D520 Lec3 Tooth Structure & Developing of the Caries
1/76
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
77 Terms
Which of these are dental caries?
All of them are caries, caries are NOT just big holes in the teeth

What is a characteristic feature about the color of enamel?
it is actually TRANSLUCENT, the yellowish-white color we see in the mouth is actually the color of dentin
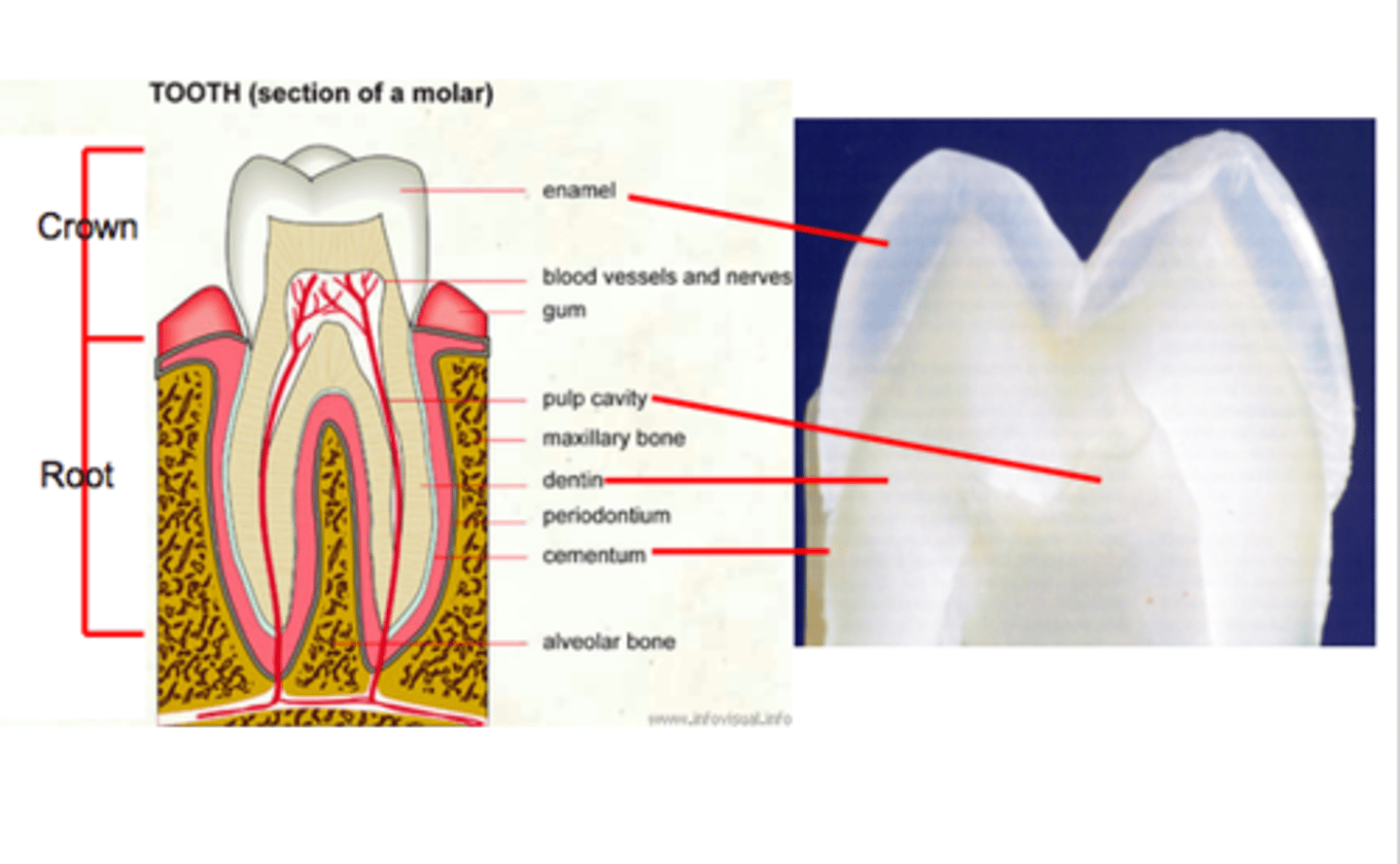
Clinical crown
Clinical crown is that part of the tooth that is visible in the oral cavity.
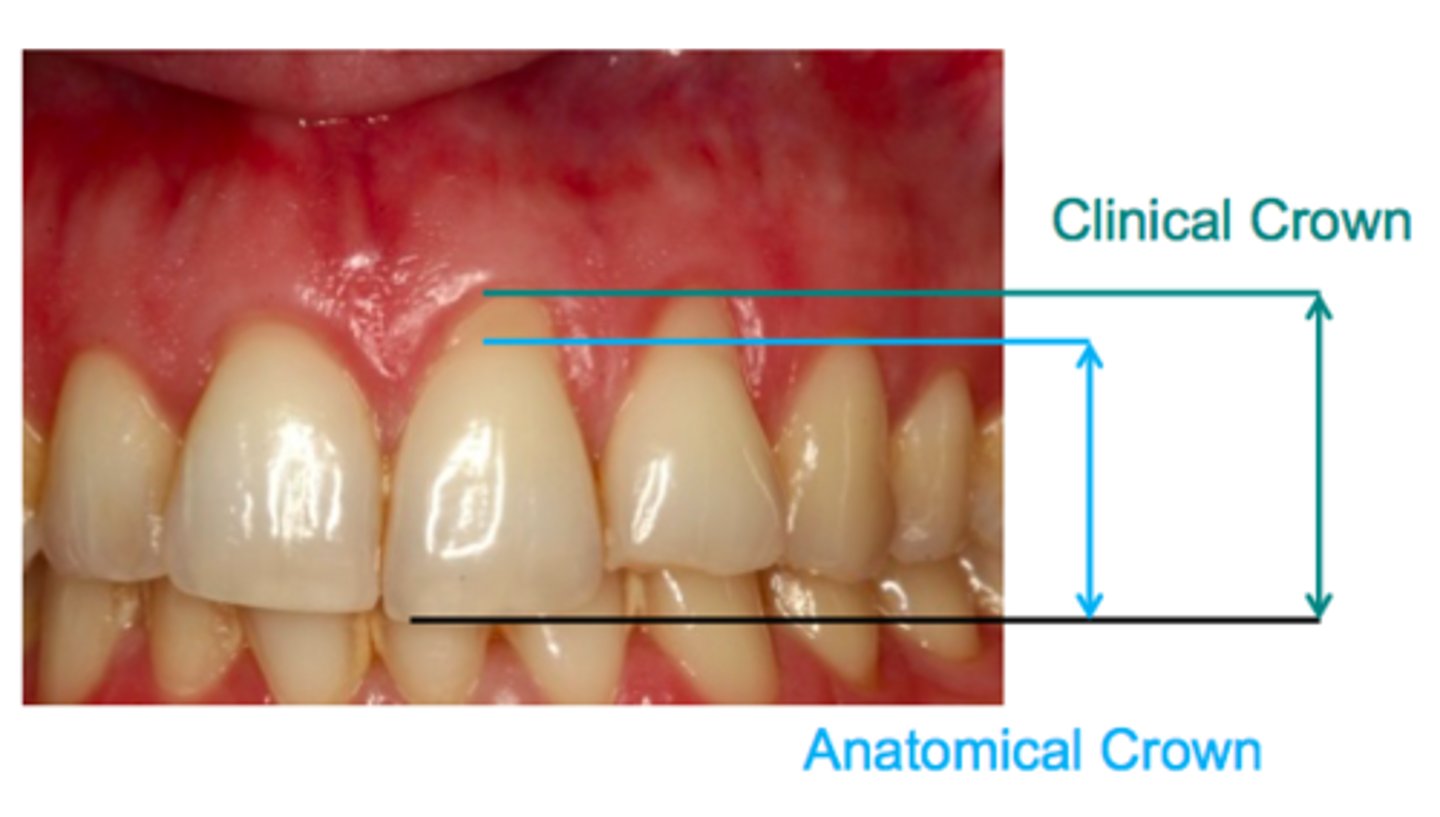
Anatomical crown
Anatomical crown is that part of the tooth that is covered by Enamel or outer covering of the tooth. Its up to the cemento-enamel junction.
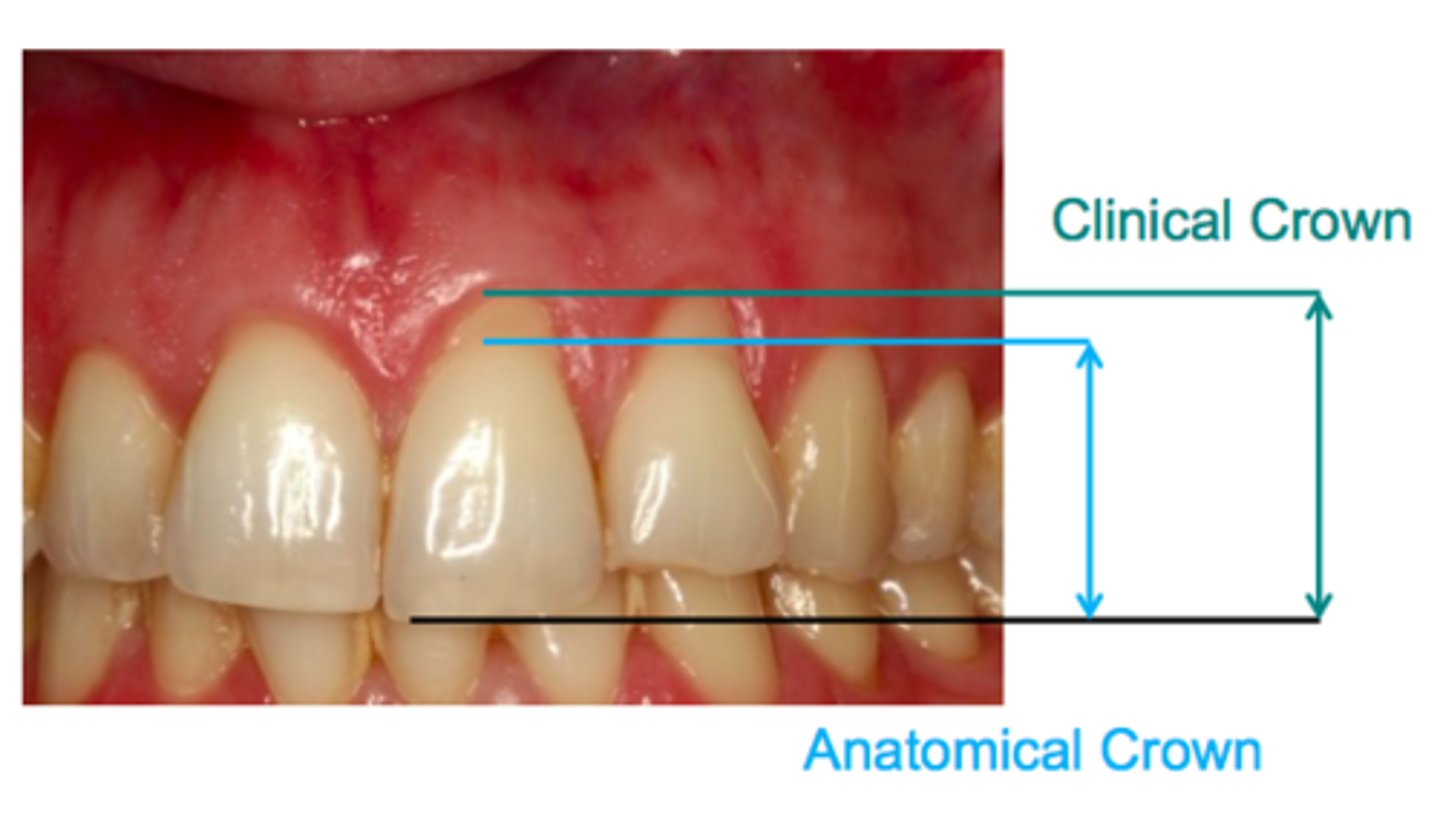
How would the clinical crown and anatomical crown be situated in a healthy individual?
the anatomical crown and clinical crown would be the SAME in a healthy individual
What does ENAMEL consist of by volume?
The enamel consists of:
85% by volume is INORGANIC (HYDROXYAPATITE), 12% by volume is WATER and 3% by volume is PROTEIN.
What does ENAMEL consist of by weight?
95% by weight is inorganic (hydroxyapatite), 4% by weight is water and 1% by weight is protein.
What is the basic unit of enamel?
the ENAMEL ROD (enamel prism)
Enamel rod
a tightly packed, highly organized mass of hydroxyapatite crystals
Hydroxyapatite
Ca10(PO4)6(OH)2
How long and wide is an enamel rod?
is 4 μm long and 8 μm high
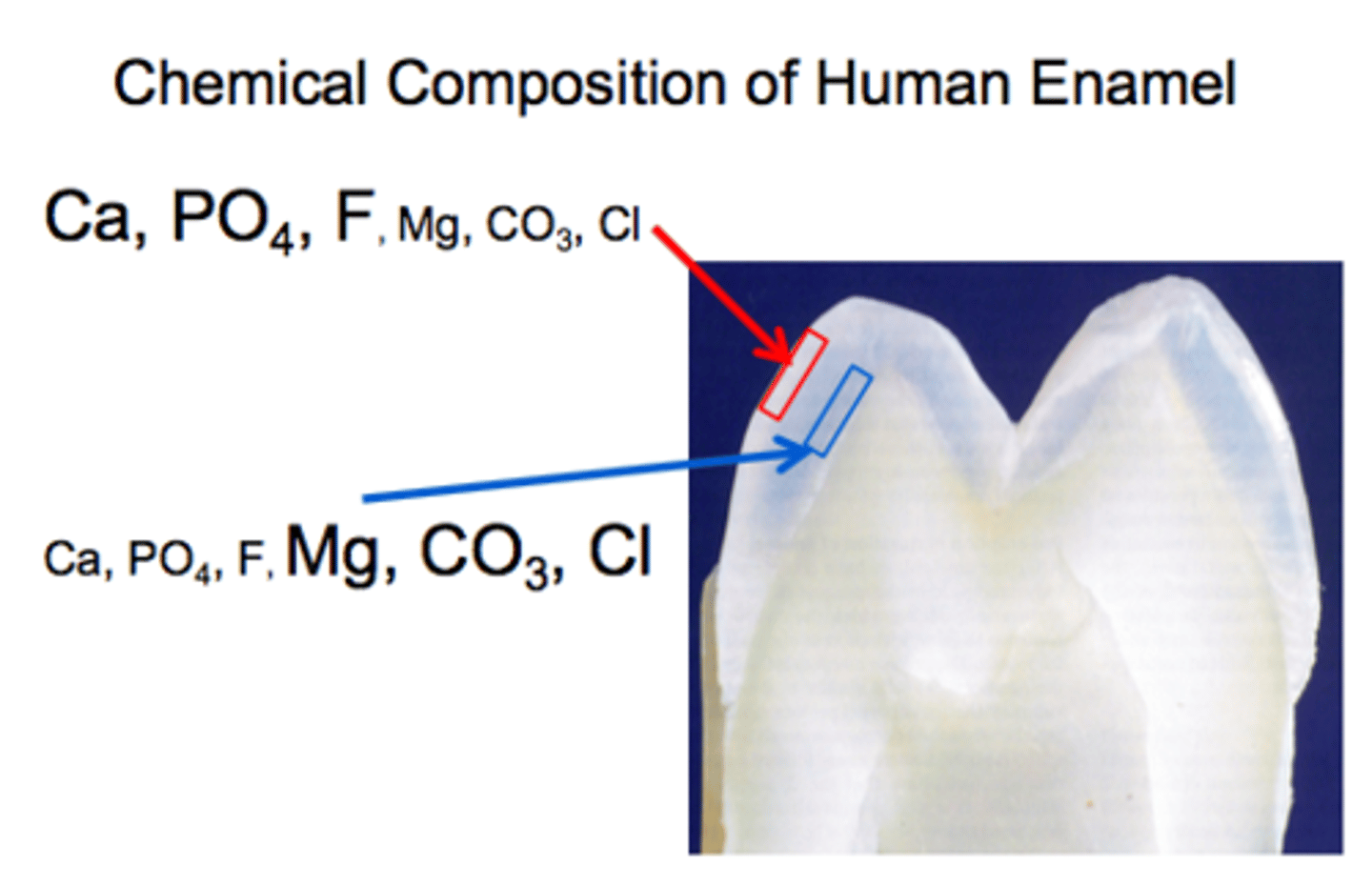
Chemical composition of human enamel:
The outer layer, the calcium phosphate fluoride is much HIGHER than the magnesium carbon chloride.
Close to the DEJ, the calcium phosphate fluoride is LESS THAN magnesium carbon chloride.
Is enamel or dentin more mineralized?
enamel
What does DENTIN consist of by volume?
55% by volume is inorganic, 20% by volume is water and 25% by volume is protein.
What does DENTIN consist of by weight?
75% is inorganic, 5% is water and 20% is protein.
Dentin is sometimes called the ______ __________ compared to enamel.
live tissue
Dentin
Physically and chemically the dentin closely RESEMBLES BONE.
The odotoblast cell bodies remain external to dentin but their processes exist WITHIN TUBULES IN DENTIN.
--> It is HARDER than bone, but SOFTER than enamel.
Why is dentin called "live tissue"?
Because enamel does not have any metabolic reaction or intercellular replacement. On the other hand, dentin does.
Primary Dentin
it is formed BEFORE eruption, forms the bulk of the tooth
Secondary Dentin
it begins formation after eruption
Tertiary Dentin
it is formed in response to irritation and appears as a localized deposit on the wall of the pulp chamber
How does saliva play a major role in the oral cavity?
Saliva plays a major role in protecting the teeth against acid challenge.
What are the specific roles of saliva?
-PROTECTION OF TEETH AND ORAL MUCOSA
-mechanical cleansing
-lubrication
-prevents tooth demineralization
-buffer capacity
-ANTIMICROBIAL ACTIVITIES
-antibacterial functions
-DIGESTIVE PROPERTIES
-facilitation of swallowing
-initial digestion
-FACILITATION OF SPEECH
Early (caries) lesion
Non cavitated lesion
White-spot lesion
Incipient/Initial (caries) lesion Subsurface (caries) lesion
They are essentially talking about EARLY STAGE OF DENTAL CARIES. Those non-cavitates white spots or white lines, when you hear those terms, they are essentially talking about the same thing. When you hear those words they are all talking about the BEGINNING OF THE LESION.
Advanced (caries) lesion Cavitated lesion
Cavitation
Cavity
Hole
ADVANCED STAGES OF DENTAL CARIES. When you hear those terms, they are talking about the later stages of the disease process.
Root caries
occurs on the root surface
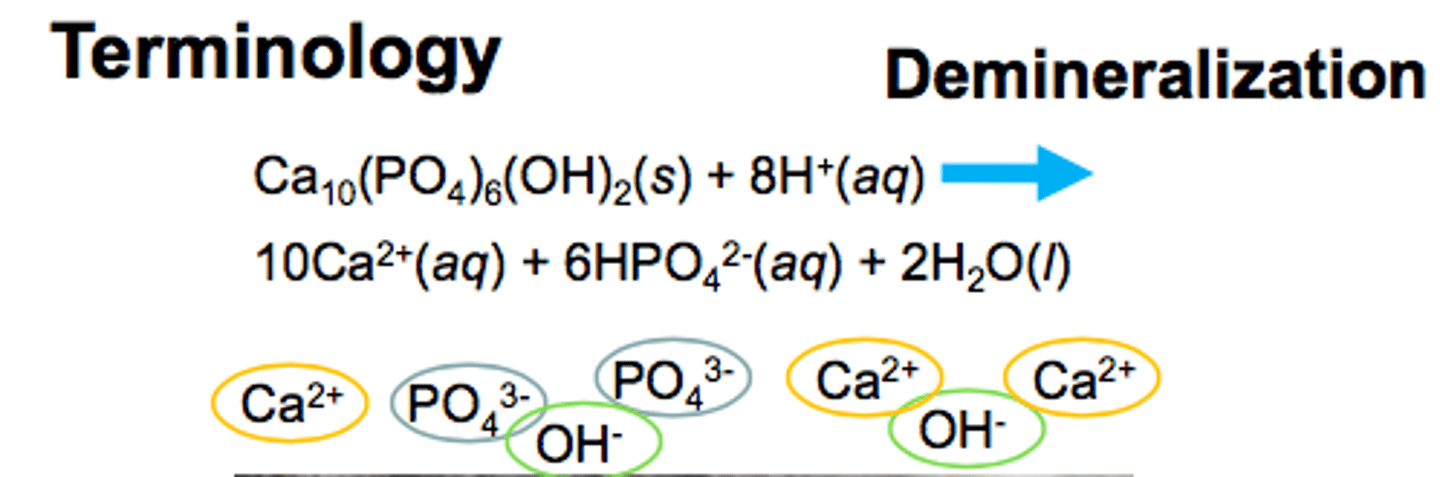
Demineralization
CALCIUM and PHOSPHATE MINERALS leeching out from healthy structure
--> You have probably heard the term decalcification. But that does not properly describe dental caries!! IT IS THE LEECHING OUT OF MINERALS!
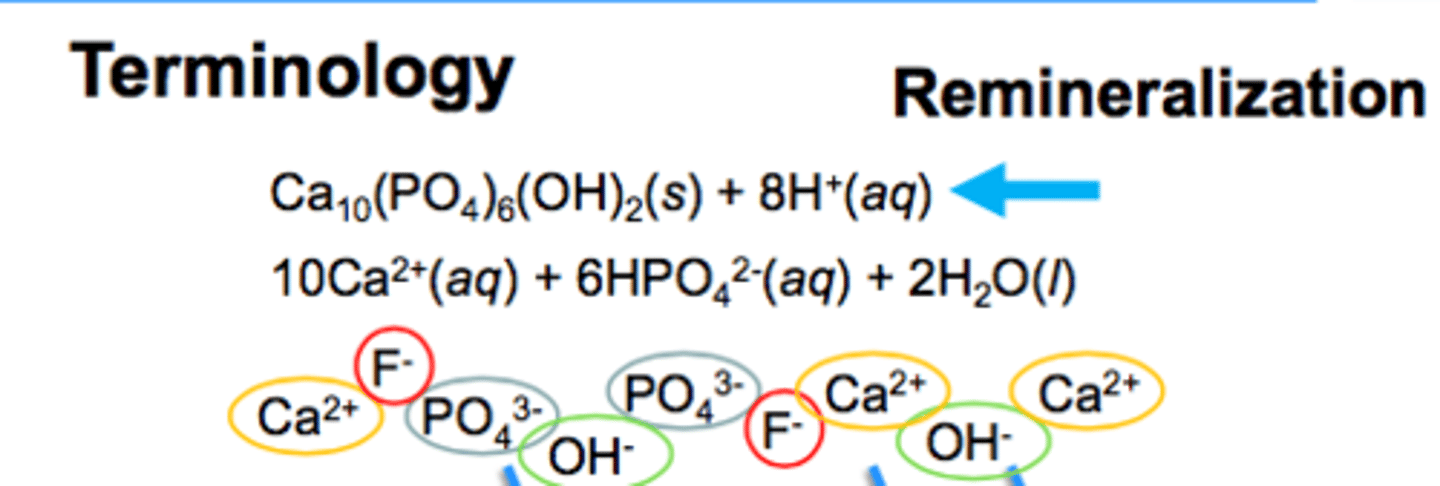
Remineralization
going back to the original structure after having been demineralized
Dental caries
Dental caries has a MULTIFACTORIAL CAUSE, is a SITE-SPECIFIC DISEASE, and is a DYNAMIC PROCESS that is modified by protective factors.
How can dental caries be preventable and interruptible?
can be achieved by identifying demineralizing (i.e., active) lesions and arresting or reversing these lesions at an early stage.
Again, dental caries is...
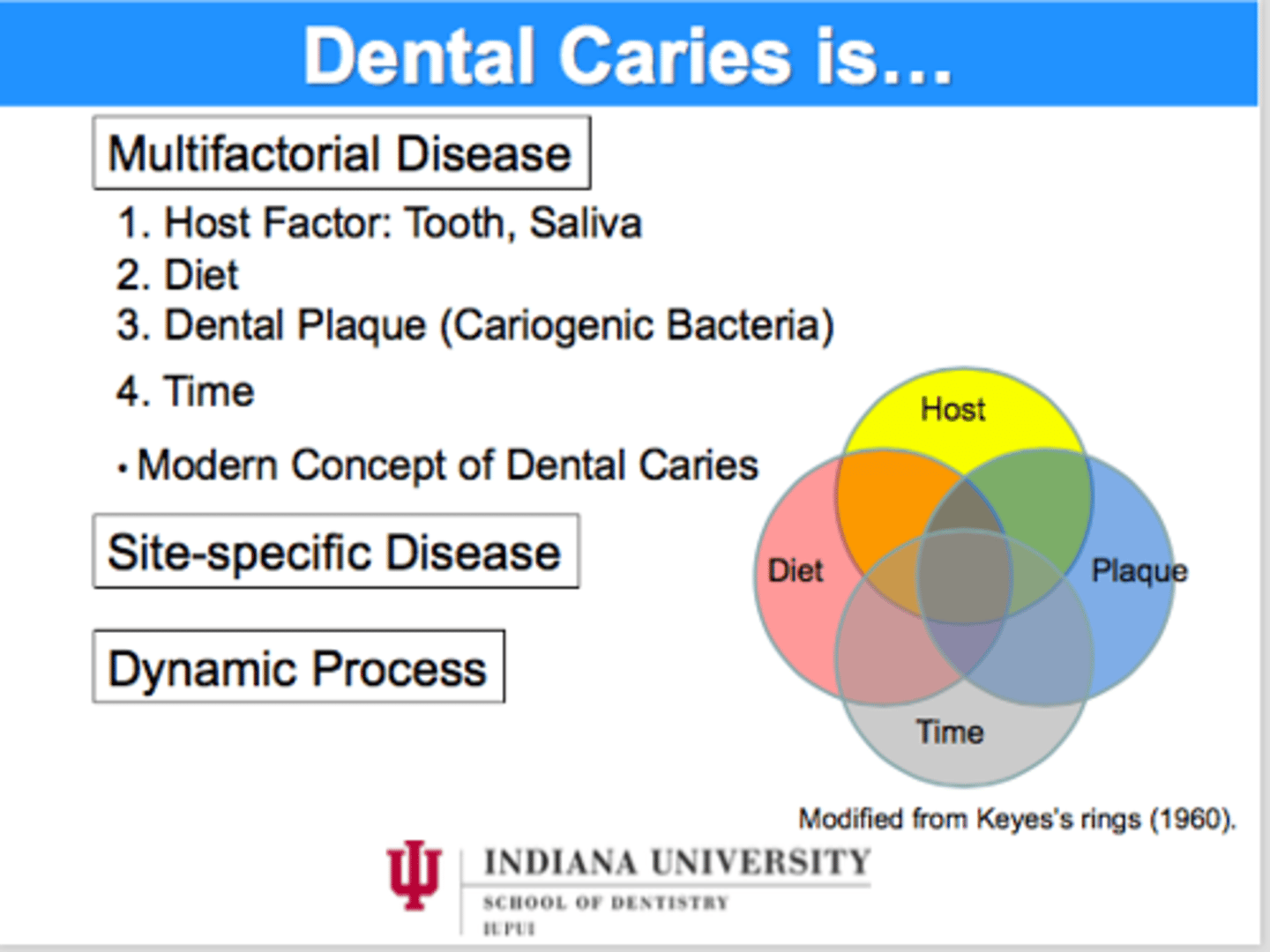
What are the pathological factors?
Diet, plaque, reduction a saliva flow, low buffering and acidic environment.
What are the 5 steps of the CARIES PROCESS?
1. pellicle formation
2. plaque formation
3. production of acid
4. diffusion of acid
5. demineralization
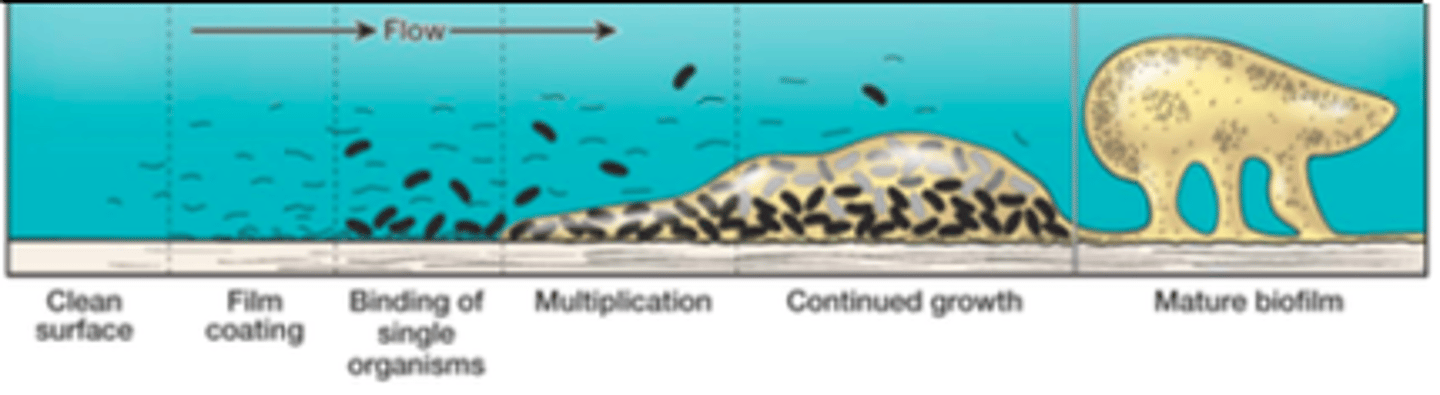
Plaque formation
1) Pellicle formation.
2) Attachment of early bacterial colonizers (like S. mutans) (0-24 h).
3) Co-adhesion and growth of attached bacteria leading to the formation of microcolonies (4-24 h).
4) Microbial succession leading to increased species diversity concomitant with continued co-adhesion and growth of microcolonies (1-7 days).
5) Climax community/mature dental plaque/biofilm (1 week or older).
--> By the end, what's going to happen, is that is will not continue to grow on the tooth surface, it will detach. It will look for a new surface to attach to. That is the life cycle of dental plaque.
Production of acids
-production of organic acids by plaque microorganisms
--> this starts the DEMINERALIZATION phase! it starts with this production of organic acids by plaque bacteria after exposure to FERMENTABLE CARBOHYDRATE
What is the critical pH (in regards to caries formation)?
5.5
--> means that the enamel structure starts dissolving
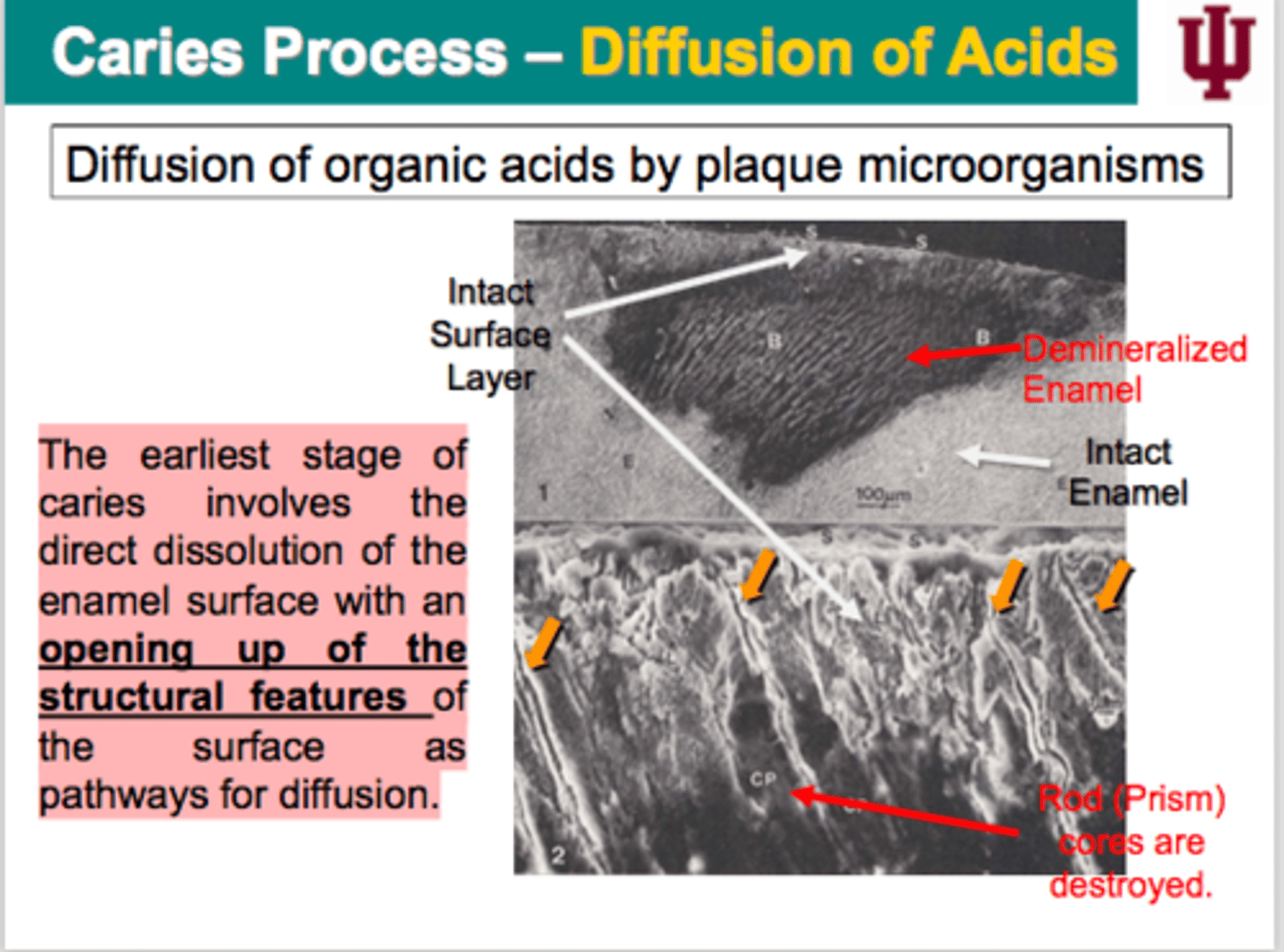
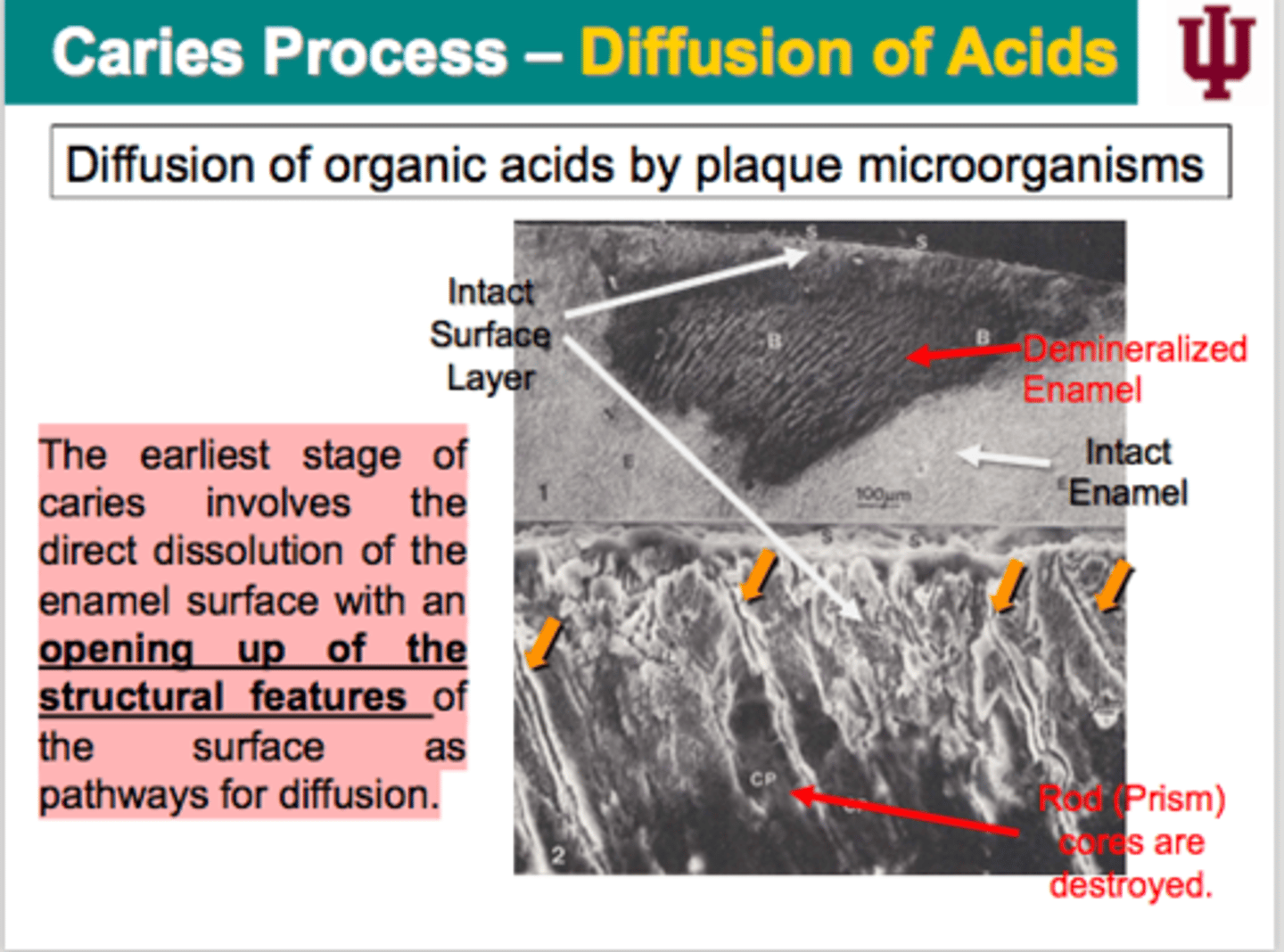
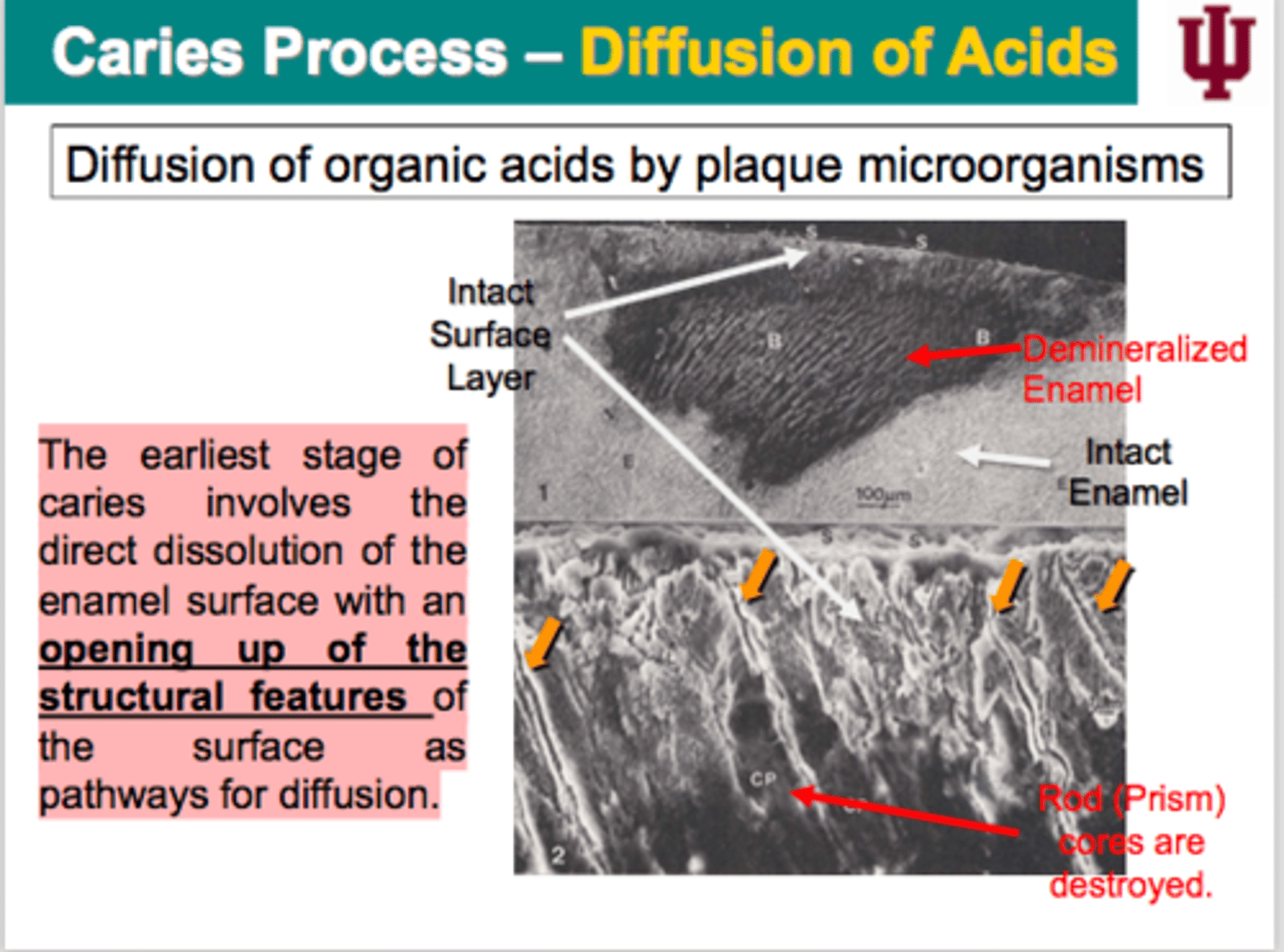
Diffusion of acids
-diffusion of organic acids by plaque microorganisms
-->The earliest stage of caries involves the direct dissolution of the enamel surface with an OPENING UP OF THE STRUCTURAL FEATURES of the surface as pathways for diffusion.
What is the channel called that things like lactic acid diffuse through to eventually cause a carious lesion?
micro channel, approximately 0.1 to 0.7 microns... starts very small and if nothing is done about it it will become a cavity
What is unique about the "diffusion of acids" stage?
This is the stage where you can certainly stop the carious process and you can maintain the current structure of your mouth.
What are some HOST FACTORS for teeth?
Location
Where?
Morphology
Shape?
Composition
Chemical component?
Ultrastructure
Physical structure?
Posteruptive age
Time?
Host factor - Location?
Morphology?
Areas of stagnation where PLAQUE can accumulate undisturbed.
-Occlusal surfaces of posterior teeth.
-Lingual pits of the maxillary incisors.
Pit and Fissure
Approxial surface
Gingival margin
Host factor - Structure?
Composition?
The LESS STABLE the crystals, the more soluble enamel are.
Carbonate (CO32-) DECREASES crystal stability and therefore increases the solubility of enamel.
The LARGER and MORE UNIFORM the crystals, the LESS the specific surface area and reactivity (solubility).
Host factors - Posteruptive age?
The caries susceptibility of the enamel surface is greatest IMMEDIATELY AFTER ERUPTION and tends to decrease with age.
-->During the eruption, the more soluble carbonate-rich apatite is preferentially lost and replaced by apatite lower in carbonate and higher fluoride.
The reprecipitated crystals may eventually grow to be larger than the original crystals, creating hypermineralized areas of enamel.
i.e. ENAMEL MATURATION
Host factor - Saliva?
LOSS OF SALIVARY FUNCTION has been associated with rampant caries activity.
Saliva plays a major role in protecting the teeth against acid challenge.
• Mechanical cleansing action
• Dilution and buffering of plaque acid • Antimicrobial properties
• Providing inorganic and organic component
What may cause saliva not to function?
RADIATION THERAPY
Q: Which side of this patient had radiation therapy?
A: left side
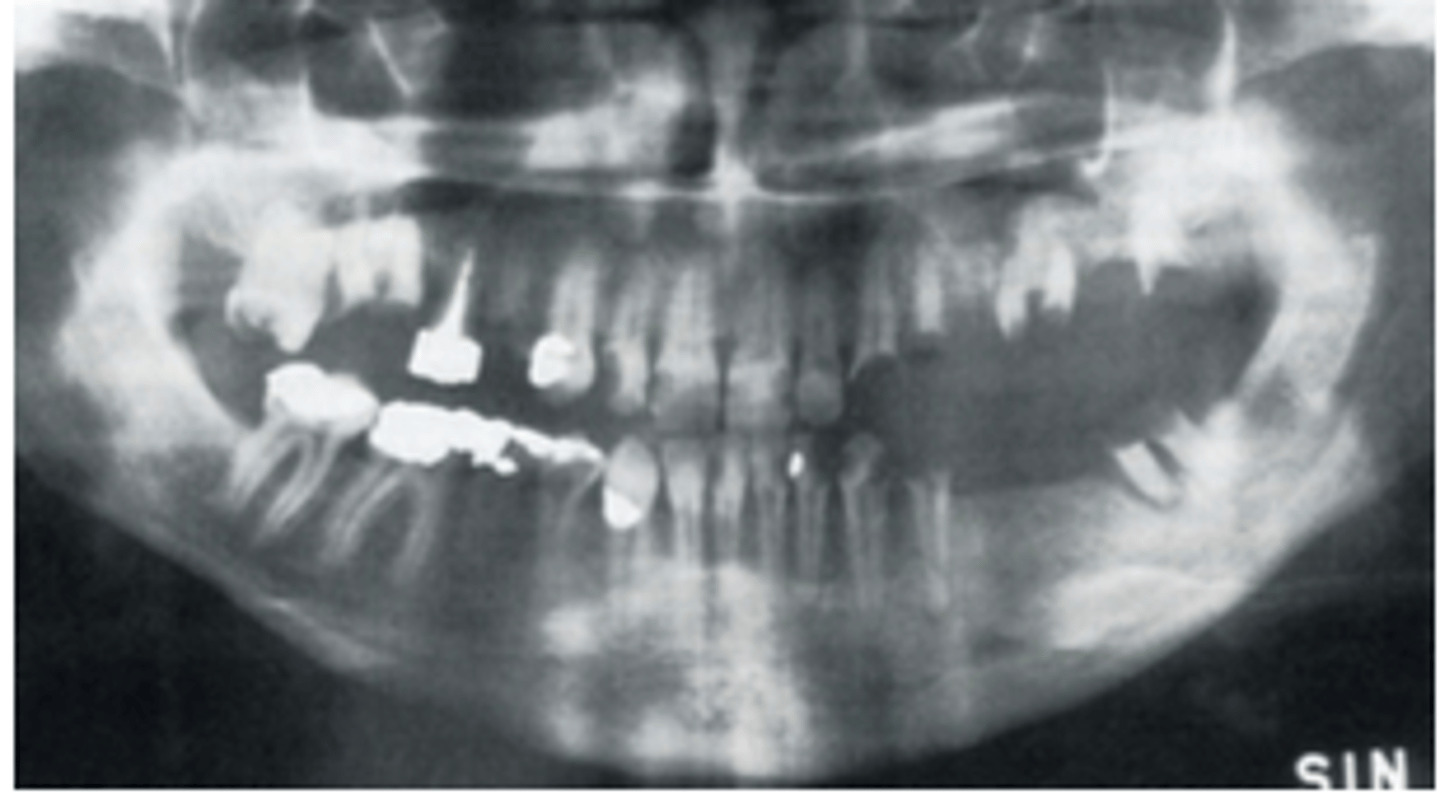
At what dosage of radiation therapy is damage caused?
>40 Gy
-causes damage to glandular parenchyma, followed by atrophy and fibrosis
-changes composition of saliva: viscous, white, yellow, or brownish fluid with REDUCED pH, poor buffering capacity, etc.
Sjögren's Syndrome
-Sjögren's syndrome is a chronic or lifelong AUTOIMMUNE DISEASE.
• When a person has an autoimmune disease, the immune system attacks the
body instead.
• In Sjögren's syndrome, this attack typically starts with the MOISTURE-PRODUCING
glands, which are called the exocrine glands. Salivary glands are exocrine glands that produce saliva.
• If the exocrine glands fail to create enough moisture, the person may experience a number of uncomfortable symptoms.
• Nine out of 10 people diagnosed with Sjögren's syndrome are WOMEN, with the average age of symptom onset IN THE 40s. Dryness symptoms associated with Sjögren's syndrome worsen during menopause.
Host factors - Diet?
The FREQUENCY OF EATING fermentable carbohydrates has been strongly associated with caries prevalence and incidence.
-The simple sugars (sucrose, glucose, fructose) are considered MORE CARIOGENIC than complex carbohydrates (starches).
-SUCROSE represents the main source of sugar and has implicated as an important determinate of dental caries.
In regards to eating, some say the AMOUNT of consumption is key. However, this is not the case. The important component in determining how eating might cause dental caries is...?
FREQUENCY of how often a person consumes fermentable carbohydrate
More sugar =
more carious lesions
With plaque, is it the AMOUNT of plaque or HOW LONG the plaque sits on your teeth that is the problem?
how long the plaque sits on your teeth
Host factors - dental plaque?
It is only under conditions that lead to FREQUENT AND PROLONGED ACIDIFICATION of dental plaque.
-These plaque microorganisms become pathogenic.
-A number of endogenous oral micoorganisms found in the dental plaque can contribute the caries process.
- Mutans streptococci
- Lactobacillus species
- Actinomyces species
What is the critical pH of dentin? Is it higher or lower? why?
between 6 and 6.6, it is HIGHER because dentin is LESS MINERALIZED
Critical pH
The pH at which a solution is just saturated with respect to a particular mineral.
--If the pH of the solution is ABOVE the critical pH, the solution is supersaturated and mineral will precipitate.
--If the pH of the solution is LESS THAN the critical pH, the solution is undersaturated and mineral will dissolve until the solution becomes saturated.
4.5-5.5 is the range of the critical pH of caries formation in enamel. This range coincides with pH of acids formed when __________________________________?
PLAQUE BACTERIA FERMENT CARBOHYDRATES
Critical pH is NOT a fixed value. It depends on the levels of what two things in plaque fluid?
calcium and phosphate
Summary of DENTAL CARIES:
tooth - area of stagnation where PLAQUE can lay undisturbed.
The LESS STABLE crystals are the more likely you are to develop dental caries.
IMMEDIATELY AFTER ERUPTION, you are most likely to develop dental caries.
LOSS OF SALIVARY FUNCTION may contribute to dental caries.
Diet - not the amount, FREQUENCY of consumption of fermentable carbohydrate may contribute to dental caries.
Plaque-also not the amount but how long (FREQUENCY AND PROLONGED ACIDIFICATION) acidic plaque sits on the tooth surface. That is the summary of what may contribute to dental caries.
Q: Are these surfaces of teeth with white spots/lesions PRE-CARIOUS?
A: No, they are CARIOUS
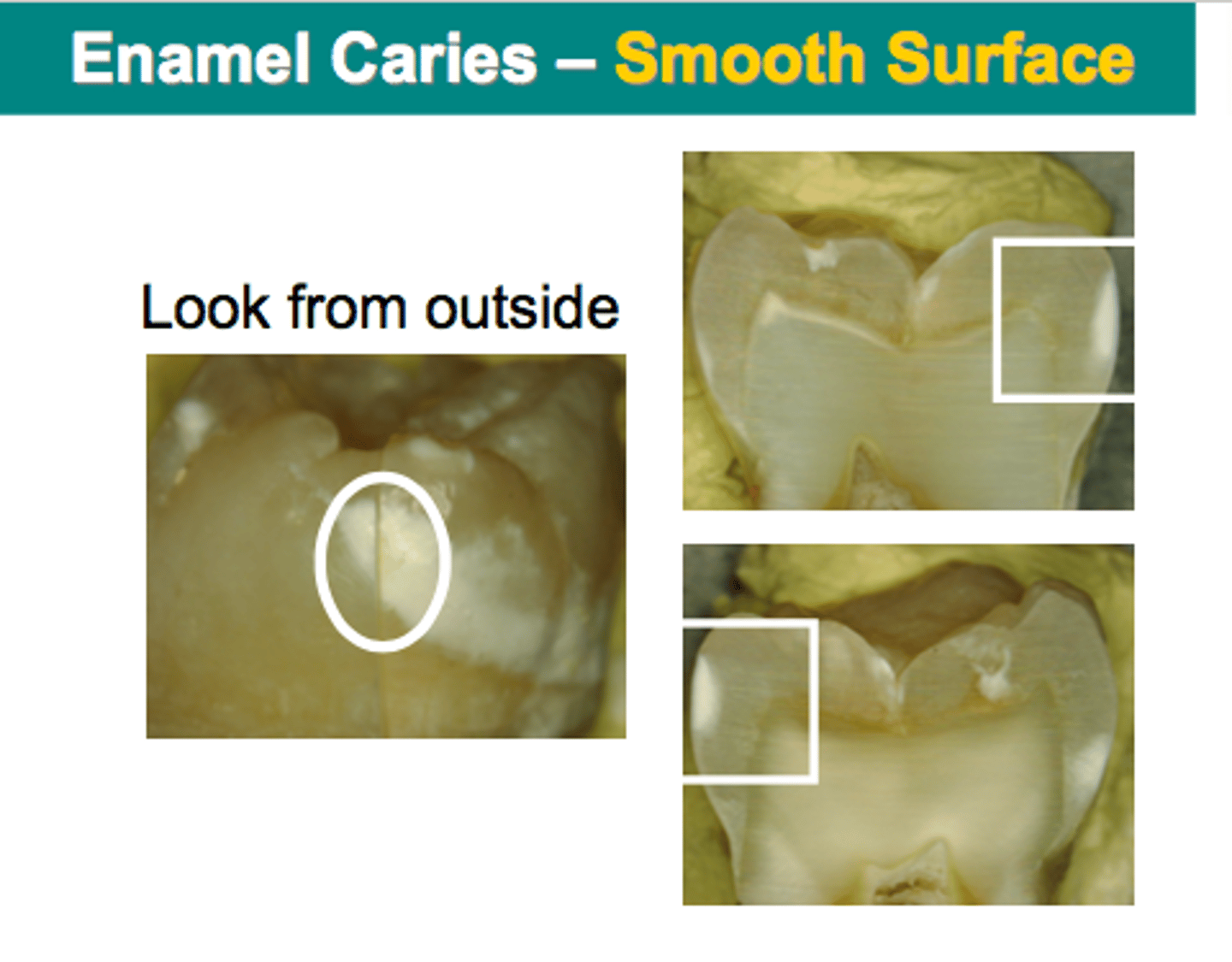
What are the ZONES OF DENTAL CARIES when cut in half?
1. surface zone
2. body of the lesion
3. dark zone
4. translucent zone
What are the two theories to explain the formation of the intact surface zone overlying the intact non-cavitated caries lesions?
1. One is a GREATER ACID RESISTANCE of the surface layer due to compositional characteristics of the surface enamel.
2. Other one is a result of RE-PRECIPITATION of minerals from dissolving sub-surface lesions.
Professor's opinion....
Surface layer formation can be explained by a combination of BOTH theories.
Dentinal (root) lesion process:
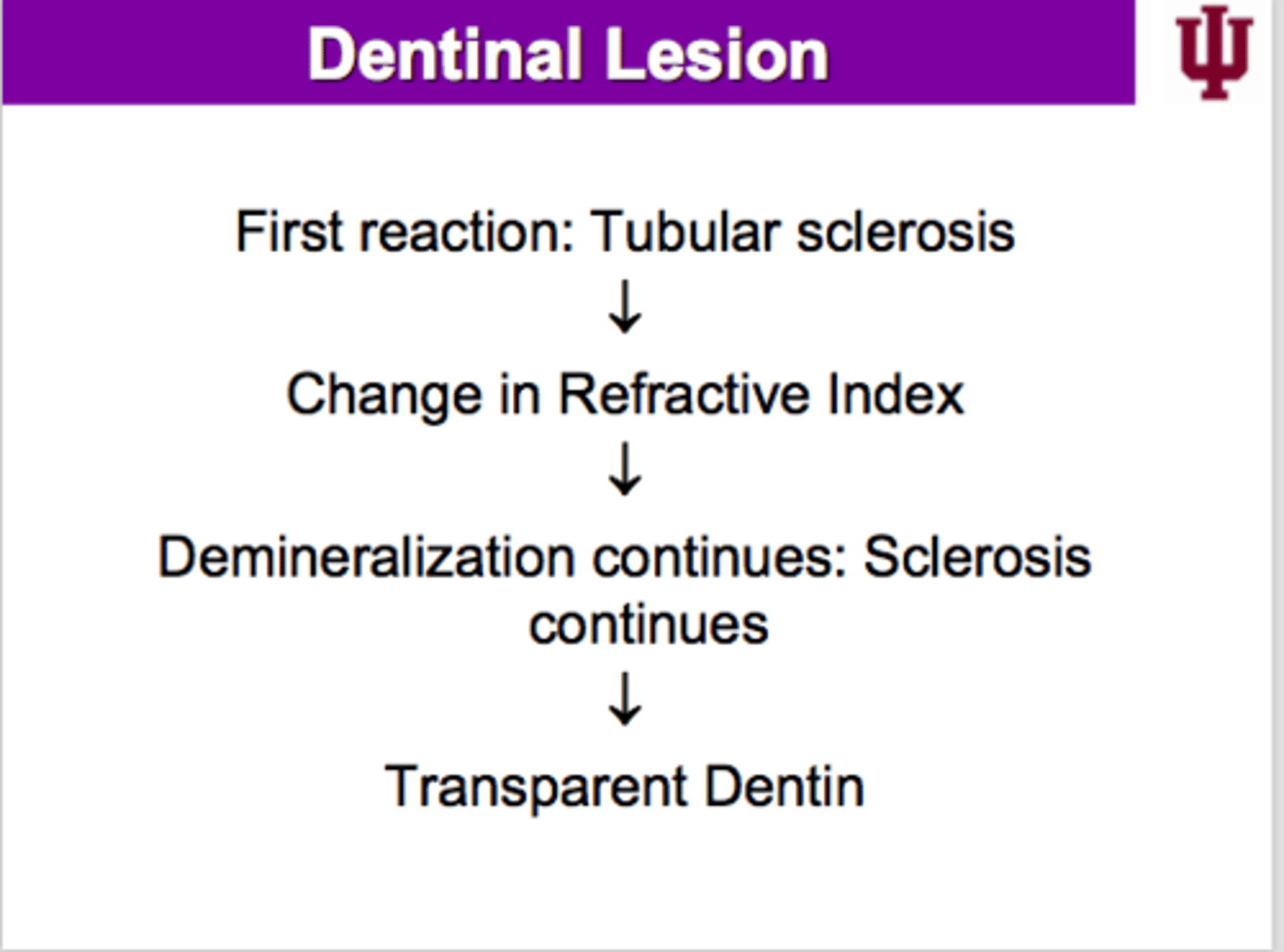
Transparent (dentin) layer
-major portion of inner carious dentin
-tubule lumina fills with Ca and PO4 (HOMEOSTATIC MECHANISM FROM THE PULP)
-Saturation with Whitlockite - grow to form gigantic rhomboidal crystals
-REDUCED permeability
Tubular sclerosis
-when dentin realizes that something is coming in from the outside, it starts to protect itself... in turn, CALCIUM and PHOSPHATE will start depositing in the dentin tubular which will change the reflective index! when demineralization continues... that is what creates the transparent dentin!!
Reflective index
change in the speed of light
When sclerosis continues, what is eventually formed?
reactive dentin (tertiary dentin) is formed
Tertiary dentin - dentinal lesion
-pulp reaction
-starts even before dentin bacterial invasion
-IRREGULAR mineralization
-IRREGULAR dentinal tubules
What two processes occur all of the time in teeth to maintain BALANCE?
demineralization and remineralization
Clinical cavitation
If MINERAL LOSS OUTWEIGHS GAIN, over time, the caries process will progress to the CLINICAL CAVITATION of the tooth surface.
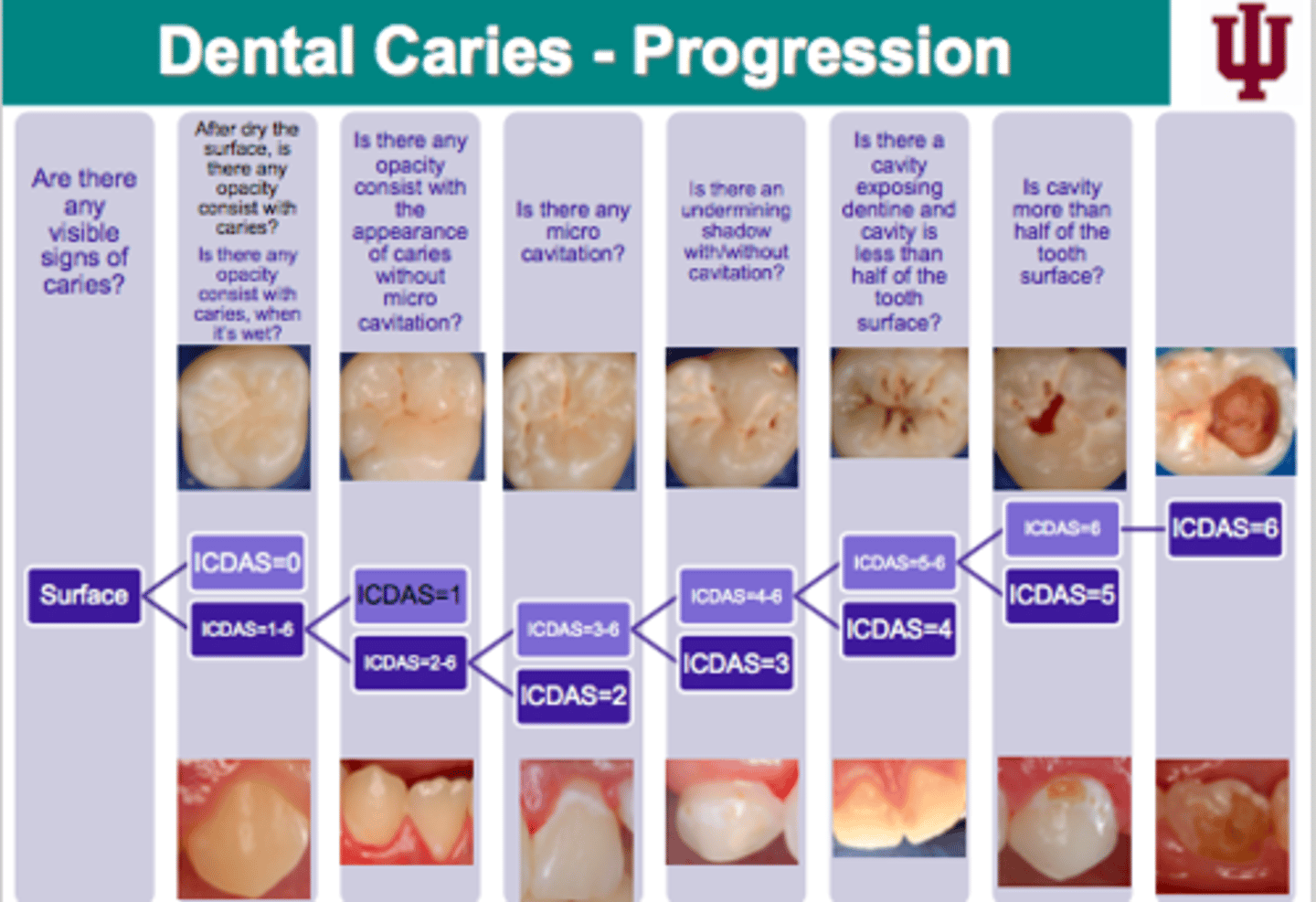
Dental caries - progression
Secondary caries
-caries lesions that exist adjacent to restorations
What are the two areas of secondary caries?
1. outer lesions
2. wall lesion
Outer lesion
considered to be caused by plaque accumulation in a manner similar to the initiation of primary lesion
Wall lesion
thought to be the result of microleakage
If you illuminate (infrared transillumination) a tooth with near infrared and there is a lesion in the tooth, what will you see?
dark shadowing
--> this method does NOT involve radiation so it can be used with pregnant women
At what "time zone" should a dentist situate behind his/her patient?
12 o clock or 11:30 of your patient
Should you ever pass an instrument over a patient's face?
never