Hyperglycemic Crises, ACLS
1/54
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
55 Terms
Diabetic ketoacidosis (DKA) =
Hyperosmolar hyperglycemic state (HHS) =
uncontrolled hyperglyc + MA + inc ketones
sev hyperglyc + hyperosmolality + dehydration w/o significant ketoacidosis
Medications that can cause hyperglycemic crises → 7
SGLT2i
glucocorticoids
antipsychotics
CPIs
sympathomimetics
thiazides
pentamidine
CLINICAL PRESENTATION
DKA vs HHS
Onset
Cognitive state
Main s/s
other s/s
Respiration
DKA hrs-days → HHS days-weeks
DKA alert → HHS change in cog
BOTH polyuria, polydipsia, -weight, dehydration
DKA NV + abd pain → HHS co-presenting w other acute illness
DKA kussmaul resp
DKA is most common in ______
T1DM
HHS is most common in _____
T2DM
DKA/HHS TREATMENT → 5
fluids
insulin
K+
phos
bicarb
FLUIDS
fluid =
________ during the first _____
Add dextrose-containing fluids (eg. 5% or 10% dextrose) when blood glucose ______ mg/dL
balanced crystalloid (LR or plasmalyte)
500-1000 mL, 2-4h
<250
INSULIN
Goals: correct hyperglycemia by ______ mg/dL/h
Goals: blood glucose
IV insulin: ______ infusion
Hyperglycemia is corrected _______ than ketoacidosis →
50-75
DKA 150-200; HHS 200-250
0.1U/kg/h
faster → -inf rate to 0.05U/kg/h when BG <250
SPECIAL CASE - EUGLYCEMIC DKA (EDKA)
Associated with ______
Glucose _____ in presence of MA diagnosis criteria
Start …
SGLT2i
<200
dextrose fluid concomitantly w insulin inf
POTASSIUM
Goals: K+ _____ mEq/L
Initiate replacement once K+ is ____ → ______ mEq KCl per liter of IV fluid
If K+ _____ → DO NOT initiate insulin therapy (risk of sev hypokalemia)
Monitor serum K+ _____
4-5
<5 → 20-30
<3.5
q 2-4h
PHOSPHATE
phosphate decreases with _____ therapy
overcorrection can cause severe _____
Repletion may be indicated in patients with … (3)
Consider _____ of potassium phos
insulin
hypocalc
muscle weakness, cardiac/resp dysfx, phos <1
20-30 mmol
BICARBONATE
Consider bicarbonate in patients with pH ____
Dosing → … until pH>^
<7
100 mEq sodium bicarb in 400 mL sterile water q2h
TRANSITIONING TO SQ INSULIN
when hyperglycemic crisis is resolved
Restart home dose or _________
Give SQ insulin _____ prior to DC continuous infusion
0.5-0.8 U/kg/day
2h
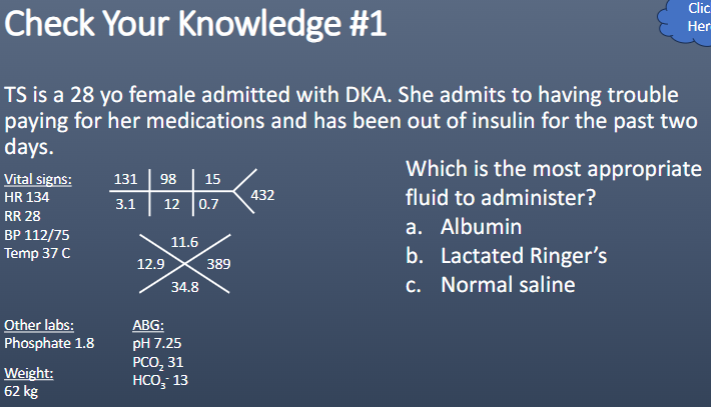
Which is the most appropriate fluid to administer?
a. Albumin
b. Lactated Ringer’s
c. Normal saline
B
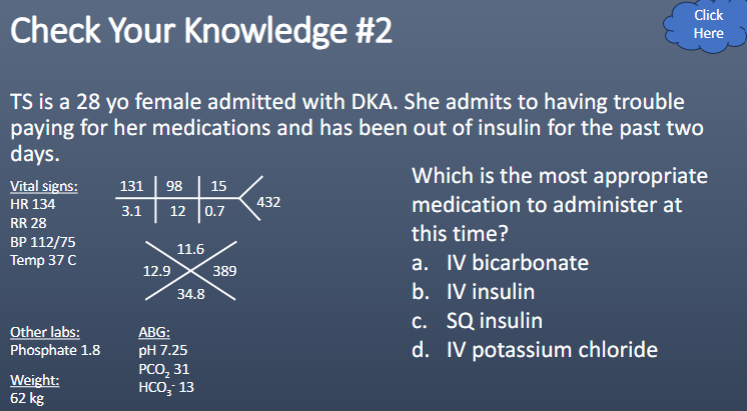
Which is the most appropriate medication to administer at this time?
a. IV bicarbonate
b. IV insulin
c. SQ insulin
d. IV potassium chloride
D
(correct K+ to 3.5 before we start insulin)
T or F:
Intensive insulin therapy is beneficial in critically ill patients.
F
(not beneficial, increases the risk of severe hypoglycemia)
TARGET GLUCOSE RANGES → 3
140-180 → most ICU pts, MICU, SICU, NSICU, etc
110-140 → cardiac surg, only if hypoglycemia is avoided (avoid BG </=70)
>180 → elderly, end of life care
RISK FACTORS FOR HYPOGLYCEMIA
_____ therapy
Interruption of ______
_________ of hypoglycemia
Reduction in ______ doses
________
________
insulin
nutrition
inappropriate mgmt
corticosteroid
renal fail
liver disease
GLYCEMIC CONTROL OF CRITICALLY ILL PATIENTS
Initiate insulin therapy when BG ______ mg/dL
Decrease insulin therapy if BG ______ mg/dL
Avoid ________ in glycemic control
>/= 180
<100
large fluctuations
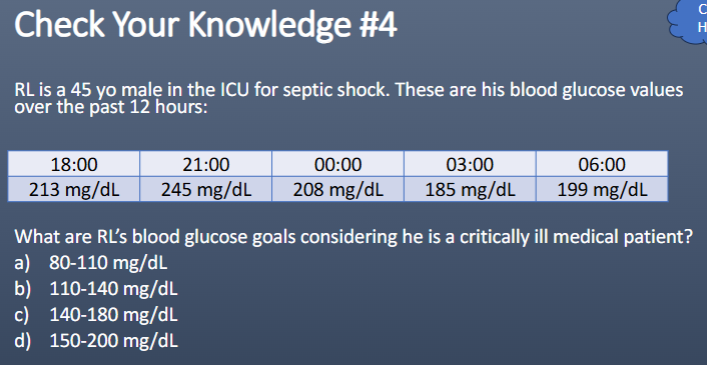
C
INSULIN ROUTES OF ADMIN
When to use …
SQ →
IV →
clinically stable, low insulin req
T1DM, DKA, changing clinical status, uncontrolled on SQ
IV TO SQ INSULIN
Calculate _______
Use ______ of total daily insulin req
Basal only →
Basal bolus →
Overlap SQ basal insulin & insulin infusion for AT LEAST _____
Start ___________ w initiation of SQ regimen
Consider restarting infusion if BG remains _____ mg/dL
24h insulin req
50-75%
insulin NPH in 2 div doses or glargine/detemir qd
50% basal + 50% bolus (div doses)
2h
sliding scale insulin
>300
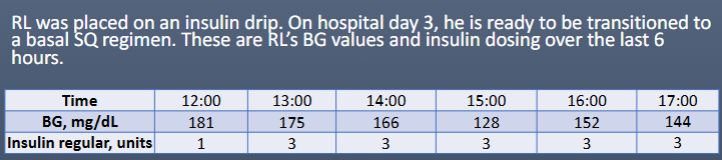
Which SQ insulin regimen is most appropriate?
a) Detemir 60 units SQ daily
b) Glargine 40 units SQ daily
c) NPH 40 units SQ BID
d) Regular 40 units SQ daily
B
(6h = 16U → 16 x 4 = 64 → 50-75% = 32-48U as SQ
NPH BID or glargine/determir qd)
SYMPTOMATIC HYPOGLYCEMIA TX
PO intake →
No PO intake → IV access
No PO intake → no IV access
15g simple carbs → recheck in 15min → if BG<70, repeat cycle
25-50 mL dex 50% IV → recheck in 15min → may repeat 2x → if still <70, start D5W or D10W → recheck in 15min
glucagon 1 mg SQ/IM → recheck in 15min
D
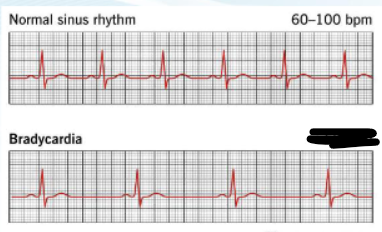
BRADYCARDIA
HR ____ bpm
s/s (unstable) → 5
Treatment →
MOA →
^max cumulative dose of _____
^INEFFECTIVE in _____ and ______
If unresponsive → 3
<60
hypotension, chest pain, dyspnea, AMS, syncope
atropine 1 mg q 3-5min
+SA node firing
3 mg
heart transplant, complete heart block
EP inf 2-10 mcg/min; DA inf 5-20 mcg/kg/min; transcutaneous pacing
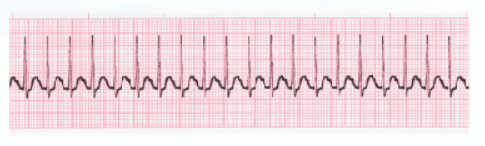
SINUS TACHYCARDIA
HR ____ bpm
s/s → 5
>100
hypotension, AMS, shock, ischemic chest discomfort, acute HF
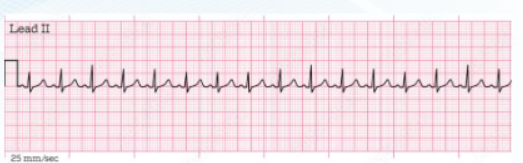
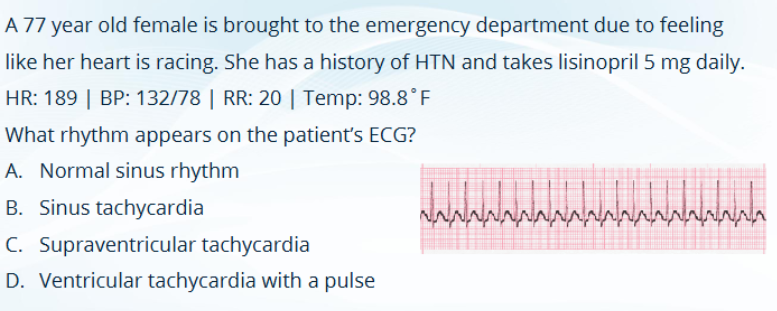
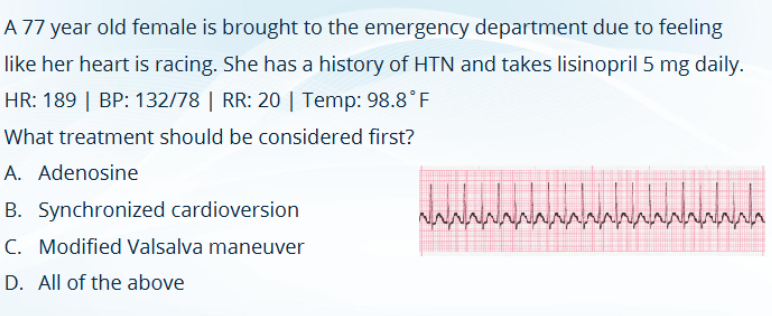
SUPRAVENTRICULAR TACHYCARDIA
HR ____ bpm
______ are 1st line → (4)
______ are 2nd line (^not successful) → dosing
^ MOA
>150
vagal maneuvers → coughing, bearing down, carotid massage, modified valsalva
adenosine → 6 mg IV rapid push initial → 12 mg rapid IV push repeat
-conduction thru SA/AV nodes
Adenosine ADEs → 5
flushing
dyspnea
chest pain
bradycardia
hypotension
ADENOSINE ADMINISTRATION
Administer via IV push over ____
Immediately administer _____ and _______
Use of ______ or ______ is recommended to facilitate faster admin
Administer via ______ as proximal to trunk
→
1-2s
20 mL flush, elevate extremity
T connector, stopcock
peripheral IV
if central → -dose 50%
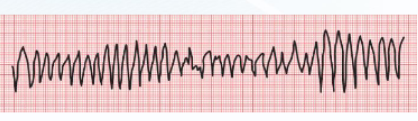
TORSADES DE POINTES
Tachycardia in setting of QTc prolongation
Treatment →
MOA → (3)
magnesium 1-2g IV/IO → push if pt no pulse; inf over 15min if pulse
slow SA node impulse formation, +conduction time, stabilize cardiac memb
QTC PROLONGING DRUG CLASSES → 6
Antiarrhythmics
serotonergics
antimicrobials
antipsychotics
diphenhydramine
methadone
C
C
GOALS OF ACLS
Primary →
Secondary →
Ultimate →
high quality CPR + rapid defib
med admin
ROSC (return of spontaneous circulation)
CPR
compress atleast ____ deep
goal rate _____ bpm
basic airway:
advanced airway (laryngeal mask, laryngeal tube, endotracheal tube):
2 in
100-120
30 comp q 2 breaths
1 breath q 6s
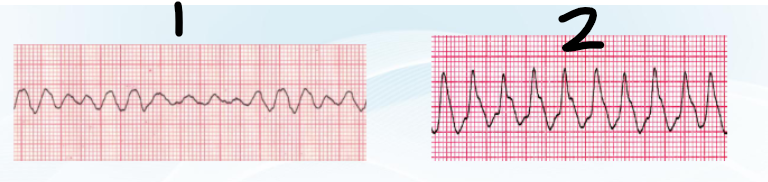
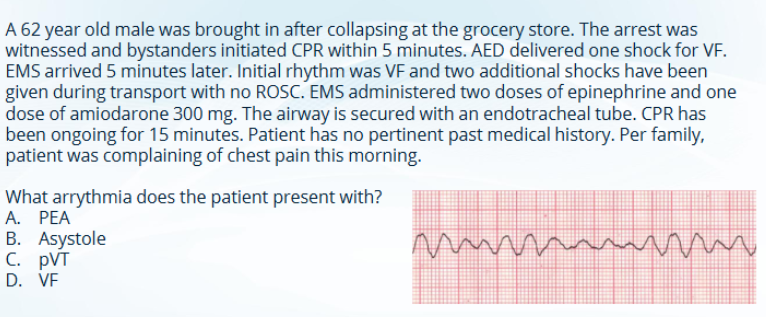
SHOCKABLE rhythms =
VF → no QRS, disorganized, no pulse
pVT → no P, organized, no pulse
SHOCKABLE RHYTHM TX (VT, pVT) → 5
CPR
defib → resume CPR immediately after shock
EP 1 mg IV/IO after 2nd shock → repeat q 3-5min
amiodarone or lidocaine after 3rd shock
continue until ROSC
EPINEPHRINE
MOA →
Dosing →
Continuous infusion at _____ for shock after ROSC
Indicated in shockable or non-shockable rhythm?
alpha/beta agonist
1 mg IV/IO q 3-5min
2-10 mcg/min
both
AMIODARONE
MOA →
Dosing →
→
ADEs → 3
Class III AA, K+ blocker
VF/pVT → 300 mg IV push followed by 150 mg IV push
tachycardia+pulse → 150 mg IV inf over 10min followed by cont inf
hypotension, bradycardia, +QTc
LIDOCAINE
MOA →
Dosing →
Max dose →
Could consider infusion after ROSC
Class IB AA, Na+ blocker
1-1.5 mg/kg IV bolus followed by 0.5-0.75 mg/kg q 5-10min
3 mg/kg
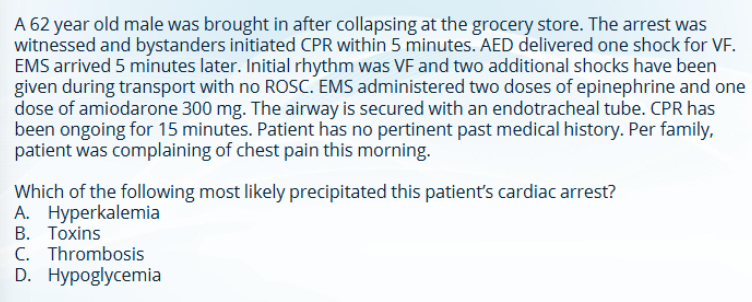
REVERSIBLE CAUSES of cardiac arrest
H’s → 6
T’s → 5
hypovolemia, hypoxia, H+ (acidosis), hypo/hyperK, hypothermia, hypoglycemia
tension pneumothorax, tamponade (cardiac), toxins, thrombosis, trauma
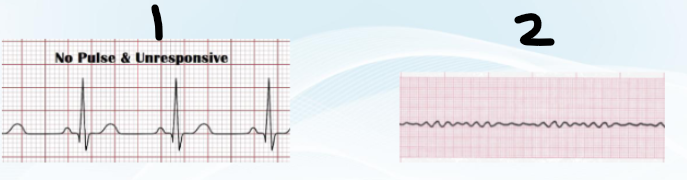
NON-shockable rhythms
PEA → electrical present, no pulse
asystole → no electrical, no pulse
NON-SHOCKABLE RHYTHM (PEA, asystole) TX
high quality CPR
EP 1 mg IV/IO q 3-5min
continue until rhythm shockable/ROSC
D
C
OTHER MEDICATIONS IN ACLS
Calcium Chloride
MOA →
Indications →
Dosing →
No benefit in cardiac arrestEnsure ________ btwn calcium & sodium bicarb admin
stabilize cardiac memb, +inotropy
hypoCa, hyperK, CCB/BB tox, massive transfusion protocol
1g IV push
line is flushed
OTHER MEDICATIONS IN ACLS
Dextrose
Indications →
Dosing →
No benefit in cardiac arrest
hypoglycemia
25-50g IV push
OTHER MEDICATIONS IN ACLS
Naloxone
MOA →
Indications →
Dosing →
May be administered via … (5)
opioid antag
opioid overdose or resp arrest
0.4-2 mg, repeat as indicated
IV, IO, IM, intranasal, ET tube
OTHER MEDICATIONS IN ACLS
Sodium Bicarbonate
MOA →
Indications → 4
Dosing →
________ is not recommended
buffers pH, move K+ into cell
MA, hyperK, certain overdoses, prolonged resus efforts
50 mEq IV/IO
routine admin
Any medication administered IV can be given ____
IO
What drugs can be administered ET?
naloxone
atropine
vasopressin
EP
lidocaine
Doses of drugs administered via ET is __________ (EXCEPT ______)
2-2.5x IV route, vasopressin
VASOPRESSIN
MOA →
Indications →
Dosing →
ADH analog
vasodilatory shock RF to fluid resus+catechol, IHCA w EP+steroids
20-40U IV/IO
TARGETED TEMP MANAGEMENT
Intentional cooling of a patient to a goal of ____________
Consider for any patient who is _____ and ______ to verbal commands after ROSC
Thought to improve neurologic fx and survival after cardiac arrest
32-37.5C for atleast 24h
comatose, unresponsive