chapter 19 thorax and lungs
1/107
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
108 Terms
Functions of the respiratory system:
Supplies oxygen to the body for energy production
Removes carbon dioxide as a waste product of energy reaction
Maintains homeostasis (acid base balance) in arterial blood
Maintains heat exchange
By supplying O2 to the blood and eliminating excess CO2, respiration maintains the pH or the acid/base balance of the blood)
Structure and function of thoracic
Thoracic cage is a bony structure with a conical shape, which is narrower at top
Defined by sternum, 12 pairs of ribs, and 12 thoracic vertebrae
- 1-7 ribs attach to sternum by costal cartilages
- Ribs 8-10 attach to costal cartilage above
- Ribs 11 and 12 are “floating,” with free palpable tips.
The costochondral junctions are the points at which the ribs join their cartilages. They are not palpable
Suprasternal Notch
shaped depression just above sternum between clavicles
sternum
breastbone
also has:
manubrium
body
xiphoid process
Costal angle
the right and left costal margins form an angle where they meet at xiphoid process
90 degrees
Manubriosternal angle: “Angle of Louis”
located in the second intercostal space in the rib
marks site of tracheal bifurcation into right and left main bronchi
rationale: The sternal angle marks the site of tracheal bifurcation into the right and left main bronchi; it corresponds with the upper borders of the atria of the heart, and it lies above the fourth thoracic vertebra on the back
Evaluate presence and quality of normal breath sounds both anterior, laterally and posterior
Use flat diaphragm of stethoscope and listen to at least one full respiration in each location
Sputum of
pulmonary edema
Tuberculosis
Croup
Viral infection
PE= pink and frothy
TB=rust-colored sputum
Croup= barking cough not spectrum production
viral infections= white or clear mucoid sputum
apex of the lungs
highest point, of lung tissue is 3 to 4 cm above the inner third of the clavicles
apices of the lungs
the apices are at the level of C7.
base
rests on the diaphragm at about the 6th rib in the midclavicular line. Laterally lung tissue extends from the apex of the axilla down to the 7th or 8th rib
What is the correct method to use when progressing from one auscultatory site on the thorax to another
start at the apices and percuss the band of normally resonant tissue across the tops of both shoulders Then, percussing in the interspaces, make a side-to-side comparison all the way down the lung region. Percuss at 5-cm intervals. Avoid the damping effect of the scapulae and ribs
Resonance
low-pitched, clear, hollow sound that predominates in healthy lung tissue in the adult
can be duller in the athlete
Assess tactile (or vocal) fremitus
Fremitus is a palpable vibration.
using 2 hands to palpate for sound
Sounds generated from the larynx are transmitted through patent bronchi and the lung parenchyma to the chest wall, where you feel them as vibrations
-most intensely Between the scapulae and sternum (major bronchi are closest to chest wall)
severe asthma. Air passing through narrowed bronchioles would produce which of these adventitious sounds
wheezing
Wheezes are caused by air squeezed or compressed through passageways narrowed almost to closure by collapsing, swelling, secretions, or tumors, such as with acute asthma or chronic emphysema
normal lung for comparison
inspection
palpation
percussion
auscultation
adventitious sounds
inspections: ap is greater than transverse diaper, 10-20 breaths/mins no cyanosis/pallor
palpation: symmetric chest expansion tactile remits present and equal bilaterally
percussion: resonant
auscultation: vesicular over peripheral fields, bronchovesicular anterior and between scapulae and posterior, infants bronchovesicular thought
crackles, is not pathologic. crackles are short, popping, crackling sounds that last only a few breaths
collapsed section of the alveoli
Inspection: a cough, a faster heart and breathing rate, cyanosis
Palpation:Chest expansion decreased on affected side. Tactile fremitus decreased or absent. With large collapse, tracheal shift toward affected side
Percussion: Dullness over area
Auscultation: Breath sounds decreased vesicular or absent over area
atelacsis (collapse)
inspection: cough initially nonproductive later purulent yellow green sputum
palpation: skin moist a night from nigh swearts
percussion: resonant initially dull over effusion
auscultation: normal/dereased vesicular breath sounds
adventitious sounds: crackles over upper lobes
tuberculosis
subjective: chest pain worse on deep inspiration, dyspenea
inspection: restles, aniety, cyanosis tachypnea,
palpation: diaphoresis (sweating) , hypotension
auscultation: tachycardia, accentuated pulmonic component of S2
adventitious sounds: crackles, wheezes
pulmonary embolism
An acute infection of the trachea and larger bronchi characterized by cough, lasting up to 3 weeks.
Inspection Cough is productive or nonproductive. Also sore throat, low-grade fever, postnasal drip, fatigue, substernal aching.
Palpation No pain, no increased fremitus.
Percussion Resonance predominates.
Auscultation May be clear and equal bilaterally. No egophony.
Adventitious sounds: no
acute bronchitis
CA type of (COPD), g.
Inspection: rasping cough productive of thick mucoid sputum. Chronic—dyspnea, fatigue, cyanosis, possible clubbing of fingers.Acute exacerbations may have worsening dyspnea and increased cyanosis
Palpation: Tactile fremitus normal.
Percussion:Resonant.
AuscultationNormal vesicular. Voice sounds normal. Chronic—prolonged expiration.
Adventitious Sounds: Crackles over deflated areas. May have wheeze, especially with acute exacerbation.
Chronic bronchitis has a history of productive cough for 3 months of the year for 2 years in a row
Chronic Bronchitis
A patient has been admitted to the emergency department for a suspected drug overdose. Respirations are shallow, with an irregular pattern, at a rate of 12 respirations per minute. The nurse interprets this respiration pattern as which of the following?
Chronic obstructive breathing
Bradypnea
Cheyne-Stokes respirations
Hypoventilation
Hypoventilation is characterized by an irregular, shallow pattern, and can be caused by an overdose of narcotics or anesthetics. Bradypnea is slow breathing, with a rate less than 10 respirations per minute. Cheyne-Stokes respirations are a cycle in which respirations gradually wax and wane in a regular pattern, increasing in rate and depth and then decreasing. Chronic obstructive breathing is characterized by normal inspiration and prolonged expiration to overcome increased airway resistance. This patient’s breathing is hypoventilation.
normal finding when assessing the respiratory system of an older adult
Decreased mobility of the thorax
The costal cartilages become calcified with aging, resulting in a less mobile thorax and thus also a slight decrease, not increase, in thoracic expansion
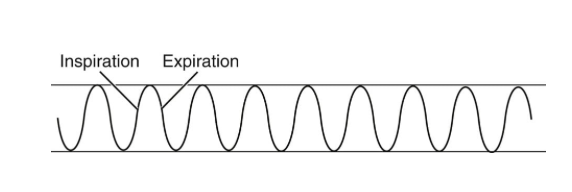
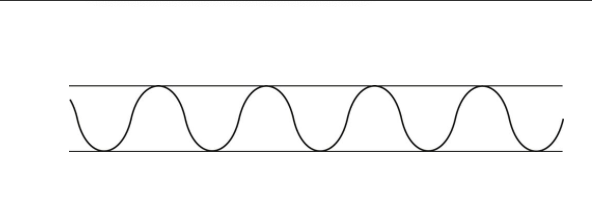
normal adult for comparison
Rate—10 to 20 breaths/min
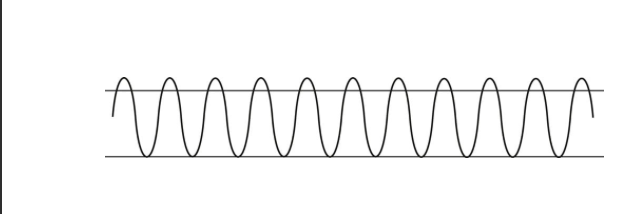
hyperventilation
increases in both rate and dept
tachypnea
Rapid, shallow breathing. Increased rate, >24 per minute
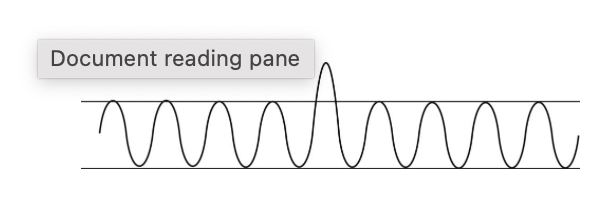
sigh
Occasional sighs punctuate the normal breathing pattern and are purposeful to expand alveoli. Frequent sighs may indicate emotional dysfunction and also may lead to hyperventilation and dizziness.
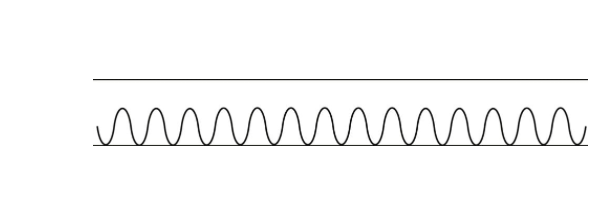
bradypynea
Slow breathing. A decreased but regular rate (<10 per minute),
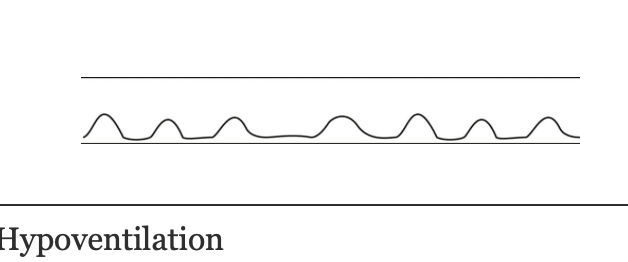
hypoventilation
An irregular shallow pattern caused by an overdose of narcotics or anesthetics
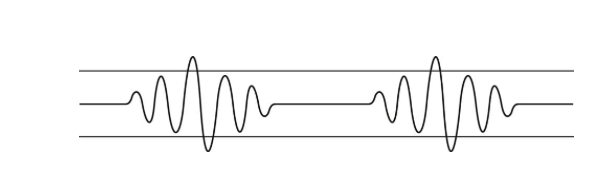
Cheyne-Stokes Respiration
respirations are a cycle in which respirations gradually wax and wane in a regular pattern, increasing in rate and depth and then decreasing
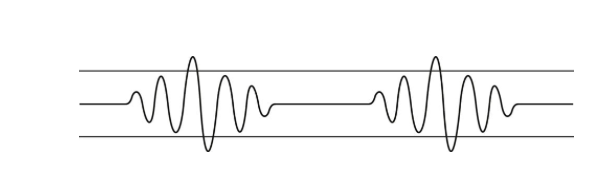
Biot Respiration
Similar to Cheyne-Stokes respiration, except that the pattern is irregular. A series of normal respirations (3 to 4) is followed by a period of apnea
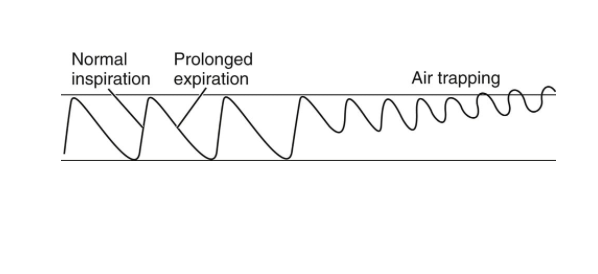
Chronic Obstructive Breathing
Normal inspiration and prolonged expiration to overcome increased airway resistance
subjective data
Cough: Acute cough lasts less than 2 or 3 weeks; chronic cough lasts over 2 months
2. Shortness of breath: Orthopnea is difficulty breathing when supine, State number of pillows needed to achieve comfort (e.g., “two-pillow orthopnea
Paroxysmal nocturnal dyspnea is awakening from sleep with SOB and needing to be upright to achieve comfort
3. Chest pain with breathing
4. History of respiratory infections
5. Smoking history
6. Environmental exposure: self care
7. Patient-centered care
Voice sounds
are not elicited routinely
testing for the possible presence of bronchophony, egophony, and whispered pectoriloquy
Normal voice transmission is soft, muffled, and indistinct; you can hear sound through the stethoscope but cannot distinguish exactly what is being said.
Muffled voice sounds and symmetric tactile fremitus
Bronchophony
repeat “ninety-nine” while you listen with the stethoscope over the chest wall
abnormal: you auscultate a clear “ninety-nine
Egophony
Greek: “the voice of a goat
Auscultate the chest while the person phonates a long “ee-ee-ee-ee” sound
abnormal: “eeee” sound changes to a bleating long “aaaaa” sound
Whispered Pectoriloquy
Ask the person to whisper a phrase such as “one-two-three” as you auscultate
abnormal: the whispered voice is transmitted very clearly and distinctly, although still somewhat faint
assessment of the left lung
The left lung has two lobes and is longer and narrower than the right lung.
It is narrower than the right lung because the heart bulges to the left. fissures
The right lung has three lobes and is shorter than the left lung because of the underlying liver. The posterior chest is almost all lower lobes.
What are the primary muscles involved in normal respiration?
diaphragm and intercostals
The major muscle of respiration is the diaphragm and the intercostal muscles are also involved in respiration as they lift the sternum and elevate the ribs during inspiration, increasing the anteroposterior diameter.
Expiration is primarily passive. Forced inspiration involves the use of other muscles, such as the accessory neck muscles—sternomastoid, scaleni, and trapezii muscles. Forced expiration involves the abdominal muscles
symptoms of a cough associated with rust-colored sputum, low-grade afternoon fevers, and night sweats for the past 2 months. Based on these findings, what is the most likely cause
Tuberculosis
TB often produces rust-colored sputum in addition to other symptoms of night sweats and low-grade afternoon fevers
Hemoptysis (sputum)
(1) white or clear mucoid—colds, bronchitis, viral infections;
(2) yellow or green—bacterial infections;
(3) rust colored—TB, pneumococcal pneumonia;
(4) pink, frothy—pulmonary edema, some sympathomimetic medications have a side effect of pink-tinged mucus
Hyperresonance
Hyperresonance is a lower-pitched, booming sound found when too much air is present such as in emphysema or pneumothorax.
A dull note (soft, muffled thud) signals abnormal density in the lungs, as with pneumonia, pleural effusion, atelectasis, or tumor
low-pitched, soft breath sounds are heard over the posterior lower lobes, with inspiration being longer than expiration
Vesicular breath sounds that are normal in that location
Vesicular breath sounds are low-pitched, soft sounds with inspiration being longer than expiration. These breath sounds are expected over the peripheral lung fields where airflows through smaller bronchioles and alveoli. Normally harsh, hollow, or tubular sounds (bronchial breath sounds) are heard over the trachea. Vesicular breath sounds, not bronchial or bronchovesicular breath sounds, are normally heard over the posterior lower lobes
aging adult
The costal cartilages become calcified; thus the thorax is less mobile
decrease in elastic properties within the lungs, making them less distensible and lessening their tendency to collapse and recoil
decrease number of alveoli therefore less surface area is available for gas exchange therefore increase in dyspnea
Condition: Infection in lung parenchyma leaves alveolar membrane edematous and porous; thus red blood cells (RBCs) and white blood cells (WBCs) pass from blood to alveoli. Alveoli progressively fill up (become consolidated) with bacteria, solid cellular debris, fluid, and blood cells, which replace alveolar air.
Subjective: Fever, cough with pleuritic chest pain, chills, SOB, fatigue, malaise.
Inspection: Increased respirations >24/min. Guarding and lag on expansion on affected side. Children—Sternal retraction, nasal flaring. Cyanosis with severe illness. Possible hypotension.
Palpation: Chest expansion decreased on affected side. Tactile fremitus increased if bronchus patent, decreased if bronchus obstructed.
Percussion: Dull over lobar pneumonia.
Auscultation: Tachycardia. Loud bronchial breathing with patent bronchus. Voice sounds have increased clarity; bronchophony, egophony, whispered pectoriloquy present. Children—Diminished breath sounds may occur early.
Adventitious Sounds: Crackles, fine to medium.
Lobar Pneumonia
Condition: Pump failure causes increased backward pressure toward the pulmonary circulation, leading to pulmonary vascular congestion (engorgement of pulmonary capillaries).
Inspection: Increased respiratory rate, SOB on exertion, orthopnea, paroxysmal nocturnal dyspnea, nocturia, ankle edema, pallor in light-skinned people. In acute heart failure, may have pulmonary edema with pink, frothy sputum.
Palpation: Skin moist, clammy. Tactile fremitus normal.
Percussion: Resonant.
Auscultation: Normal vesicular. Heart sounds include S3 gallop.
Adventitious Sounds: Crackles at lung bases
Heart Failure
Condition: Free air in pleural space causes partial or complete lung collapse. Air in pleural space neutralizes or reverses the usual negative pressure present; thus lung collapses. Usually unilateral. can be (1) spontaneous (air enters pleural space through rupture in lung wall, (2) traumatic (air enters through opening or injury in chest wall), or (3) tension (trapped air in pleural space increases, compressing lung and shifting mediastinum to the unaffected side).
Inspection: Unequal chest expansion. If large, tachypnea, cyanosis, apprehension, bulging interspaces.
Palpation: Tactile fremitus decreased or absent. With tension pneumothorax, may see tracheal shift to opposite (unaffected) side. Chest expansion decreased on affected side.
Percussion: Hyperresonant.
Auscultation: Breath sounds decreased or absent. Voice sounds decreased or absent.
Adventitious Sounds: None
Pneumothorax
Conditio: nCollection of excess fluid in the intrapleural space, with compression of overlying lung tissue. may contain watery capillary fluid
Inspection: Increased respirations, dyspnea; may have dry cough, tachycardia, cyanosis, asymmetric expansion, abdominal distention.
Palpation: Tactile fremitus decreased or absent. Tracheal shift away from affected side. Chest expansion decreased on affected side.
Percussion":Dull on affected side.
Auscultation:Breath sounds decreased or absent. Voice sounds decreased or absent. When remainder of lung is compressed near the effusion, may have bronchial breath sounds over the compression along with bronchophony, egophony, whispered pectoriloquy.
Adventitious Sounds:Crackles, pleural rub
Pleural Effusion (Fluid
Condition: An allergic hypersensitivity to certain inhaled allergens (pollen), irritants (tobacco, ozone), microbes, stress, or exercise that produces a complex response characterized by bronchospasm and inflammation, edema in walls of bronchioles, and secretion of highly viscous mucus into airways. These factors greatly increase airway resistance, especially during expiration, and produce the symptoms of wheezing, dyspnea, and chest tightness.
Inspection: During severe attack: increased respiratory rate, SOB with audible wheeze, use of accessory neck muscles, cyanosis, apprehension, retraction of intercostal spaces. Expiration labored, prolonged. When chronic, may have barrel chest.
Palpation:Tactile fremitus decreased, tachycardia.
Percussion:Resonant. May be hyperresonant if chronic.
Auscultation:Diminished air movement. Breath sounds decreased, with prolonged expiration. Voice sounds decreased.
Adventitious Sounds:Bilateral wheezing on expiration, sometimes inspiratory and expiratory wheezing
Asthma (Reactive Airway Disease)
fine crackles
pneumonia, bronchiolitis, or atelectasis
The nurse is reviewing the characteristics of breath sounds. Which statement about bronchovesicular breath sounds is true?
Expected near the major airways
Bronchovesicular breath sounds are moderate in pitch and amplitude and are equal in length in inspiration and expiration. They are heard over major bronchi where fewer alveoli are located posteriorly—between the scapulae, especially on the right; and anteriorly, around the upper sternum in the first and second intercostal spaces. The other responses are not correct
Conditions with characteristic timing of cough
(1) continuous throughout day—acute illness (e.g., respiratory infection);
(2) afternoon/evening—may be exposure to irritants at work;
(3) night—postnasal drip, sinusitis;
(4) early morning—chronic bronchial inflammation of smokers
what is the costochondral junctions
are the points at which the ribs join their cartilages. They are not palpable
what are the reference lines
Midsternal
Midclavicular
Axillary Line - posterior, mid and anterior axillary line
Posterior Thoracic Landmarks
Vertebra Prominens - most prominent bony spur at base of neck (C-7)
spinous process
Scapula - inferior border usually at 7th or 8th rib
Physical Exam/Assessment (Objective)
Inspect posterior chest – note symmetry
Skin color and condition
Palpate symmetric chest expansion
Tactile fremitus - palpable vibration (“99")
Palpate chest wall for tenderness, skin temperature and/or masses
Percussion - note resonance or dullness over the lung fields
Diaphragmatic excursion- not routinely done and not required
Auscultate lungs in all lung fields (note whether clear or adventitious sounds, decreased or absent sounds), not necessary to determine - bronchial, bronchovesicular, or vesicular)
Pulse oximeter
A healthy person with no lung disease and no anemia normally has an SpO2 of 97% to 98%.
SpO2, known as oxygen saturation, is a measure of the amount of oxygen-carrying hemoglobin in the blood
Every SpO2 result must be evaluated in context of a person’s Hb level, acid-base balance, and ventilatory status
inspection
Thoracic cage, respirations, skin color, and condition
A person’s facial expression, and LOC
palpation
Confirm symmetric expansion and tactile fremitus.
Detection of any lumps, masses, or tenderness
Percussions
a. Lung fields, assess for resonance
4. Auscultation posterior, lateral and anterior chest
Assess breath sounds (presence and quality),
normal and note any abnormal/adventitious breath sounds (crackles[rales] and wheezes [ronchi])
normal: Spinous processes appear in a straight line.
abnormal Skeletal deformities limiting excursion (e.g., scoliosis, kyphosis
normal: Thorax is symmetric and elliptical. Ribs slope downward at about a 45-degree angle to the spine
abnormal: Barrel chest" (AP diameter = transverse diameter), ribs are horizontal (often seen in COPD). Chronic emphysema, occurs normal with aging
normal Anteroposterior (AP) diameter is less than transverse diameter
abnormal: Tripod position (leaning forward, arms braced) to aid in expiration (COPD
abnormal findings
Pectus carinatum
breastbone sinks inward into the chest, creating a noticeable depression or "funnel" shape.T
he chest looks caved in.
(pigeon breast/chest) - forward protusion of the sternum(second rib level
Tachypnea
increased RR, rapid shallow breathing greather than 24
Bradypnea
slow breathing pattern, (<10 respirations per minute
Cheyne-Stokes respirations
respirations gradually wax and wane, with periods of apnea, in a regular pattern, usually a sign of a poor prognosis
Pleural Effusion
collection of excess fluid in the intrapleural space
Pneumothorax
free air in pleural space causes lung collapse
Bronchitis
Inflammation of bronchi, may have partial obstruction of bronchi from secretions or inflammation causing constriction. Characterized by hacking, “mucousy” wet and often productive cough. Crackles with auscultation, usually CXR will be clear.
Pneumonia
Infection of the lung parenchyma, alveoli become consolidated with bacteria and fluid. Lung sounds will auscultate crackles or be diminished, especially in the bases, percussion will illicit a dull sound
Asthma
Reactive airway disease, an allergic response or hypersensitivity to allergens, irritants, microorganisms, and exercise. Characterized by bronchospasm, inflammation and very thick mucous production in the airways
Chronic obstructive breathing
normal inspiration and prolonged expiration to overcome increased airway resistance chronic obstructive lung disease
Atelectasis (Collapsed Lung
Collapsed section of lung or entire lung. Significantly decreased or absent lung sounds over affected area
Rhonchal fremitus
Rhonchal fremitus is palpable with thick bronchial secretions.
Pleural friction fremitus is palpable with inflammation of the pleura).
Crepitus is a coarse, crackling sensation palpable over the skin surface. It occurs in subcutaneous emphysema when air escapes from the lung and enters the subcutaneous tissue, as in tension pneumothorax or after open thoracic injury or surgery
Kyphosis
An exaggerated posterior curvature of the thoracic spine (humpback) that causes significant back pain and limited mobility. Severe deformities impair cardiopulmonary function. If the neck muscles are strong, compensation occurs by hyperextension of head to maintain level of vision
Increased Tactile Fremitus
occurs with conditions that increase the density of lung tissue, thereby making a better conducting medium for vibrations (e.g., compression or consolidation [pneumonia]
Decreased Tactile Fremitus
Occurs when anything obstructs transmission of vibrations (e.g., an obstructed bronchus, pleural effusion or thickening, pneumothorax, and emphysema). Any barrier that gets in the way of the sound and your palpating hand decreases fremitus
Rhonchal Fremitus
Vibration felt when inhaled air passes through thick secretions in the larger bronchi. This may decrease somewhat by coughing
Pleural Friction Fremitus
Produced when inflammation of the parietal or visceral pleura causes a decrease in the normal lubricating fluid. The opposing surfaces make a coarse grating sound when rubbed together during breathing.
Crackles—Fine (formerly called rales
Discontinuous, high-pitched, short crackling, popping sounds heard during inspiration that are not cleared by coughing; you can simulate this sound by rolling a strand of hair between your fingers near your ear
Late inspiratory crackles occur with:
pneumonia, heart failure, and interstitial fibrosis
Early inspiratory crackles occur with obstructive disease: chronic bronchitis, asthma, and emphysema
crackles-course
Loud, low-pitched bubbling and gurgling sounds that start in early inspiration and may be present in expiration; may decrease somewhat by suctioning or coughing but reappear shortly—sounds like opening a Velcro fastener
Pulmonary edema, pneumonia, pulmonary fibrosis
Atelectatic
Sound like fine crackles but do not last and are not pathologic; disappear after the first few breaths
Sound like fine crackles but do not last and are not pathologic; disappear after the first few breaths
Pleural friction rub
very superficial sound that is coarse and low pitched; it has a grating quality as if two pieces of leather are being rubbed together; sounds just like crackles, but close to the ear
Pleuritis, accompanied by pain with breathing (rub disappears after a few days if pleural fluid accumulates and separates pleurae
musical sounds
Wheeze—High-pitched (sibilant
High-pitched, musical squeaking sounds that sound polyphonic (multiple notes as in a musical chord);
acute asthma or chronic emphysema
Wheeze—Low-pitched (sonorous rhonch
Low-pitched; monophonic, single-note, musical snoring, moaning sounds;
Bronchitis
Stridor
High-pitched, monophonic, inspiratory, crowing sound; louder in neck than over chest wall
Croup and acute epiglottitis in children and foreign inhalation; obstructed airway may be life-threatening
what is hypercapnia
increased carbon dioxide in the blood
which part of the lungs is assessed on the posterior chest
all parts of the lower lob
decreased tactile fremitus is consistent with which diagnosis
pleural effusion
decreased fremitus occurs what the bronchus si obstructed
pleural effusion
pneumothorax
emphysema
which breath sounds would be considered normal
bronchovesicular
vesicular
bronchial
which finding would the nurse expect upon osculating the lung sounds of a pt with heart failure
crackles in the lung bases
rationale: The nurse is likely to hear crackles at the lung bases. Occasional wheezing may be identified while auscultating the patient with emphysema. Crackles over the upper lobes are heard in the patient with tuberculosis. Bilateral wheezing may be heard in the patient with asthma
Palpable rhonchal fremitus indicates which condition
Thick bronchial secretions
Fremitus is a palpable vibration. When the patient is asked to say something, the sounds generated from the larynx are transmitted through the patent bronchi and the lung parenchyma to the chest wall, and can be felt as vibrations. Rhonchal fremitus is found when bronchial secretions are thick. A pneumothorax may result in decreased fremitus. Inflammation of the pleura may cause pleural friction fremitus. Consolidation of lung tissues may cause increased fremitus.
Which statement precisely describes the "angle of Louis
It is the articulation of the manubrium and the body of the sternum.
It is a useful place to start counting the ribs
Which abnormality would the nurse expect in a patient with kyphosis
An exaggerated posterior curvature of the thoracic spine
humpback
Which condition does the nurse attribute the patient’s regular breathing rate of eight breaths per minute to?
Drug-induced depression
Which additional muscle would be involved in increasing the size of the thoracic cage during forced inspiration after heavy exercise? Select all that apply. One, some, or all responses may be correct
Intercostal muscles
Sternomastoids
Diaphragm
Trapezii
Scaleni
sternomastoid
trapezii
scaleni