Q8 - ICS III Final Study guide
1/239
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
240 Terms
What is bacteremia vs septicemia?
Bacteremia: transient load of bacteria in the blood stream
Septicemia: chronic load of bacteria in the blood
Why is antibiotic prophylaxis done?
Aimed to prevent bacteremia from reaching a site of compromised blood flow (artificial join or heart valve) to prevent infection
What does cellulitis indicate?
Infection that is not localized but is acute and spreading
What does an abscess indicate?
Infection that is localized, walled off, and filled with pus
T or F
Antibiotics are very effective against abscesses.
False; Due to poor blood supply antibiotics have minimal effect
What is the treatment for abscesses?
Incision and drainage
Remove source of infection
What is pathogenesis of a bacteria determined by?
- Quantity
- Virulence of bacteria
What percent of odontogenic infections are mixed anaerobic and aerobic?
60%
What aerobic bacteria make up the majority of infections?
- Streptococcus (90%)
- Staphylococcus (10%)
What anaerobic bacteria make up the majority of infections?
- Gram + peptostreptococci
- Gram - prevotella
Odontogenic infections are initiated by ________ bacteria.
aerobic
What is alveolar osteitis?
AKA dry socket
- Occurs when pathogens contribute to loss of clot
- Collagenase produced by bacteria destroy clot
What type of streptococcus causes endocarditis post dental treatment?
Alpha hemolytic Strep viridans
What is the problem with treating staphylococcus infections?
Most are resistant to penicillin due to penicillinase enzyme that breaks down antibiotic
What is prevotella buccae resistant to ?
Clindamycin
Describe bacterial exotoxins
- Easily destroyed at body temp
- High toxicity
- Mostly from gram + bacteria
Describe bacterial endotoxins
- Stable and can withstand autoclaving
- Low toxicity
- Mostly from gram - bacteria
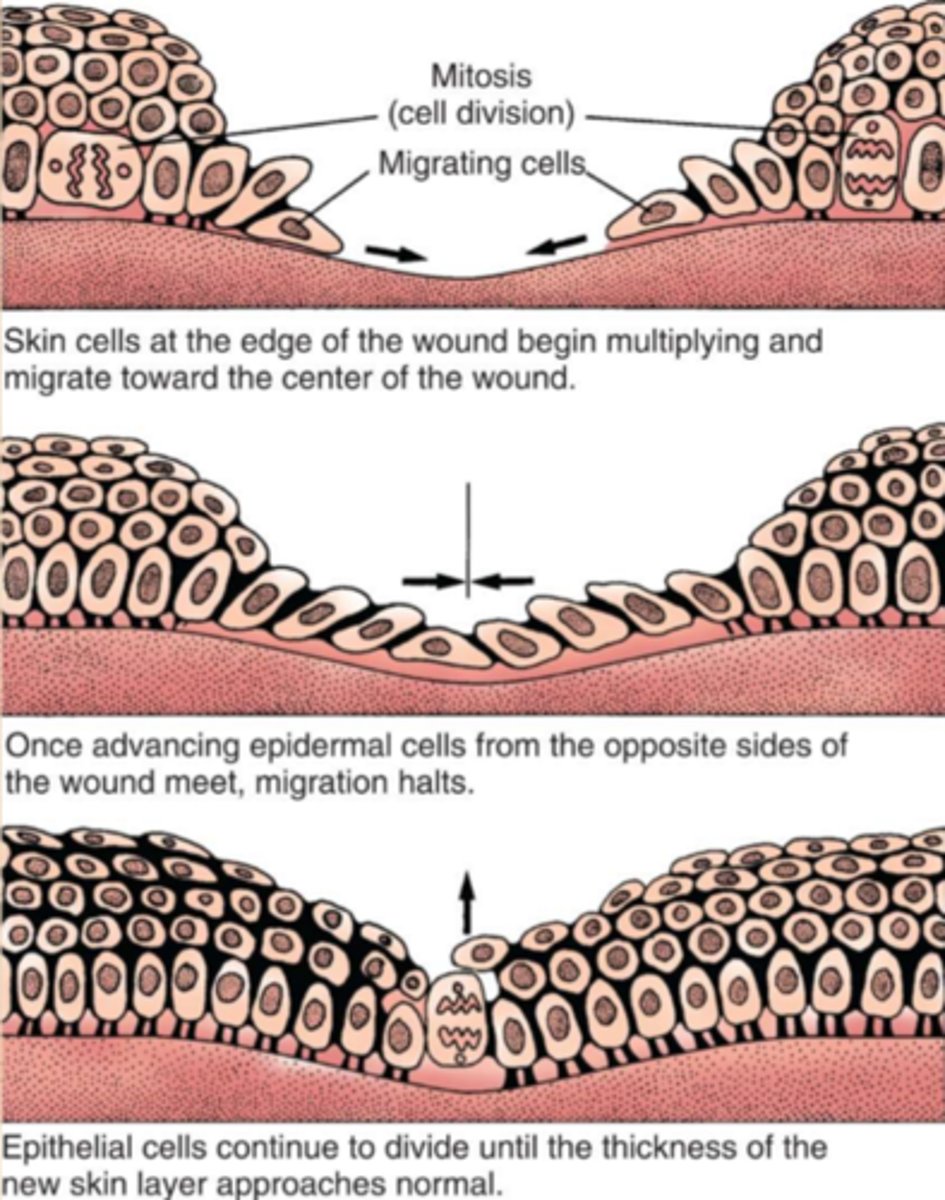
How do wounds re-epithelialize?
The sides grow towards the middle like a volcano
How do you perform source control on an odontogenic infection?
- Extraction
- Decrease
- Release pus and bacterial byproducts (Incise and drain)
T or F
You should perform I&D during abscess stage ONLY, NOT cellulitis.
False; Perform I&D during either cellulitis or abscess stage to stop progression of infection
What should you keep in mind when doing I&D?
- Incise healthy skin
- Full thickness mucoperiosteal flap
- Explore entire infected space
When should you extract a tooth causing an odontogenic infection?
- If it is nonrestorable
- Remove ASAP to remove source
When do buccal space infections occur?
- Apices above/below buccinator muscle attachments
When do sublingual space infections occur?
- When infection drains above the mylohyoid muscle
- Usually mandibular teeth
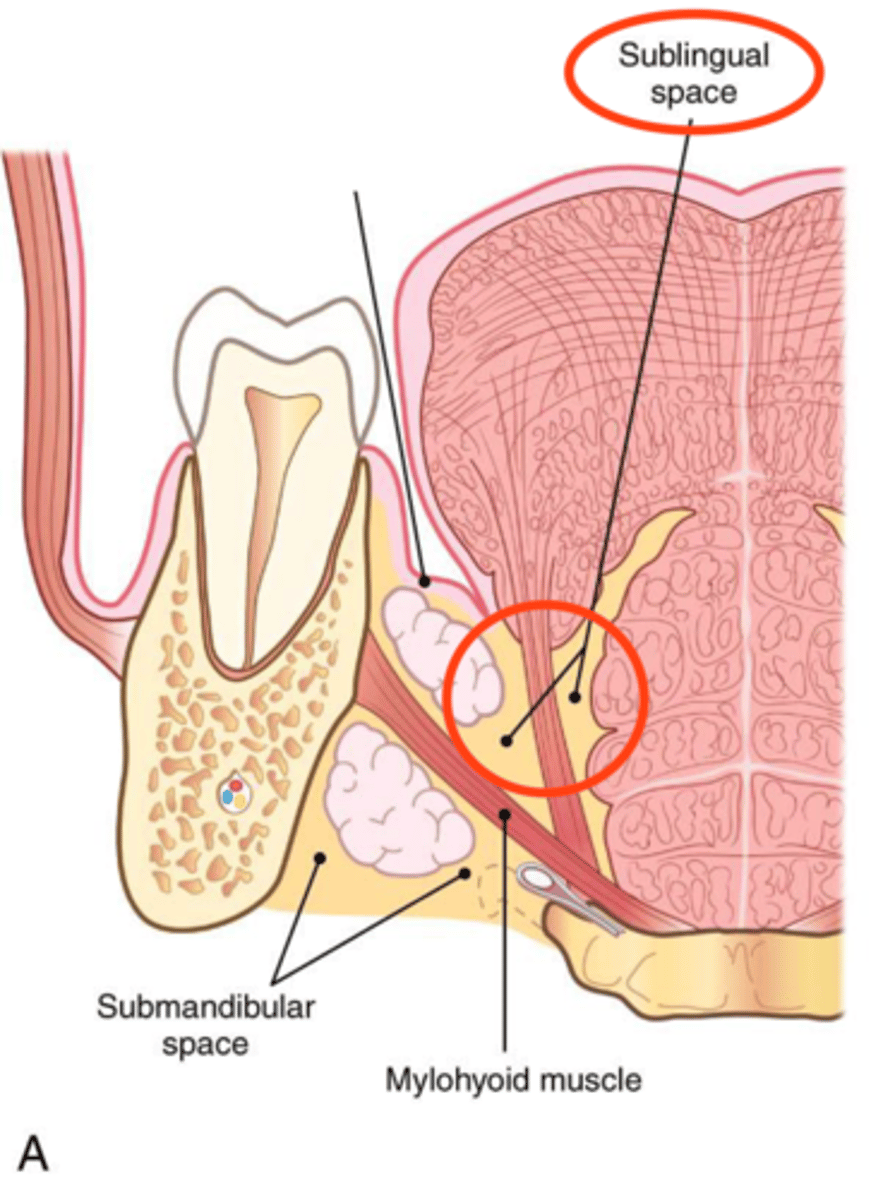
What space communicate with sublingual space?
- Submandibular space
When do submandibular space infections occur?
- When infection drains below the mylohyoid muscle
Where do submandibular space infections tend to spread?
- Extend medially and posterior towards digastric muscle and hyoid
T or F
The Submental space is not commonly the solely infected space.
True
What is the canine space?
- Muscular space
- Bordered by Levator anguli oris and levator labii superioris
- Often invades orbit
Where do maxillary infections tend to drain?
- Posterior
- Superior
What is cavernous sinus thrombosis?
- Orbital cellulitis that travels through angular veins to cavernous sinus
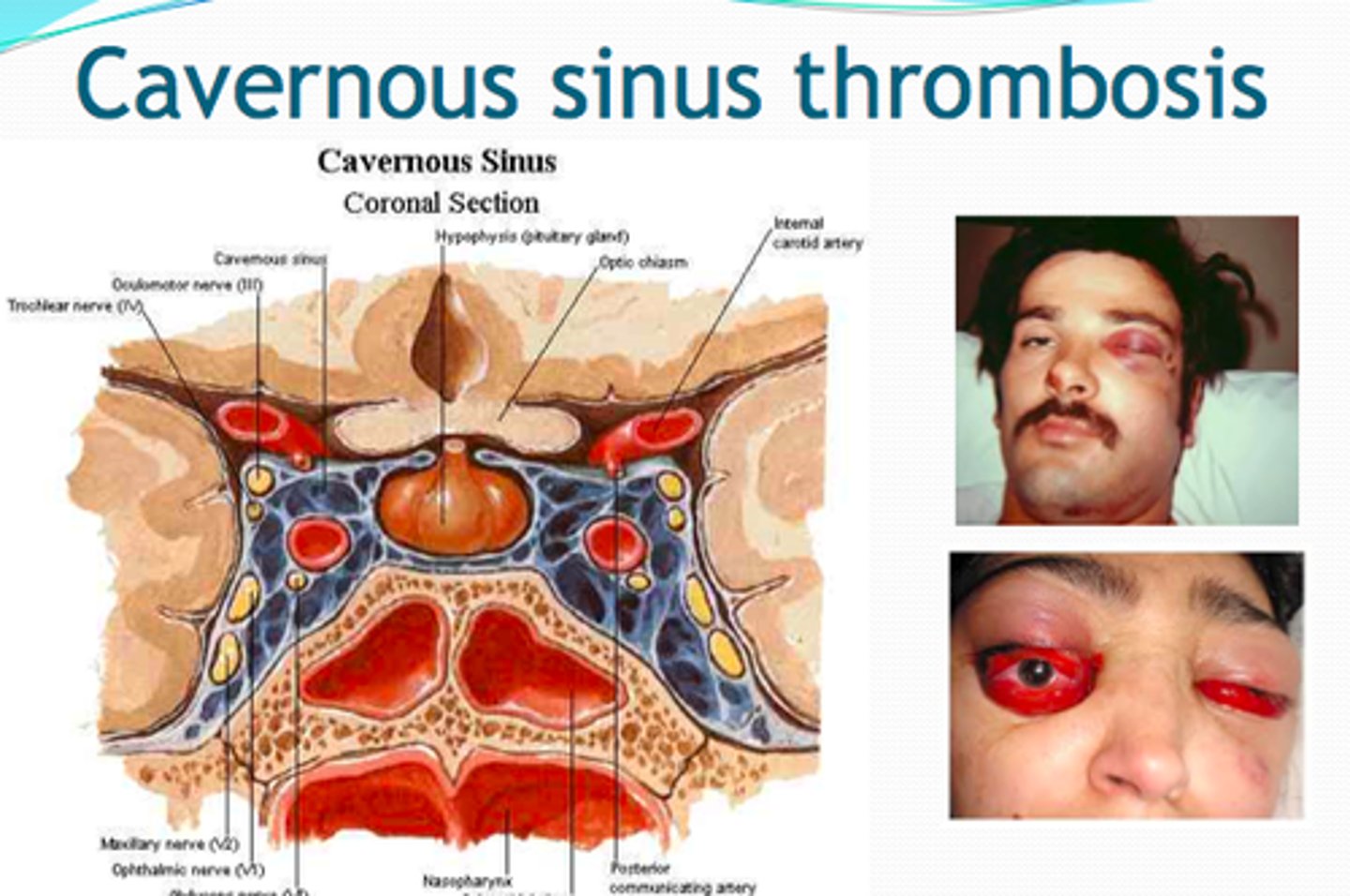
Why does cavernous sinus thrombosis occur?
Veins of the face lack valves so retrograde infection is quite easy
What are signs and symptoms cavernous sinus thrombosis?
- Proptosis
- Fever
- Altered state of consciousness
- Orbital cellulitis

What are contents in the cavernous sinus?
- CN III
- CN IV
- CN V1 and V2
What space infections are often associated with trismus?
- Masticator space
- Temporal space
- Masseteric space
What defines the masticator space?
Split in deep cervical fascia at inferior of mandibular border
What are common symptoms for Masticator space infections?
- Trismus
- Pin
- Swelling
What space do we inject during an IA block?
Pterygomandibular space
T or F
Pterygomandibular space infections can present as trismus without swelling.
True
Where do mandibular infections tend to drain?
- Posterior
- Inferior
What is Ludwig's angina?
Bilateral cellulitis that has spread from submandibular, sublingual, and submental spaces
What is the main concern with Ludwig's angina?
Occlusion of airway
What are the clinical signs of Ludwig's angina?
- FOM hard and elevated
- Tongue filling mouth
- Difficulty breathing and swallowing
What is the old belief regarding extracting teeth that are acutely infected?
It used to be thought that extracting acutely infected teeth would lead to spread of infection
What should be done if a tooth is acutely infected and causing a space infection?
- Extract tooth as soon as possible
- I &D and Antibiotics if indicated
T or F
More than half of these severe odontogenic infections are caused by aerobic bacteria.
False; More than half of infections are caused by anaerobic bacteria
What are some life threatening complications from odontogenic infections?
- Airway obstruction
- Sepsis
- Mediastinitis
- Brain abscess
- Jugular vein thrombosis
What are the treatment options for deep neck infections?
- Immediate I&D
- Intervenous antibiotics
What was the old thought behind I&D for cellulitis and abscesses?
- Fluctuant abscess swelling would be I&D
- Cellulitis would receive antibiotics
How do you tell the difference between cellulitis vs abscess?
- Duration
- Pain
- Size
- Localization
- Pus is the main indicator
What are the two ways you can differentiate cellulitis and abscesses?
- Presence of pus upon I&D
- Contrast enhanced CT
What is the fear behind not treating cellulitis?
Further spread of infection
What was found during a study regarding accuracy to clinically determine abscess vs cellulitis?
Majority of odontogenic abscesses were underestimated to be cellulitis
What was found when reviewing the literature on whether or not to drain abscesses and cellulitis in odontogenic infection?
Differentiating between cellulitis and abscess is less important -> Immediate treatment (I&D) is most important
How can cellulitis be treated if it is correctly diagnosed in a stable patient?
IV antibiotics are sufficient
What antibiotic works against all oral pathogens?
No single antibiotic works for all pathogens due to the polymicrobial nature of odontogenic infections
When is penicillin not effective in odontogenic infections?
- 21% of the time
- Common in severe hospitalized cases
What are the first line antibiotics used for outpatient treatment of infections?
- Amoxicillin
What are the first line antibiotics used for outpatient treatment of infections if the patient is allergic to penicillin?
- Clindamycin
- Azithromycin
What are the first line antibiotics used for inpatient treatment of infections?
- Ampicillin/Sulbactam
- Clindamycin
- Penicillin + Metronidazole
What works better, short course or long course antibiotics?
It was shown there were no difference in cure rates as long as surgical treatment was done (so go with short term)
What are the advantages of short course antibiotic therapy?
- Fewer side effects
- Lower risk of resistance
- Higher compliance
What is the most cost effective antibiotic?
Amoxicillin
How should providers choose antibiotics?
- Bacteria susceptibility
- Cost
- Safety
What have laboratory studies shown in terms of bacteria susceptibility in odontogenic infections?
Newer and broader spectrum antibiotics are more effective
What was found comparing resistance of bacteria in outpatient infection vs inpatient infections?
Much higher rate of penicillin resistance in severe hospitalized cases
What is a biofilm?
community of bacteria embedded in a extracellular matrix
T or F
Most bacteria exist in a biofilm.
True
What percent of biofilm are actual bacteria?
15%
What are the benefits for bacteria being in a biofilm?
- Evade antibiotics
- Immune cells can't penetrate entire biofilm
- Quorum sensing allows entire biofilm to change gene expression depending on environment
Do antibiotics work against biofilms?
- May kill surface bacteria but unable to penetrate and kill deep bacteria
- Cause for recurrent infections
How do biofilms explain the need for I&D and source removal?
Antibiotics alone cant kill space infection biofilms, therefore debridement and drainage are NECESSARY
There are many diseases of the mouth that are caused by biofilms of bacteria. What is the common treatment for all these diseases? (ex. periodontitis, osteomyelitis, pulpitis, MRONJ)
Debridement! This is the only way to erradicate a biofilm since antibiotics won't work
What kind of bacteria do antibiotics help with?
Planktonic AKA free floating
What species tends to become virulent in post extraction sites?
Prevotella
What puts a patient at high risk for prevotella infection post-ext?
- Excessive plaque
- Nearby gingivitis
- Periodontitis
- Immunocompromised patients
What antibiotics resolves most post-extraction infections caused by prevotella species?
Metronidazole
What prevotella strain was found in odontogenic infections and pericoronitis that was resistant to empirical antibiotics?
Prevotella buccae
T or F
Prevotella bacteria are not common inhabitants of the oral cavity but are often introduced during extractions.
False; They are normal inhabitants of the periodontal sulcus
What is the most common facultative anaerobic species in odontogenic infections?
Viridans streptococci
What are the most common obligate anaerobic bacteria in odontogenic infections?
- Bacteriodes
- Prevotella
- Peptostreptococci
T or F
Deep space infections of the neck are most commonly from odontogenic origin.
True
What are the main principles of source control?
- Decreased bacterial load via I&D
- Drain swelling and pus to improve blood supply
- Irrigate to remove bacteria and toxins
- Extract tooth
What are the most common causes of odontogenic infections?
- Caries (65%)
- Pericoronitis
- Periodontitis
What was found regarding Prevotella intermedia and its effects on the immune system?
- inhibit proliferation of B-cells and T cells leading to immunosuppression
- Shields bacteria from humoral response
- Degrades antibodies
- Degrades compliment
Where is P. buccae normally found?
- Peri-implant bone
- Periodontitis
- Root canal infections
- Radicular cysts
What happens to opportunistic pathogens after a few days of antibiotic prophylaxis?
Resistance was observed along with ecological disturbance
T or F
Clindamycin is always effective against all prevotells species.
False
What is a good first line empiric antibiotic to prescribe if Prevotella is suspected?
Penicillin plus Flagyl (metronidazole)
What kind of antibiotic is metronidazole?
- Nitroimidazole
- Antibiotic and antiprotozoal
What is the first choice for treatment of C. difficile?
Metronidazole
How does Metronidazole work?
forms free radical toxic metabolites in bacterial cell that damage DNA
What is the risk of taking Metronidazole?
- Disulfiram-like reaction with alcohol
- Symptoms include nausea, vomiting, respiratory depression, death
What should be determined before prescribing B-lactam antibiotics?
Ability of bacteria to produce B-lactamase; this is to avoid potential antibiotic resistance
What bacteria species produce B-lactamase the most?
Prevotella
What kind of bacteria does Metronidazole work on?
Anaerobic bacteria only
What antibiotics are prevotella species most susceptible to?
- Amoxicillin + clavulanic acid
- Metronidazole
- Clindamycin
What should be done if a single opportunistic organism dominates a culture from an infection?
Suscpetibility testing should be performed and then the appropriate antibiotic prescribed
What should be used if Metronidazole does not cure a complicated anaerobic infection?
Meropenem
What antibiotics are Prevotella species resistant to?
Beta lactam antibiotics (-cillins) and Clindamycin