8. Oncology Drugs Intro and DNA Modifiers (copy)
1/21
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
22 Terms
Describe the key challenges in anticancer therapy and they key strategies to deal with such challenges
Strategies for key challenges in anticancer therapy
main strategy against resistance - drug combinations
main strategy against toxicities - improve selectivity, rescuing agents to mitigate (make less harmful) toxicity
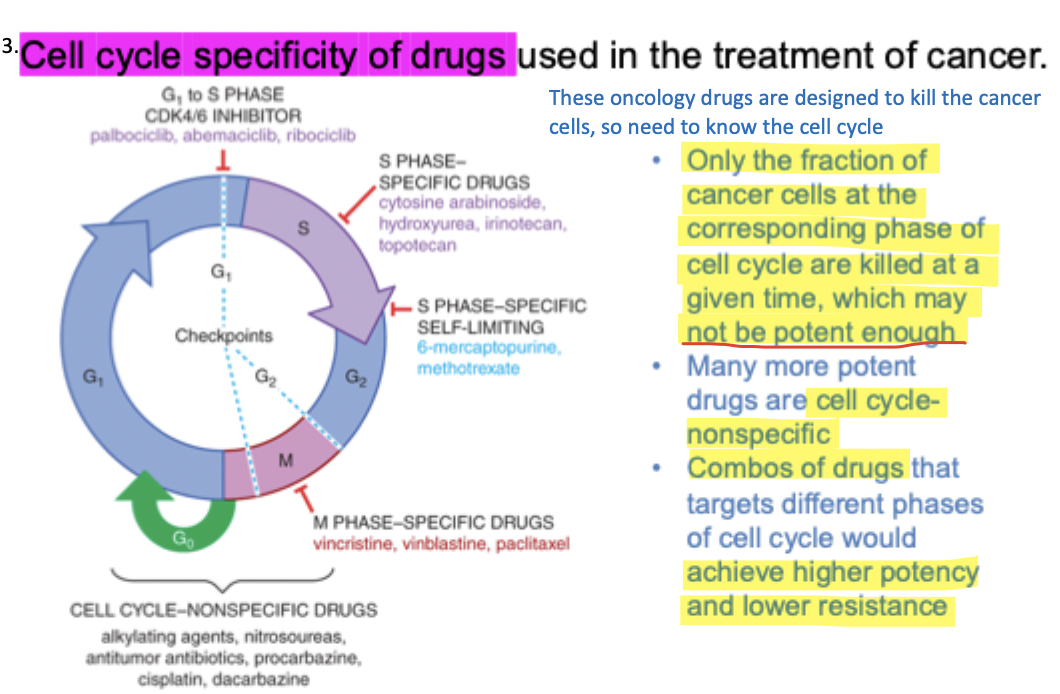
Start from G1 phase - growing of these cells, making proteins and membranes - a lot here is not replication of DNA
S phase - replication of genomic DNA, easily observed
This is where DNA is opened and serves as a template for these replications
When opened, also more vulnerable to a lot of these agents to damage them; if DNA is not being used, then the DNA is condensed to histones - more protected
This is why a lot of these agents mimics the building blocks of DNA, and they get mistaken by the bases, gets into the DNA and are able to kill the cells
G2 phase - chromosome is now replicated, but still far from being ready
A lot of "checking" "correcting" occurs here before going to next phase
If there is too many errors, then cells undergo apoptosis and die
M Phase - two copies of DNA start to condense and then split ..?
G0
Many chemotherapy drugs only work when cancer cells are in a certain stage of the cell cycle, so they cannot kill all the cancer cells at once. At any given time, only some cancer cells are in that sensitive phase, so each treatment kills only a portion of the tumor. Over multiple treatment cycles, more cancer cells enter that phase and are gradually destroyed.
cell cycle non-specific means the agent targets multiple phases of the cell cycle and are often more effective than cell cycle specific agents (these only target cancer cells in one phase of the cell cycle)
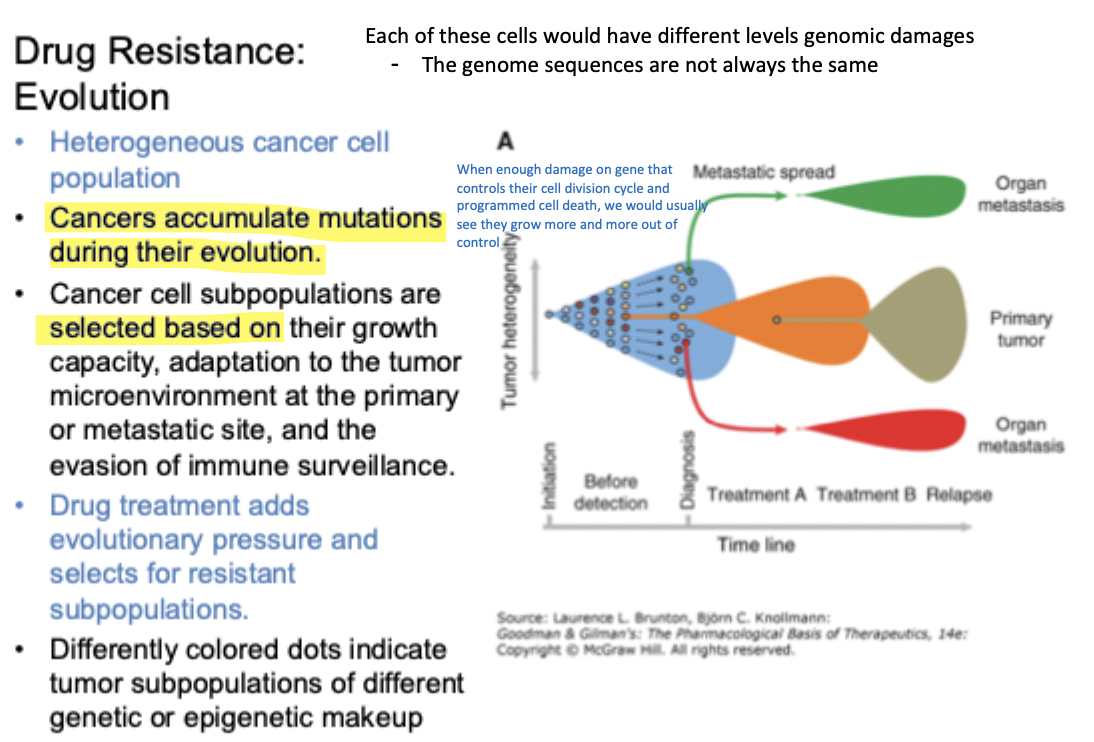
Describe the drug resistance problem in cancer based on cancer cell heterogeneity and on the mutation load model
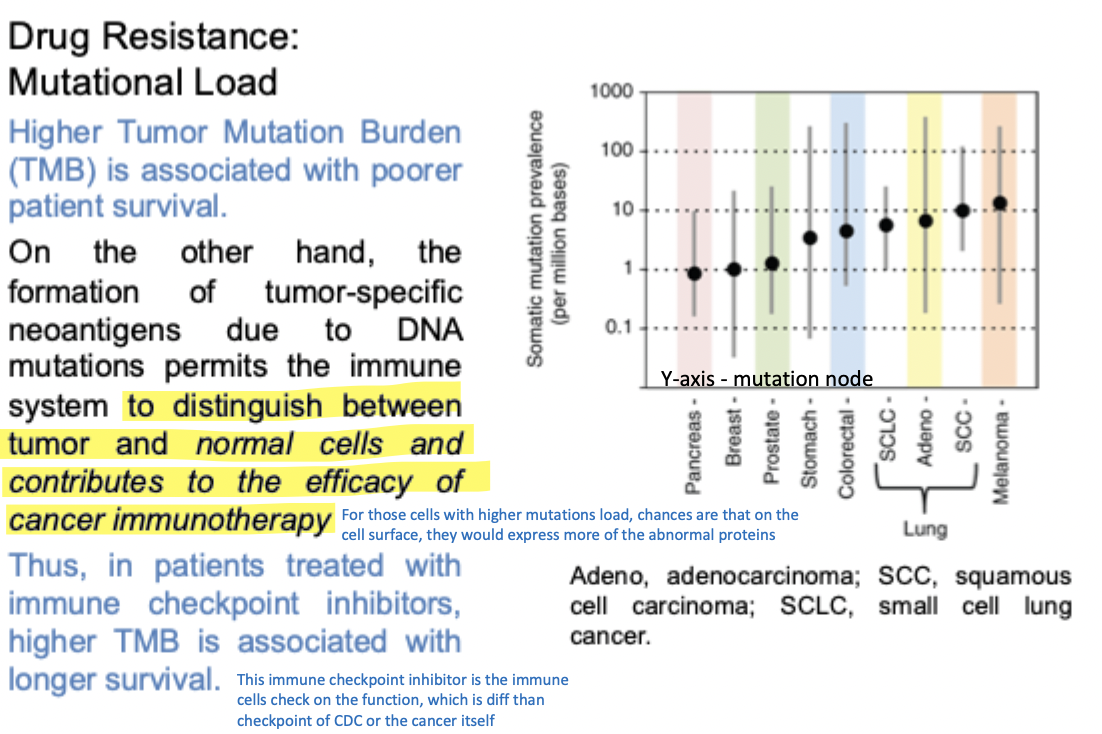
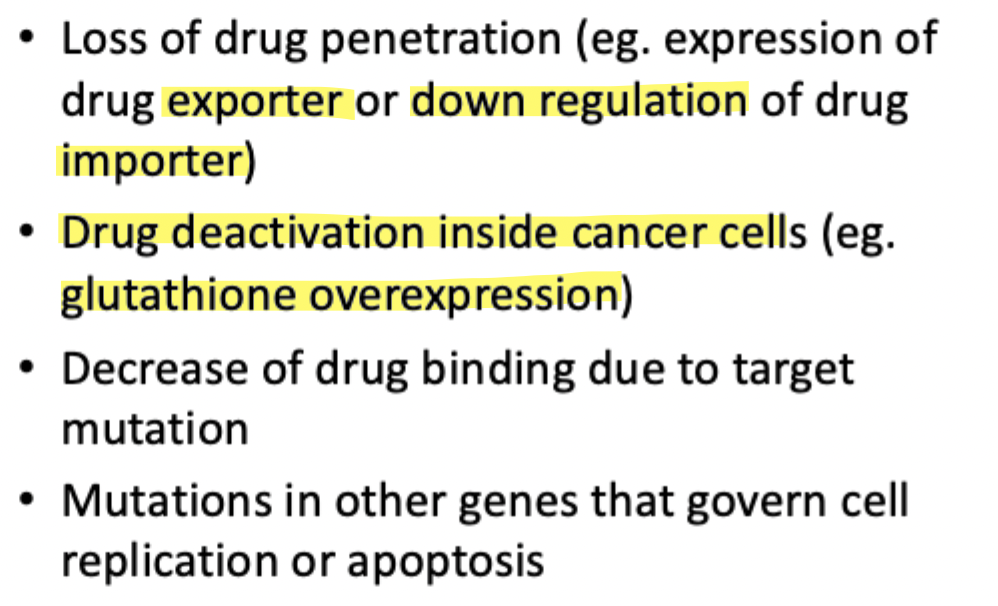
Common mechanisms of resistance to Anticancer Agents
General features of DNA Alkylators
Agents
Structural features
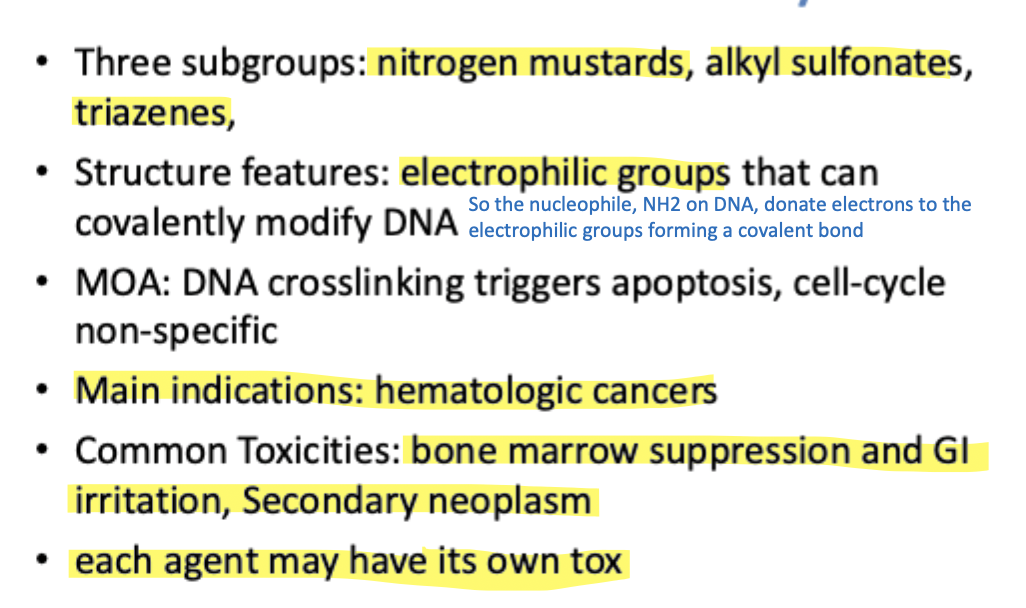
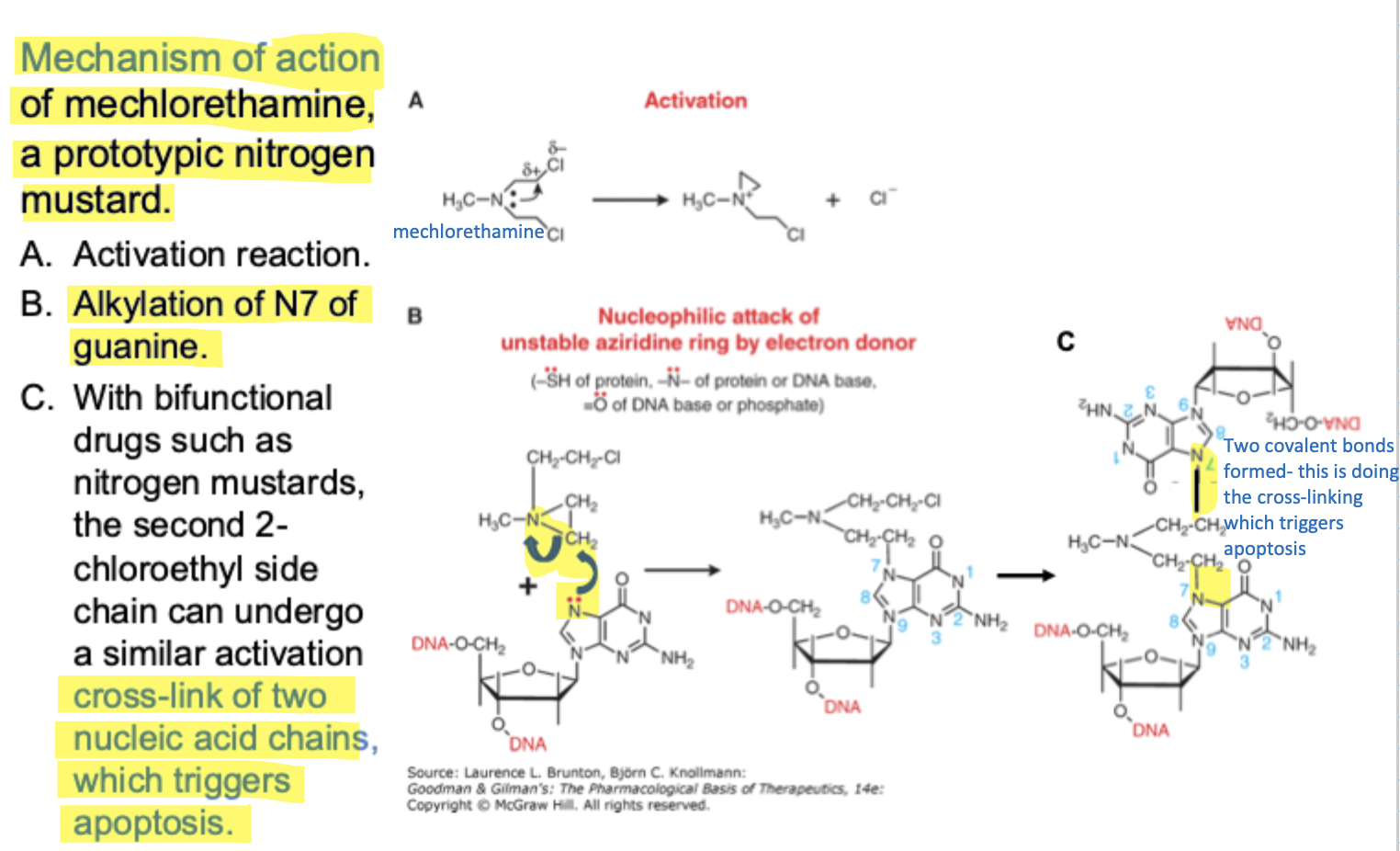
Crosslinking - One agent forms two covalent bonds, each one strand of DNA would crosslink, messing up and ties DNA together and forms a structure for repairing enzymes to do their job - this is why apoptosis is triggered
Cell cycle is non-specific
DNA is not only used for making new cells during replication - it is also constantly being used to make proteins through transcription. Some chemotherapy drugs can damage or "cross-link" the DNA while the cell is trying to read and use it. When the DNA becomes too damaged, the cell can no longer properly make proteins or function normally, so the cell eventually dies
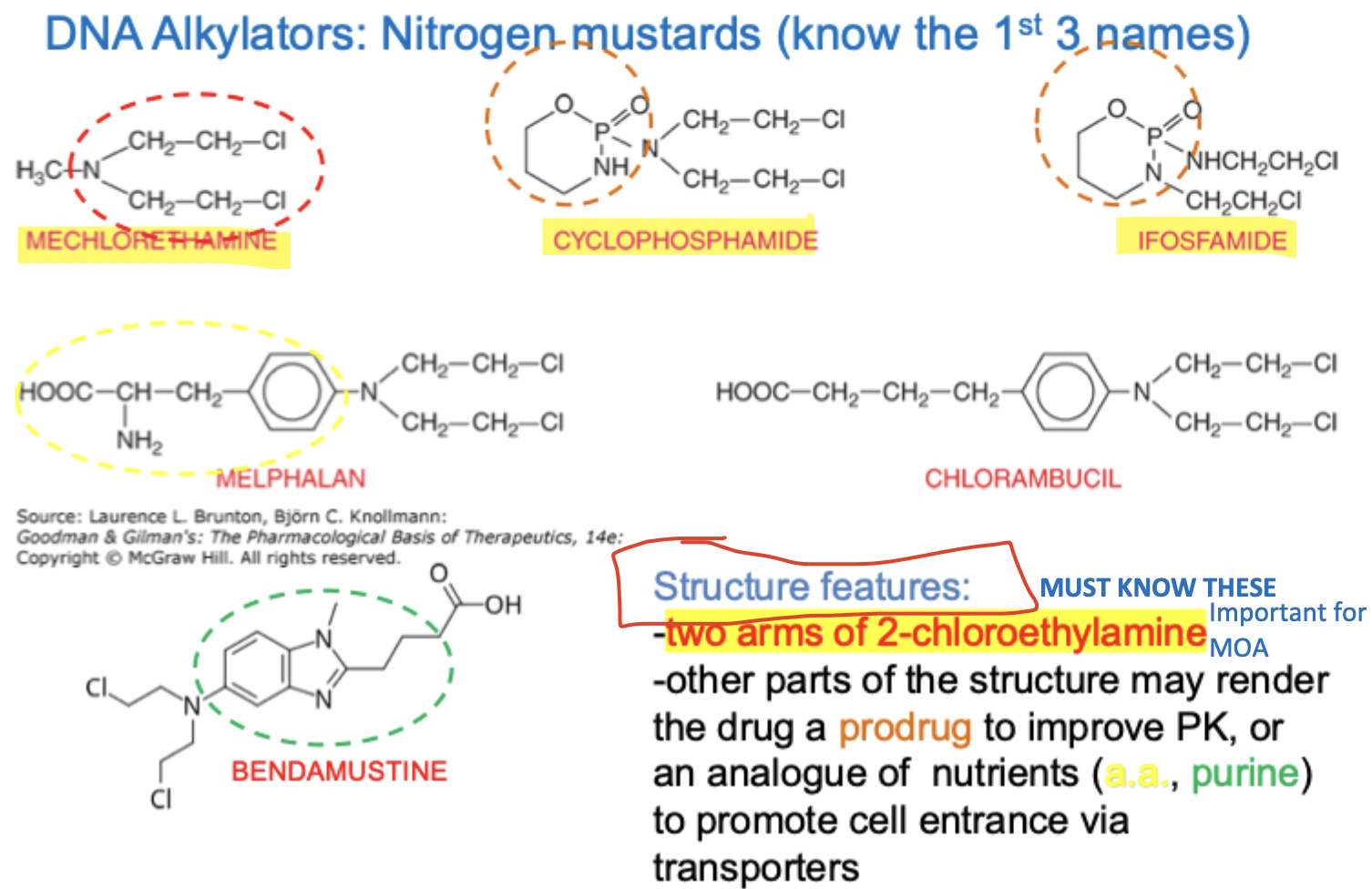
MOA of prototypic nitrogen mustard
MOA of cyclophosphamide and Ifosfamide
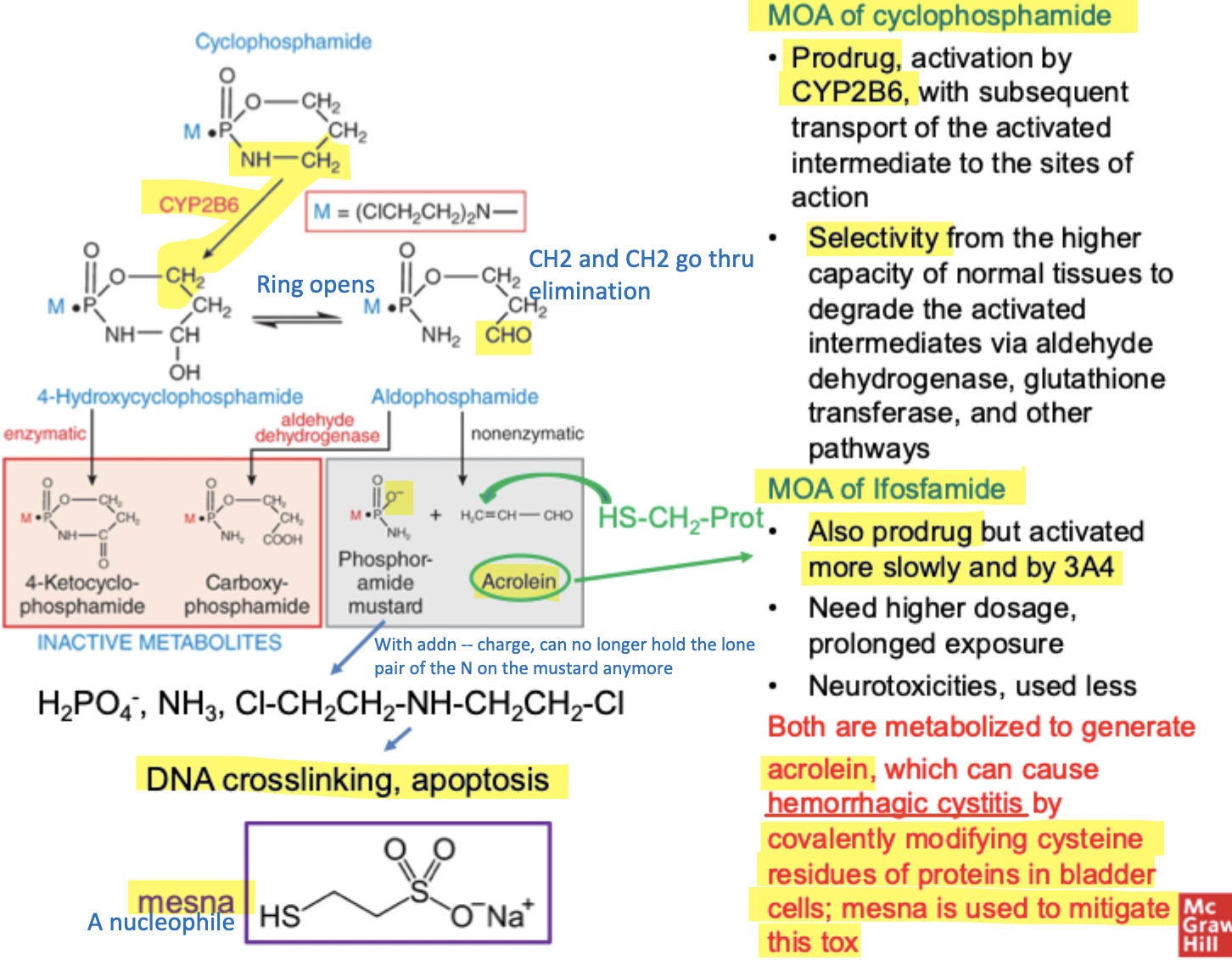
1. Cyclophosphamide and Ifosfamide are initially “inactive”
These drugs contain a nitrogen mustard group, which is the part that can damage DNA.
Normally, nitrogen mustards are very reactive and can attack DNA right away.
But in cyclophosphamide/ifosfamide, that mustard is temporarily “locked” by a phosphamide ring.
So before metabolism:
the drug is relatively inactive
the nitrogen’s lone pair is tied up
it cannot easily attack DNA yet
That is why these drugs are called prodrugs.
2. The liver activates the drug
The liver enzyme system called cytochrome P450 (especially CYP2B6 for cyclophosphamide) metabolizes the drug.
The enzyme:
adds an OH group near the nitrogen
this makes the ring unstable
the ring opens and breaks apart
This produces two important products.
3. Product #1 = the ACTIVE anticancer compound
One product eventually releases the fully activated nitrogen mustard.
This active mustard:
forms reactive intermediates
binds DNA
creates DNA cross-links
These cross-links prevent the cancer cell from:
copying DNA
reading DNA
making proteins
Eventually the cell dies.
That is the main anticancer mechanism.
4. Product #2 = acrolein (the toxic byproduct)
The second product formed is acrolein, which is an alpha-beta unsaturated aldehyde.
Acrolein is highly electrophilic/reactive.
It can react with proteins in bladder cells, especially cysteine residues containing sulfur (–SH groups).
Because acrolein becomes concentrated in urine:
it travels through the urinary tract
accumulates in the bladder
damages bladder lining cells
This can cause:
inflammation
bleeding
hemorrhagic cystitis
5. Mesna protects the bladder
To prevent bladder toxicity, patients are often given Mesna.
Mesna contains an –SH (thiol) group.
That sulfur group reacts with acrolein and neutralizes it before acrolein can damage bladder tissue.
So Mesna acts like a sacrificial protector:
it “soaks up” the toxic acrolein
protects the bladder
6. Why cancer cells are affected more than normal cells
Some normal tissues contain enzymes like:
aldehyde dehydrogenase
glutathione transferase
These enzymes can detoxify/reactivate intermediates and protect normal cells better than cancer cells.
That contributes to the drug’s selectivity.
What are the Platinum Complexes
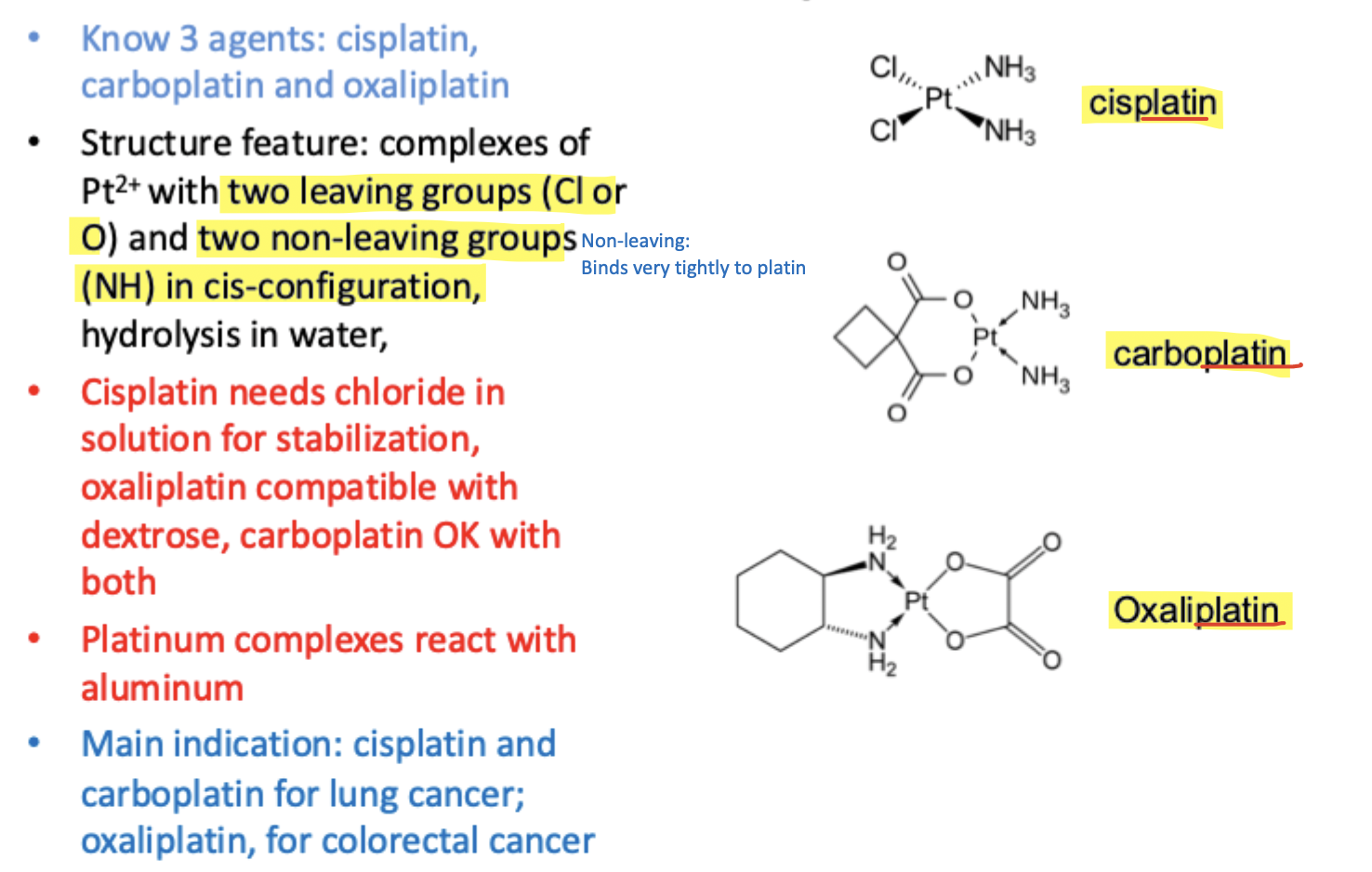
Cisplatin
The chloride are better leaving groups, leaving activates platin and also makes it have positive charges making it more active
More easily activates and more potent b/c faster leaving group
If have cisplatin in the solution, want to make sure there is chloride in the solution for stabilization
Carboplatin and oxaplatin are more stable because they have different leaving groups that leave more slowly
Platinum drugs react with aluminum - becomes metallic Platinum (Pt)
Metal ions can donate electrons to Pt so if there's an interaction with aluminum needles, equipment:
Redox reaction occurs, Pt gets reduced, black precipitate may form, drug becomes damaged/inactive, which is why aluminum containing needles, equipment is generally avoided
Common indications
Cisplatin and Carboplatin
Commonly used for lung cancer
Oxaliplatin
Commonly used for colorectal cancer
MOA of Pt Complexes
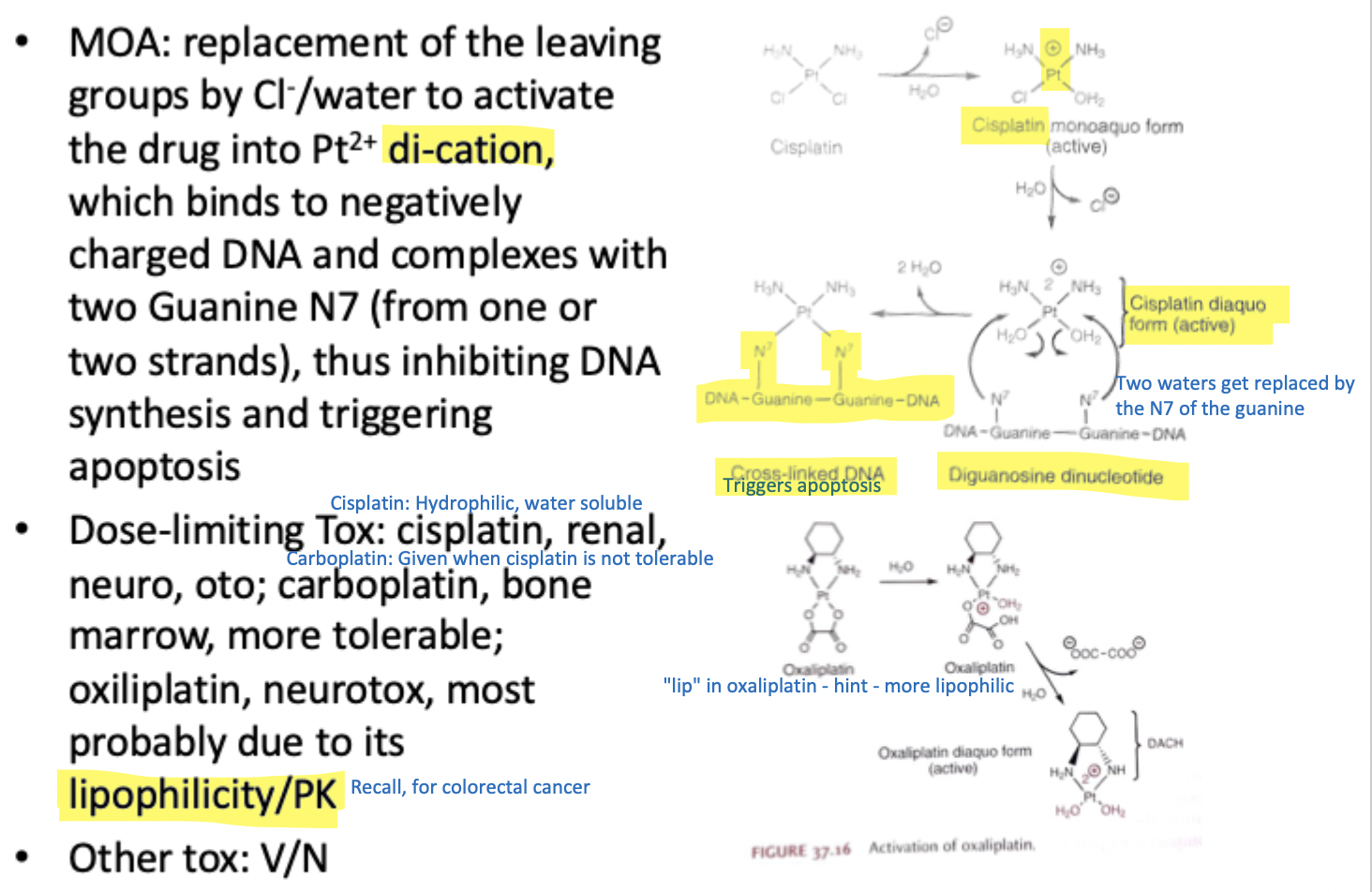
Leave groups will leave, and when they leave, they will be replaced with water; water has no charge, so now the net charge of Pt becomes positive
MOA of Amifostine - mitigates tox of Pt drugs
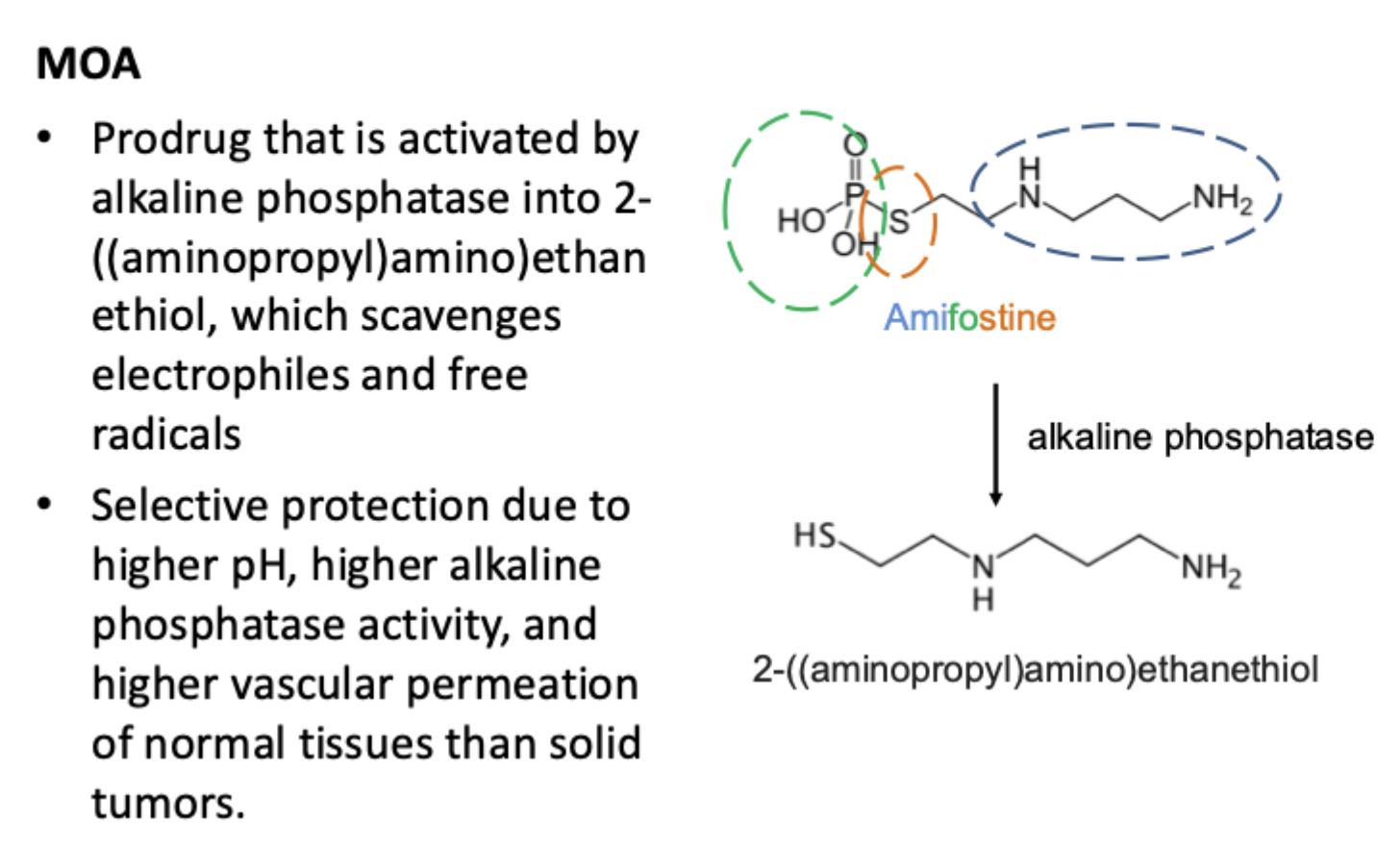
Phosphate group that linked to sulfa, and the rest of amine group
This is a toxicity mitigating agent
Unique, the SH group is blocked by the phospho group, making it a selective toxicity mitigator
Agent goes in vivo and is converted to alkaline phosphatase that cleaves the phospho group, which activates the SH group which is a nucleophile, and it can link to the Pt to deactivate it.
Where is the selectivity?
Normal tissues have high pH and more alkaline phosphatase so amisfostine is activated more in normal tissues than cancer tissues
That creates the selectivity
Cancer tissues are more acidic (low pH), often hypoxic, and have less alkaline phosphatase activity
MOA of DNA Intercalators
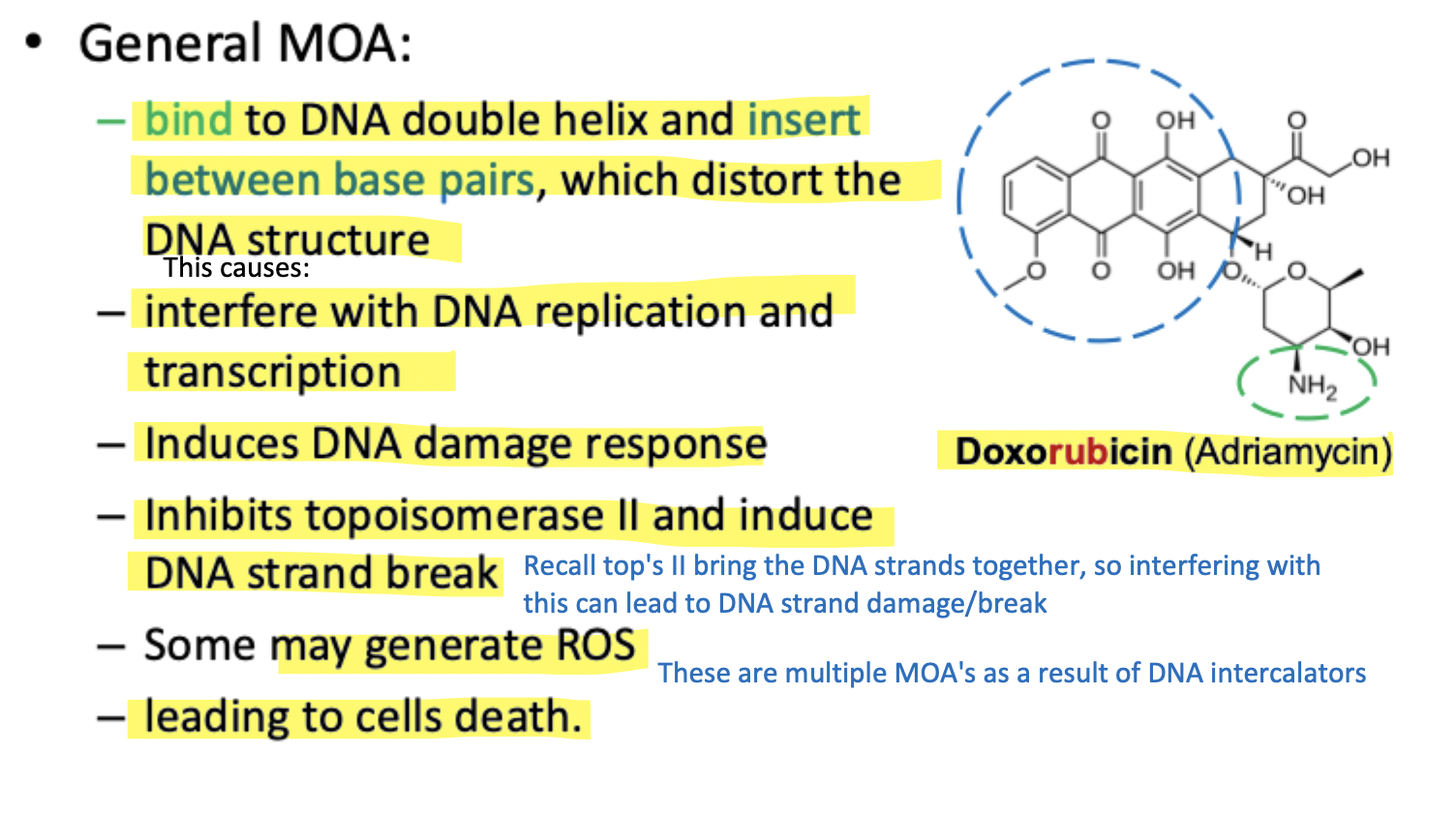
P backbone is -- charge and intercalator are positive charge = attraction
Doxorubicin contains a protonated amine-containing group that provides the positive charge to help the drug bind to the negatively charged DNA backbone through electrostatic attraction
Then once the drug is close to DNA:
The large flat aromatic ring structure slides between the DNA base pairs
This process is called intercalation
Because these ring systems contain many conjugated double bonds, they can easily accept electrons and form stabilized free radicals. These free radicals then react with oxygen to generate reactive oxygen species (ROS), which further damage cellular components and contribute to cancer cell death.
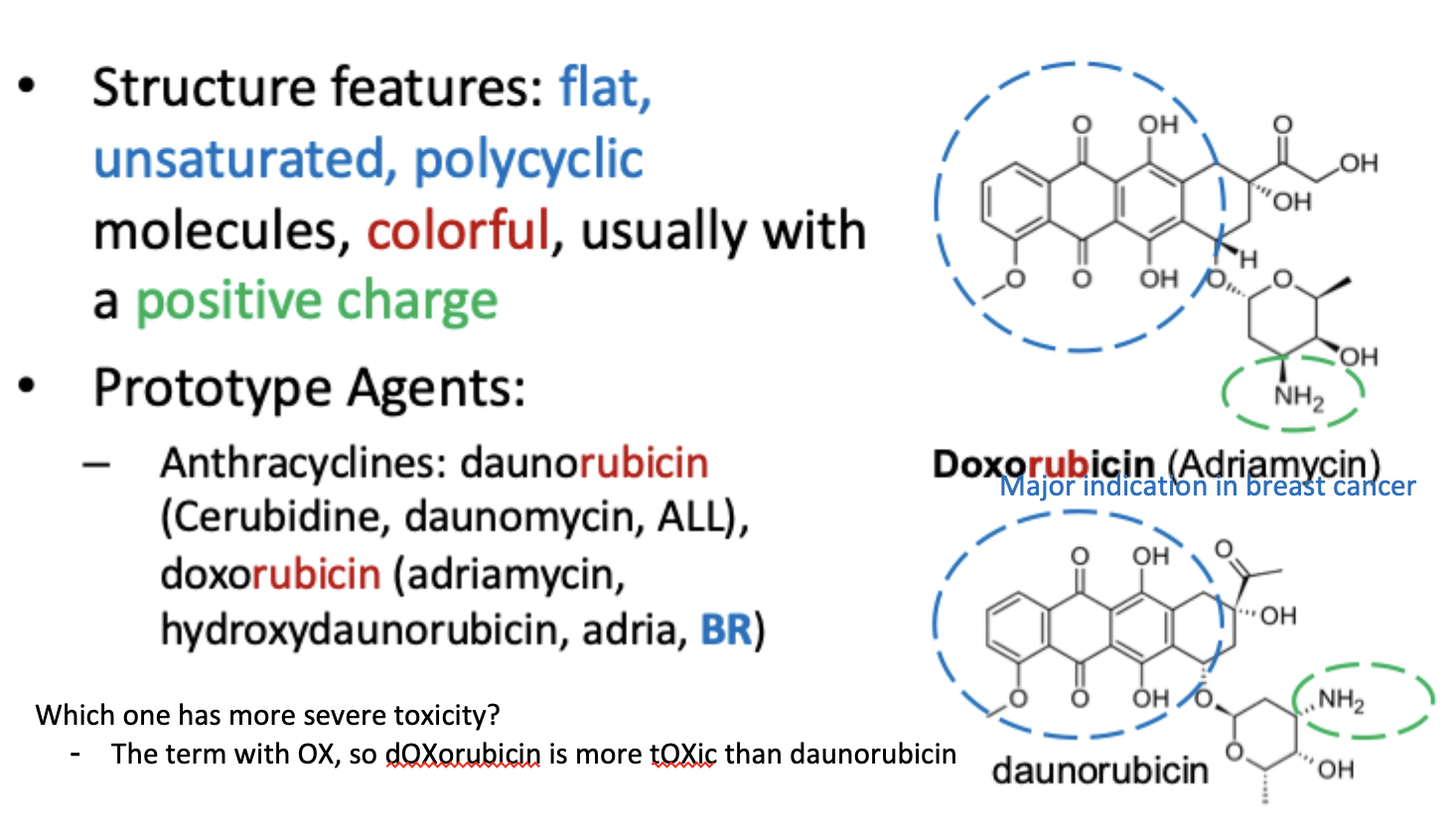
List the DNA Intercalator Agents
Pros and Cons
Toxicity
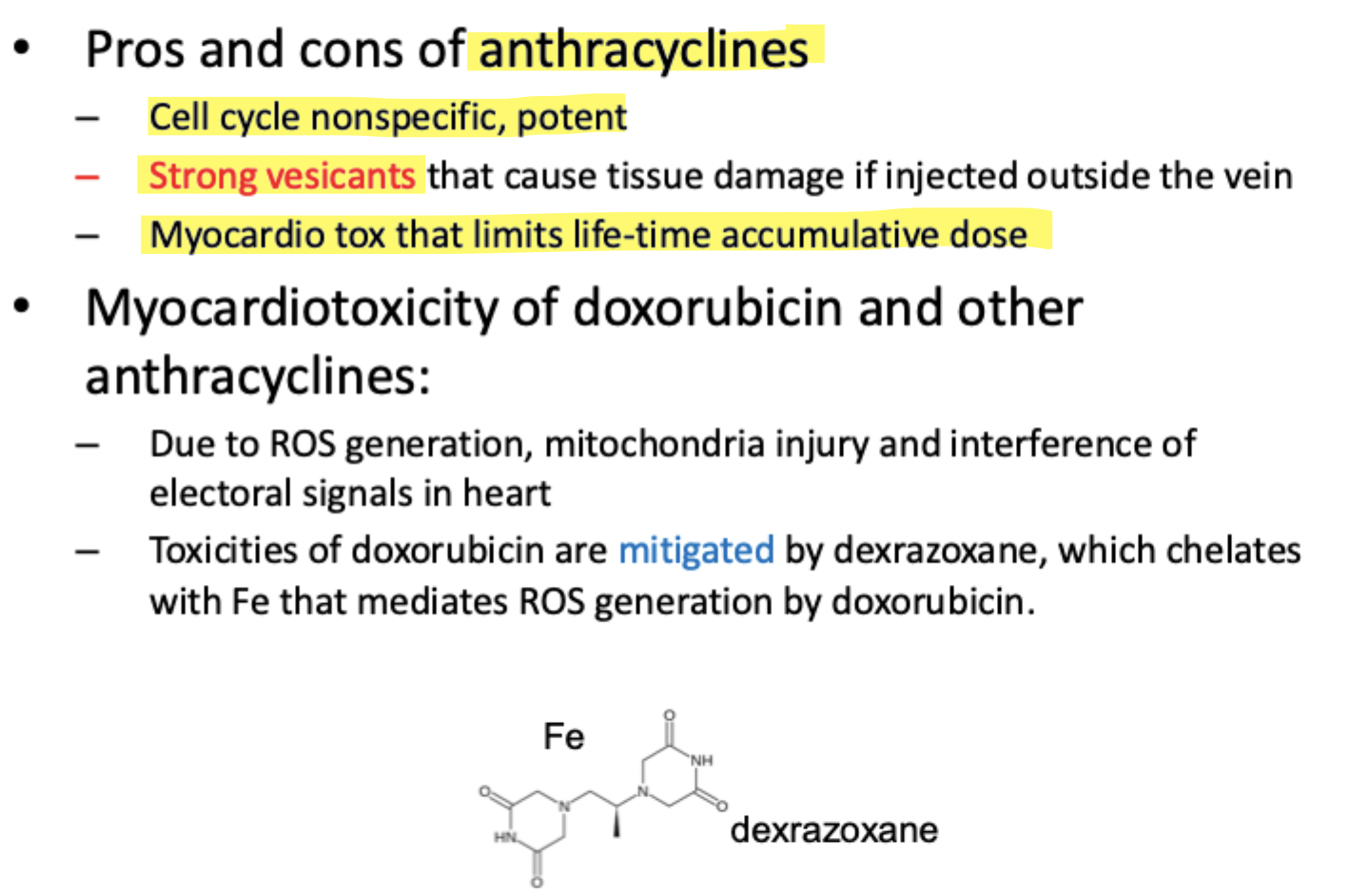
Many enzymes in the body, including cytochrome P450 enzymes, use iron-containing heme groups to carry out redox (electron-transfer) reactions. Iron can help generate free radicals and reactive oxygen species (ROS). Anthracyclines like doxorubicin can participate in these redox reactions, leading to excessive ROS formation, especially in heart cells that contain many mitochondria.
Dexrazoxane works by binding (chelating) iron. By removing available iron, it decreases free radical and ROS formation, which helps protect heart tissue from oxidative damage and reduces doxorubicin-induced cardiotoxicity.
Significance of Liposomal DNA Intercalator Formulations
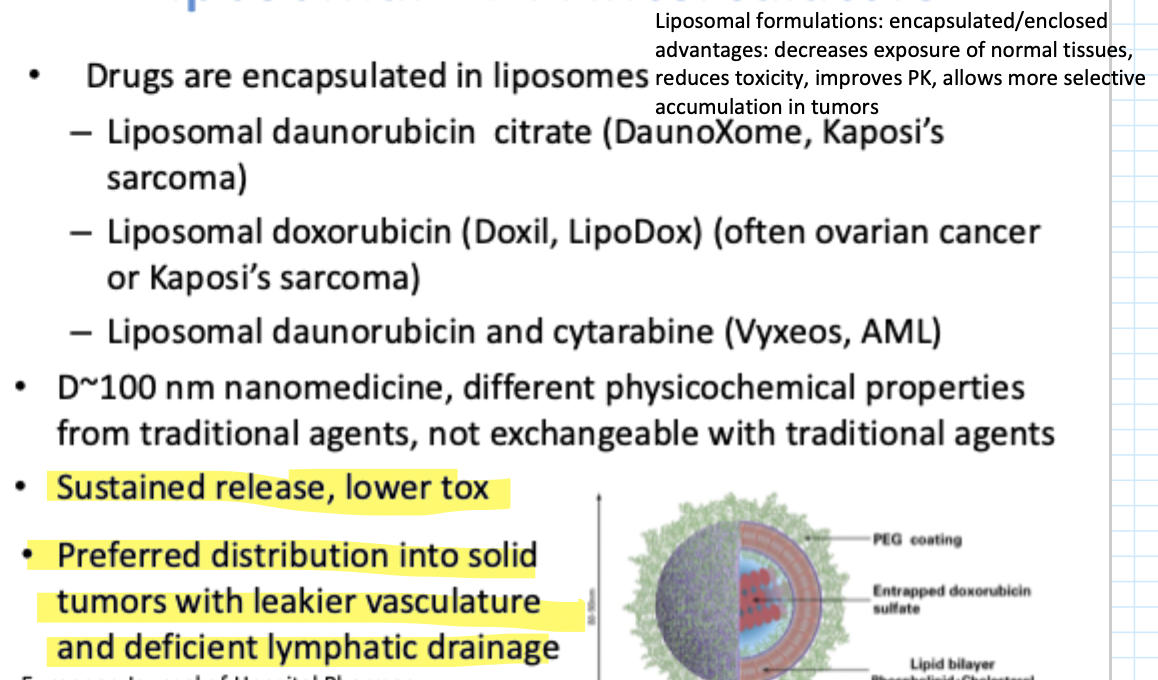
DNA Intercalators are very potent b/c they have multiple MOA's
However, they also cause significant toxicity (esp cardiotoxicity)
To reduce this:
One strategy: using protective/mitigating agents like Dexrazoxane
Anther: Nanoparticle/liposomal drug delivery systems
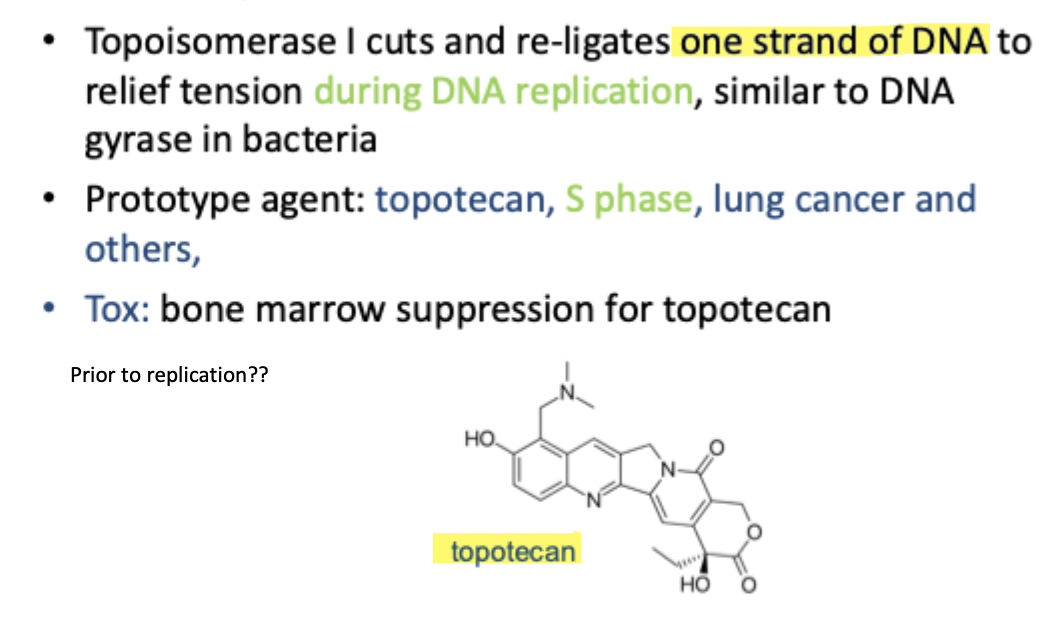
Topoisomerase I Inhibitors
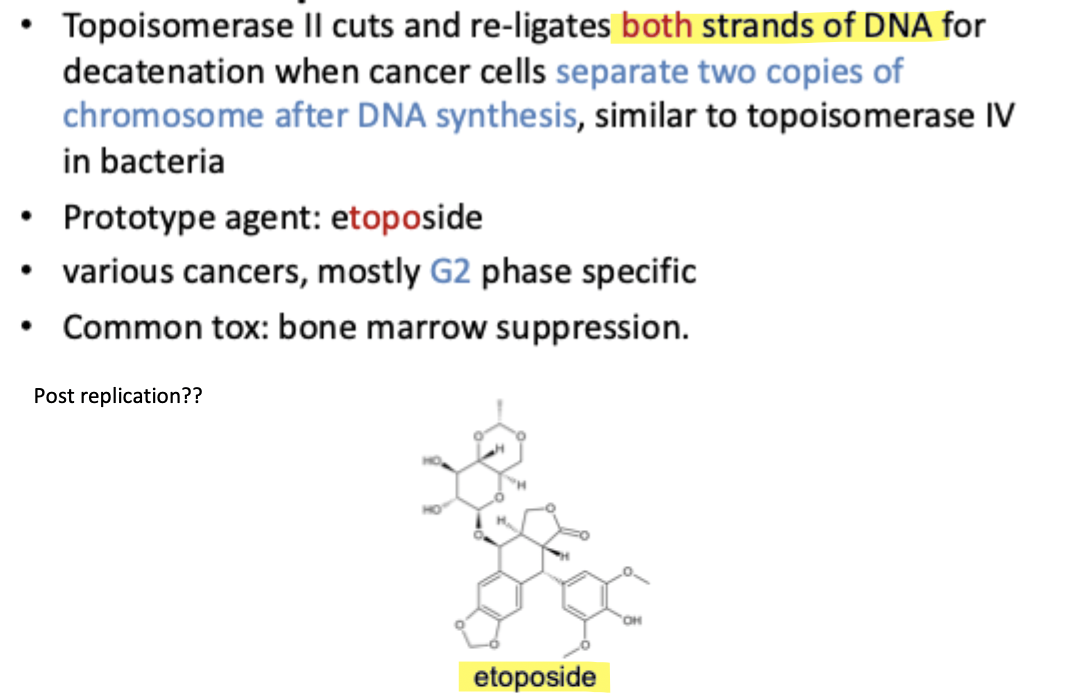
Topoisomerase II inhibitors
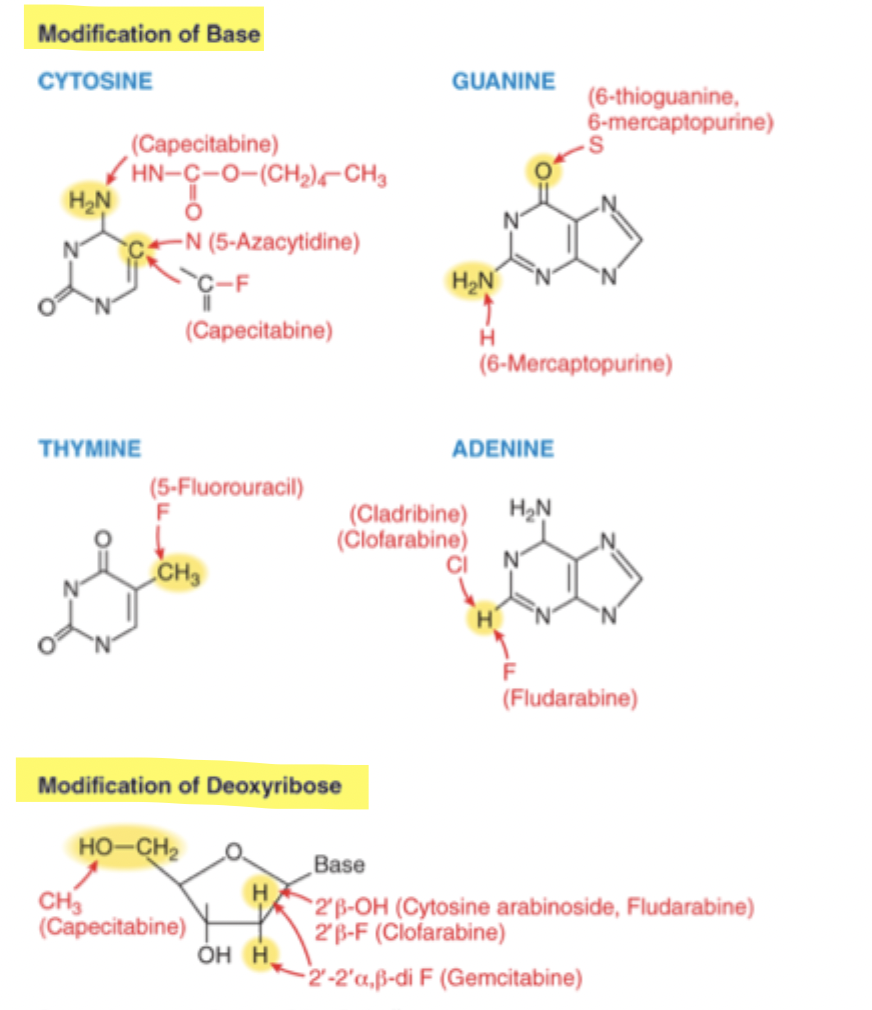
Antimetabolites as anticancer agents
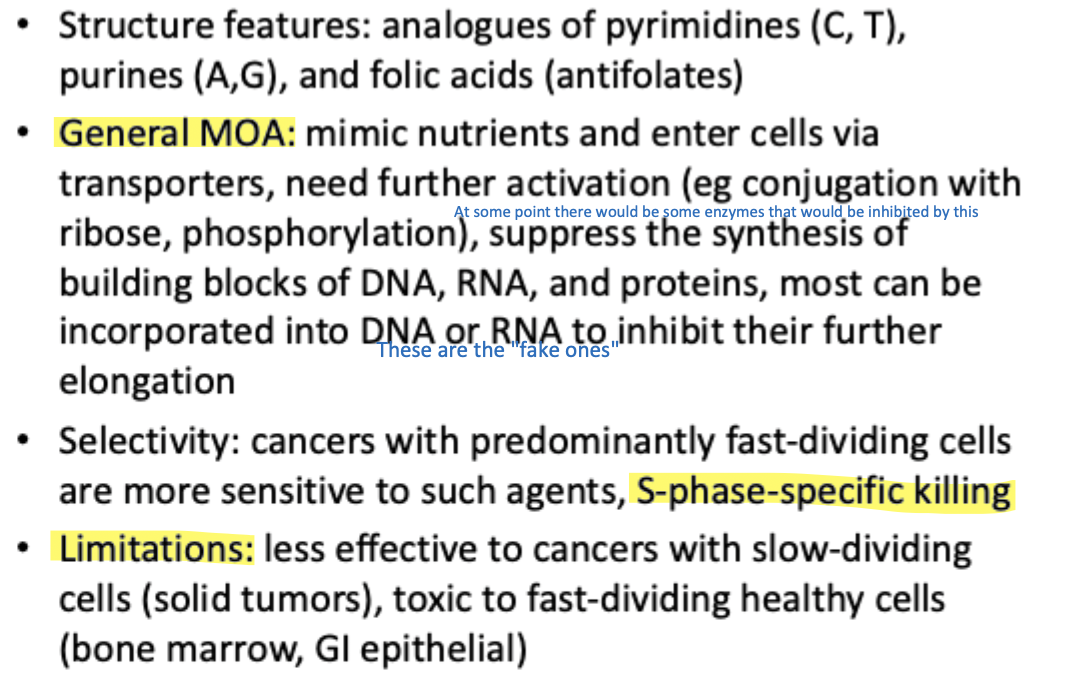
Structural modification of base and deoxyribonucleoside analogues
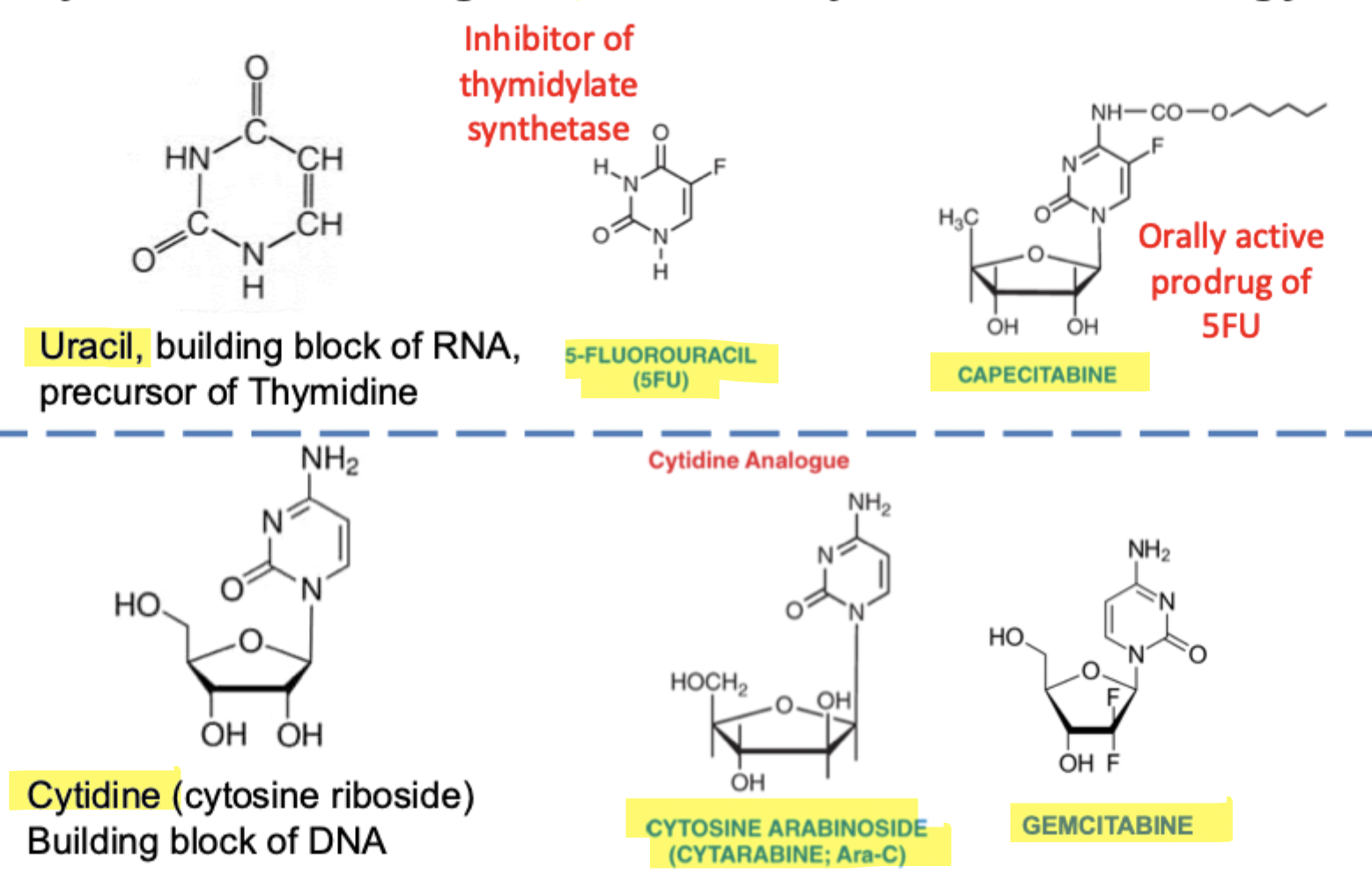
Pyrimidine analogues commonly used in oncology
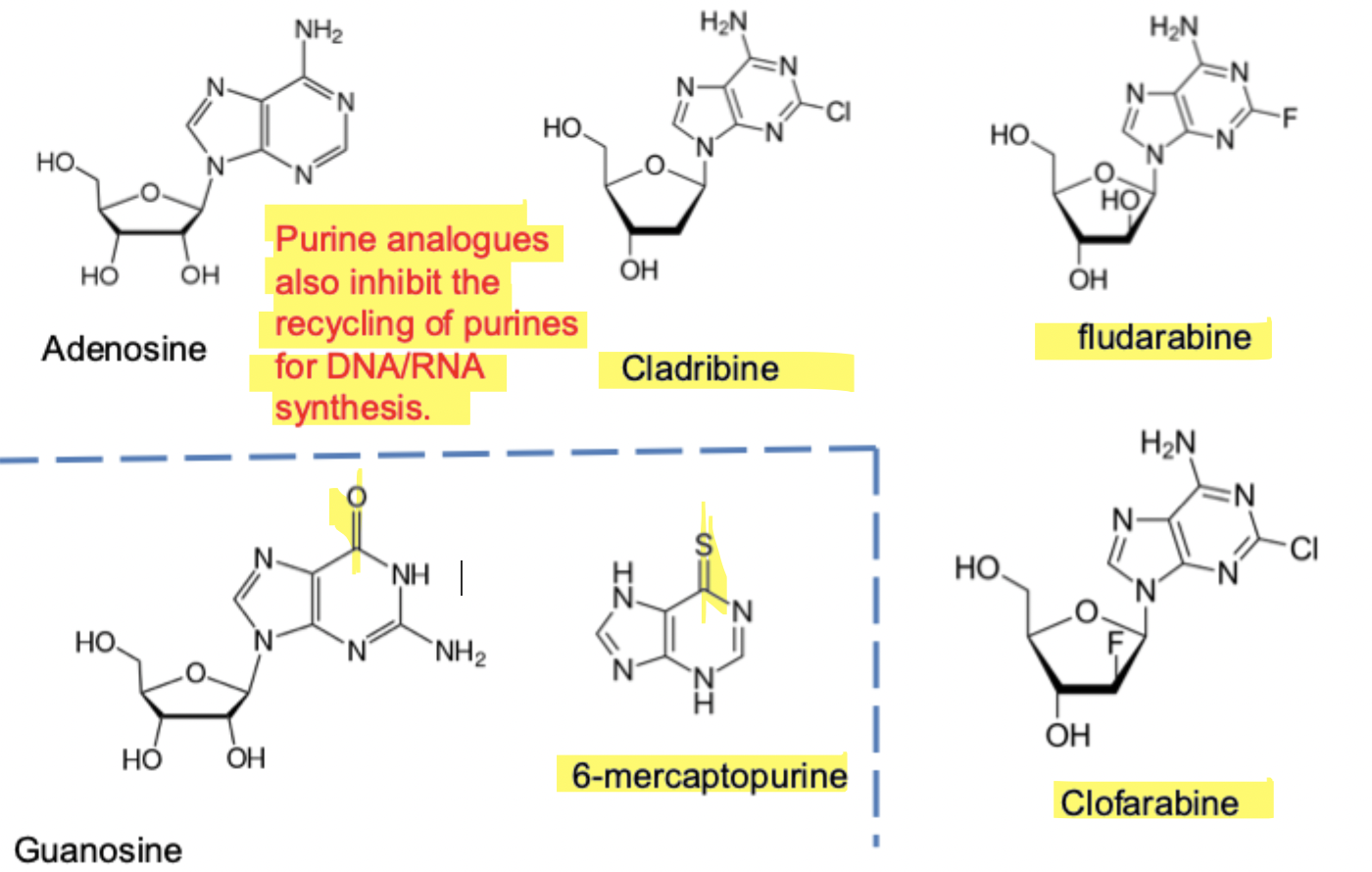
Purine analogues commonly used in oncology
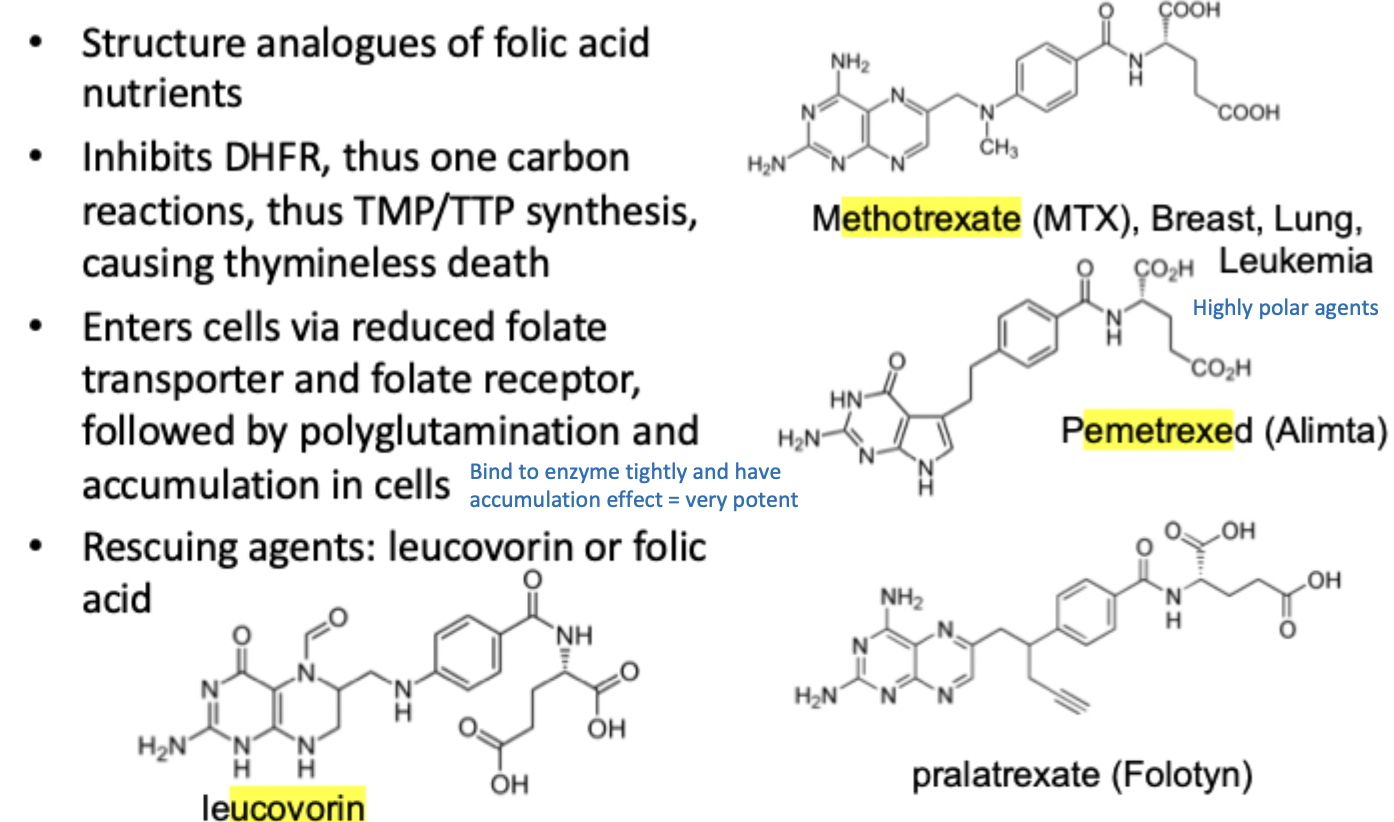
Antifolates as anticancer agents
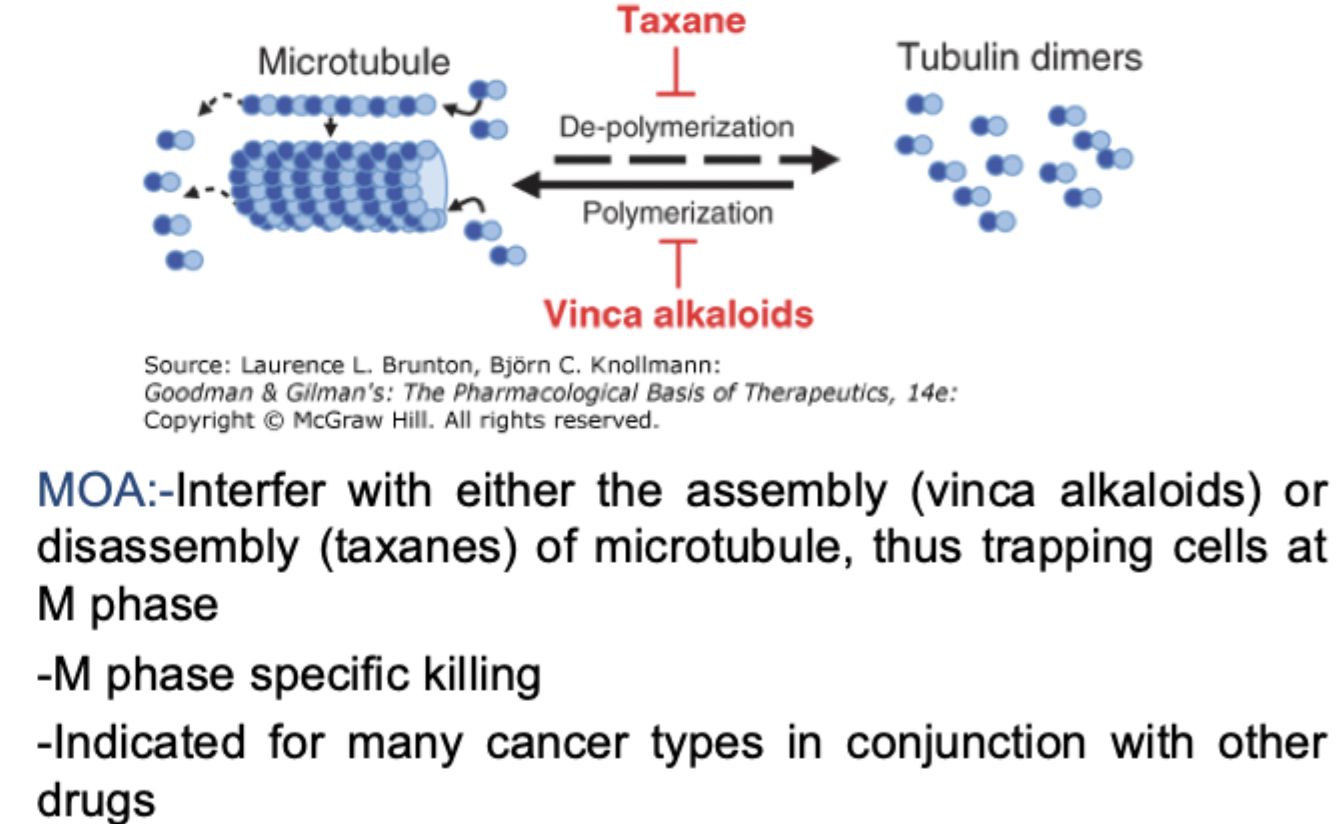
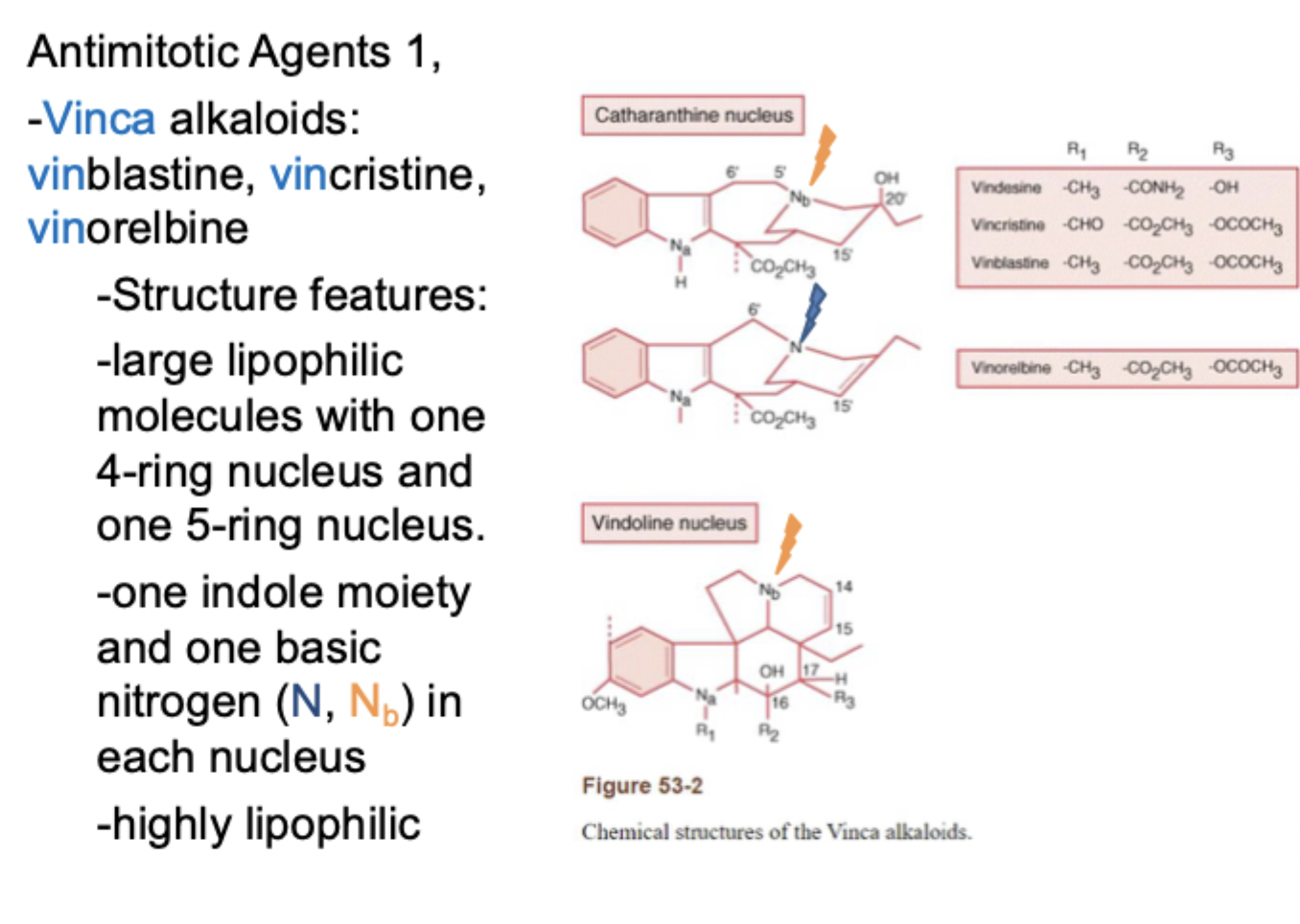
Antimitotic agents
MOA
What phase does it target
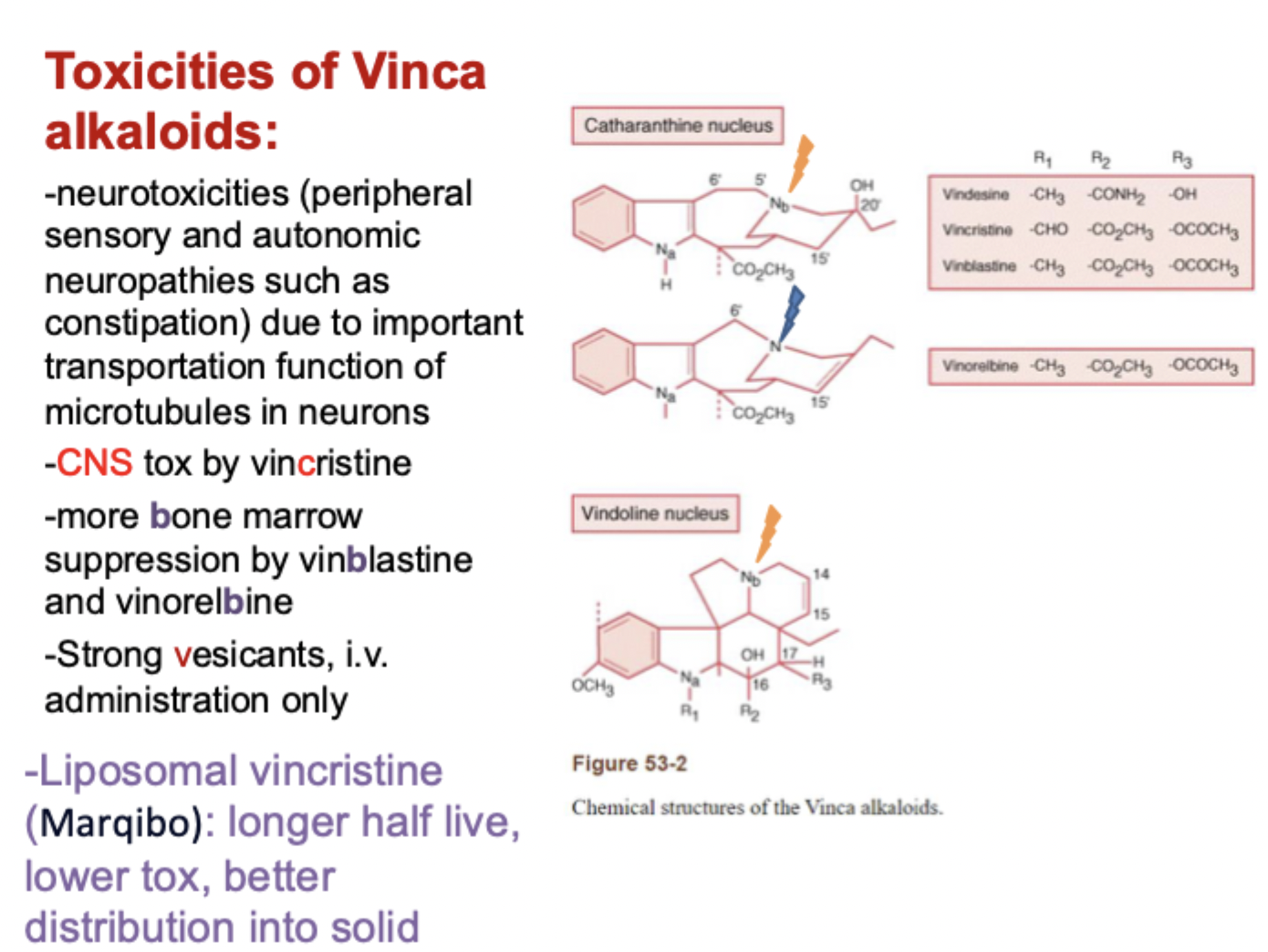
Toxicities of Vinca alkaloids
Toxicities of Taxanes