maternity unit 3: ch 18 - fetal monitor
1/47
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
48 Terms
how can FHR be measured
externally with doppler
internally with fetal scalp electrode
tocodynamometer
measures frequency of contractions externally on abdomen @ level of fundal height
doesn't measure intensity
intrauterine pressure Catheter
measures contractions internally
measures intensity
baseline
average FHR over 10 minutes rounded to the nearest 5 bpm
variability
fluctuations in the FHR of 2 cycles per minute or greater
absent
minimal - normal
moderate
marked
most important indicator of fetal Oxygen status
should be traced for 10-20 minutes
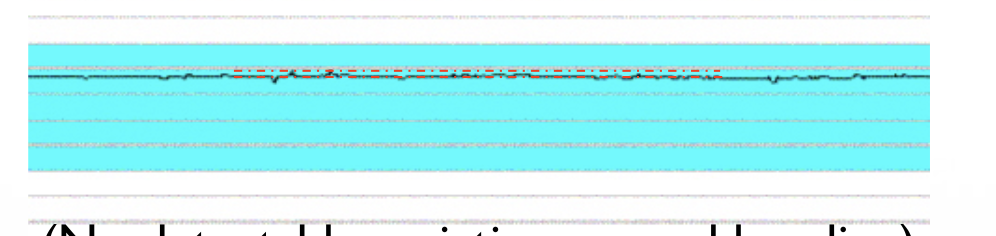
this is what type of variability
absent variability - amplitude range is undetectable (straight line)
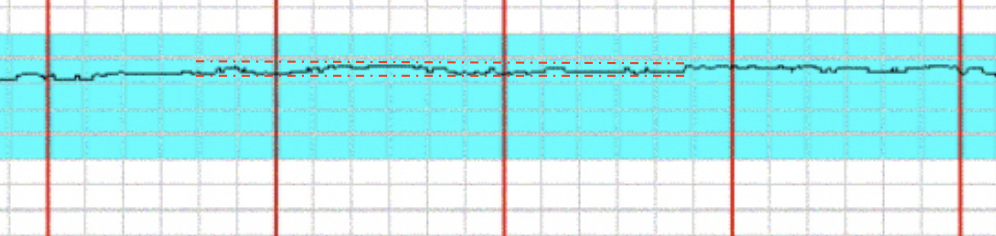
this is what type of variability
minimal variability - 5 or less change bpm
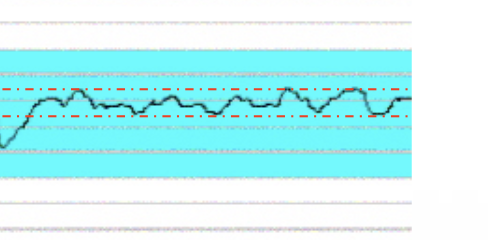
this is what type of variability
moderate (normal) - 6-25 change in bpm
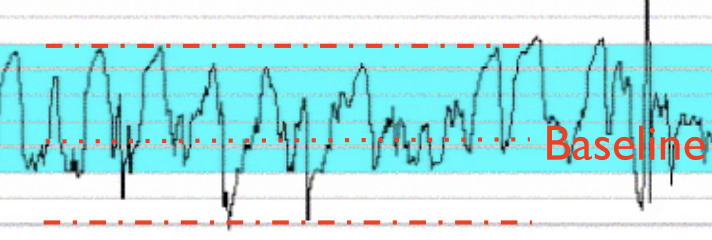
this is what type of variability
marked - greater than 25 change in bpm
causes of decreased variability
fetal sleep cycles
hypoxemia / acidosis
certain drugs (magnesium/ narcotics)
prematurity
arrhythmias
fetal tachycardia
nuero abnormalities
congenital anomalies
how do we stimulate a sleeping fetus
give mom ice, sugar (cookie or juice)
fetal scalp stimulation
causes of increased variability
fetal stimulation
mild, transient hypoxemia
sympathomimetic drugs
acceleration
a visually abrupt increase in HR
onset to peak is less than 30 seconds
duration is measured from onset to when the HR returns to basleline
we want 2 accels in a 20 minute period
accelerations in a 32 week baby
acme (peak) of 15 bpm lasting 15 seconds or more, but no more than 2 minutes
accelerations in a baby less than 32 weeks
acme (peak) of 10 bpm lasting 10 seconds or more, but no more than 2 minutes
prolonged acceleration
lasts 2 minutes or more but no more than 10 minutes
more than 10 minutes is a change in baseline
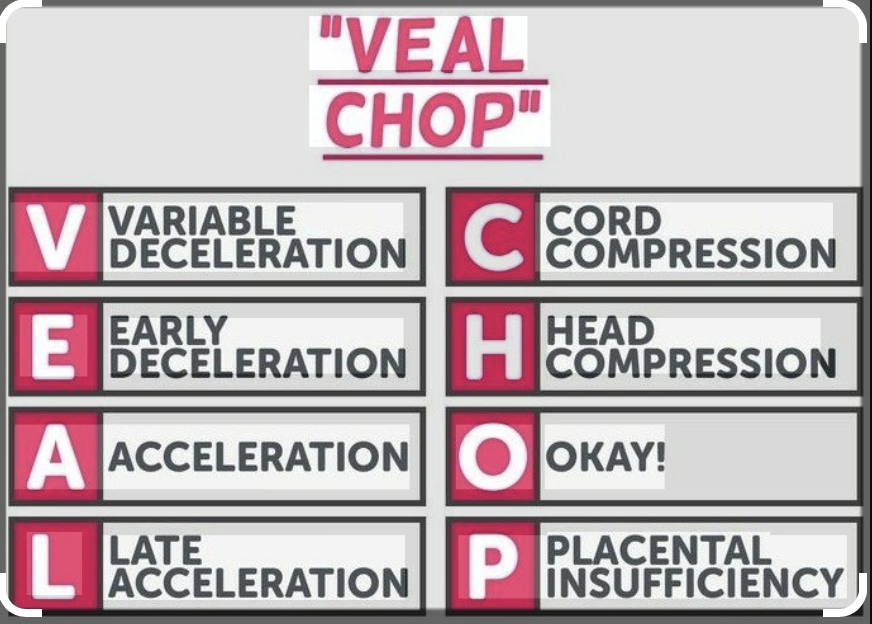
variable deceleration
abrupt decrease in FHR
onset to nadir is less than 30 seconds
15 bpm drop or less
lasts at least 15 seconds or more but no more than 2 minutes
not associated with contractions (can happen with or without contractions)
what are variable decelerations caused by
cord compression
fetal head compression - causes vagal nerve stimulation
if it happens after ROM it is associated with cord prolapse (cord delivers before mom)
when associated absent or minimal variability, it can indicate hypoxemia or acidosis
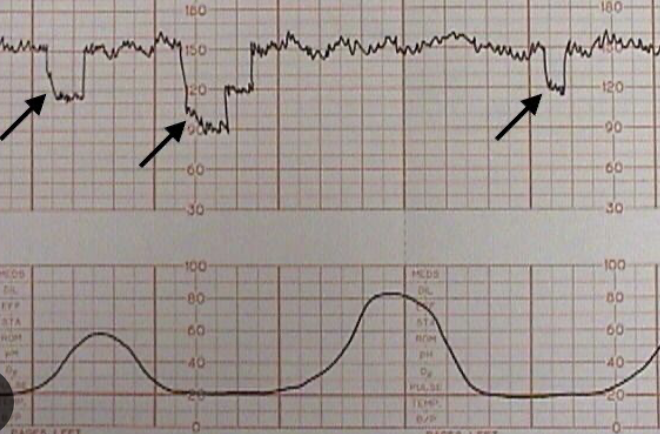
this is showing?
variable deceleration
early deceleration
gradual decrease and return to baseline FHR
onset to nadir is 30 seconds or more
Nadir occurs at the same time as the peak of mom’s contractions
what are early decelerations caused by
fetal head compression - causes vagal nerve stimulation
not associated with hypoxemia or acidosis
if early In labor , it may indicate cephallopelvic disproportion
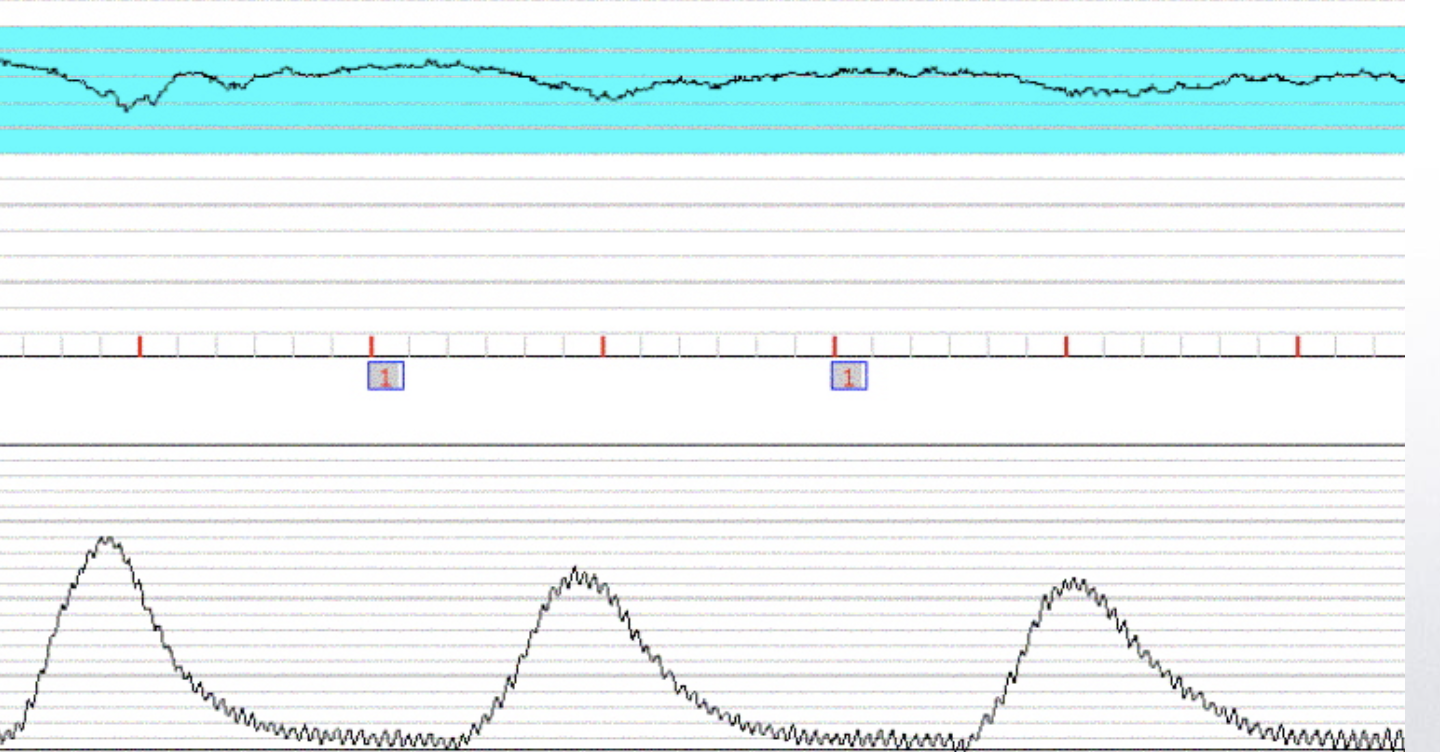
this is showing
early decelerations - Nadir is aligned with peak of contractions
late deccelerations
gradual decrease and return to baseline FHR
onset to nadir is 30 seconds or more
Nadir occurs after the peak of mom’s contractions
what are late decelerations caused by
uteroplacental insufficiency (uterine perfusion, uterine tone or placenta function)
always relative hypoxia, but not always hypoxemia or acidosis
some causes are reversible some ore not
reversible causes of late decelerations
maternal hypotension
uterine hyperactivity - can stop with tocolytics (relaxes smooth muscle)
irreversible causes of late decelerations
placental abruption or infarction (placenta detaches from uterine wall, must deliver baby immediately - both mom and baby are hemorrhaging)
placenta previa - placenta implanted lower than normal
may or may not be reversible causes of late decelerations (5)
chorioamnionitis - infection (high temp & tender uterus)
IUGR
maternal hypertension, diabetes, anemia or cardiac issue
Rh isoimmunization
maternal tabbacco use
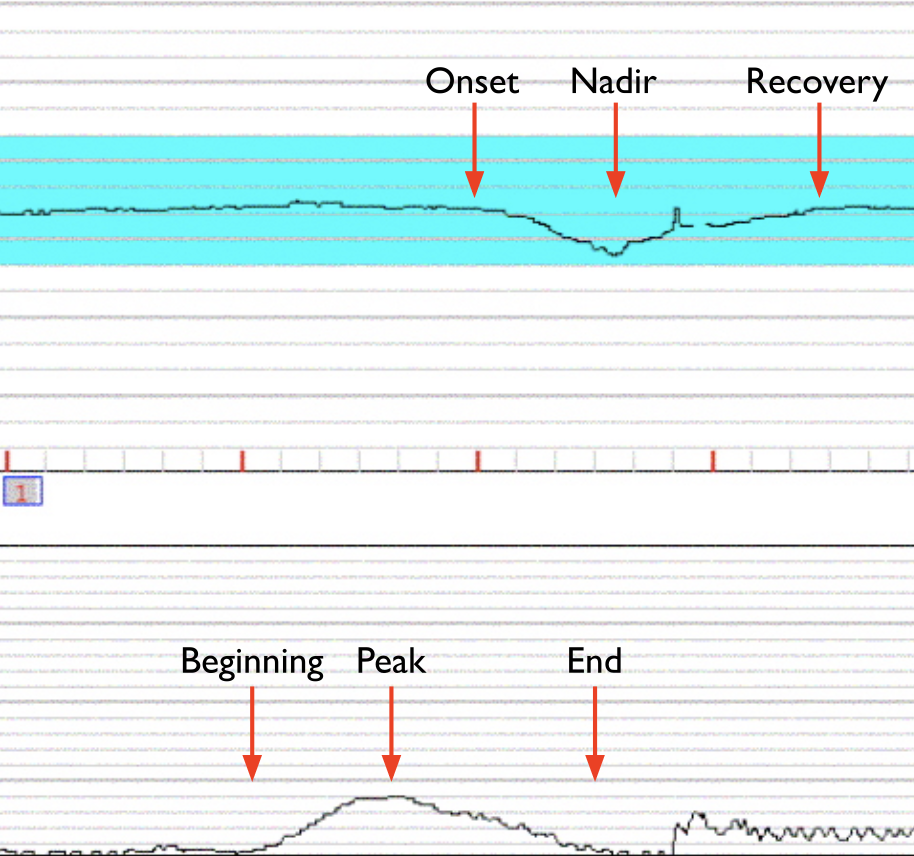
this is showing
late deccels
prolonged decceleration
decceleration drops 15 bpm or more, lasting at least 2 min but less Than 10 minutes
after 10 minutes it is a change in baseline
causes of prolonged decelerations (7)
cord compression/ cord prolapse
profound maternal hypotension
maternal hypoxia
tetanic contractions - no break in between contractions
amniotic fluid embolism (fatal) - goes into moms bloodstream, may go to her lungs/heart
prolonged head compression
paracervical anesthesia
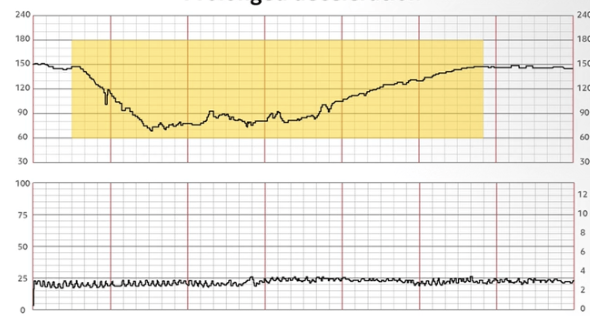
this is showing?
prolonged decelerations
VEAL CHOP
causes of specific decelerations
causes of fetal tachycardia (greater than 160bpm)
maternal fever, sepsis, chorio
drugs
fetal hypoxemia
tachyarrythmias
fetal heart failure
hydrops - fluid overload in fetus
severe fetal anemia
maternal hyperthyroidism
interventions to fetal tachycardia
assess moms temp - may have fever or chorioamnionitits
asses for arrhythmias
oxygen
look for non-reassuring sings in FHR - may have to deliver
causes of fetal bradycardia (less than 110)
drugs
hypoxemia
maternal hypotension
hypothermia
maternal hypoglycemia
fetal bradyarrythmias
congenital heart blcok
cord compression
amniotic fluid embolism
interventions to fetal bradycardia 9
turn pt to left lateral Side - avoids supine hypotension
fluid bolus (increases CO)
lower head of bed
vasopressor - ephedrine (raises maternal BP)
give oxygen
stop oxytocin / give tocolytic - gives rest time between contractions if tachysystole
exam abdomen for rigidity - indicates bleeding/ placental abruption
assess for congenital heart block
may need to deliver if interventions fail
sinusoidal pattern
medical emergency - must call MD ASAP
severe fetal anemia
caused by Rh isoimmunization, fetal blood loss, fetal hypoxemia or acidosis, or maternal drug use
persists for 20 minutes or greater
psuedosinusoidal pattern
seen intermittently in 15% of births
associated with drugs administered during labor
less uniform and transient
not associated with adverse outcomes
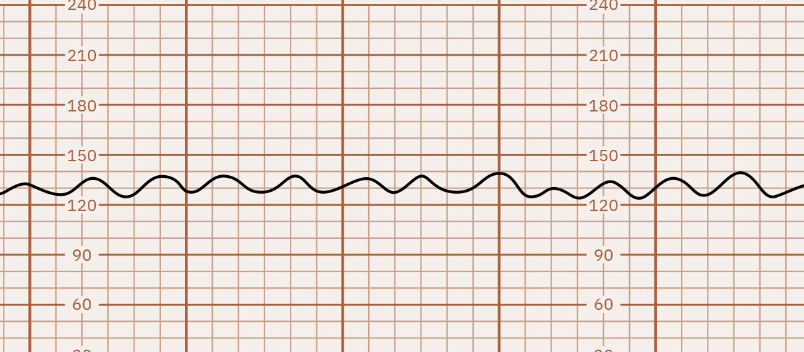
this is showing
sinusoidal pattern
contractions
counted as the # of contractions in a 10 minute window
averaged over 30 minutes
measured from peak to peak
normal contractions: 5 or less contractions in 10 minutes
tachysystole contractions:
more than 5 contractions in 10 minutes
always qualified to presence or absence of fetal deccels
applies to both SROM or induced labor
interventions for late deccels 8
turn pt to left lateral Side - avoids supine hypotension
fluid bolus (increases CO)
lower head of bed
vasopressor - ephedrine (raises maternal BP)
give oxygen
stop oxytocin / give tocolytic - gives rest time between contractions if tachysystole
exam abdomen for rigidity - indicates bleeding/ placental abruption
may need to deliver if interventions fail
interventions for variable deccels 5
change maternal positon to receive cord compression
give oxygen
stop oxytocin / give tocolytic - gives rest time between contractions if tachysystole
vaginal exam - check for cord prolapse
amnioinfusion - replacing amniotic fluid loss
interventions for decreased variability
observation to see if they are transient (fetal may be sleeping)
look over hx - may be from maternal drug use
Position change, O2, fluids - helps relieve hypoxia
stop oxytocin / give tocolytic
fetal scalp stimulation
interventions for prolonged deccels
stop oxytocin / give tocolytic
Position change, O2, - helps relieve hypoxia
asses for hypoxemia, hypotension, placental abruption, or cord prolapse
may need to deliver if it doesn’t resolve within 6 minutes
Category 1
normal
strongly predict normal acid -base status
no intervention required
category 2
intermediate
do not predict abnormal acid-base status
require evaluation and continued surveillance
category 3
abnormal
predict abnormal acid-base status
require immediate evaluation and intervention