N260 Exam #2 Study Guide
1/14
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
15 Terms

Anxiety (12 Q’s)
Anxiety: is an emotional response to anticipation of danger. It is not the same as stress. Anxiety becomes problematic when it becomes disabling that an individuals functioning on a daily basis is adversely affected.
Signs & Symptoms of Generalized Anxiety Disorder
Generalized Anxiety Disorder (GAD): The presence of excessive anxiety and worry about a variety of topics, events, or activities
Worry occurs more often than not for at least 6 months and is clearly excessive
The worry is experienced as very challenging to control
The worry in both adults and children may easily shift from one topic to another
Symptoms:
Edginess or restlessness
Tiring easily; more fatigued than usual
Impaired concentration or feeling as though the mind goes blank
Irritability (may or may not be observed by others)
Increased muscle aches or soreness
Difficulty sleeping
“Caught in an endless loop”
Similar to MDD, pts w/ GAD are so overwhelmed by the “anxiety loop” that they become irritable, indecisive, and lose motivation to participate in life
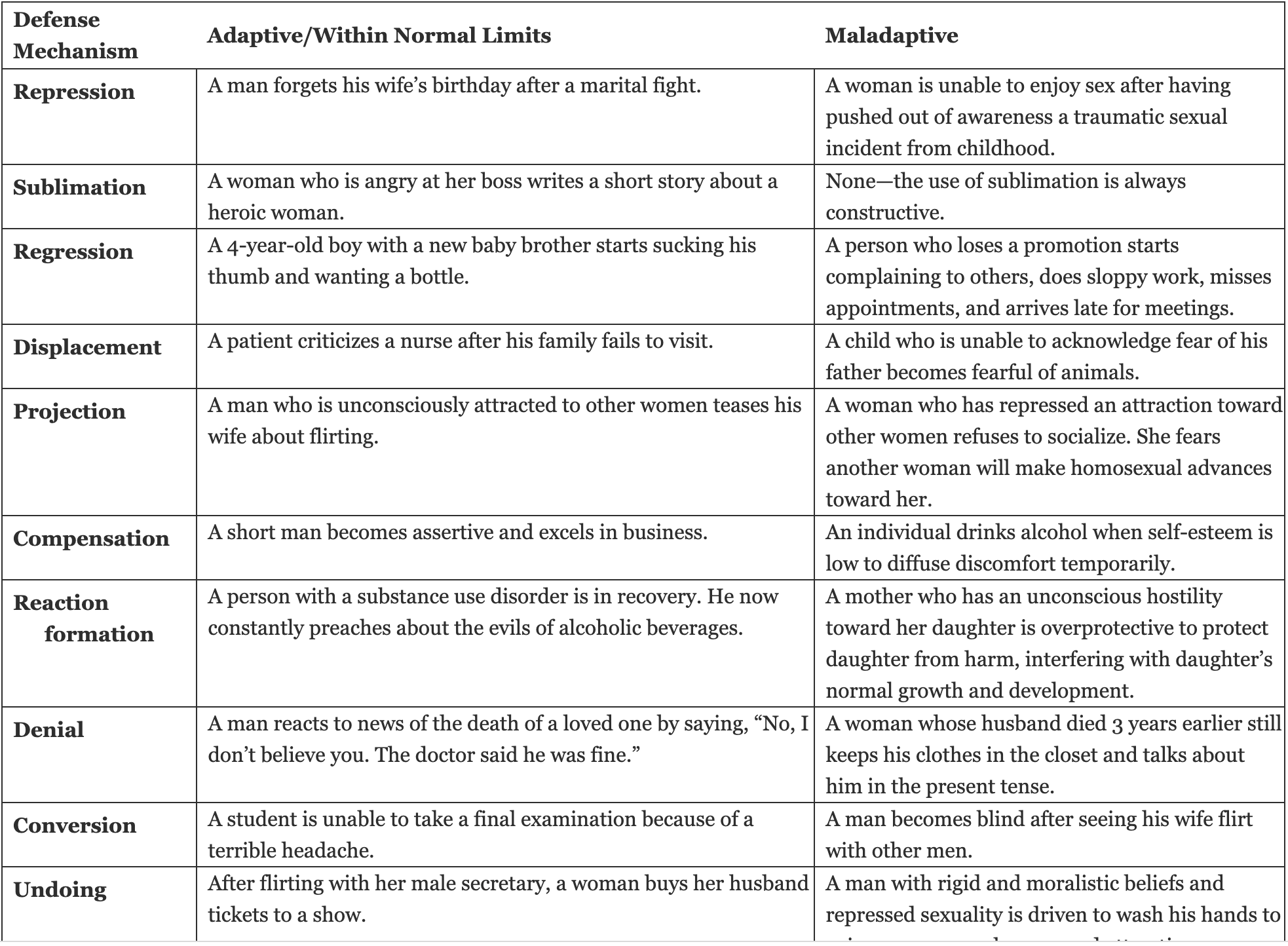
Defense Mechanisms of GAD
Defense mechanisms serve to help the pt subconsciously distance themselves from unwanted feelings and prevent new unwanted ones from forming. Tension reduction is the overall goal of defense mechanisms. It is protective
Projection is highlighted in your materials as an immature defense mechanism where:
A person unconsciously rejects emotionally unacceptable personal features
Attributes those unacceptable traits to other people, objects, or situations
Manifests as blaming, scapegoating, prejudicial thinking, and stigmatization
Can be associated with paranoia
Example: People who always feel others are out to deceive or cheat them may be projecting their own characteristics that they find distasteful and cannot consciously accept.
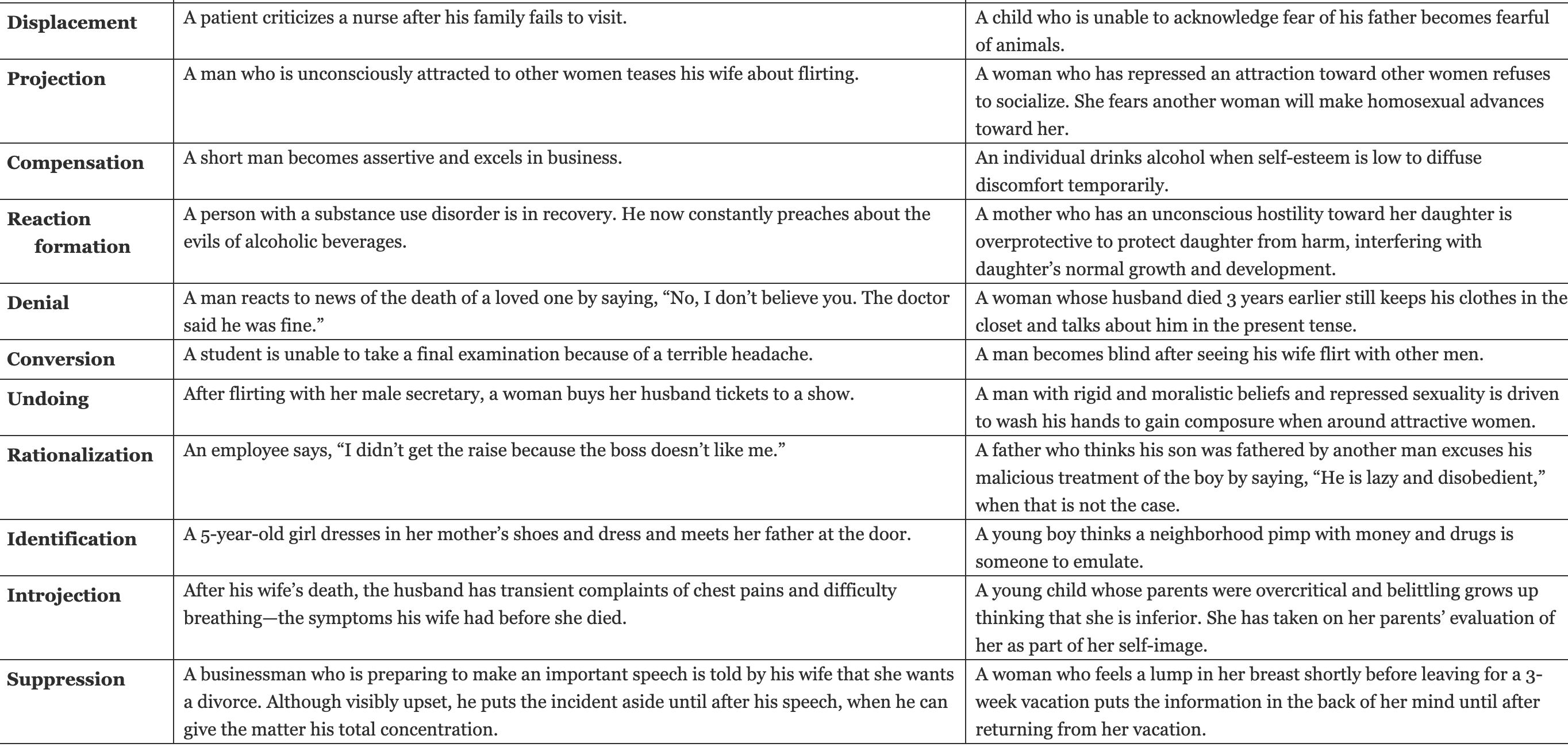
Other defense mechanisms:
Conversion
Compensation
Denial
Displacement
Identification
Idealization
Intellectualization
Introjection
Isolation
Rationalization
Reaction formation
Regression
Repression
Splitting
Sublimation
Suppression
Undoing
Healthy Defenses
Altruism → in altruism, emotional conflicts and stressors are addressed by meeting the needs of others. Unlike self-sacrificing behavior, in altruism, the person receives gratification either vicariously or from the response of others.
Six months after losing her husband in a car accident, Jeanette began to spend 1 day a week doing grief counseling with families who had lost a loved one. She found that she was effective in helping others in their grief, and she obtained a great deal of satisfaction and pleasure from helping others work through their pain.
Humor → Humor makes life easier. An individual may deal with emotional conflicts or stressors by emphasizing the amusing or ironic aspects of the conflict or stressor through humor.
A man is interviewed for a job by the top executives of a company. He has recently had foot surgery, and on entering the interview room, he stumbles and loses his balance. There is a stunned silence, and then the man states calmly, “I was hoping I could put my best foot forward.” With everyone laughing, the interview continues in a relaxed manner.
Suppression is the conscious denial of a disturbing situation or feeling.
A student who is studying for the state board examination says, “I can’t worry about paying my rent until after my exam tomorrow.”
GAD Outcomes
Generalized anxiety disorder (GAD) is characterized by excessive anxiety and worry about a number of events and activities. People with GAD find it difficult to shake their concerns and report being unable to relax. It is sometimes referred to as the “worry disease” (What if I’m late? … What if I fail? … What if I am fired?). A diagnosis of GAD is made if at least three of the following symptoms are present: restlessness, fatigue, poor concentration, irritability, muscle tension, and sleep disturbance
When planning care for patients with GAD, outcomes focus on reducing anxiety symptoms and improving coping abilities. Here are the key desired outcomes:
Symptom Management Outcomes
Reduced Anxiety Levels:
Decreased frequency and intensity of worry
Reduction in "what if" thinking patterns
Improved ability to control excessive worry
Decreased physical symptoms (muscle tension, fatigue, restlessness, sweating, nausea)
Improved Cognitive Function:
Better concentration and focus
Enhanced decision-making ability
Reduced fear of making mistakes
Functional Outcomes
Effective Coping:
Patient demonstrates use of healthy coping strategies
Engages in stress-reduction techniques (breathing exercises, progressive muscle relaxation, guided imagery)
Practices positive self-talk and challenges negative thinking
Participates in support groups or therapy
Daily Functioning:
Returns to normal activities of daily living
Maintains work/school performance
Sustains healthy relationships
Manages responsibilities effectively
Behavioral Outcomes
Active Participation in Treatment:
Engages in psychotherapy (CBT, ACT, or other evidence-based approaches)
Adheres to medication regimen if prescribed (SSRIs, buspirone)
Practices cognitive restructuring techniques
Uses relaxation and mindfulness strategies
Family/Caregiver Outcomes:
Family members understand the condition
Support system is engaged in patient's care
Family demonstrates effective coping with patient's anxiety
Timeline Considerations
Outcomes may be short-term or long-term depending on:
Severity of symptoms
Patient's coping response
Nature of the stressor
Available support systems
Remember: Coping with stress takes time. Ongoing communication and reassessment are essential to evaluate whether interventions are promoting adaptation and whether the patient's expectations are being met.
Nursing interventions for GAD
Actively listen to the individual and encourage exploration of feelings
Reassure individual about their safety
Validate their feelings and concerns
Explore alternative/new coping strategies
Help acknowledge anxiety rather than deny or intellectualize it
Assist in identifying behaviors that indicate individual is feeling anxious
Assist pt w/ connecting anxiety w/ uncomfortable physical, emotional, or behavioral responses
Discourage use of caffeine, alcohol, or drugs to “calm nerves”
Provide information
Teach the pt and family/significant others about anxiety disorders
Educate pts about the signs and symptoms of the disorder
Support treatment adherence
Promote care of self including nutrition and sleep
Access informatics that can provide patients w/ information and learning
Assessment of Anxiety/Recognizing Cues
Assess and acknowledge presence of anxiety (behavioral and somatic symptoms)
Assess pt’s perception of the situation
Evaluate psychosocial stressors and developmental issues
Assess for suicidal ideation, intent, and/or plan
Conduct a head to toe assessment w/ vital signs
Explore hx of mental illness or substance use
Assess pt’s ability to focus and concentrate
Observe and assess pt’s speech
Assess current coping mechanisms
Request labs including thyroid, function, blood, glucose, echo, tox screen
GAD-7 screening tool
The Generalized Anxiety Disorder Scale-7 (GAD-7) is a validated screening instrument mentioned in your textbook materials for assessing anxiety disorders, particularly in perinatal populations.
What is the GAD-7?
The GAD-7 is a brief, 7-item self-report questionnaire that screens for the presence and severity of generalized anxiety disorder. It asks patients how often they've been bothered by anxiety symptoms over the past 2 weeks.
Clinical Use
Your textbook specifically mentions the GAD-7 as one of the screening tools for anxiety disorders in pregnant and postpartum women, alongside:
Edinburgh Postnatal Depression Scale (EPDS)
Perinatal Anxiety Screening Scale
Patient Health Questionnaire-9 (PHQ-9)
Scoring & Interpretation
The GAD-7 uses a 0-3 point scale for each item:
0 = Not at all
1 = Several days
2 = More than half the days
3 = Nearly every day
Total scores range from 0-21:
0-4: Minimal anxiety
5-9: Mild anxiety
10-14: Moderate anxiety
15-21: Severe anxiety
A score of 10 or higher typically warrants further evaluation and possible intervention.
Symptoms Assessed
The GAD-7 evaluates core GAD symptoms including:
Feeling nervous, anxious, or on edge
Not being able to stop or control worrying
Worrying too much about different things
Trouble relaxing
Being restless
Becoming easily annoyed or irritable
Feeling afraid something awful might happen
Nursing Implications
Positive screening results require:
Further comprehensive assessment
Appropriate referrals
Prompt treatment initiation
Follow-up screening to monitor progress
The effectiveness of screening depends on proper follow-up for positive results to ensure patients receive needed care.
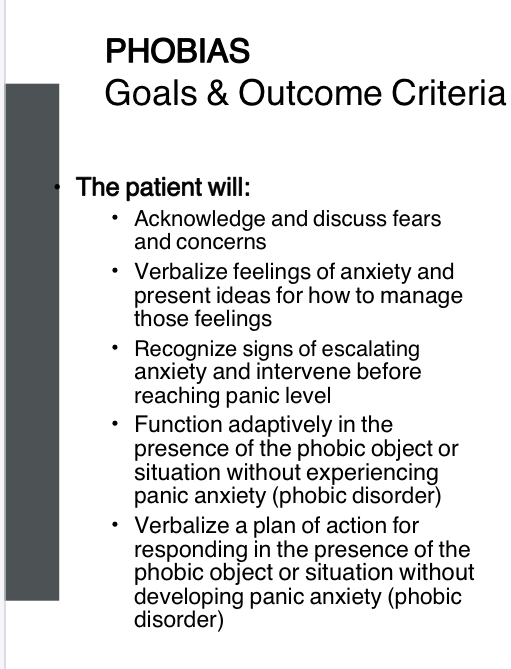
Phobias
An irrational and disproportionate fear of an object or situation
Person is generally aware that the fear is unreasonable and excessive
Pts have overwhelming symptoms of panic when exposed to phobic stimulus. Remove the stimulus, the anxiety goes away.
Diagnosis made only if avoidant behavior causes problems in functioning (occupational social relationships) or if pt is distressed about having the fear
Cognitive Behavioral Therapy (CBT) is among the most evidence-based therapies for treating phobias, including social anxiety disorder and agoraphobia. CBT examines how negative thoughts contribute to anxiety and how individuals behave in situations that trigger fear.
Key CBT Components:
Challenges cognitive distortions through cognitive restructuring
Teaches that our thoughts, not external events, affect how we feel
Helps identify "automatic" thoughts that trigger anxiety
Acceptance and Commitment Therapy (ACT) is an action-oriented approach where patients:
Learn to accept distressing emotions as appropriate to certain situations
Commit to making behavioral changes despite anxiety
Has research support for treating social anxiety disorder
Behavioral Therapy Techniques
Behavioral therapies are based on the premise that all behaviors are learned and unhealthy behaviors can be unlearned. Common techniques include:
Exposure Therapy - Gradual exposure to feared situations
Relaxation Training:
Breathing exercises
Progressive muscle relaxation
Guided imagery
Meditation (helps enter a state of relaxation or restful alertness)
Important Note: While relaxation techniques help reduce anxiety symptoms, there's no good evidence these techniques alone effectively treat phobias. They work best as components of other evidence-based behavioral therapies.
Pharmacological Interventions
Antidepressants (SSRIs):
Help reduce anxiety in phobias
Particularly effective for agoraphobia
Can treat comorbid depression
Anxiolytics (Benzodiazepines):
May be used for short-term anxiety relief
Examples: diazepam, alprazolam
Nursing Interventions
Empowerment through education about:
The nature of phobias
Treatment options
Coping strategies
Sensory interventions:
Music therapy
Aromatherapy
Behavioral interventions combined with cognitive strategies like encouraging positive self-talk and questioning negative thinking
Behavioral
Systemic desensitization
creation of graduate exposure to the fear of the stimuli. Encouraged to refrain from using avoidance response
Implosion
Bombarding or flooding the pt with an exaggerated version of the phobic stimuli
Education → concept that phobias are learned behaviors that can be unlearned and discuss how new behaviors can be learned
Agoraphobia interventions
Psychotherapy (First-Line Treatment)
Cognitive Behavioral Therapy (CBT) is the most evidence-based treatment for agoraphobia. CBT helps patients:
Identify and challenge cognitive distortions about feared situations
Understand that thoughts, not external events, drive anxiety
Restructure negative thinking patterns through cognitive restructuring
Exposure Therapy (a behavioral technique) is particularly effective for agoraphobia:
Gradual, systematic exposure to feared situations (crowded places, public transportation, open spaces)
Helps "unlearn" conditioned fear responses
Based on the premise that unhealthy behaviors can be changed through new learning
Acceptance and Commitment Therapy (ACT):
Teaches acceptance of distressing emotions in certain situations
Focuses on committing to behavioral changes despite anxiety
Action-oriented approach stemming from traditional CBT
Behavioral Techniques
Relaxation Training (used as adjuncts to therapy):
Breathing exercises
Progressive muscle relaxation
Guided imagery
Meditation for restful alertness
Important: These techniques help reduce symptoms but aren't effective alone—they must be combined with evidence-based therapies like CBT.
Pharmacological Treatment
Antidepressants (SSRIs/SNRIs):
Most widely prescribed for long-term anxiety treatment
Effective for agoraphobia
Treat cooccurring depression
Caution: Start with low doses due to activating effects that may temporarily increase anxiety
Must be tapered slowly when discontinuing to prevent withdrawal syndrome
Anxiolytics (Benzodiazepines):
Short-term anxiety relief only
Examples: diazepam, alprazolam
Not recommended for long-term use
Nursing Interventions
Education: Empower patients with knowledge about agoraphobia and treatment options
Encourage positive self-talk and questioning negative thinking
Sensory interventions: Music therapy, aromatherapy
Support therapy adherence and practice of coping skills
Monitor medication response and side effects
Combined Approach
Psychotherapy and pharmacotherapy are frequently used together for optimal outcomes, especially when patients have barriers to accessing therapy alone.
Panic attack
Recognize the signs
Remain calm
Stay with the pt
Don’t make assumptions about what the person needs
Speak to the person in short simple sentences using a soothing voice
“I am here for you”
“I won’t leave”
“It won’t last long”
“You are safe”
Avoid repeating saying things like “don’t worry”
Don’t repeatedly ask if they are alright
Be predictable
Help slow the person’s breathing by breathing w/ them or by counting slowly to 10
Hand over belly
Slow deep breathing
Remind them to keep breathing
Do not touch them unless invited to do do
Grounding:
Ice cube
Frozen orange
Feet on ground
Anxiolytics and antidepressants used to treat panic
Anxiolytics
Benzos
“pams”
Non-benzos

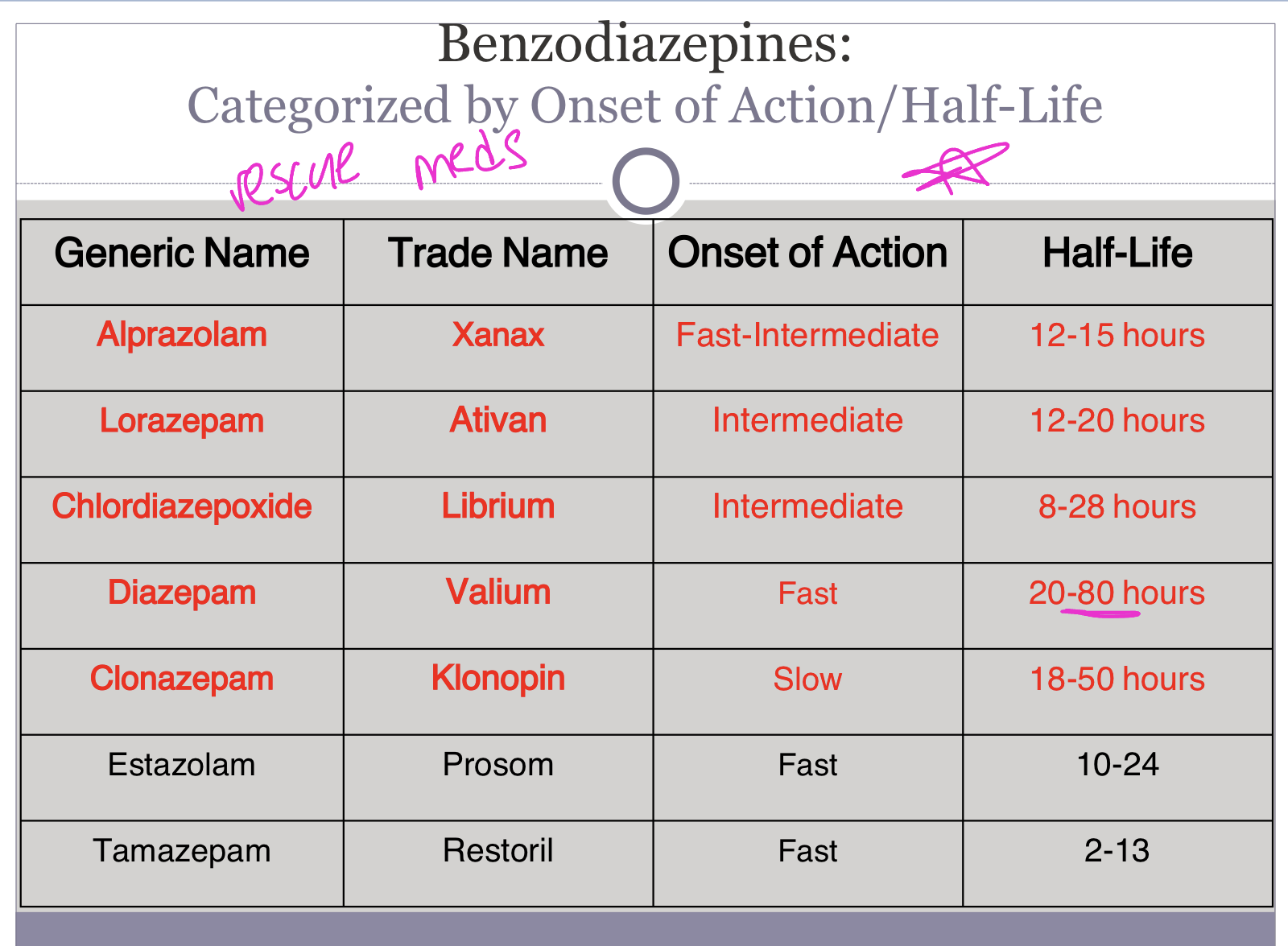
Benzodiazepines
E.g → Librium, Valium, Klonopin and Xanax
Benzodiazepines were previously one of the most commonly used pharmacological agents for anxiety, but due to tolerance, high levels of abuse, and recent connections to dementia, they are losing favor among providers. They are now being recommended for only short-term use and should be avoided with opioid medications. Benzodiazepines promote the activity of GABA by binding to a specific receptor on the GABAA receptor complex. Fig. 4.11 shows that benzodiazepines such as diazepam (Valium), clonazepam (Klonopin), and alprazolam (Xanax) bind to GABAA receptors with different α-subunits.
“pams”
MOA: Increasing the efficacy of GABA to decrease the excitability of neurons. Blocking the release of the stress hormone cortisol associated w/ panic and anxiety
This process reduces the communication between neurons, therefore has a calming effect on many of the functions of the brain especially the limbic system
Side effects: (depresses CNS)
Drowsiness/sedation
Confusion
Ataxia
Dizziness
Respiratory depression
Increased irritability
Tolerance, dependency
Re-bound insomnia/anxiety
Nursing implication:
Significant risk of dependence → ordered for short periods of time
Dangerous in overdose → especially w/ alcohol
Severe withdrawal symptoms if stopped abruptly → withdrawal slowly
Cautions + warnings →
Don’t operate heavy machinery or drive motor vehicle
Dangerous when taken w/ alcohol→ intensifies depressive effects
Glaucoma, dont use w/ pts w/ glaucoma unless recieving appropriate anti-glaucoma therapy
Don’t use pregnant or breastfeeding
Elderly/children → more prone to s/e and paradoxical effects (1/2 to 1/3 dose)
Half-Life
Understanding the half-lives of these benzodiazepines is clinically critical for several nursing considerations:
1. Withdrawal Risk Management
Abrupt withdrawal after prolonged benzodiazepine use causes serious complications including:
Autonomic withdrawal symptoms
Seizures
Delirium
Rebound anxiety
Myoclonus (involuntary muscle contractions)
Sleep disturbances
Longer half-life drugs (Valium, Librium) taper more gradually in the body, potentially causing less severe withdrawal. Shorter half-life drugs (Xanax) leave the system quickly, causing more abrupt and potentially dangerous withdrawal.
2. Overdose and Reversal
When benzodiazepines are combined with alcohol or other CNS depressants, outcomes can be lethal due to respiratory arrest.
Flumazenil (benzodiazepine antagonist) reverses benzodiazepine effects, but:
May cause acute withdrawal syndrome, including seizures in patients on long-term therapy
Effectiveness and monitoring duration depend on the benzodiazepine's half-life
A longer-acting drug may require extended monitoring even after flumazenil administration.
3. Dosing Schedules
Half-life determines:
Frequency of administration (shorter half-life = more frequent dosing)
Accumulation risk in the body
Duration of therapeutic effect
4. Special Populations
Older adults have:
Increased sensitivity to benzodiazepines
Decreased metabolism (Beers Criteria warns against use)
Higher risk of delirium, falls, and hangover effects
Longer half-lives compound these risks through drug accumulation.
5. Tapering Protocols
Safe discontinuation requires gradual dose reduction—decreasing by 50% every 2 nights until reaching minimal doses. Knowing half-lives helps determine appropriate tapering schedules.
6. Substance Use Disorder Treatment
Benzodiazepines with cross-tolerance are used in alcohol withdrawal management. Longer-acting benzodiazepines provide smoother symptom control during detoxification.
Clinical Bottom Line: Half-life knowledge prevents withdrawal complications, guides safe tapering, informs overdose management, and protects vulnerable populations.
Benzodiazepines Withdrawal Syndrome
Potentially life threatening
Why are benzodiazepines addictive?
Non-bensodiazepines
Anxiety meds
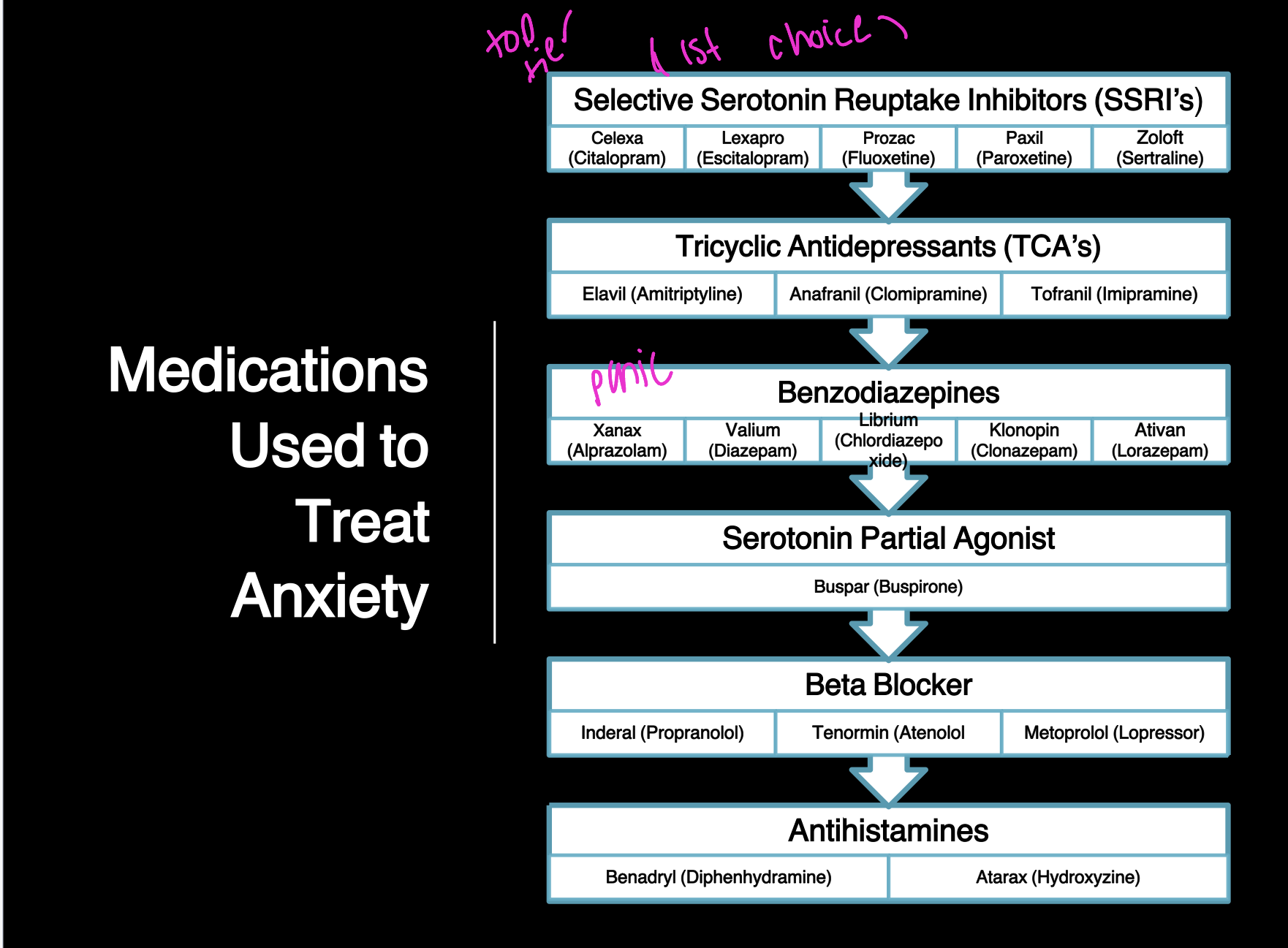
Antidepressants have been found effective in treating anxiety disorders because of many shared symptoms, neurotransmitters, and circuits. SSRIs are commonly used to treat panic disorder, generalized anxiety disorder (GAD), OCD, PTSD, and social phobia. The SNRIs venlafaxine (Effexor) and duloxetine (Cymbalta) are also used to treat GAD.
First-Line: Antidepressants
SSRIs (Selective Serotonin Reuptake Inhibitors) are prescribed with success for panic disorder and are the most widely prescribed for long-term treatment:
Fluoxetine (Prozac)
Sertraline (Zoloft)
Paroxetine (Paxil)
Other SSRIs
SNRIs (Serotonin-Norepinephrine Reuptake Inhibitors) are also effective for anxiety disorders including panic.
Important Considerations for Antidepressants:
Start with low doses due to activating effects that can temporarily increase anxiety
Treat cooccurring depression
Must be tapered slowly when stopping to prevent discontinuation syndrome
Can increase suicide risk (monitor closely)
In patients with bipolar disorder, may precipitate manic episodes
Short-Term: Benzodiazepines
Anxiolytics provide immediate relief but are indicated for short-term treatment only:
Alprazolam (Xanax)
Diazepam (Valium)
Lorazepam (Ativan)
Clonazepam (Klonopin)
Why Short-Term Only?
Tolerance develops over time (requiring higher doses)
Addiction risk, especially with substance use history
Withdrawal symptoms if stopped suddenly
Associated with memory/cognitive concerns and dementia
Increased fall risk and mortality
Not helpful for long-term anxiety treatment
Paradoxical agitation possible (5% of cases, especially children/elderly)
Contraindicated in pregnancy and breastfeeding
Dangerous Interactions:
When combined with alcohol, opiates, or other CNS depressants, benzodiazepines can cause life-threatening respiratory depression.
Combined Approach
Psychotherapy and pharmacotherapy are frequently used together for optimal outcomes. Psychotherapy (trauma-focused CBT, exposure therapy) is typically the first-line intervention, with medications added when needed.