get rid of CO2 → CO2 climbs → carbonic acid climbs → acidosis
Causes:
pneumonia, airway obstruction, chest injury
drugs that depress the respiratory center
COPD → chronic resp. acidosis
severe impairment or lack of compensation → decomp. resp. acidosis
Metabolic acidosis
causes
diarrhea → excessive HCO3 loss
inc use of serum bicarb
renal disease or failure → dec. excretion and produciton
decomp. metabolic acidosis
Respiratory alkalosis
drop in CO2
Causes
hyperventilation
anxiety, high fever, overdose
head injury
brainstem tumors
Metabolic alkalosis
increase in serum bicarb
Causes
loss of hydrochloric acid
hypokalemia
excessive ingestion of antacids