Chest Tubes
1/9
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
10 Terms
Chest Tube rationale
-indicated when negative pressure in the pleural space is disrupted as from thoracic surgery or unanticipated trauma
-Normally the 2 membranes are separated by a small amount of serous pleural fluid
-Fluid (pleural effusion)
-Blood (hemothorax)
-Air (pneumothorax)
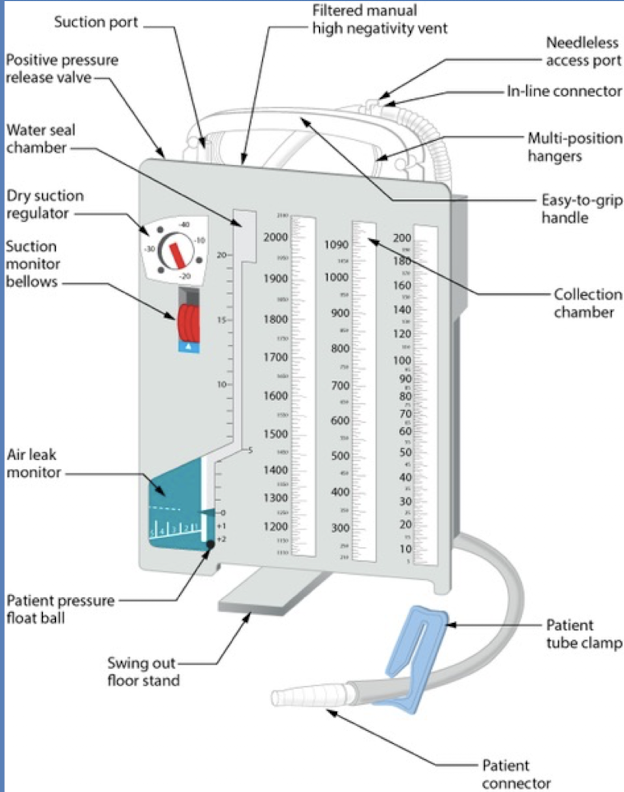
Three primary chest tube components
-Collection chamber (2500 mL)
-Water seal chamber (one-way valve)
-Suction control chamber
Assessment of Drainage
-Regularly measure (at least once a shift if not more) and document (on the drainage chamber markers- date, time, and initial)
-Check for any kinks or folds in the drainage tubing
-Notify the provider if: frank bleeding from insertion site or into drainage within first few hours of placement, Bleeding recurs after initial slowing, Other patient signs and/or symptoms indicate possible hermorrhage
-Encourage patient to independently reposition regularly
-Encourage frequent deep breathing with periodic coughing to promote fluid mobilization and drainage
Water Seal Function
-Air vent is in place to provide an escape for air leaving the pleural space
-Water seal is a one-way valve which prevents air re-entrance into the pleural space
-Tidaling is an appropriate fluctuation of fluid which occurs during respiration (rise with inspiration and fall with expiration)
-Will stop when the hung has re-expanded, the tubing is kinked, or the tubing is obstructed
-Intermittent bubbling in the water seal chamber is normal
-Continuous bubbling in the water seal chamber indicates an air leak
-The origin must be located quickly and search the tubing connections completely as the drainage system may require replacement
Assess the Suction Apparatus
-Ordering provider will specify suctioning requirement
-10-20 cm H20 is normal (the wall suction amount does not control the chest tube)
->50 cm may result in tissue compromise
-If drainage produced is inadequate, encourage the patient to cough and reposition
-Continuous gentle bubbling in the suction control chamber is normal
-Vigorous bubbling does not increase suction; only causes H2O to dissipate more quickly
Optimizing Chest Tube Function
-Always keep drainage system at least 2-3 feet lower than the insertion site
-Place upright on the floor near the bed (minimize tubing exposure due to fall risk)
-Avoid unnecessary clamping and prolonged clamping (unless considering removal)
-Ensure the tubing is not occluded
-Tubing should be long enough to promote safe ambulation
-Ensure that suction is maintained as ordered
-May be removed from suction (if permitted by the medical team) for ambulation and off-unit testing
Ongoing Assessment
-Assess every 2-4 hours, more frequently as needed
-Breath sounds, respiratory pattern and quality, pulse oximetry
-Chest symmetry, level of resonance, cyanosis, dyspnea, site complications
-In the case of tension pneumothorax, palpate thorax for crepitus (subQ emphysema)
-Educate the patient about the importance of incentive spirometry
-Dressing at site should be secure and changed per institutional policy: always have 2 additional clamps, normal sterile saline, and 4×4s at bedside
-Only clamp the tube under one (or more) of the following conditions:
-(1) per order, (2) checking for an air leak, (3) changing the drainage container, or (4) strongly considering removal
-Chest tube removal consideration and implementation is at the discretion of the medical team
-Document color, amount, quality of drainage at least once per shift, and mark drainage chamber
Nursing Responsibilities
-Include assisting with insertion, monitoring the patient’s status and response to the treatment, monitor the patency of the chest drainage system, patient education, and assisting with removal of the chest tube
-Once the tube is in place, monitor the patient’s response, including respiratory status and vital signs, check the site and site dressing, and maintain the patency and integrity of the drainage system
Complications
-Dramatic increase in chest tube drainage: note activity changes before this occurred, notify provider and reassess frequently, depending on the drainage and characteristics, may need to activate condition C
-Continuous bubbling in water seal chamber: Assess the insertion site, tubing, connections, and collection system for air leaks, Adjust the level of suction per orders if required
-Excess or deficiency of fluid in water seal chamber
-Excess: remove excess fluid with a syringe and needle through resealable diaphragm; do not invert to remove
-Deficiency: fill to required level with desired amount of sterile water or saline
-Collection system falls over or invers
-Orient to the appropriate position as soon as possible
-Assess to ensure all connections and tubing remains intact
Chest Tube removal
-Should be removed as early as safely possible to decrease pain and infection risk, and promote ambulation
-Pre-medicate roughly 30 minutes prior to removal (painful procedure)
-Patient clinical condition should be generally stable (or close-to-baseline)
-Radiograph may be conducted to ensure that pleural space has been adequately drained
-In most adults, total 24-hour discharge prior to removal should be less than 200-400mL (and not exudative)
-Clamping prior to removal or removal of suction
-Chest radiograph may be conducted within 3 hours post-removal, or with acute status changes post-removal