Pharm - GI
1/174
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
175 Terms
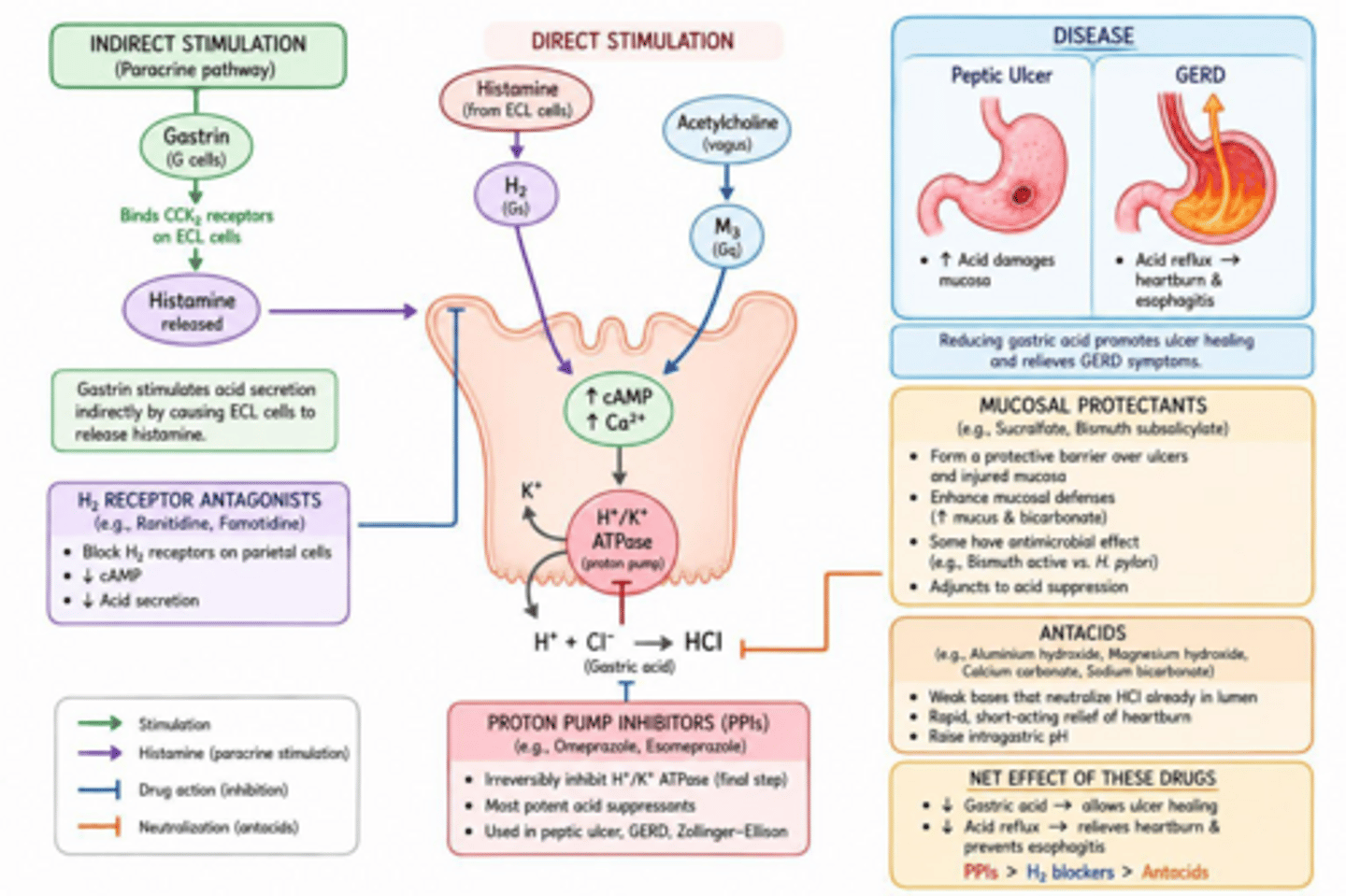
What are the three primary ways drugs work to treat Peptic Ulcer Disease (PUD)?
Reduce gastric acid secretion, increase mucosal resistance, or kill pathogens (H. pylori).
How does an ulcer differ from an erosion pathologically?
An ulcer extends through the muscularis mucosa; an erosion is superficial and does not.
What is the most common cause of gastric and duodenal ulcers?
H. pylori.
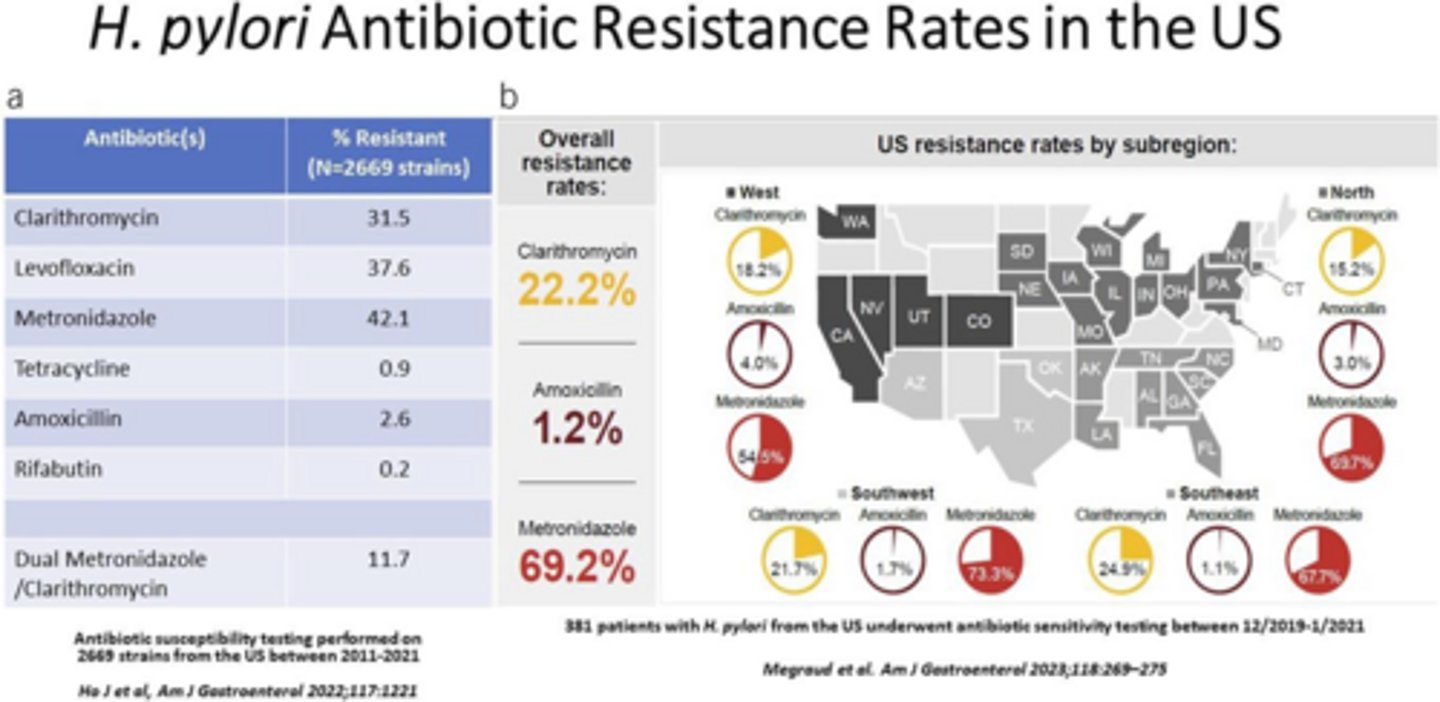
H. pylori has lots of resistance to which antibiotics?
Metronidazole, clarithromycin and levofloxacin.
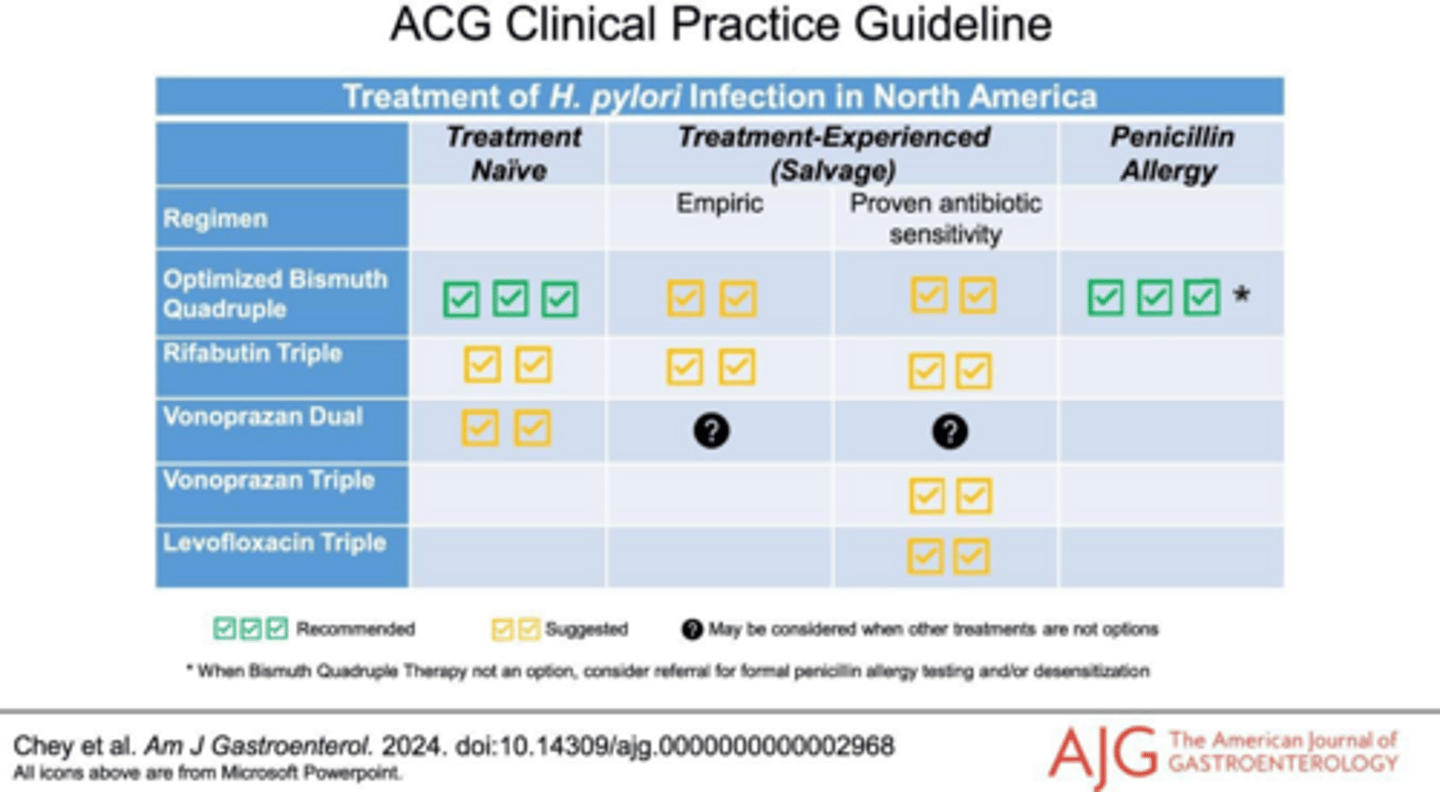
What is the preferred treatment-naïve regimen for H. pylori infection?
Bismuth Quadruple Therapy (BQT) for 14 days.
What are the components of Bismuth Quadruple Therapy (BQT)?
Standard-dose PPI, bismuth subsalicylate (300mg 4x daily), tetracycline (500mg 4x daily), and metronidazole (500mg 3 or 4x daily).
Which H. pylori regimen is considered 'least preferred' due to resistance?
PPI Triple Therapy (PPI + Clarithromycin + Amoxicillin).
What is the preferred next option if BQT fails in H. pylori treatment?
Rifabutin triple therapy (Omeprazole + Amoxicillin + Rifabutin).
How long should all H. pylori treatment regimens last?
14 days.
Why should omeprazole and lansoprazole be avoided in CYP2C19 rapid metabolizers?
They are eliminated faster, resulting in lower intragastric pH and reduced effectiveness.
Which agents are preferred for H. pylori in CYP2C19 rapid metabolizers?
Esomeprazole, rabeprazole, or vonoprazan (vonoprazan bypasses CYP2C19-dependent acid suppression)
When should H. pylori eradication be confirmed with testing?
4 weeks after therapy completion and ≥2 weeks after stopping PPIs.
What is the standard dose of Lansoprazole for H. pylori treatment?
30 mg BID.
What is the standard dose of Omeprazole, Rabeprazole and Esomeprazole for H. pylori treatment?
20 mg BID.
What is the standard dose of Pantoprazole for H. pylori treatment?
40 mg BID (though non preferred option due to weaker acid inhibitory effect)
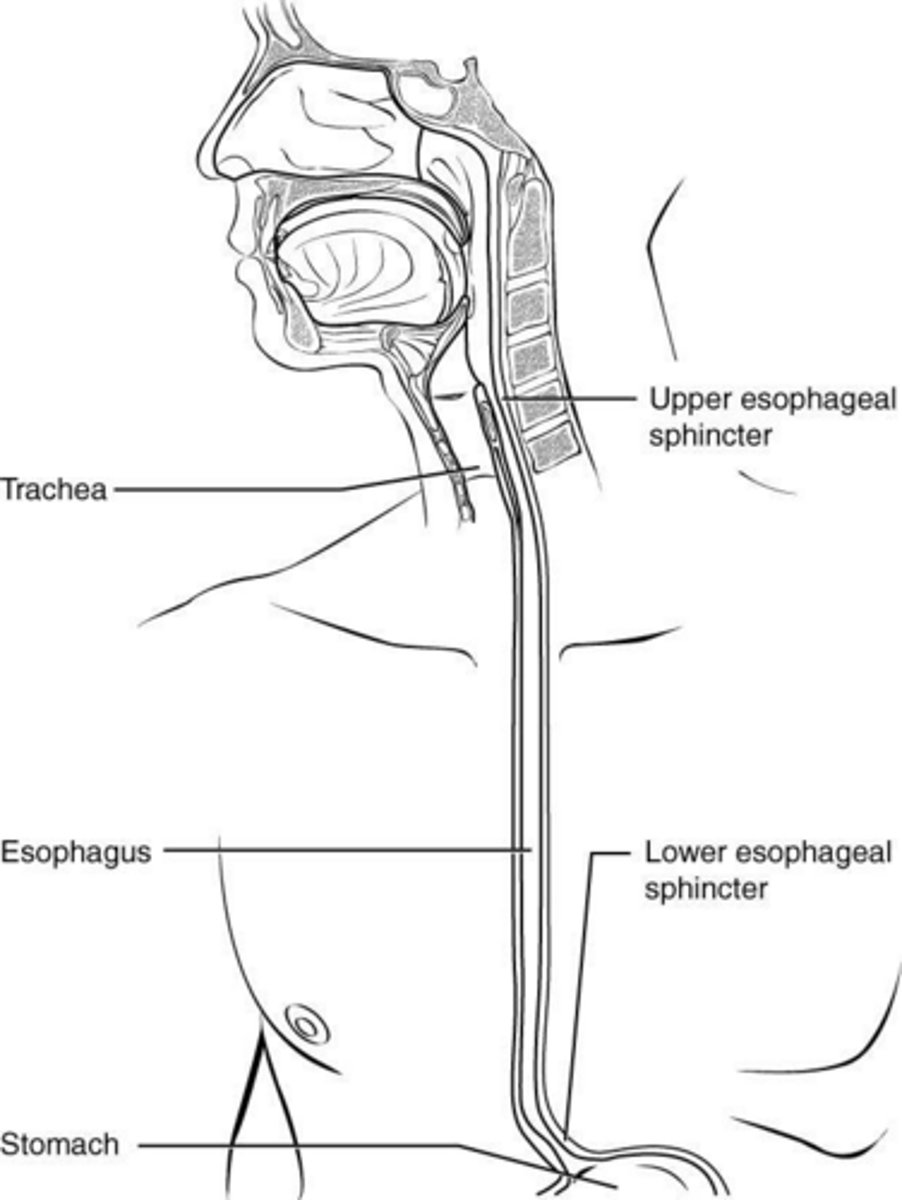
What physiological mechanism causes Gastroesophageal Reflux Disease (GERD)?
Lower esophageal sphincter (LES) relaxation and pressure allowing stomach acid to rise.
Which medications can decrease LES pressure and worsen GERD?
Anticholinergics, caffeine, CCBs, dopamine, estrogen, progesterone, nitrates, nicotine, theophylline, and tetracycline.
Which medications can directly irritate the esophageal mucosa?
NSAIDs, bisphosphonates, iron, and potassium.
What are the goals of GERD treatment?
Decrease sx, prevent progression, promote mucosal healing and prevent complications.
What are the non-pharmacologic lifestyle modifications for GERD?
Weight loss, elevate head of bed, smoking cessation, and avoiding late meals.
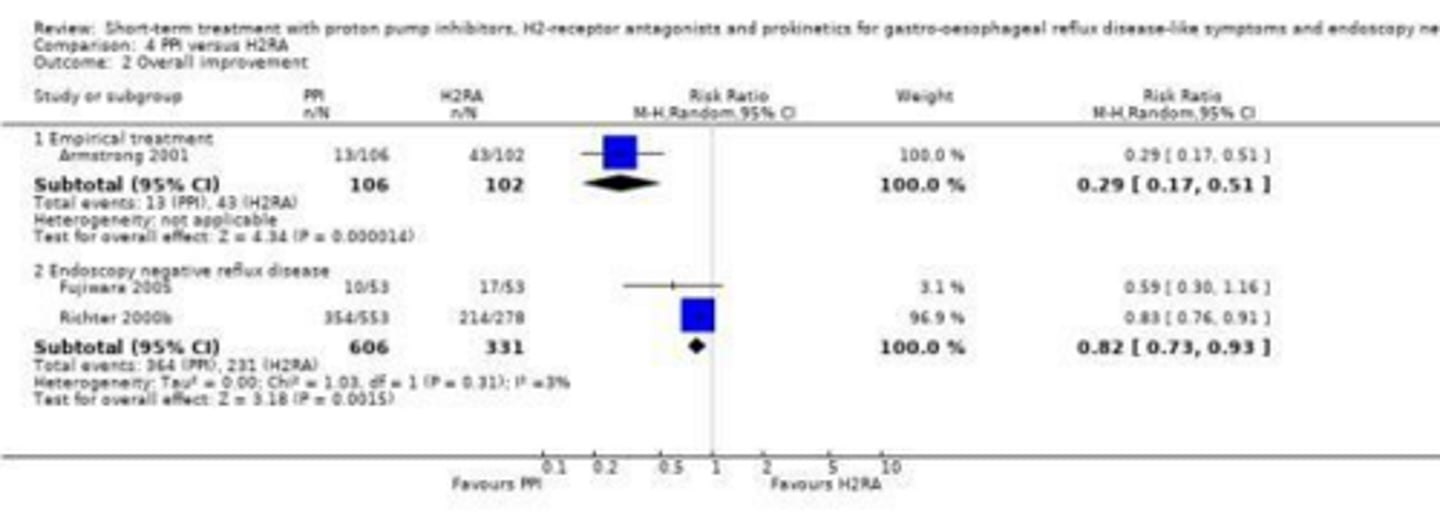
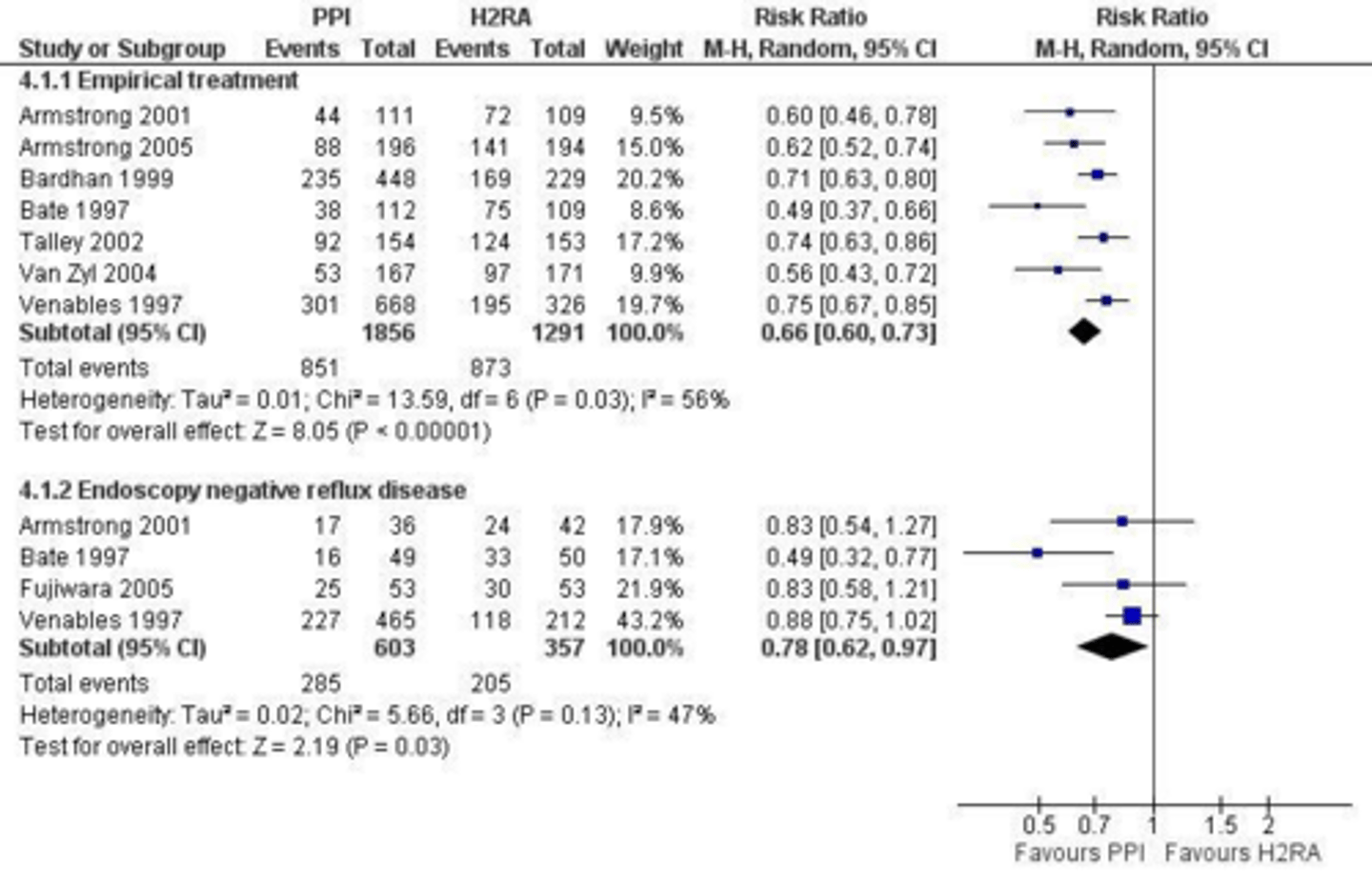
What is the most effective medical treatment for GERD?
Proton pump inhibitors (PPIs).
What are the conditions for OTC treatment of GERD?
Mild intermittent symptoms (<2x a week and not troublesome)
What are the options for OTC treatment of GERD?
PRN antacids only, H2RA BID (or PRN) +/- PRN antacids, PPI daily +/- PRN antacids.
What is the OTC treatment limit for PPIs before seeing a provider?
2 weeks.
What are the conditions for Rx for GERD?
Moderate-severe, persistent symptoms (≥2x week or troublesome)
What are the options for Rx treatment for GERD?
PPI daily x 4-8 weeks (+/- PRN antacids) or H2RA BID X 6-12 weeks (+/- PRN antacids)
What is 'Step up' therapy in GERD?
Starting with non-pharm, then H2RA, then PPI.
What is 'Step down' therapy in GERD?
Starting with a PPI and stepping down to an H2RA.
How is refractory GERD with nocturnal acid breakthrough often managed?
Increase PPI dose, switch PPIs, or add an H2RA at bedtime.
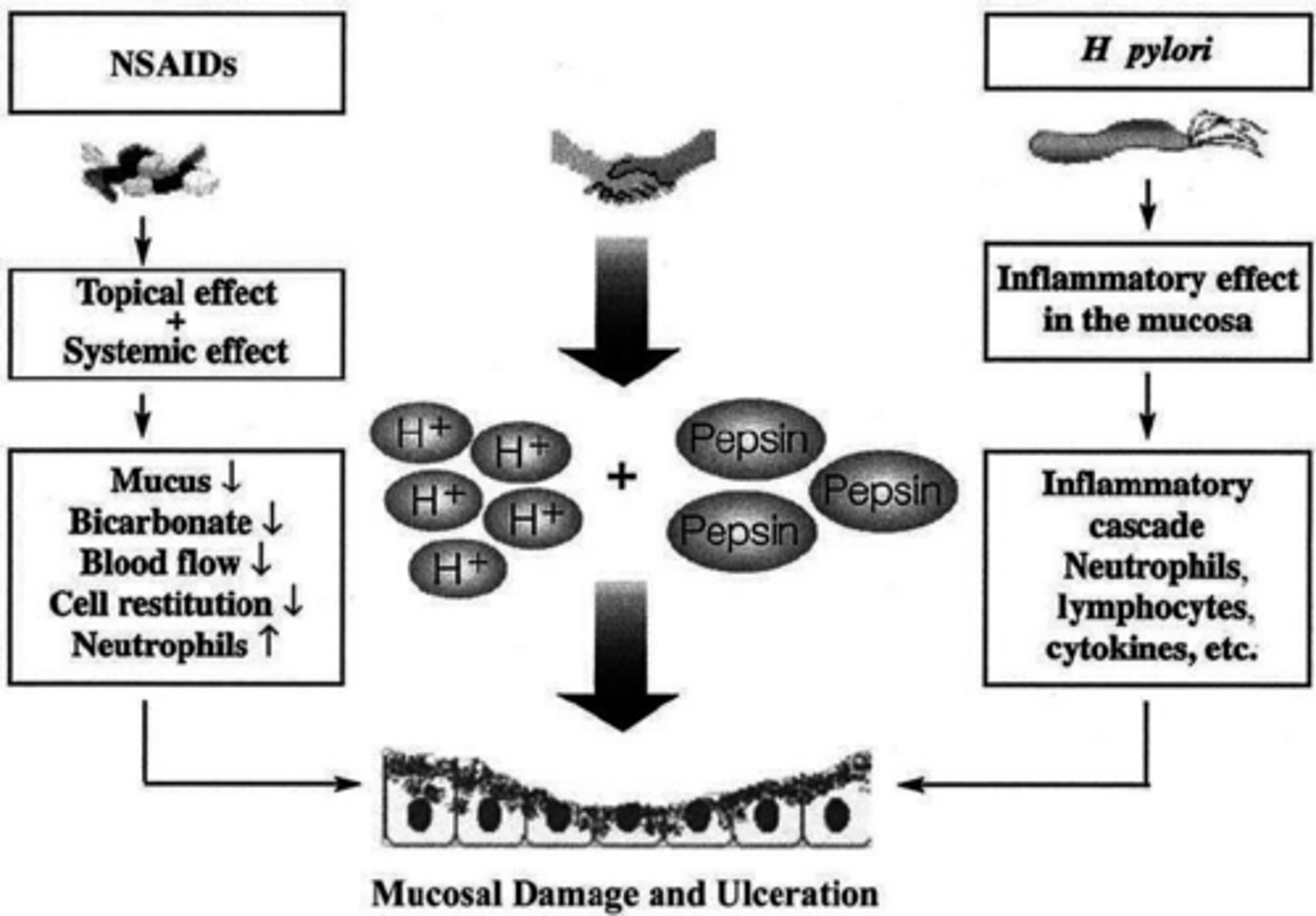
How do NSAIDs cause GI ulcers?
They inhibit COX-1, decreasing protective prostaglandins, mucus, bicarbonate production, blood and leading to direct inflammation.
What are the BBW of NSAIDs?
MI, stroke, GI bleeding.
Which NSAID is COX-2 selective and carries lower GI risk?
Celecoxib (Celebrex).
Which NSAID is highly COX-1 selective and carries the highest GI risk?
Ketorolac.
What are the primary risk factors for NSAID-induced PUD?
Age >65, high dose NSAIDs, previous PUD, and concomitant anticoagulant or steroid use.
What is the preferred pharmacologic prevention for NSAID-induced ulcers?
Take NSAIDs with food, change NSAID to COX-2 selective NSAIDs or PPI or misoprostol.
What are the treatment options for NSAID induced ulcers?
PPI daily x 4 weeks (works best), H2RA x 6-8 weeks, or Misoprostol. Could also decrease NSAID dose, d/c NSAID or use alternative like APAP or Celecoxib.
What is the primary cause of Stress-Related Mucosal Damage (SRMD)?
Decreased blood flow to the gastric mucosa.
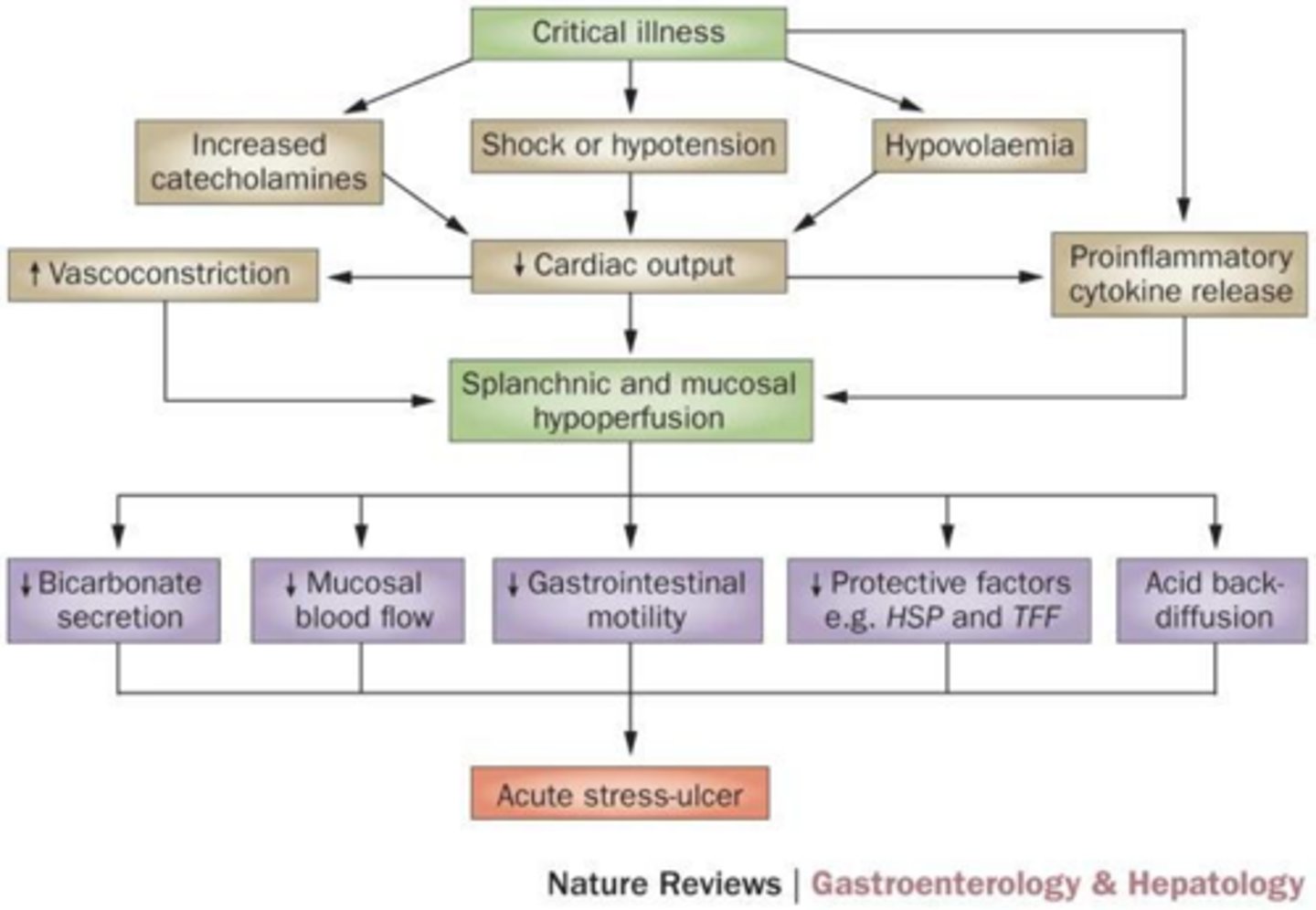
What are the two major risk factors for SRMD in the ICU?
Mechanical ventilation (>48 hours) and coagulopathy.
What is the goal GI pH for SRMD prophylaxis?
Maintain pH >4, or provide mucosal protection.
What is used for prophylaxis for SRMD?
H2RA like IV or PO Famotidine (has the most evidence), or PPIs or Sucralfate. H2RA and PPI help with maintaining pH >4, Sucralfate helps with mucosal protection.
When should SRMD prophylaxis be discontinued?
When discharged from ICU and/or RF no longer present.
Which drugs are PPIs?
Ending is -prazole.
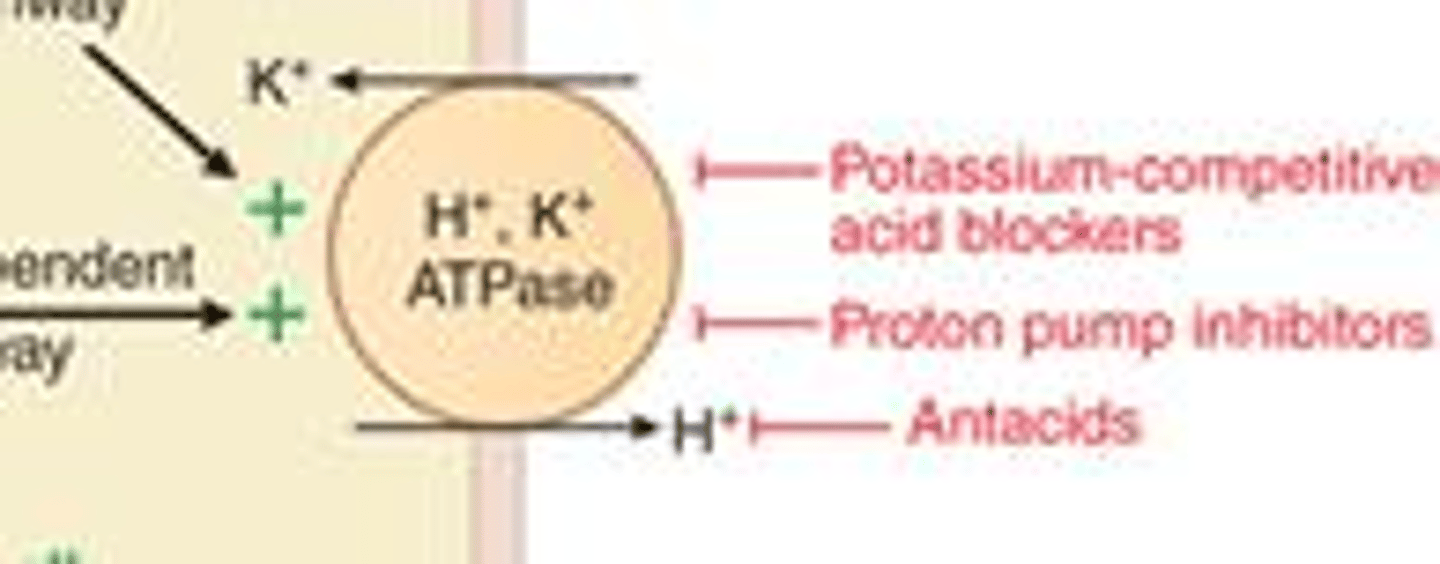
What is the mechanism of action of Proton Pump Inhibitors (PPIs)?
Irreversibly inhibit (H+/K+)-ATPase pumps, decreasing gastric acid secretion. They are prodrugs that require acid to activate them.
How long does it take for PPIs to reach steady-state acid suppression?
3-5 days.
What are the ADE of PPIs?
Abdominal pain, GI issues, dizziness, HA (generally well tolerated)
What are the potential long-term adverse effects of PPIs?
Increased risk of pneumonia, C. diff, fractures, and magnesium/B12 deficiencies.
Why should PPIs be tapered over 4-6 weeks?
To prevent rebound acid hypersecretion.
Which PPIs have the highest risk of reducing clopidogrel (Plavix) efficacy?
Omeprazole and esomeprazole (via CYP2C19 inhibition). Pantoprazole and Rabeprazole have lowest risk.
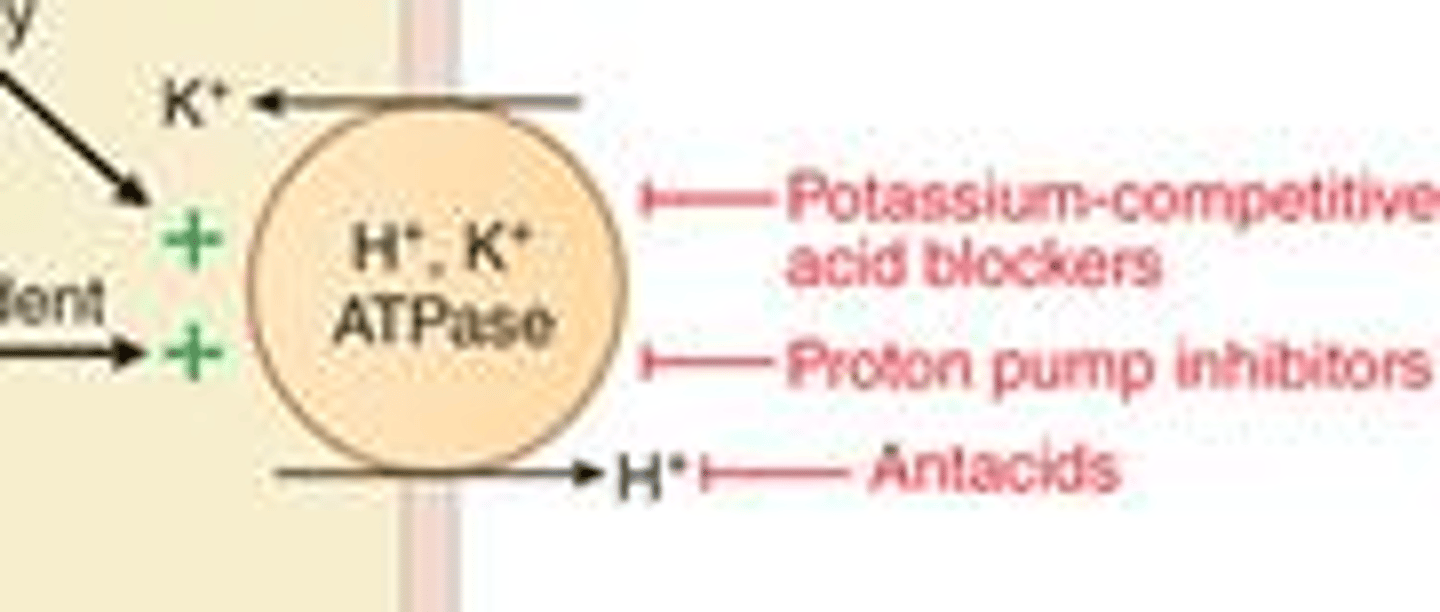
What is the mechanism of action of Vonoprazan (Voquenza)?
Potassium-competitive acid blocker (PCAB) that inhibits (H+/K+)-ATPase pumps.
What is a major advantage of Vonoprazan over PPIs?
Does not require acid activation or premeal dosing; works within 2-3 hours. Greatest advantage in severe erosive esophagitis and in maintenance of healing.
What are the ADEs of Vonoprazan?
GI, HTN, UTI. Generally well tolerated.
Which drugs are H2RAs?
Ending in -tidine.
What is the mechanism of action of H2RAs (Histamine-2 Receptor Antagonists)
Inhibit H2 receptors to decrease gastric acid secretion. Work in 30 minutes, last 4-10 hours.
What are the ADE of H2RAs?
GI, dizziness, HA, can cause confusion, hallucinations in older adults with renal/hepatic impairment due to its anticholinergic activity.
Which H2RA requires renal dose adjustment when CrCl <50?
Famotidine.

Which H2RA is associated with gynecomastia and significant CYP450 drug interactions?
Cimetidine.
Which H2RA is most likely to cause DDI?
Cimetidine because it inhibits CYP1A2, 2C19, and 3A4. Watch out for warfarin, phenytoin, theophylline and lidocaine.
What is the MOA of antacids?
They directly neutralize stomach acid. Works within 5 minutes, lasts about 30 minutes.

Which drugs/combo of drugs are antacids?
Aluminium + Mg, Calcium carbonate, Ca + Mg, Mg hydroxide, Na bicarb, to name a few.
What is the primary side effect of aluminum-containing antacids?
Constipation. Rare: bone demineralization and GI obstruction.
What is the primary side effect of calcium-containing antacids?
Constipation. Rare: hypercalcemia.
What is the primary side effect of magnesium-containing antacids?
Diarrhea. Rare: anti-arrhythmias, respiratory depression, hypotension, muscle paralysis.
What is the primary side effect of sodium-containing antacids?
Hypernatremia (avoid in HF, HTN, CKD, edema and cirrhosis)
What are some pearls about antacids?
Take after meals and at bedtime, low efficacy usually used PRN, and separate >2 hours from other meds to prevent decreased absorption (like tetracyclines and fluoroquinolones)
What is the mechanism of action of Sucralfate?
Binds to positively charged proteins in the ulcer base to create a barrier.
What are the ADE of Sucralfate?
Constipation.
What are some pearls of Sucralfate?
Used for GERD/pregnancy or ulcers, dosed 4x day, separate by >2 hours from other meds.
What is the MOA of Bismuth subsalicylate (pepto bismol)?
Anti-secretory, anti-microbial, and anti-inflammatory.
What are the adverse effects of Bismuth subsalicylate?
Black-colored stool/tongue, tinnitus, GI issues, bleeding and neurotoxicity.
What are the OTC CI of Bismuth subsalicylate?
Allergy, GI ulcer or active bleeding. Also don't give to kids with viral illness (Reye's syndrome risks!)
What is the GI indication and MOA of Misoprostol?
Prevention of NSAID-induced ulcers; prostaglandin E2 analogue that suppresses acid and promotes mucus.
What are the ADE of Misoprostol?
Dose-related diarrhea (13-40%) and abdominal pain (7-20%)
What is the BBW for Misoprostol?
CI in pregnancy, because it stimulates uterine cx.
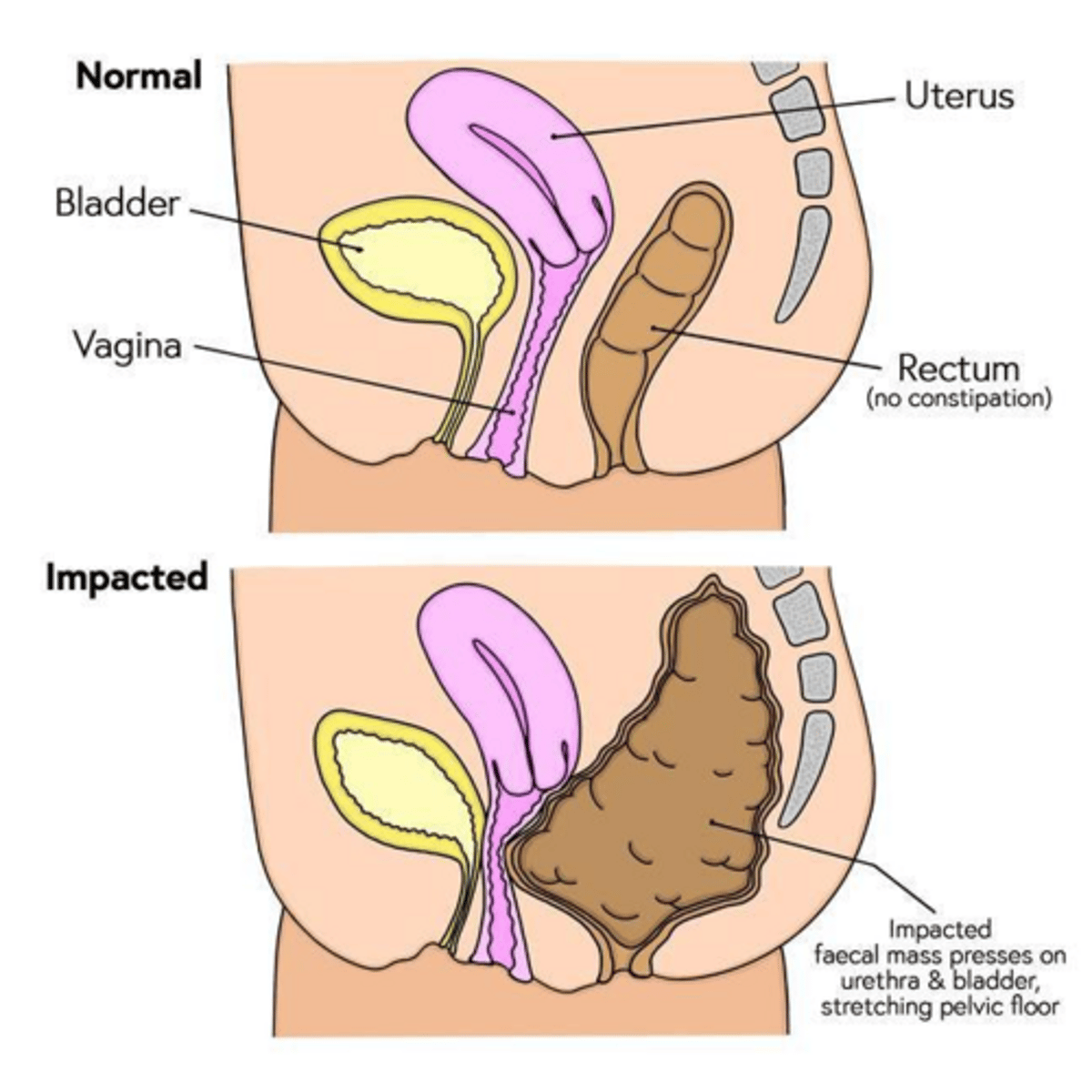
What are the Rome IV criteria for functional constipation?
≥2 of: <3 BM/week, straining, lumpy/hard stools, incomplete evacuation, or blockage feeling.
Which common medications cause constipation?
Iron, aluminum/calcium antacids, anticholinergics, verapamil, and opioids.
What are some non-pharmalogical treatments for constipation?
Address causes, increase fluids, increase fiber.
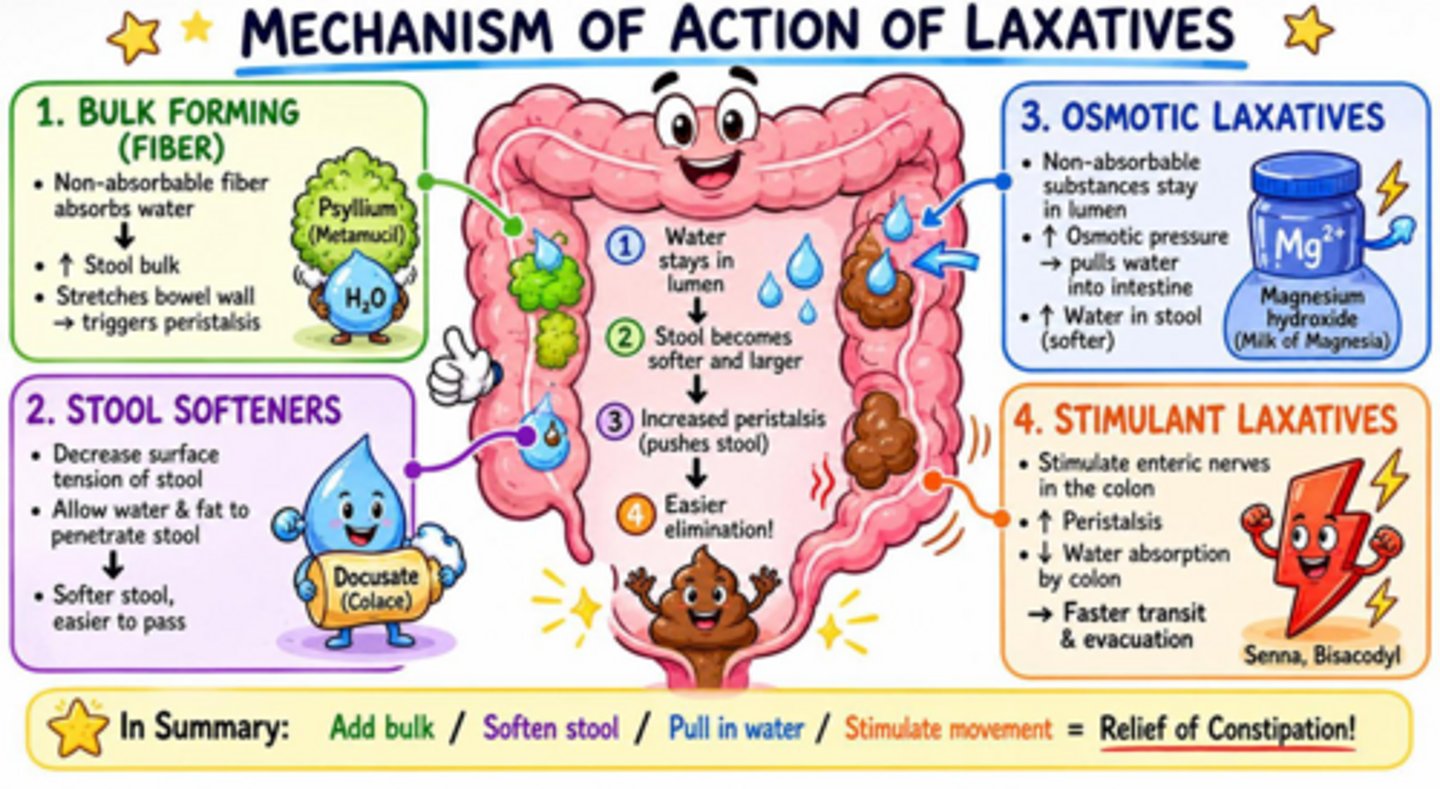
How do bulk-forming laxatives like Psyllium work?
Absorb water to increase bulk, which stimulates peristalsis.
Which fibers are soluble fibers?
Calcium polycarbophil, psyllium and wheat dextrin.
Which fibers are insoluble fibers?
Methylcellulose.
What are the ADE of Bulk forming fibers?
Abdominal pain, bloating, cramping, flatulence.
What are pearls for bulk forming fibers?
Need to take with at least 8 oz water and takes 12hr-3 days to work (best for maintence/prevention)
What is the standard dose and MOA of Docusate (stool softener)
50-100 mg daily; surfactant that allows water/oils to penetrate stool.
How do stimulant laxatives like Bisacodyl and Senna work?
Stimulate enteric nerves to increase peristalsis and water secretion.
What are the ADE of Stimulants?
Nausea, cramping, electrolyte imbalances. Senna can change urine to red-orange color. Rectal irritation/pain
What are the pearls for stimulants?
Orla bisacodyl takes 6-12 hrs to work, suppositories take 15-60 minutes. Can cause dependence if used long term.
What is the standard dose and MOA of PEG 3350 (Osmotics, like MiraLax)?
17 grams daily; osmotic agent that draws fluid into the colon.
What are other examples of Osmotics?
Glycerin, Lactulose, and Sorbitol.
What are the ADE of Osmotics?
Nausea, cramping, flatulence, electrolyte imbalances. Rectal irritation/pain
What are the pearls for osmotics?
PEG/Lactulose work in 1-3 days, Glycerin/sorbitol work in 15 to 60 minutes.
What is the MOA of Lubricants?
Decrease water absorption and lubricates intestines.
What is used as lubricant?
Mineral oil and castor oil.
What are the ADE of Lubricants?
Anal leakage, pain and aspiration (must stay upright after taking)
Which laxative class can cause decreased absorption of fat-soluble vitamins (ADEK)?
Lubricants (Mineral oil).
In what population should lubricants be avoided?
Pregnant (castor oil can cause uterine cx), <6 yo, elderly, bedridden, or have difficulty swallowing.
What are the Rx options for constipation treatment?
Lubiprostone, Plecanatide, Linaclotide, Prucalopride.
When is Lubiprostone indicated?
Chronic idiopathic constipation, IBS-C in women ≥ 18 years, and opioid-induced constipation.
What is the mechanism of action of Lubiprostone (Amitiza)?
Chloride channel activator.
What are the ADRs of Lubiprostone?
Nausea (most common), diarrhea, gas, bloating, HA (most common non-GI ADR)
What are the common medication causes of diarrhea?
Magnesium, antibiotics, PPIs, NSAIDs, Metformin, and GLP-1 RAs.
What are the exclusions for self-treatment of diarrhea?
Fever, severe pain, blood in stool, pregnancy, or symptoms >72 hours.