Exercise and Bones
1/25
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
26 Terms
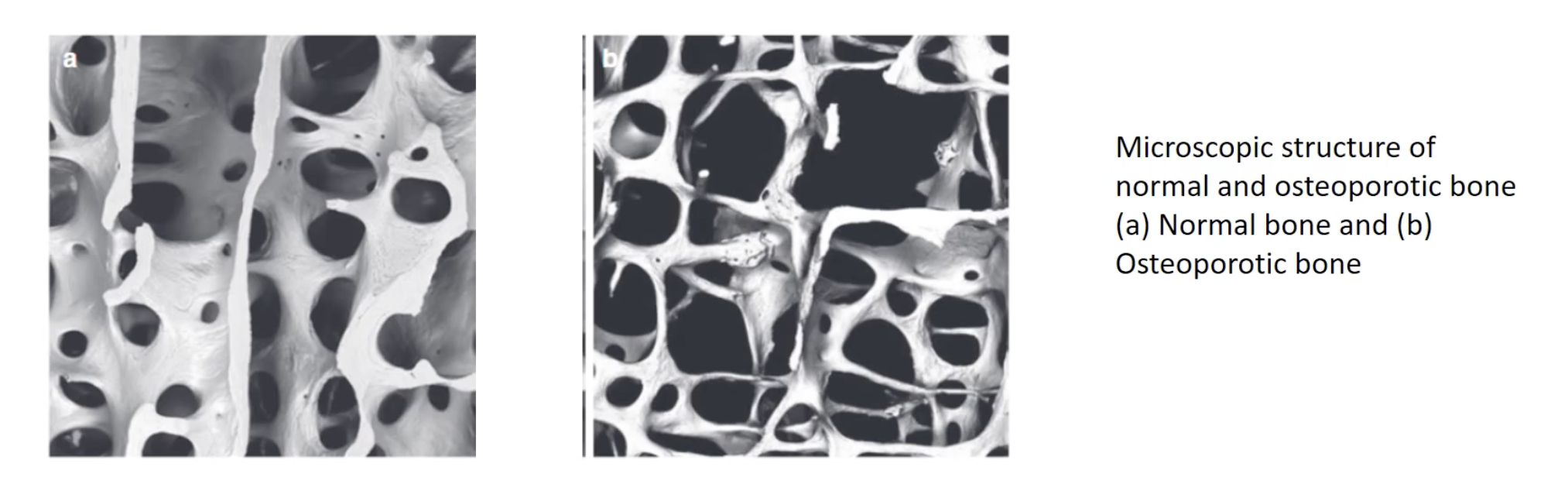
2 types of bone cells + their functions
Osteoclasts
Osteoblasts
Osteoclast function + effect of function
Demineralise bone
Releasing calcium into the bloodtstream
Osteoblast function + how
Lay down new bone (by secreting collagen + other minerals)
How often is compact bone replaced?
approximately every 10 years
How often is spongy bone replaced?
every 3 to 4 years
When is bone mass maintained?
When activity between osteoclasts and osteoblasts is balanaced
When is bone mass lost?
When the activity of osteoclasts exceeds that of osteoblasts
Osteopenia def + what it increases risk for
Bone mineral loss but not yet severe enough to be considered osteoporosis
Higher risk of fractures
Osteoporosis clinical def +
Bone density is 2.5 standard deviations below the mean
Bones become thin, weak + fragile
Bones susceptible to osteoporosis fractures (3)
Hips, pelvis, spine + wrists
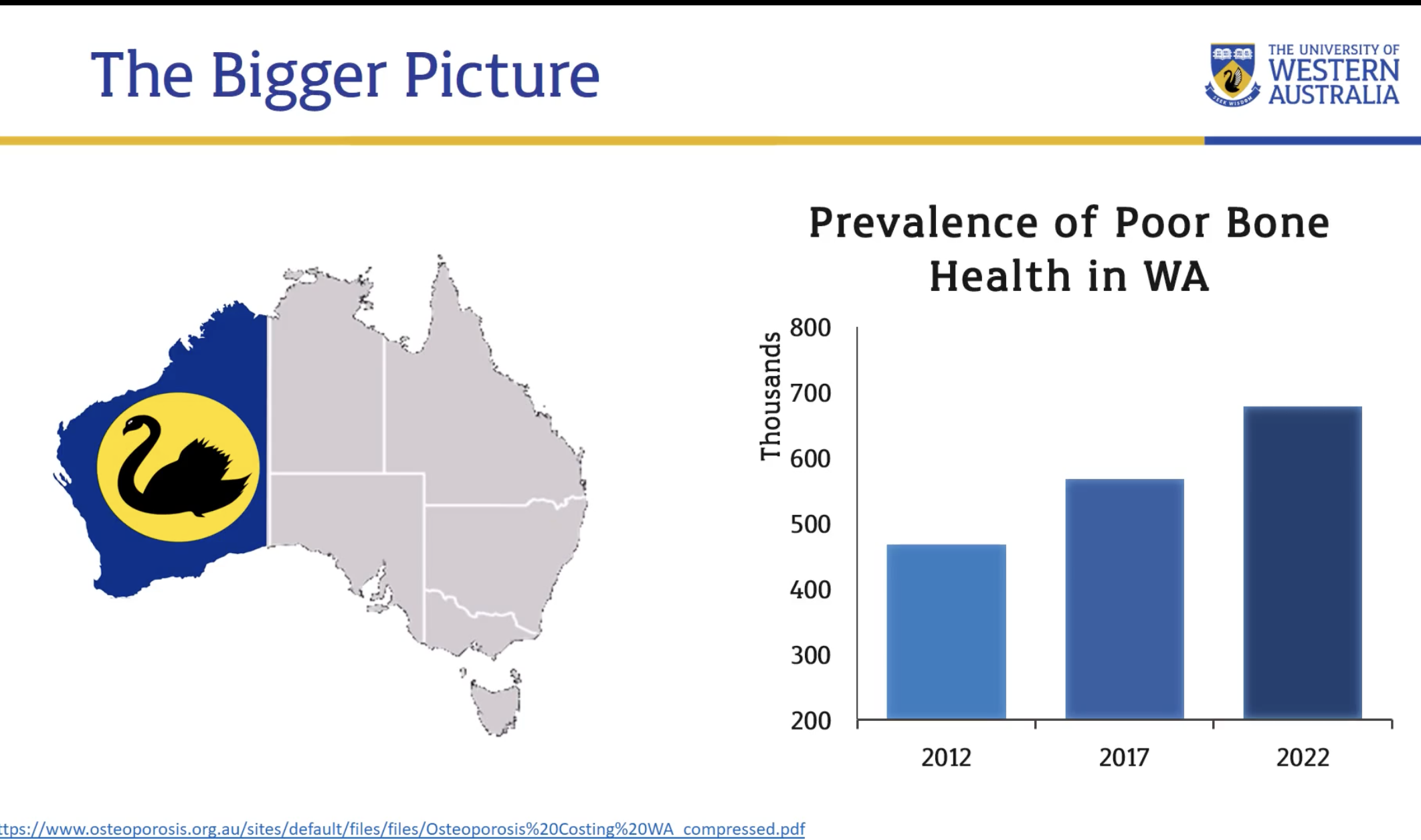
Prevalence of poor bone health (1)
Increasing
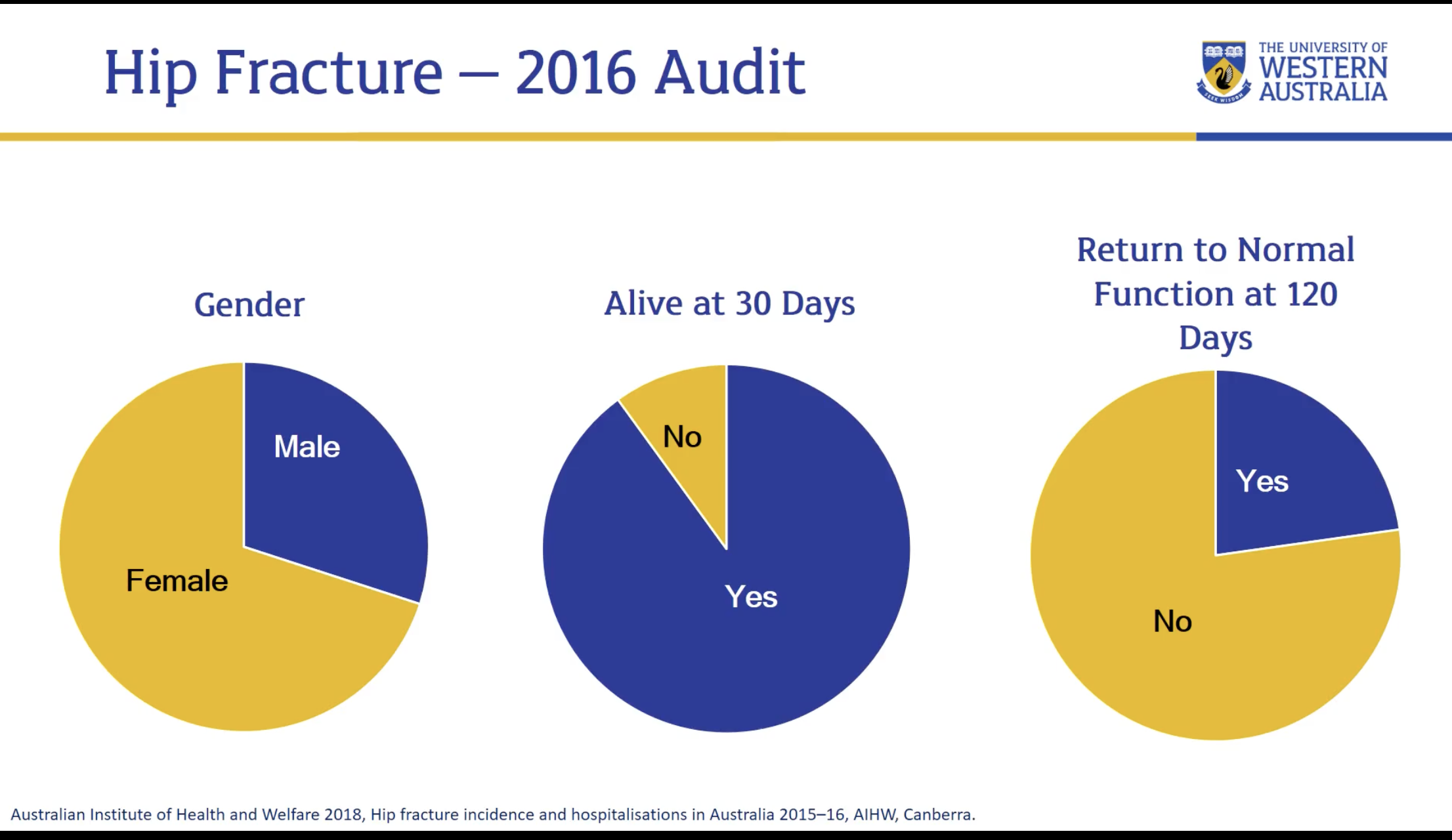
Gender differences, mortality + health outcomes
Gender Risk: Women are at a higher risk, accounting for over 70% of hip fractures in patients aged 50 and over. However, men account for 30% of fractures, indicating it is not exclusively a female disease.
Mortality: 10% of patients do not survive 30 days after a hip fracture; 25% die within one year of the injury.
Morbidity: 78% of survivors do not regain their pre-fracture walking ability within three months of the accident.
Economic cost of osteoporosis

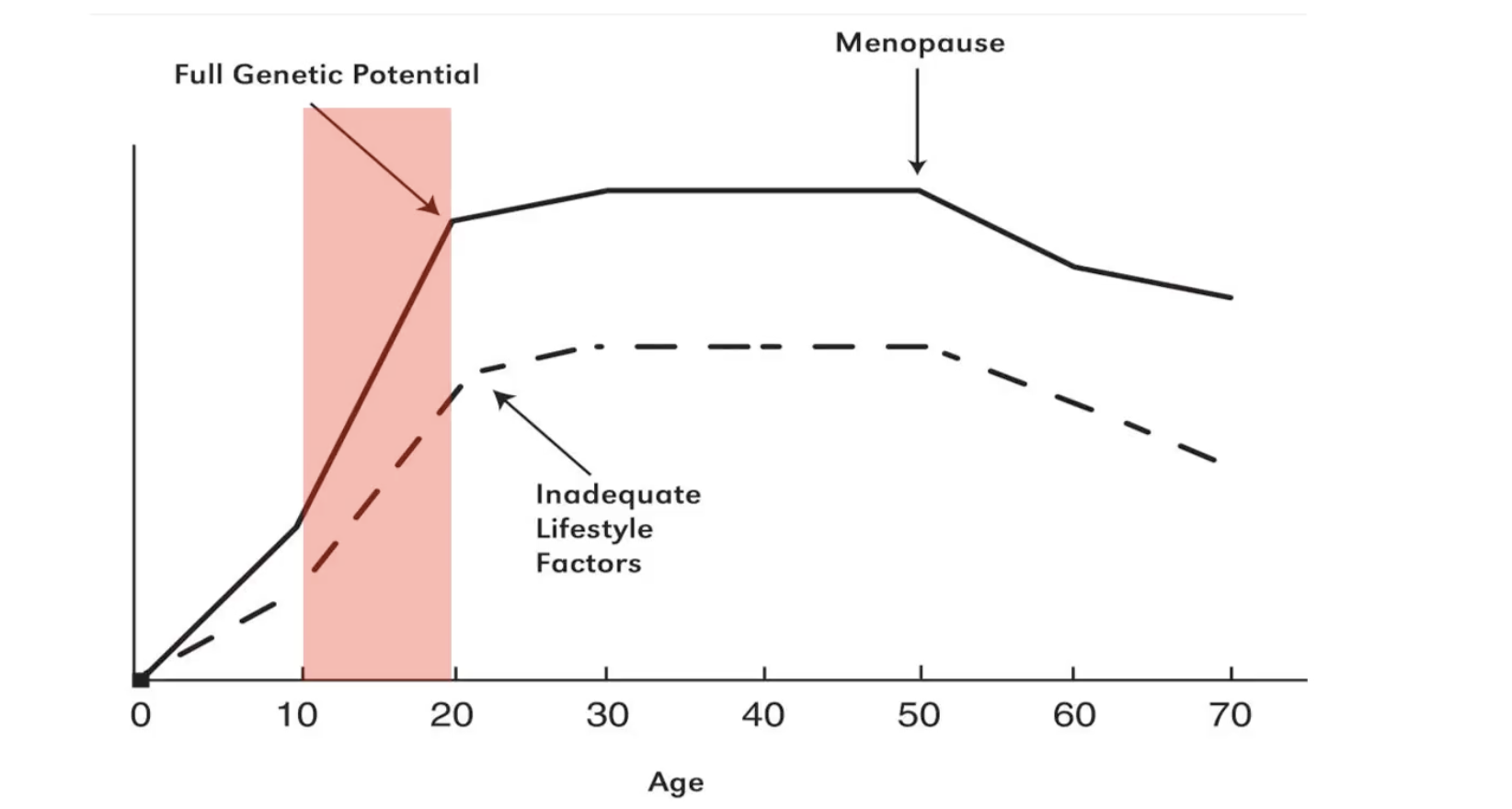
Overarching way to prevent bone health problems in later life (1)
Accrue as much bone mass as possible in bone building years
Purposes of bone remodelling
Meet shifting mechanical demands
Repair micro damage (replace old, brittle bone)
Maintains homeostasis of blood calcium levels → prevents mineral salts from crystallising and making bones brittle and susceptible to fractures
Factors affecting bone remodelling (3)
Nutrition: sufficient calcium intake
Mechanical stimulation
Vitamin D + hormones
Interesting note on calcium impact in older age
Additional intake has little impact on bone density in older age (although insufficient intake def increases osteoporosis risk)
Wolff’s Law (on mechanical influence) (2)
Increased loading on bone → increases bone density to improve ability of bone to resist force
Decreased loading → encourages catabolism of bone
Keeping in mind Wolff’s Law, what can be done to maintain bone strength/density?
Regular exercise
Weight bearing exercise best (running/walking/weights), but non-weight bearing (cycling, swimming) can still be effective
Benefits of resistance training for bone health
Highest degree of specificity in targeting bone strengthening of specific areas (many machines + exercises)
Strategies for creating resistance training program to optimise bone health
Compound/multi-joint movements → force through spine + hips to use greater absolute loads
E.g. squats, cleans, deadlifts, press
Axial Skeleton Loading: Placing weight over the shoulders (e.g., in a gym setting) stresses the spine and hips—the sites most commonly affected by osteoporosis and osteopenia.
Multi-directional Loading: Ensuring bones are stressed from various directions to account for their anisotropic nature.
What does skeletal health also encompass? (3)
Tendons, ligaments, and cartilage
Impact of resistance training on tendons + ligaments (1)
Resistance training → muscle growth → net growth of tendons + ligaments (which aerobic training doesn’t do) → can withstand greater force
How does cartilage get its nutrient supply?
From synovial fluid (no direct blood supply)
Effect of exercise on cartilage health
Joint movement from exercise → O2 to cartilage
Effect of moderate vs strenuous exercise on joint health + note on activity involving repetitive high impact force
Both generally beneficial for cartilage, strenuous exercise the not deleterious for joints as commonly thought
However, repetitive high impact force can increase risk of joint injury → which can in turn lead to cartilage degeneration