OMM Fall Cumulative
1/67
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
68 Terms
Cervical CS AC 1 TP
Ra
pt is supine
lateral aspect of C1 transverse process b/w ramus of mandible and mastoid process
rectus capitis lateralis muscle
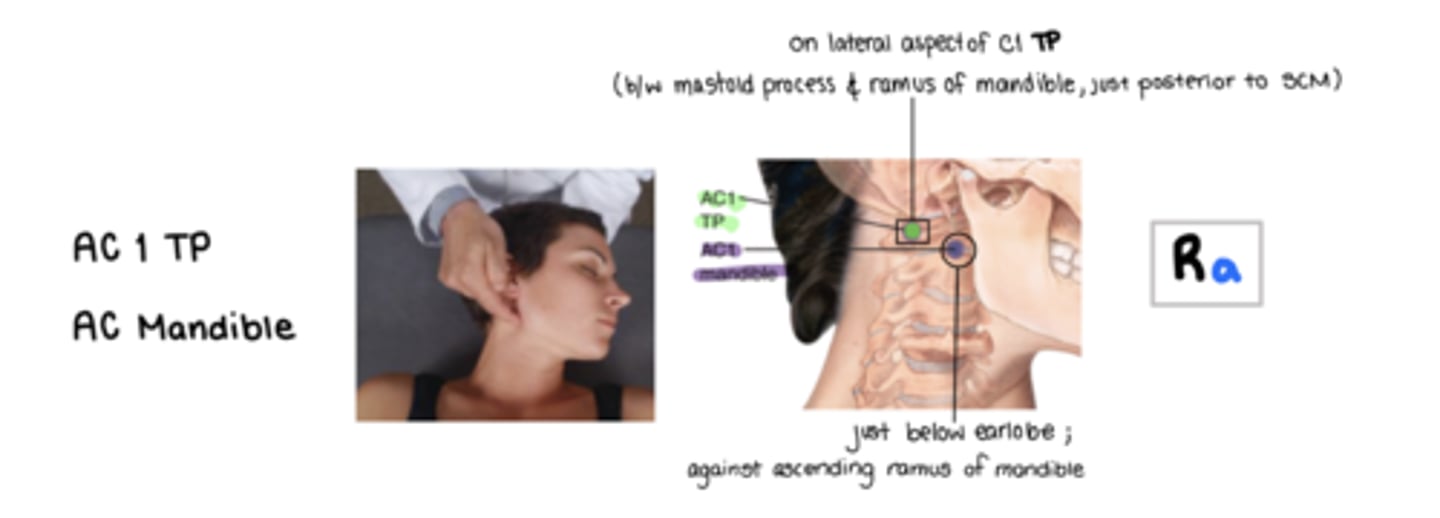
Cervical CS AC1 Mandible
Ra
pt is supine
on the posterior surface of the ascending ramus of the mandible at or just below earlobe
rectus capitis anterior muscle
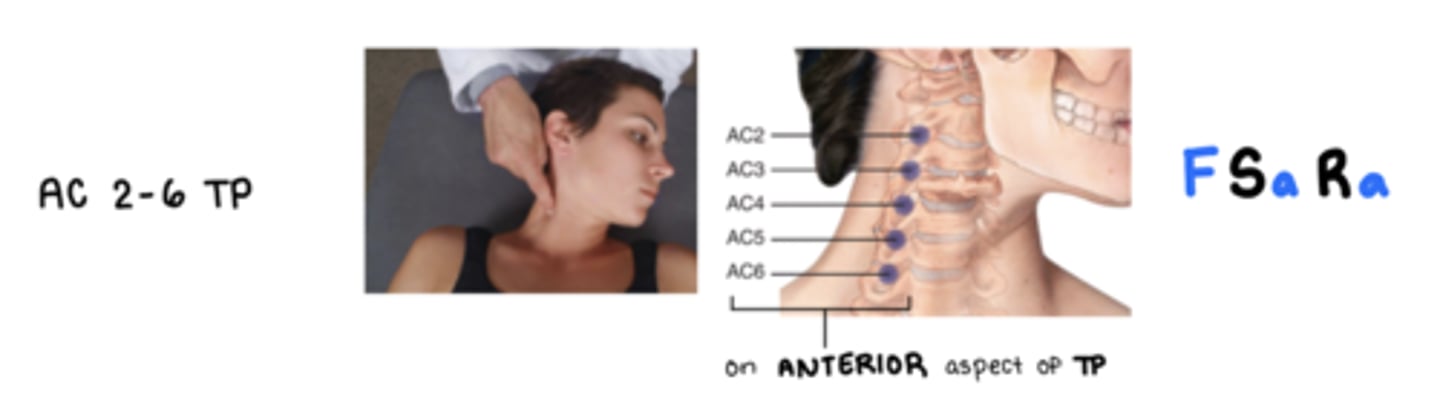
Cervical CS AC 2-6 TP
F Sa Ra
on anterior lateral aspect of the A/P tubercles of the transverse process of the corresponding vertebrae
2- middle scalene and longus colli mm.
3/4- anterior, middle scalenes, longus capitis and longus colli mm.
5/6- anterior, middle, posterior scalenes, longus capitis and longus collii mm.
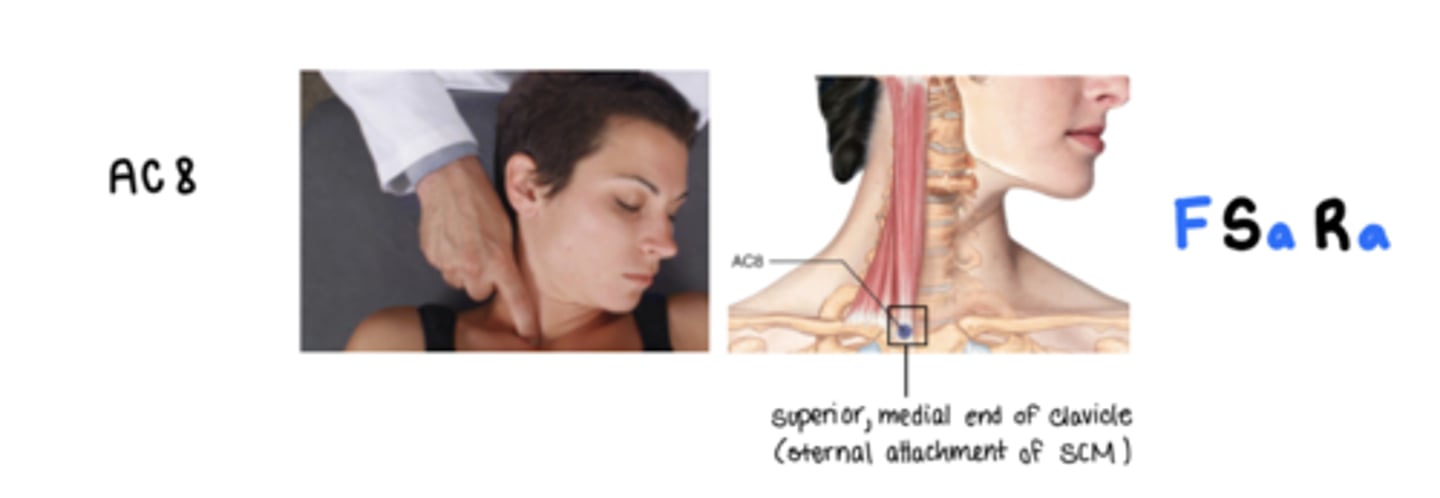
Cervical CS AC8
F Sa Ra
on the superior medial end of the clavicle at the sternal attachment of the SCM
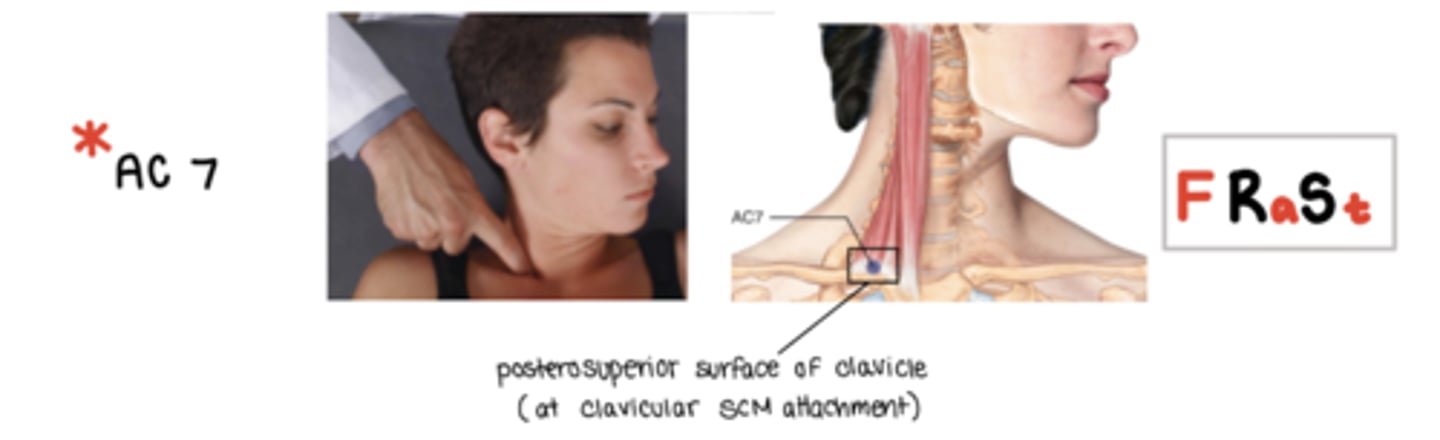
Cervical CS AC7
F Ra St
lucky number 7
on the posterosuperior surface of the clavice at the clavicular attachment of the SCM
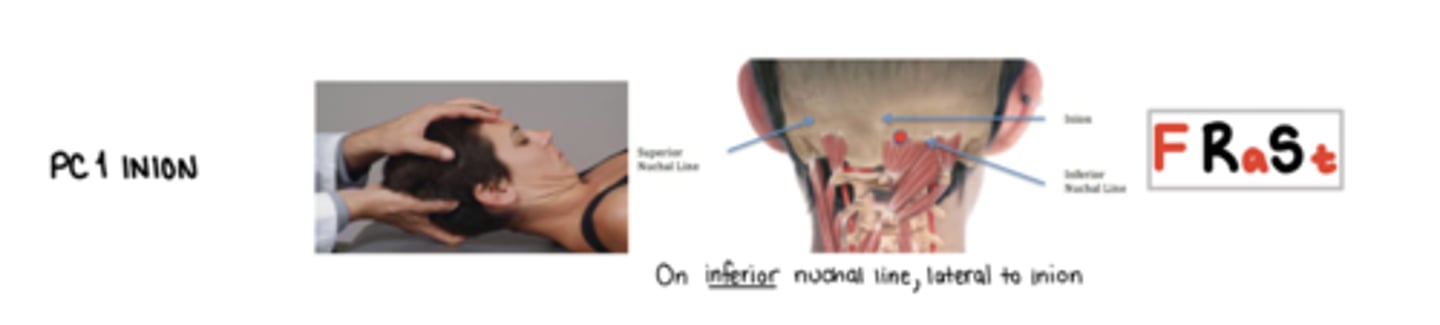
Cervical CS PC1 Inion
F Ra St
on the inferior nuchal line, lateral to the inion
Cervical CS PC1 Occiput
E Sa Ra
on inferior nuchal line midway b/w inion and mastoid
splenius capitis, rectus capitis posterior major/minor, oblique capitis superior mm.

Cervical CS PC 2 Occiput
E Sa Ra
inferior nuchal line w/n the semispinalis capitis m
associated with greater occipital nerve

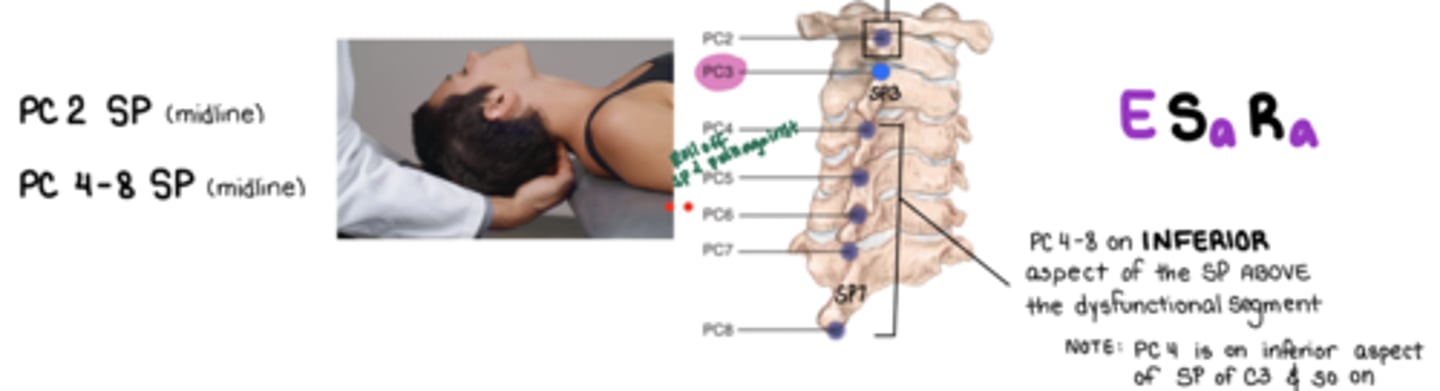
Cervical CS PC2 SP
E Sa Ra
**SUPERIOR aspect of SP C2
rectus capitis posterior minor/major and olbiquus capitis inferior
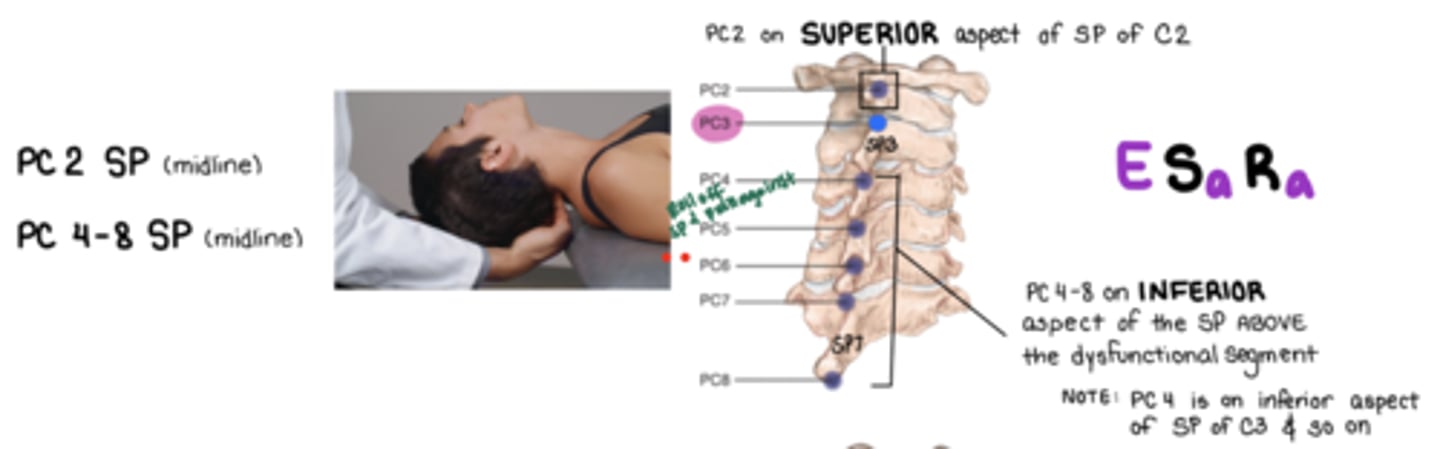
Cervical CS PC4-8 SP
E Sa Ra
3- middle scalenes, longus capitis, longus colli
4-8 semispinalis capitis, multifidis, rotatores
Cervical CS PC 3 SP
F Sa Ra

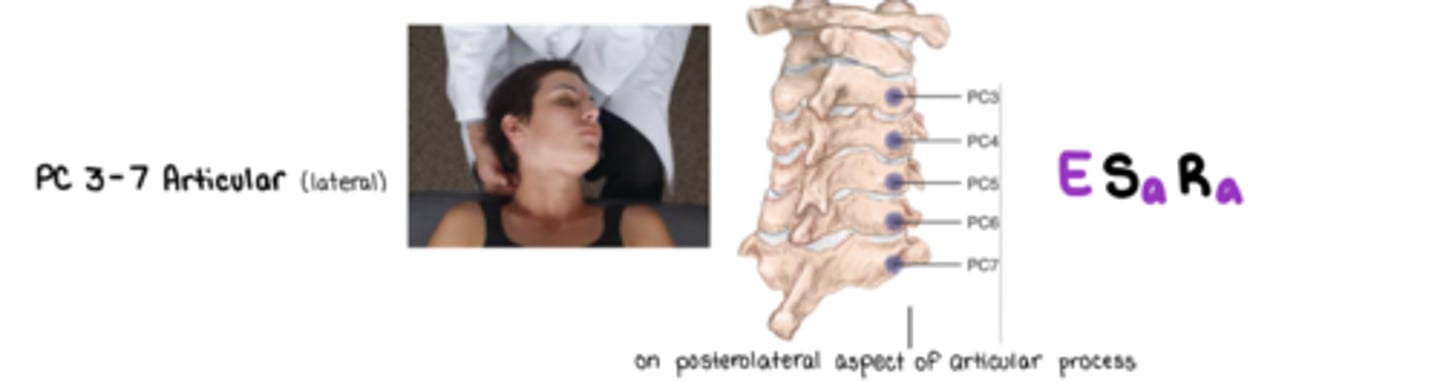
Cervical CS PC 3-7 Articular
E Sa Ra
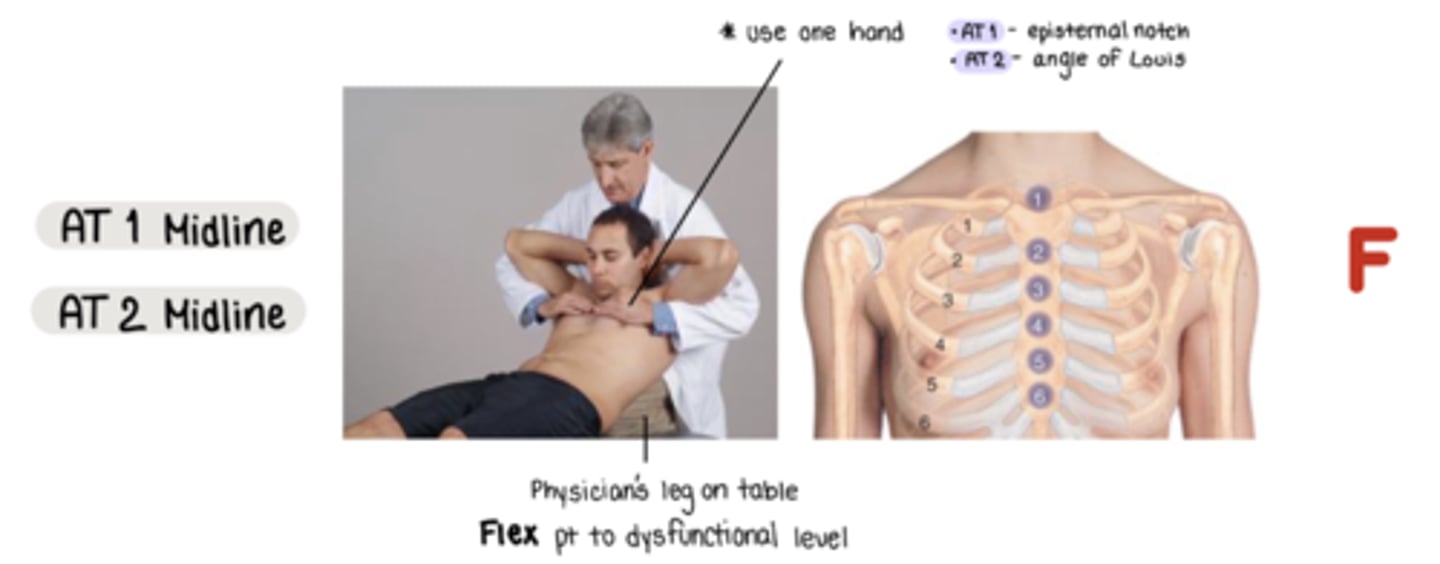
Thoracic CS AT 1 Midline
F
located @ episternal notch
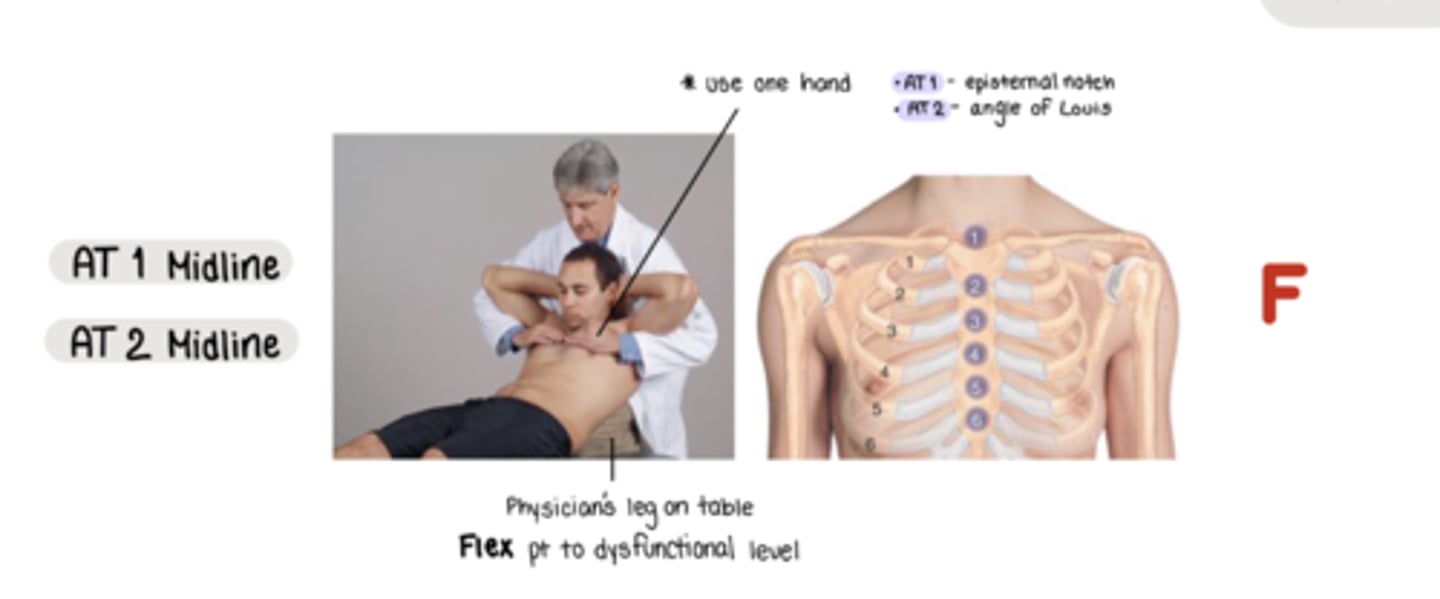
Thoracis CS AT 2 Midline
located @ sternal angle
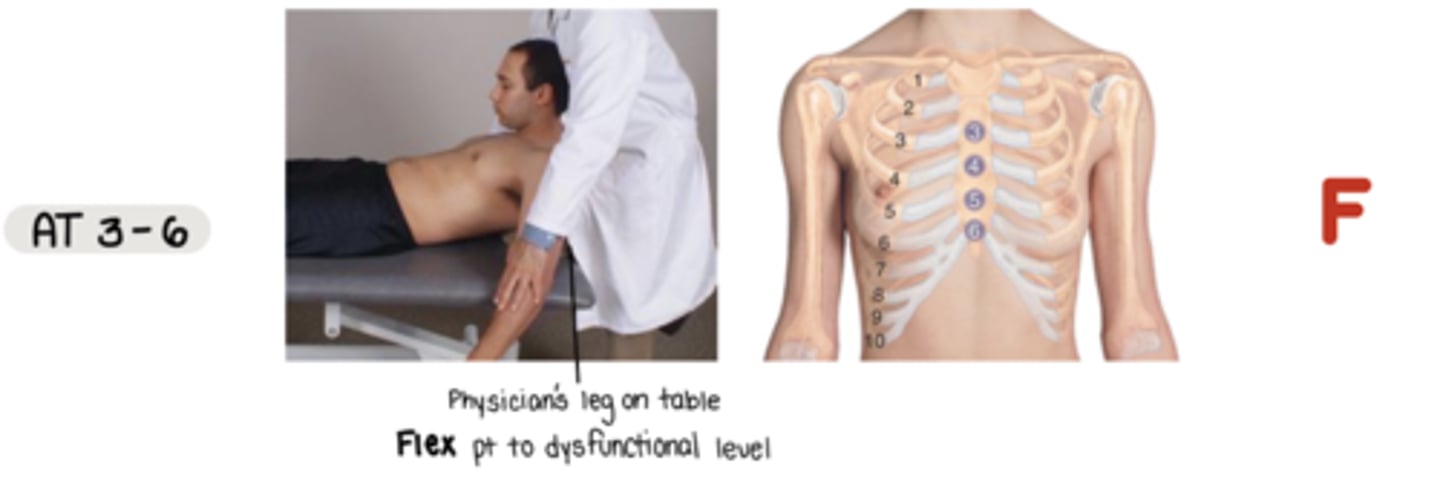
Thoracic CS AT 3-6
F to dysfunctional level
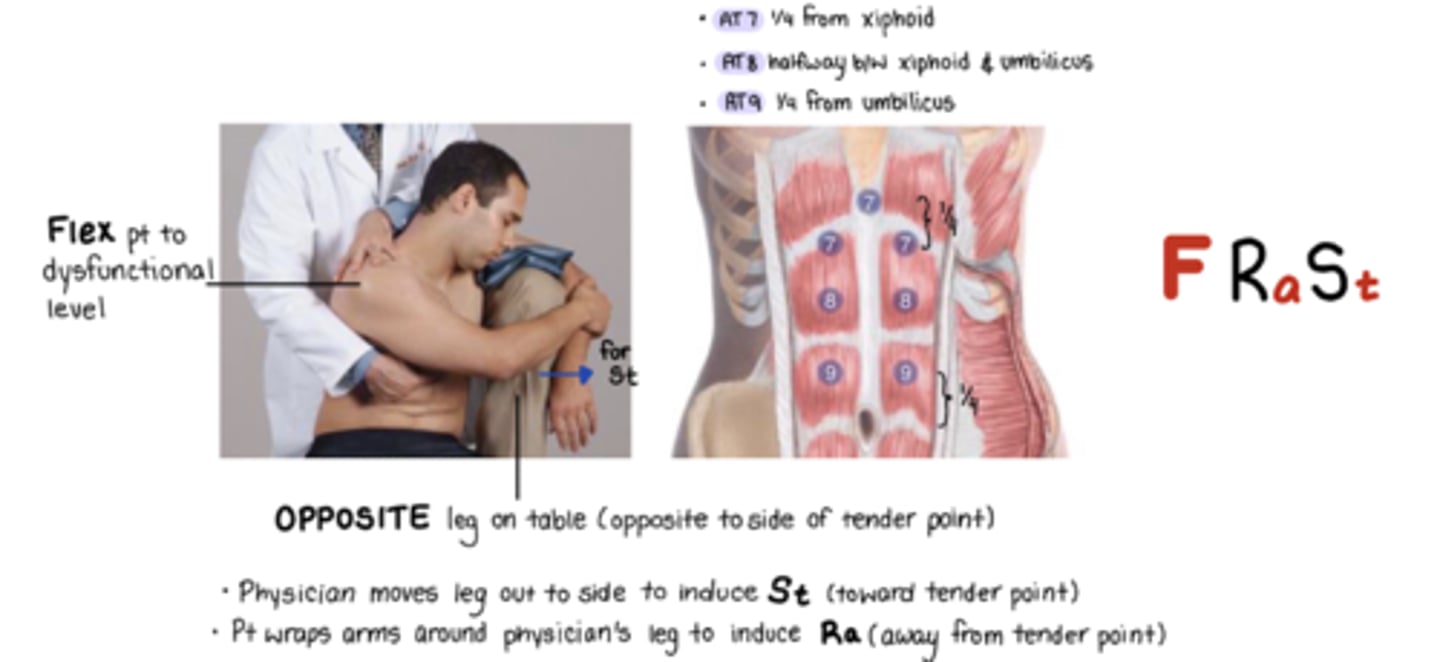
Thoracic CS AT 7
F Ra St
1/4 from xiphoid process
St = move leg out to induce pt side bending toward TP
Ra = pt wraps arm around physicians leg to induce Ra from TP
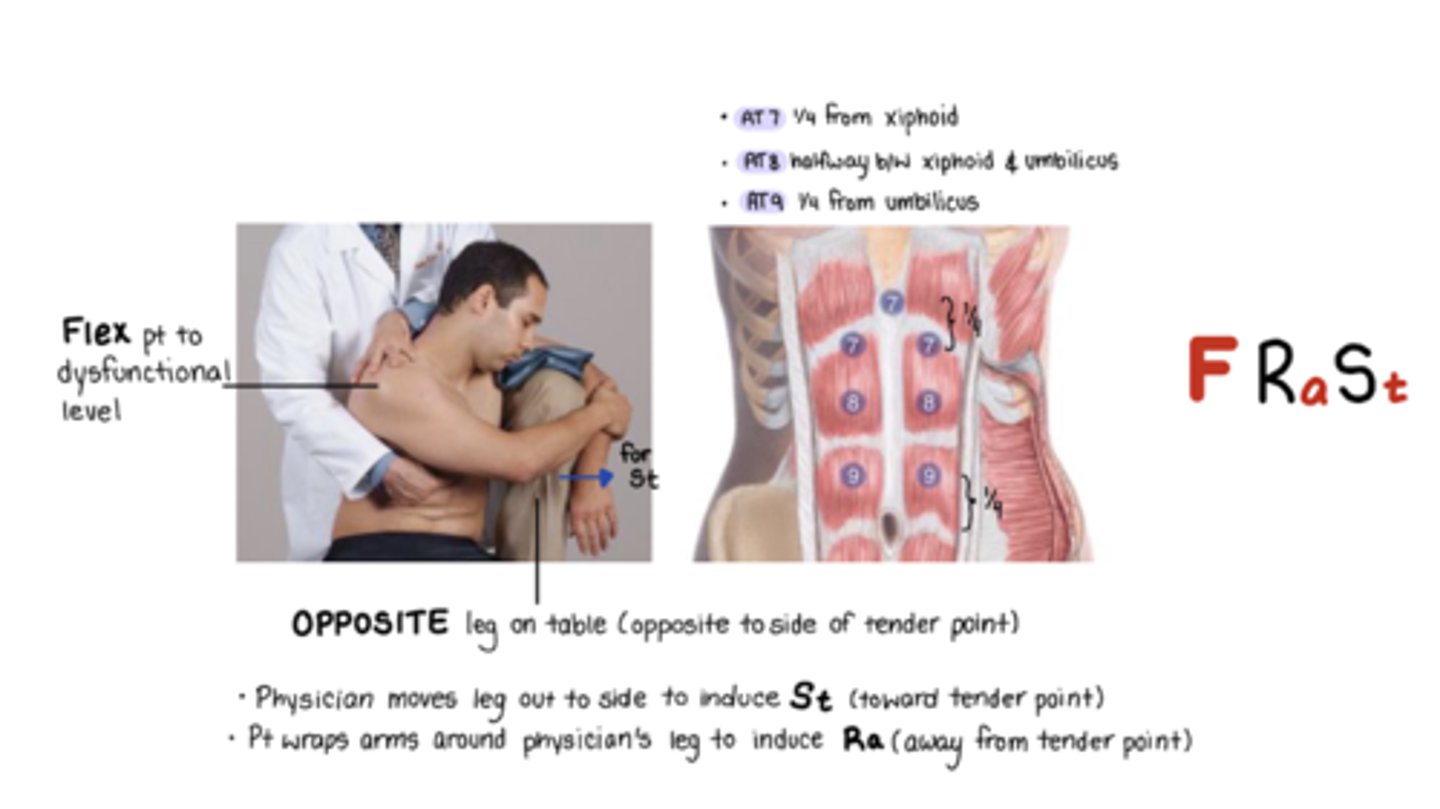
Thoracic CS AT 8
F Ra St
halfway xiphoid and umbilicus
St = move leg out to induce pt side bending toward TP
Ra = pt wraps arm around physicians leg to induce Ra from TP
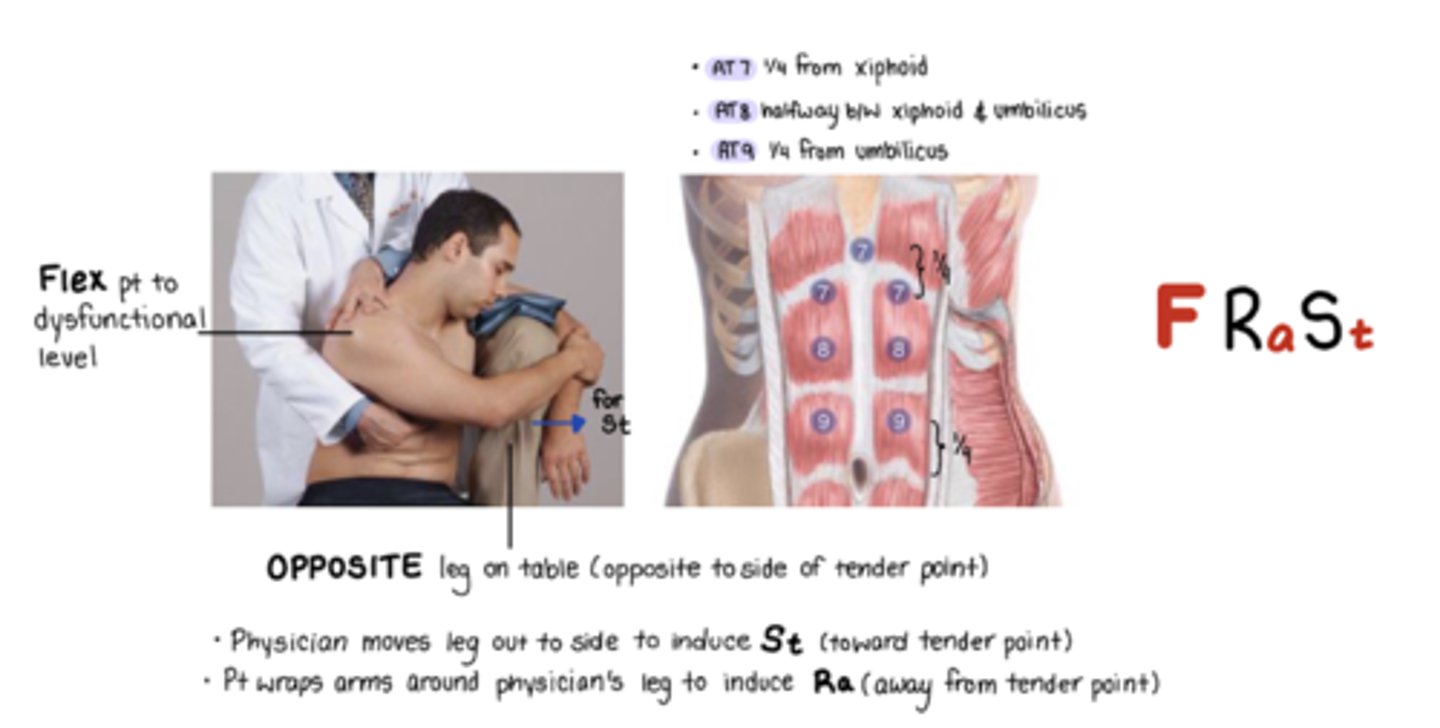
Thoracic CS AT 9
F Ra St
1/4 from from umbillicus
St = move leg out to induce pt side bending toward TP
Ra = pt wraps arm around physicians leg to induce Ra from TP
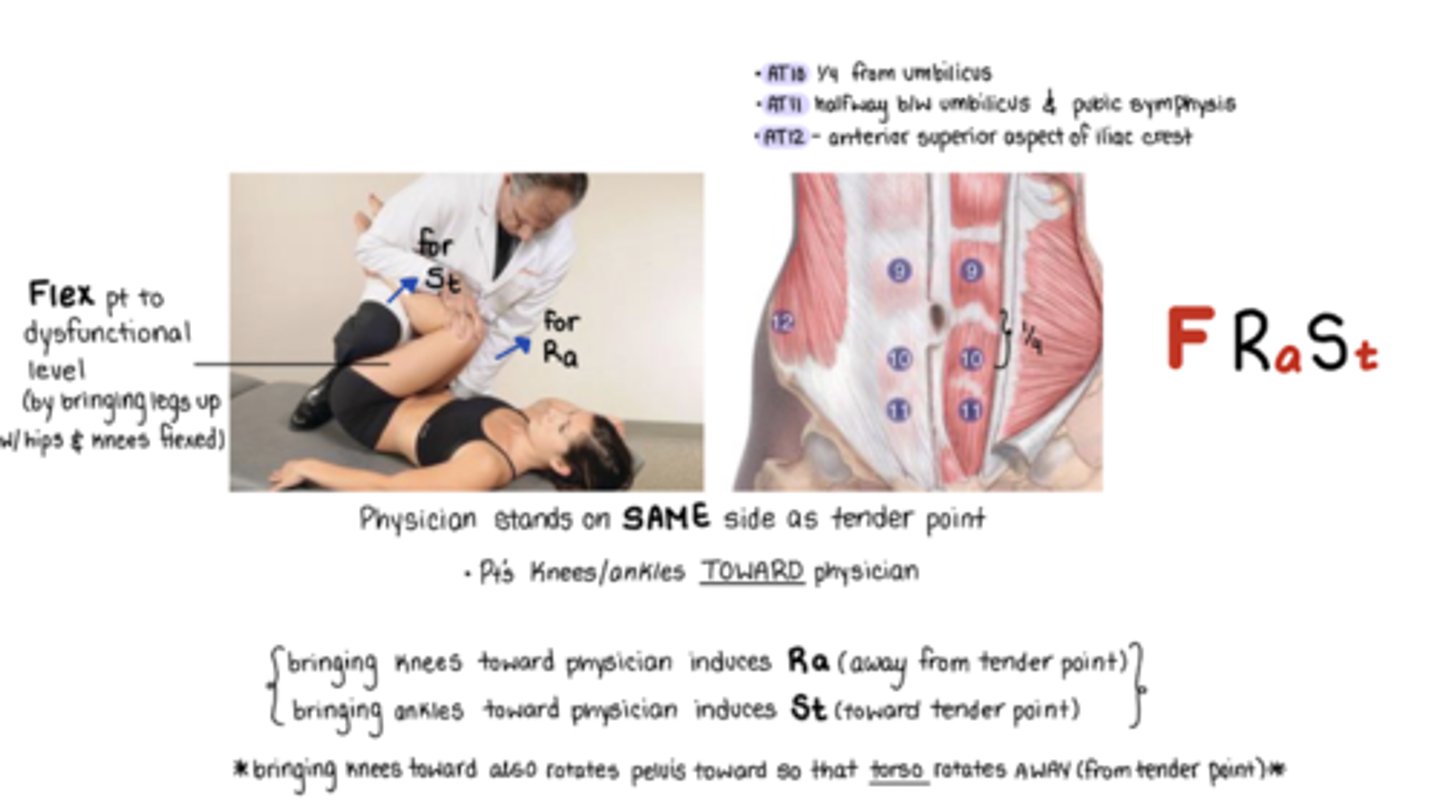
Thoracic CS AT 10
F Ra St
TP @ 1/4 from umbilicus to pubic symphysis
Physician on SAME side as TP
Pt crosses legs
Knees and ankles to me
Ra = bring knees toward physician
rotates pelvis toward so that torso rotates AWAY from TP
St = bring ankles toward physician
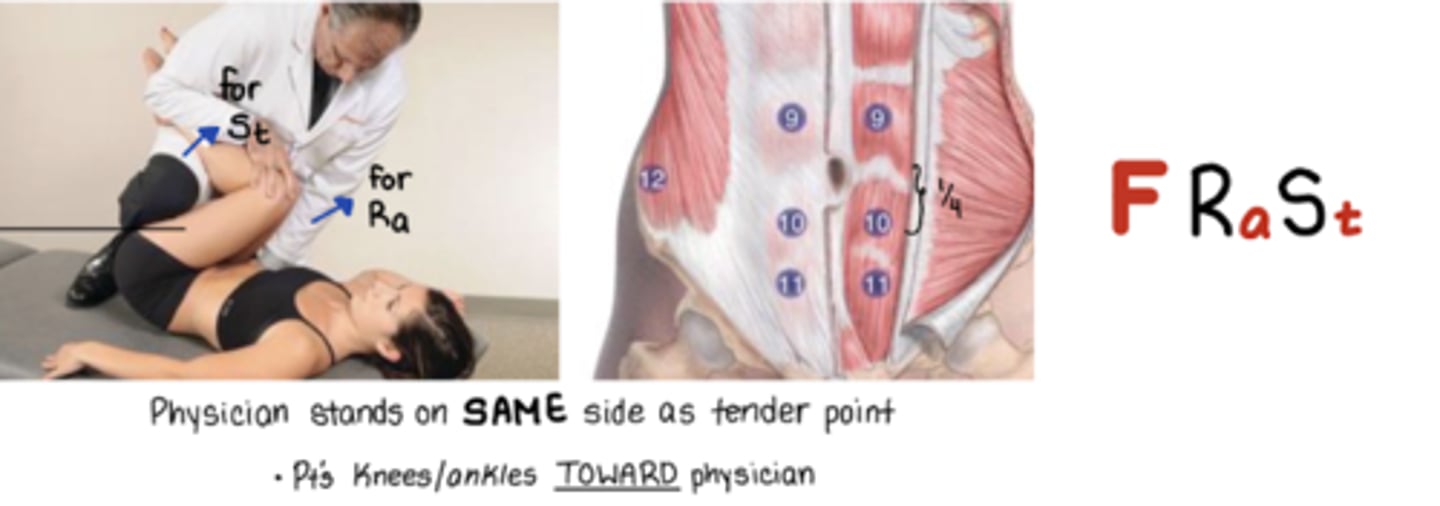
Thoracic CS AT 11
F Ra St
halfway b/w umbilicus and pubic symphysis
Physician on SAME side as TP
knees and ankles toward me
Ra = bring knees toward physician
rotates pelvis toward so that torso rotates AWAY from TP
St = bring ankles toward physician
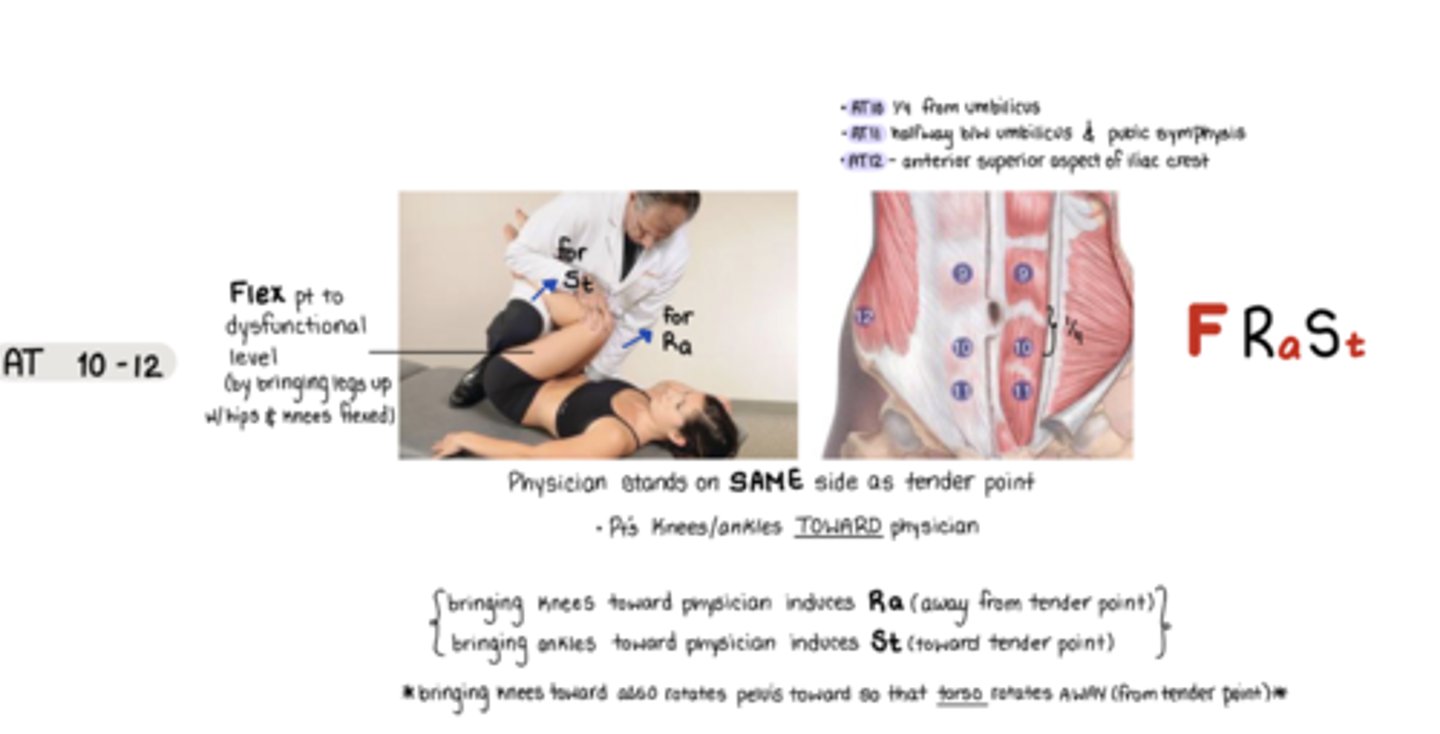
Thoracic CS AT 12
F Ra St
located @ anterior super aspect of iliac crest
Physician on SAME side as TP
knees and ankles to me
Ra = bring knees toward physician
rotates pelvis toward so that torso rotates AWAY from TP
St = bring ankles toward physician
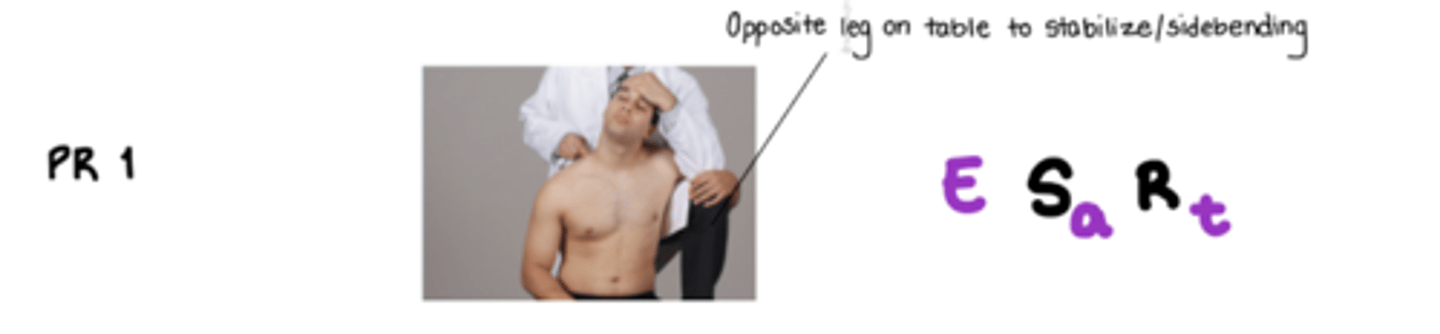
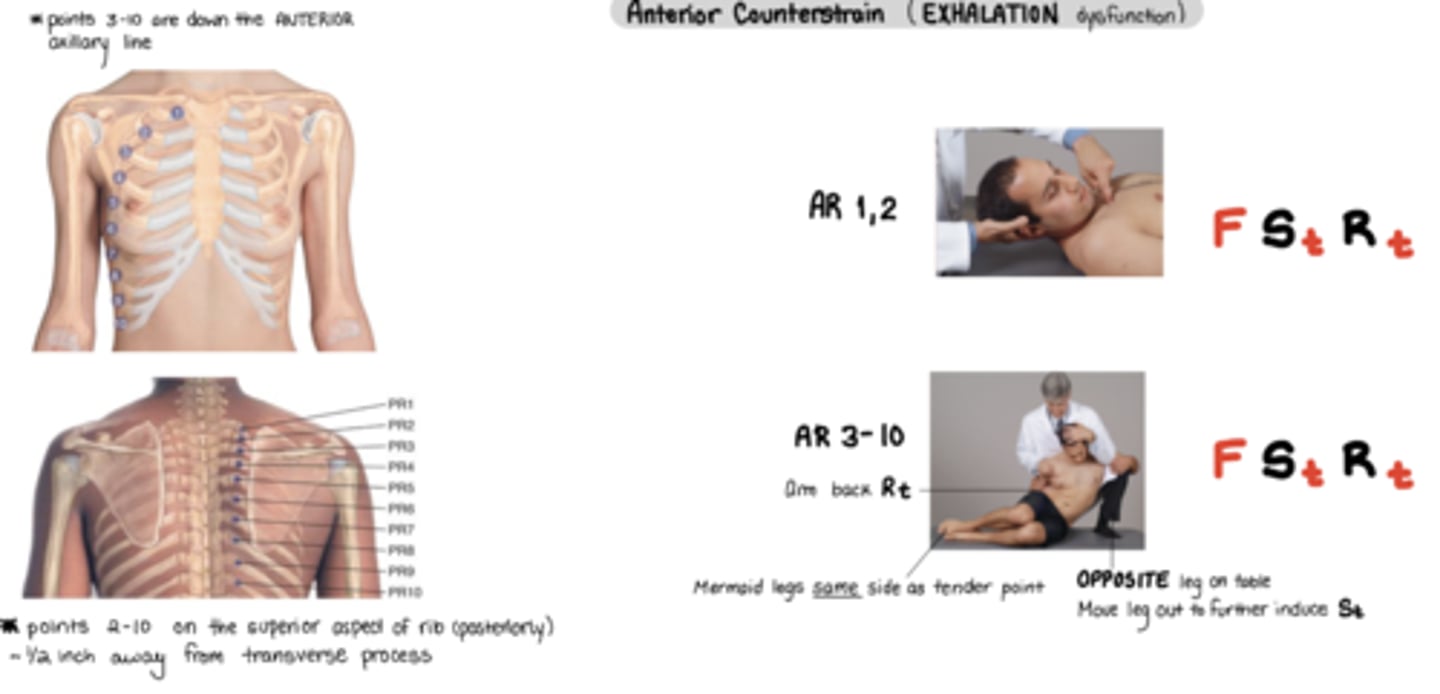
Rib CS PR 1
PIE is OP
posterior
I = 1
E = E Sa Rt
OP = use opposite leg for stabilizing
E Sa Rt
*inhalation
Rib CS PR 2-10
F Sa Ra
*inhalation

Rib CS AR 1,2
F St Rt
*exhalation
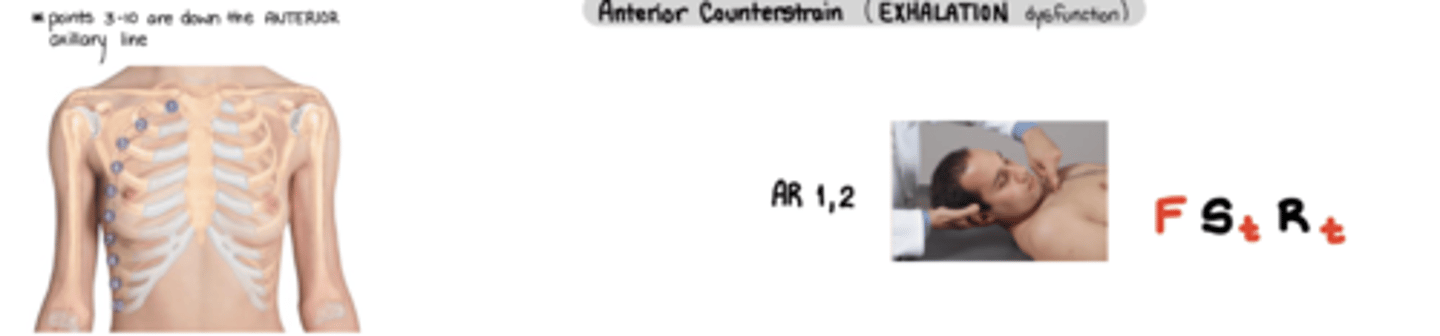
Rib CS AR 3-10
F St Rt
ASS! - anterior same side -> pt mermaid legs same side as TP
* exhalation
Arm back = Rt
Physician moves leg out = further into St
Lumbar CS AL1
F Ra St
TP = medial to ASIS
ankles and knees to me

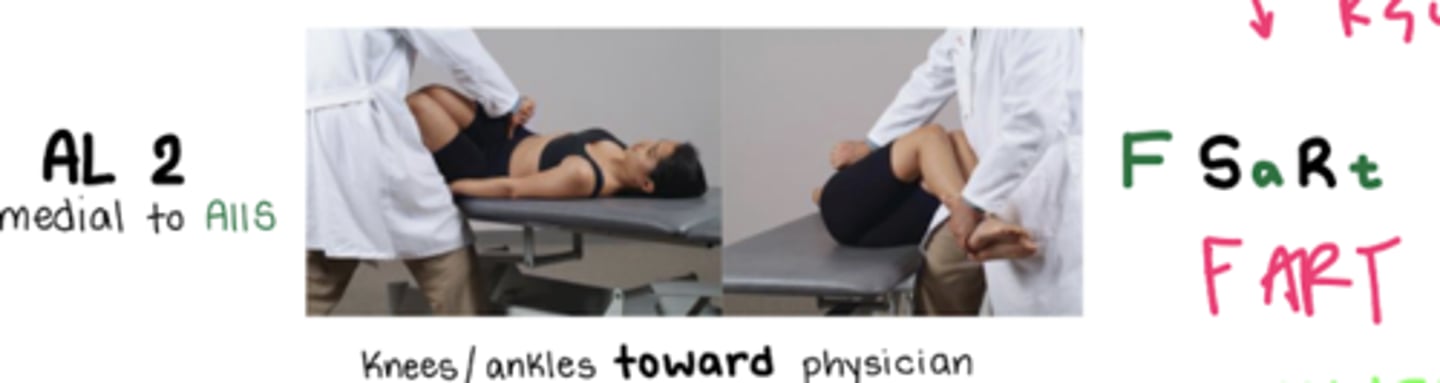
Lumbar CS AL 2
F Sa Rt
TP = medial to AIIS
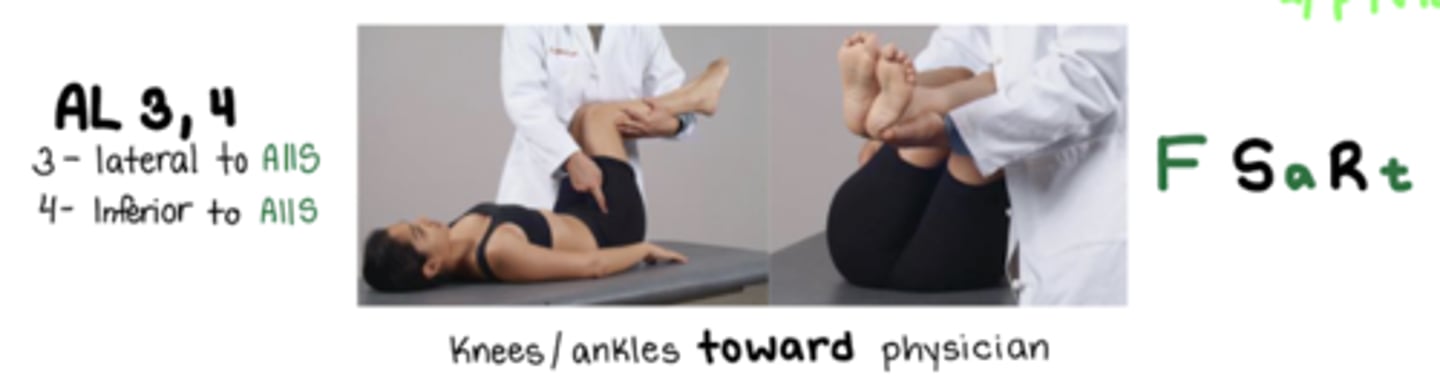
Lumbar CS AL 3
F Sa Rt
TP = lateral to AIIS
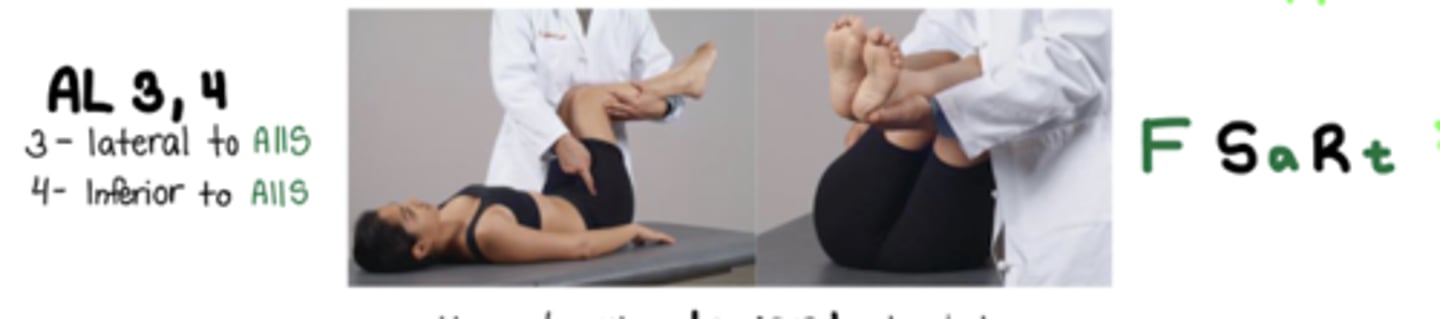
Lumbar CS AL 4
F Sa Rt
TP = inferior to AIIS
Lumbar CS AL 5
F Sa Ra
TP = lateral to pubic symphasis
ONLY lumbar anterior CS ankles are AWAY

AL 1 and 5 stand on
same side as TP
AL 2-4 stand on
opp side of TP
*across the floor
Lumbar CS PL 1-5 SP
E Sa Ra
EXTEND, ADDUCT, EXTERNALLY ROTATE
Stand OPPOSITE of TP
hold leg ABOVE knee
When standing on same side
Use your knee to lift leg closest to you to externally rotate, extend, and ADduct
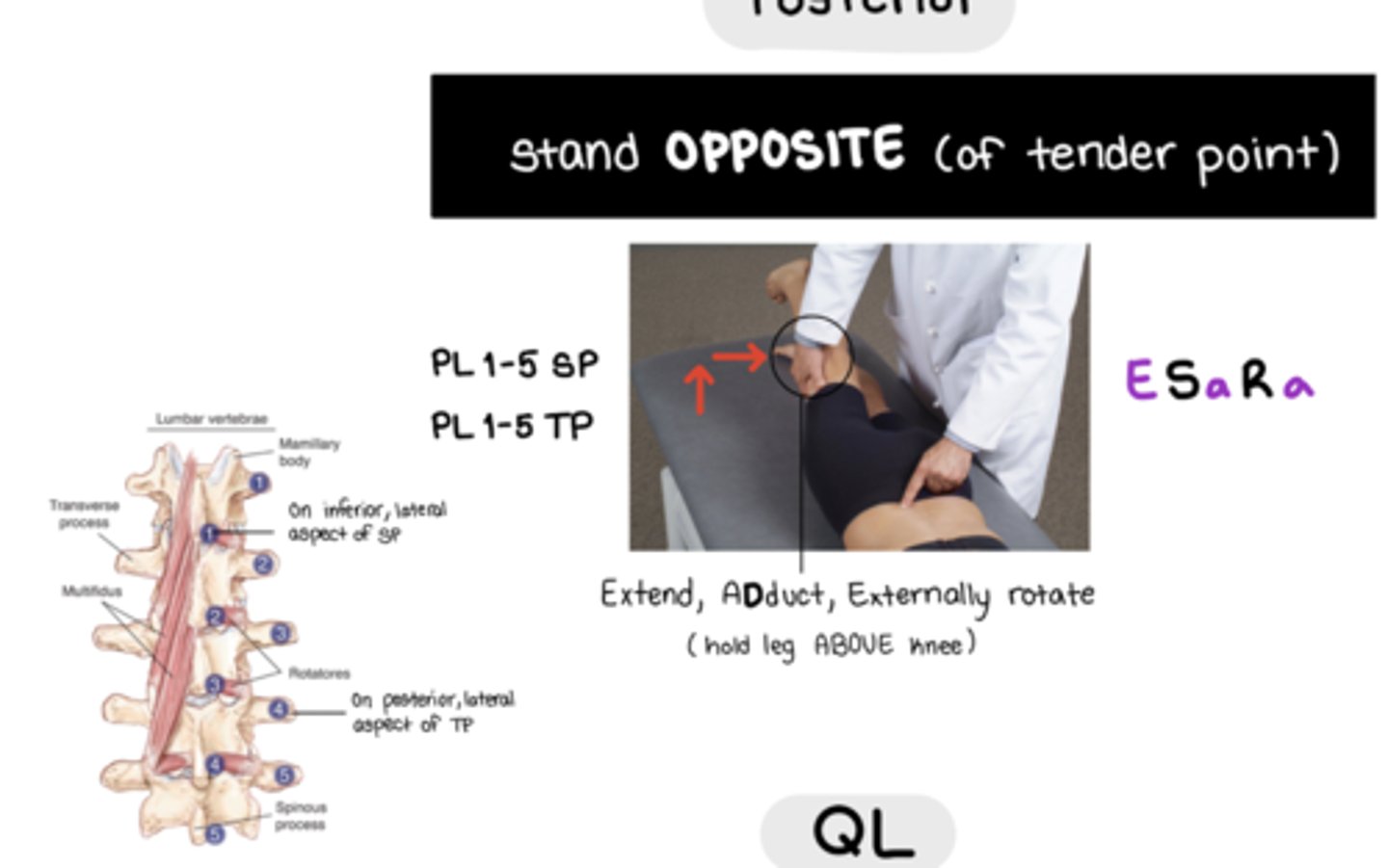
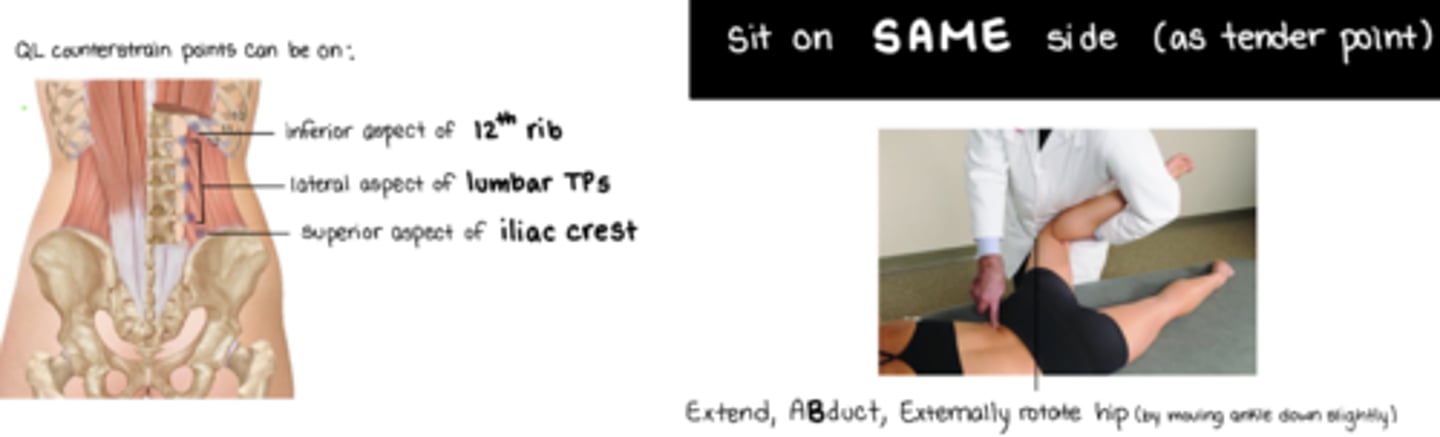
QL CS
EXTEND, ABDUCT, EXTERNALLY ROTATE HIP
Stand on SAME SIDE of TP
QL attachments: inferior aspect of 12th rib, lateral aspect of lumbar TPs, superior aspect of iliac crest
OA MET flexed SD
v-hold: pads of thumb and index finger just under occiput
pt is moved further into barrier E Sa Ra

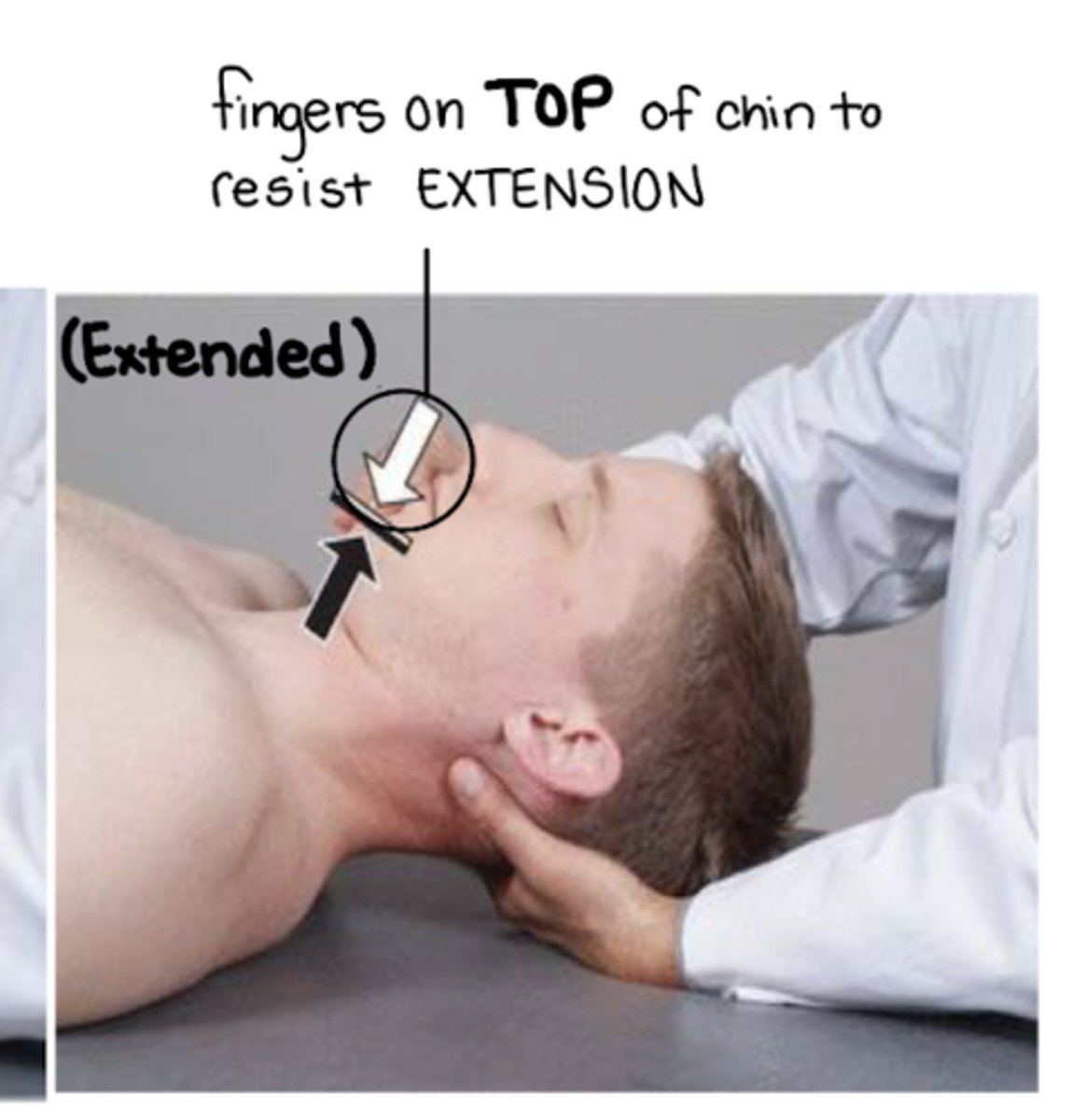
OA MET extension SD
v-hold: under occiput, pads of fingers contact the suboccipital musculature
pt is moved further into barrier F Sa Ra
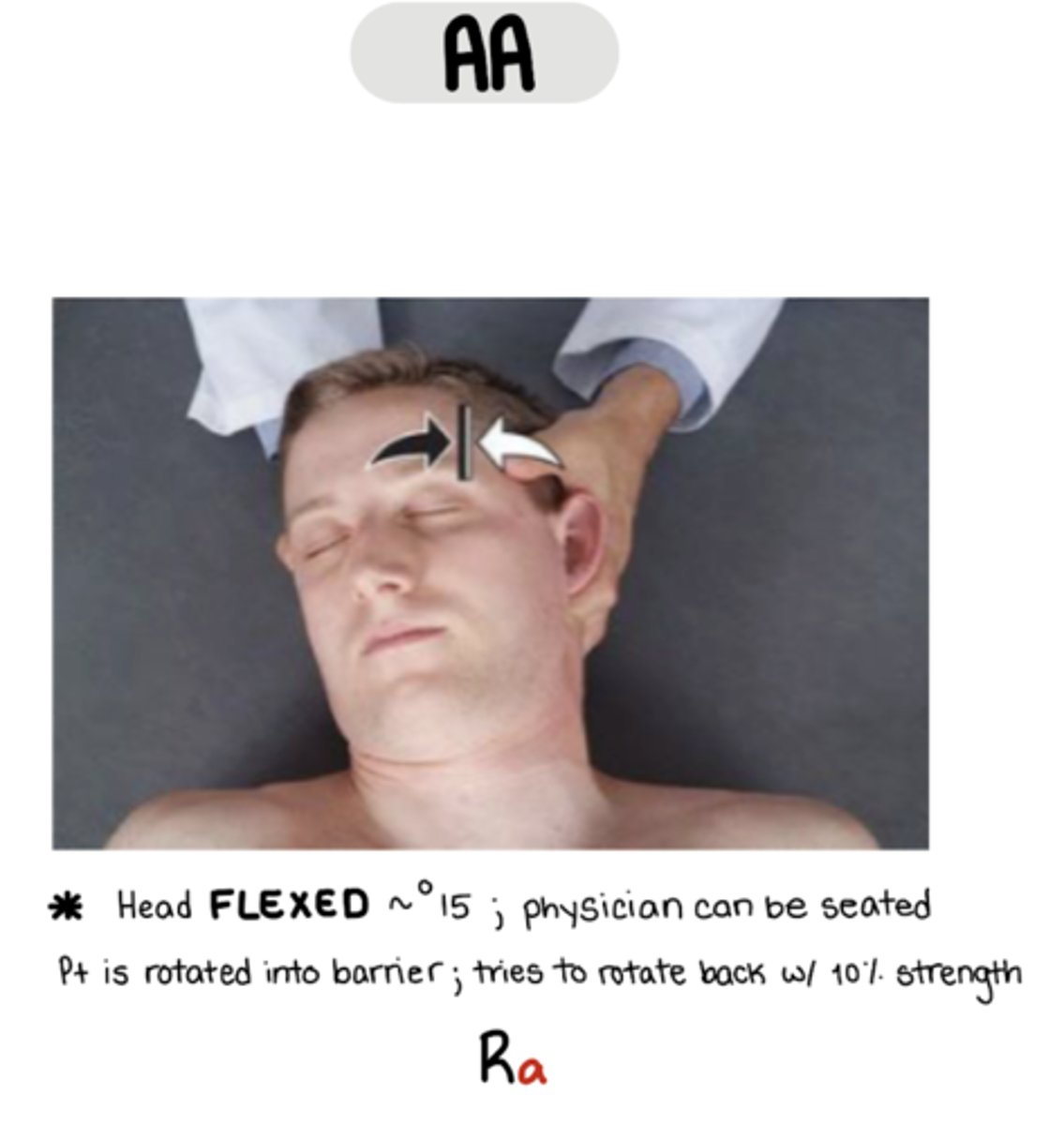
AA MET
Ra
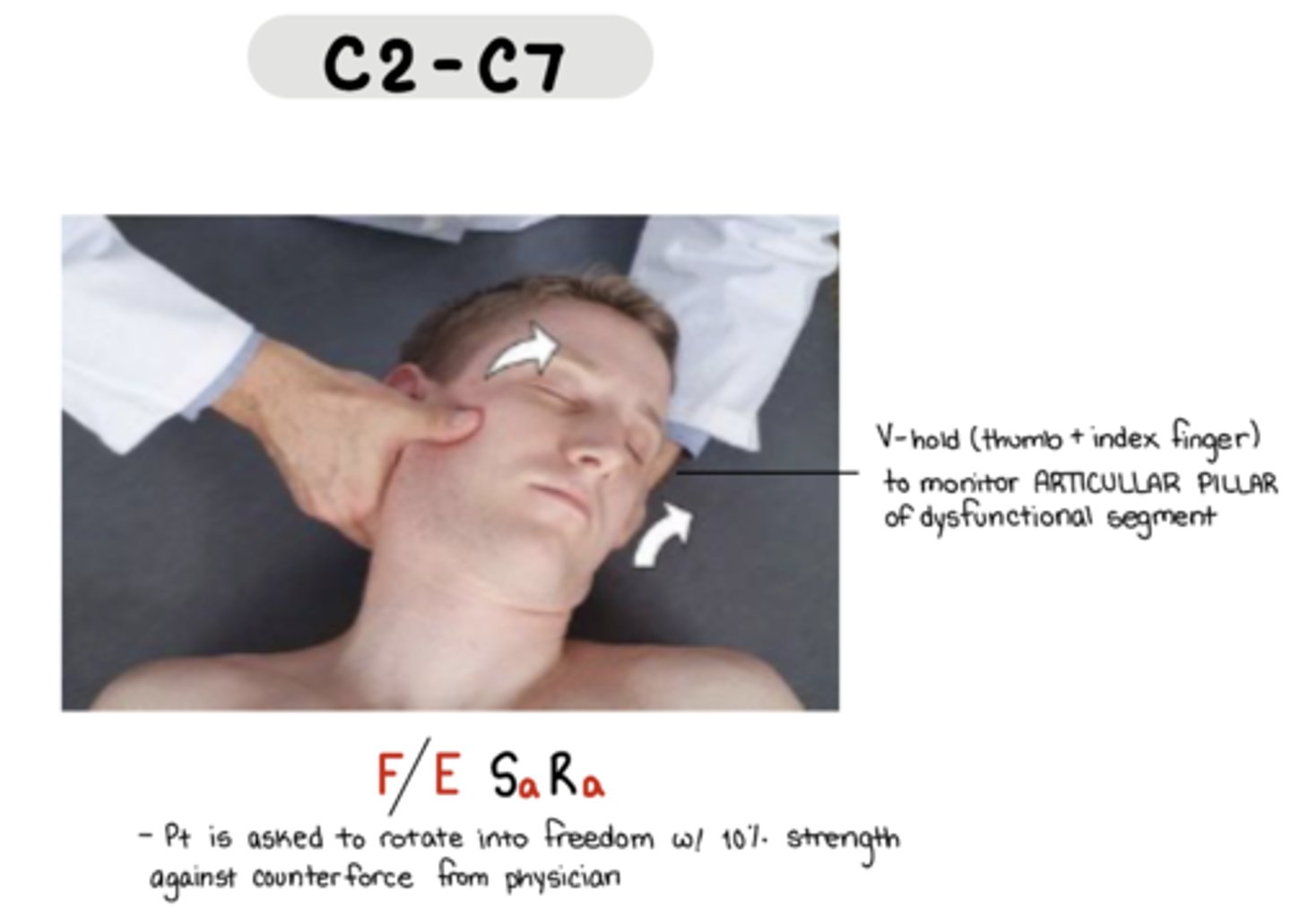
C2-C7 MET
F/E Sa Ra
V-hold: thumb and index fingers to monitor articular pillae
pt is asked to rotate into freedom with 10% strength against counterforce
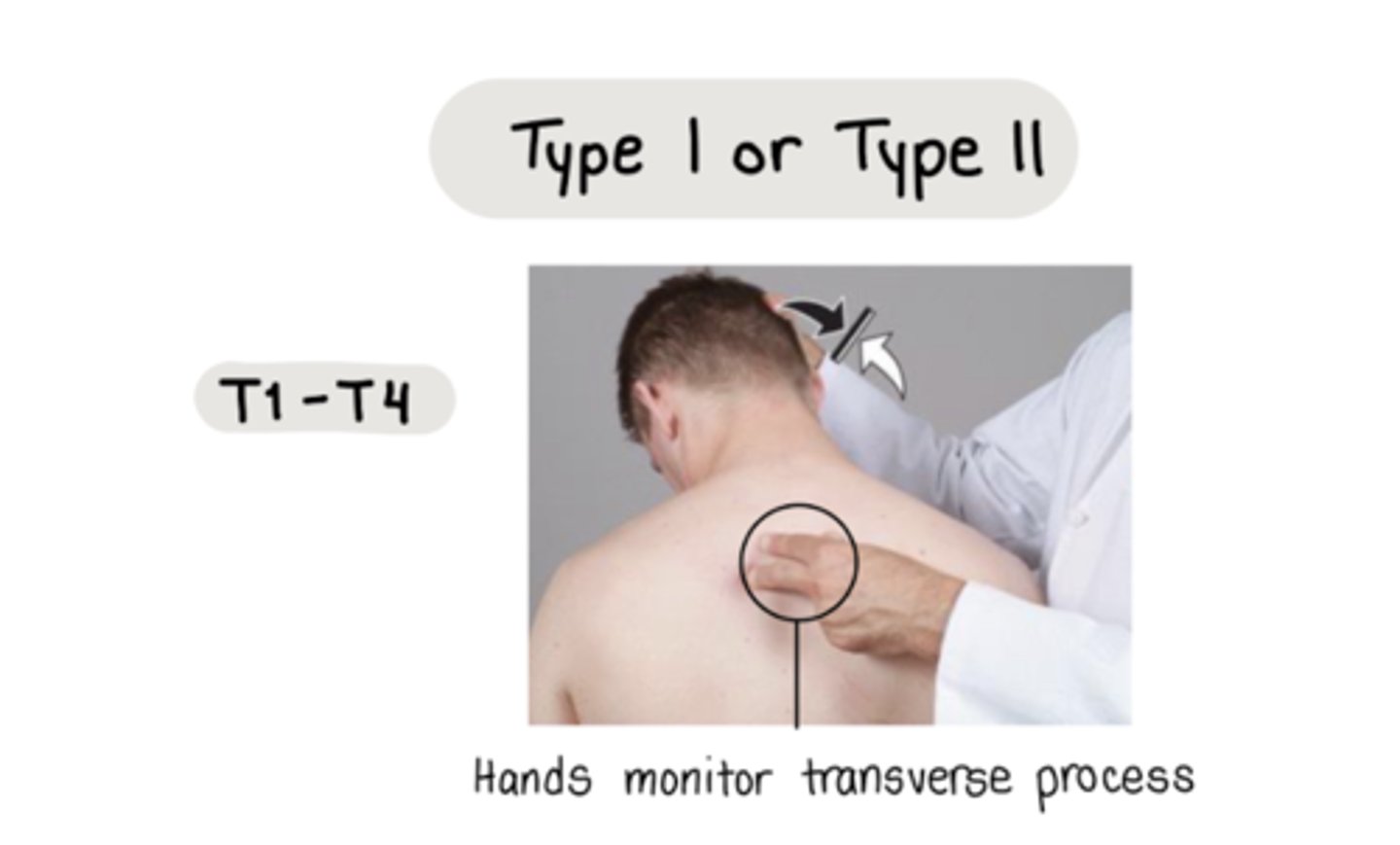
Thoracic MET Type 1 T1-T4
hands monitor transverse process
direct: moving pt INTO barrier in ALL PLANES
active: pt moves back toward direction of freedom in one plane
Thoracic MET Type 1 T5-T12
pt hand on neck on SAME side as rotational component
physician stand on OPPOSITE side of rotational component
hands monitor TP
direct: moving pt INTO barrier in ALL PLANES
active: pt moves back toward direction of freedom in one plane

Thoracic MET Type 2 T5-T12
osteopathic hug
physician stand on OPPOSITE side of rotational component
direct: moving pt INTO barrier in ALL PLANES (F/E R S)
active: pt moves back toward direction of freedom in one plane
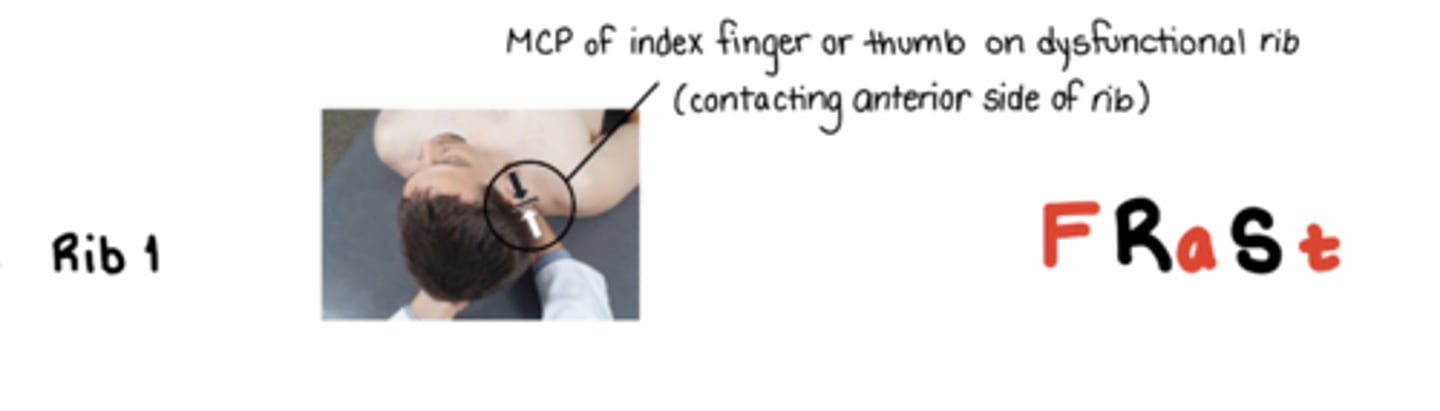
Rib 1 Inhalation MET
F Ra St
MCP of index finger or thumb on dysfunctional rib contacting anterior side of rib - resisting with INHALATION, following into EXHALATION
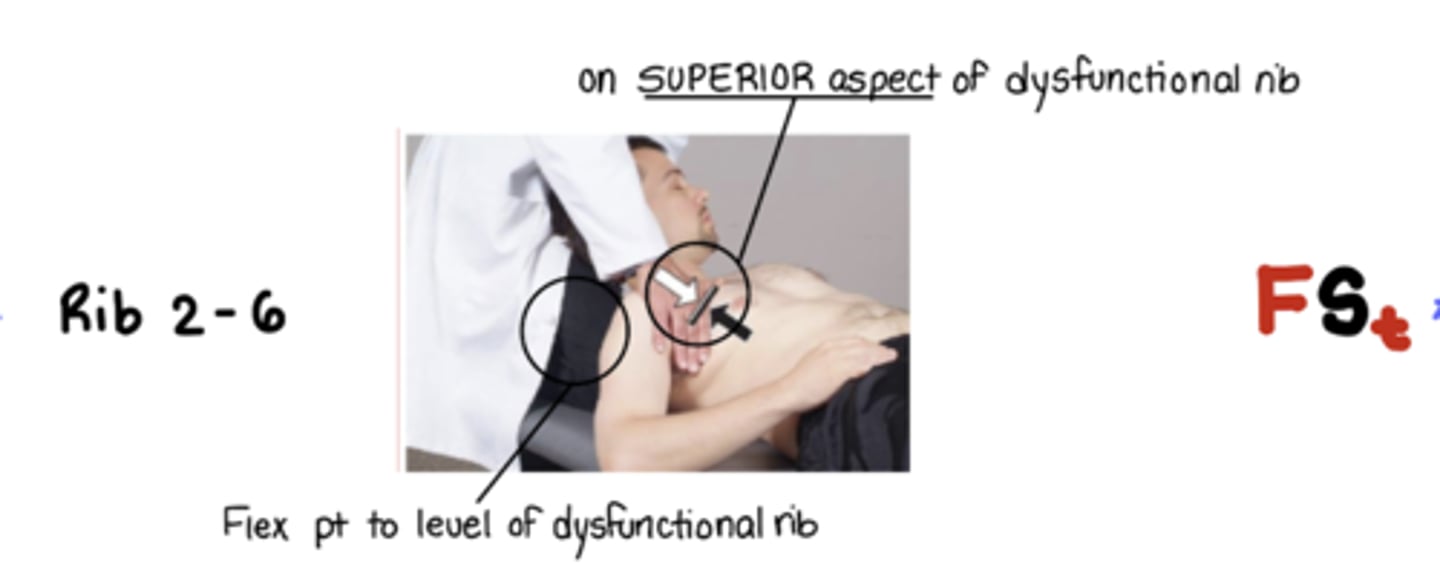
Rib 2-6 Inhalation MET
F St
MCP on superior aspect of rib - resisting with INHALATION, following into EXHALATION
Flex pt to level of dysfunctional rib
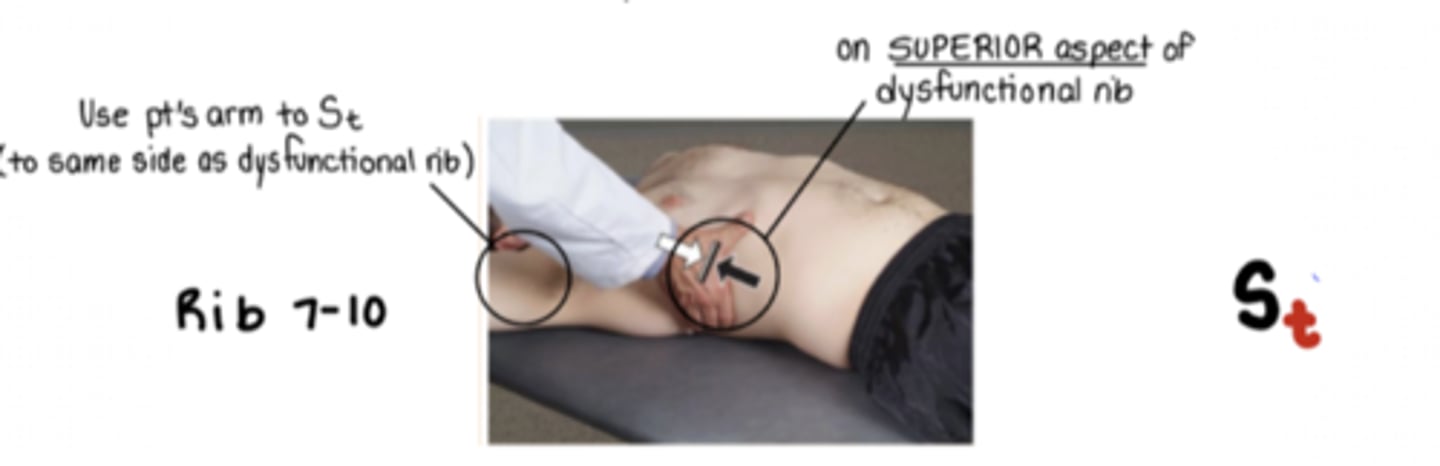
Rib 7-10 Inhalation MET
St
MCP on superior aspect of dysfunctional rib - resisting with INHALATION, following into EXHALATION
*use pt's arm to St
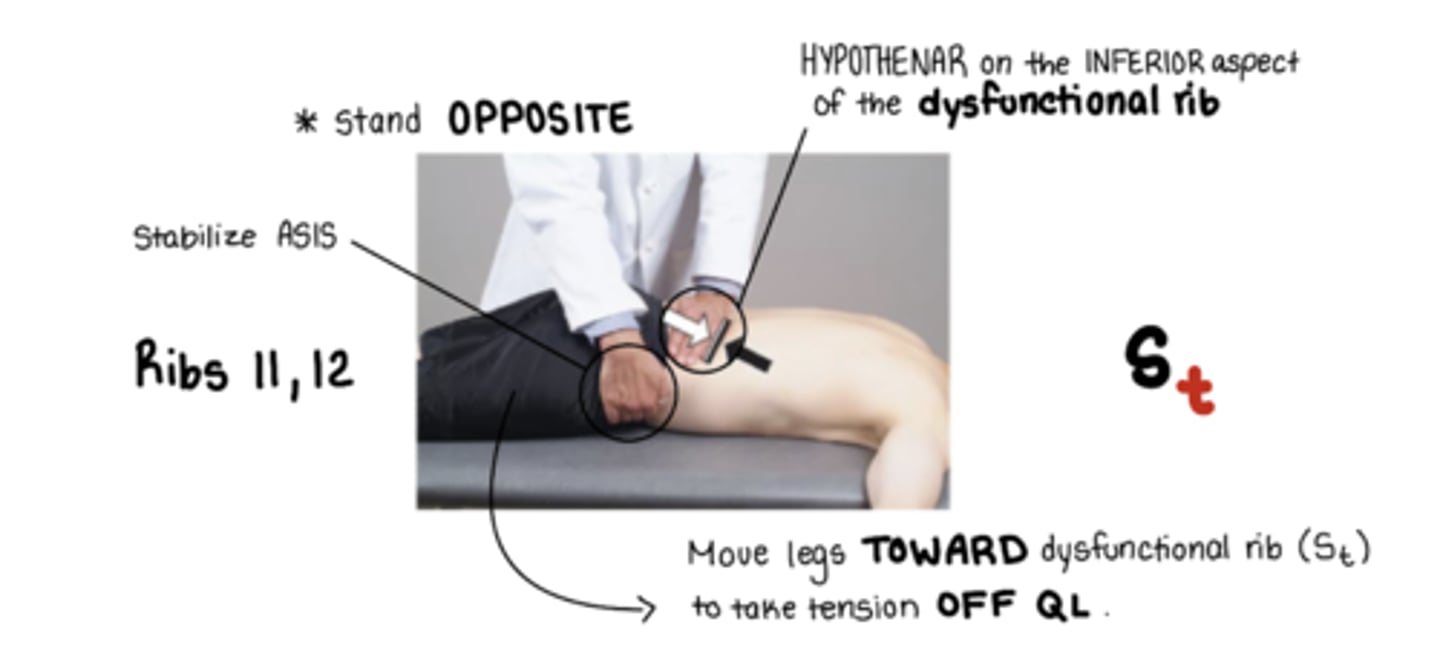
Ribs 11,12 Inhalation MET
St
active hand: HYPOTHENAR on the INFERIOR aspect of the dysfunctional rib resisting with INHALATION, following into EXHALATION
other hand stabilizing @ ASIS
HYPOTHENAR on the INFERIOR aspect of the dysfunctional rib
move legs away from me
(to take tension OFF QL)
ribs are stuck DOWN
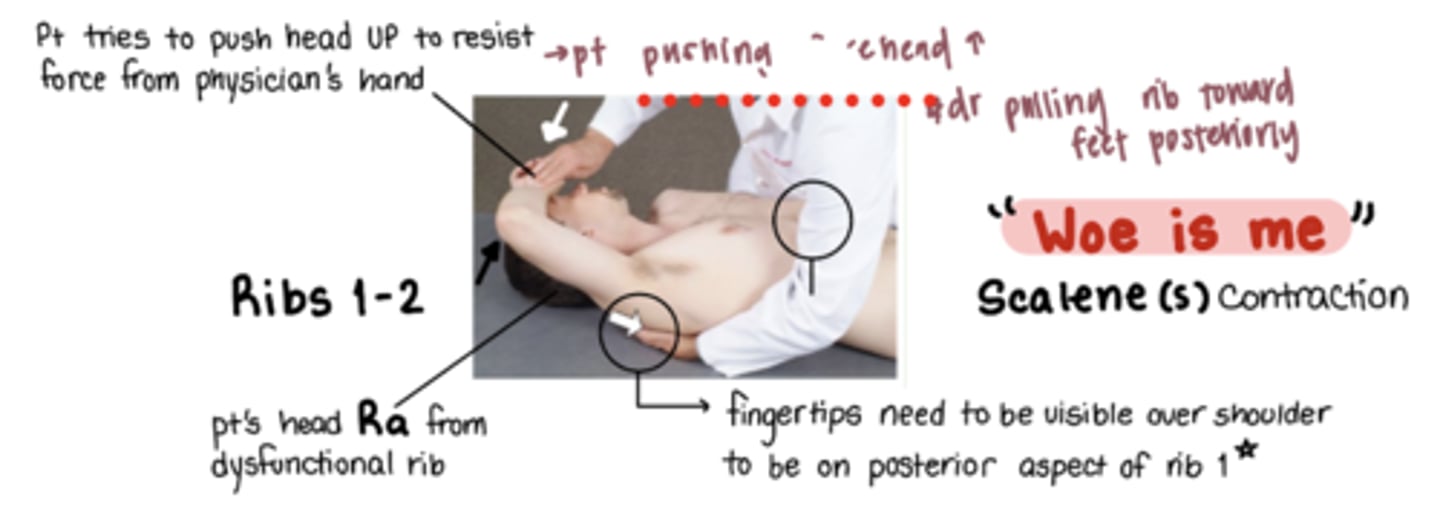
Ribs 1-2 Exhalation MET
"woe is me"
m: scalenes
stand on same side as SD
Pt head RA from dysfunctional rib
index and middle finger hook onto posterior and SUPERIOR aspect of the dysfunctional rib pulling rib inferolaterally at the rib angle
ribs are stuck DOWN
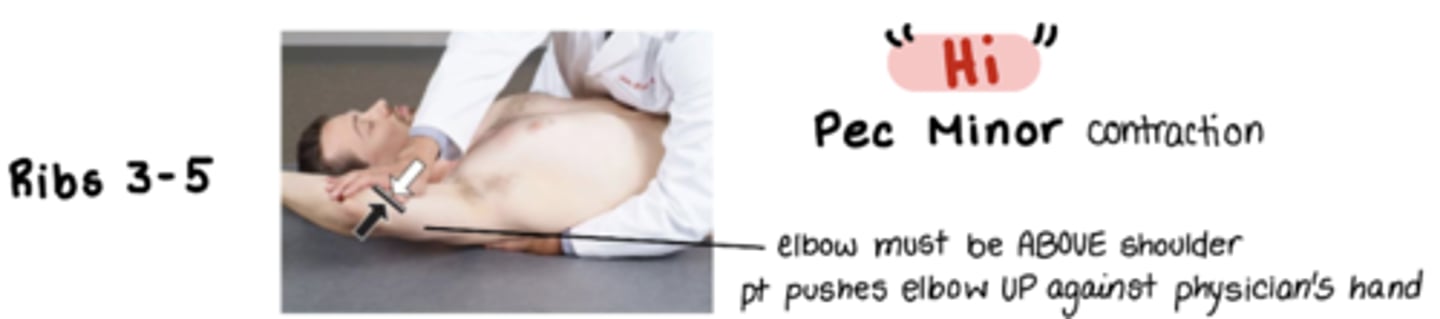
Ribs 3-5 Exhalation MET
"hi"
m: pec minor
pt elbow ABOVE shoulder pt pushes elbow UP against physicians hand
stand on same side as SD
index and middle finger hook onto posterior and SUPERIOR aspect of the dysfunctional rib pulling rib inferolaterally at the rib angle
ribs are stuck DOWN
Ribs 6-8 Exhalation MET
"stop"
m: serratus anterior
pt pushes elbow UP against physicians hand
stand on same side as SD
index and middle finger hook onto posterior and SUPERIOR aspect of the dysfunctional rib pulling rib inferolaterally at the rib angle
ribs are stuck DOWN

Rib 9 & 10 Exhalation MET
"Yes"
m: latissimus dorsi
stand on same side as SD
pt tries to push arm back DOWN against physician arm/leg
index and middle finger hook onto posterior and SUPERIOR aspect of the dysfunctional rib pulling rib inferolaterally at the rib angle
ribs are stuck DOWN

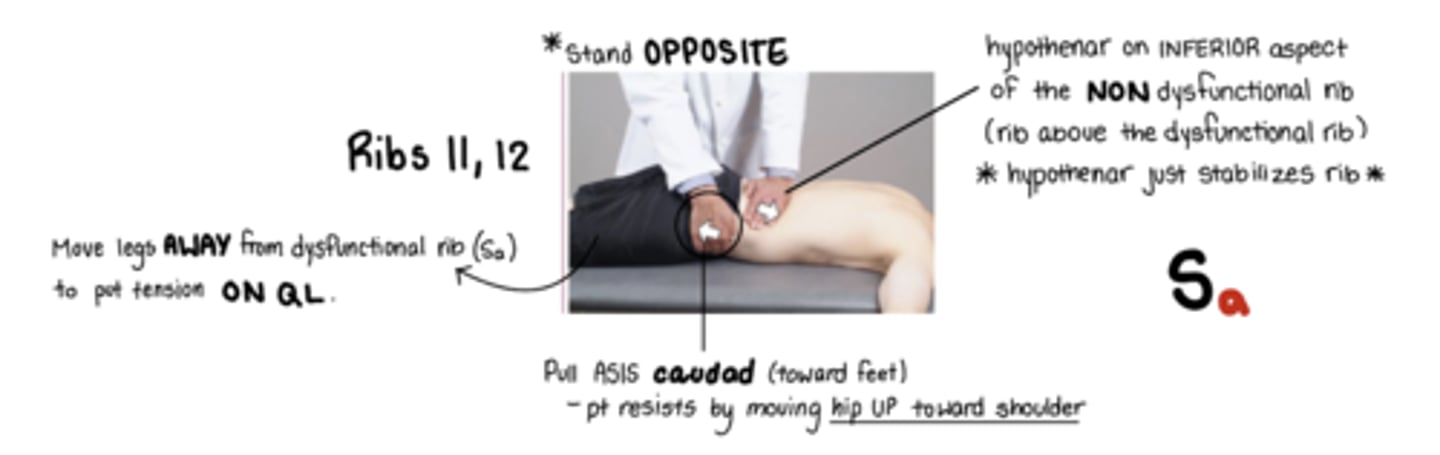
Ribs 11 & 12 Exhalation MET
Sa
*STAND OPPOSITE SIDE
active hand is the one on the ASIS - Pull ASIS caudad, pt resist by trying to pull their hip to shoulder
other hand stabiliizes rib:
hypothenar on INFERIOR aspect of the nondysfunctional rib (rib above the dysfunctional rib)
Sa = move legs to me
(ribs are stuck UP. QL does the work to push rib back down)
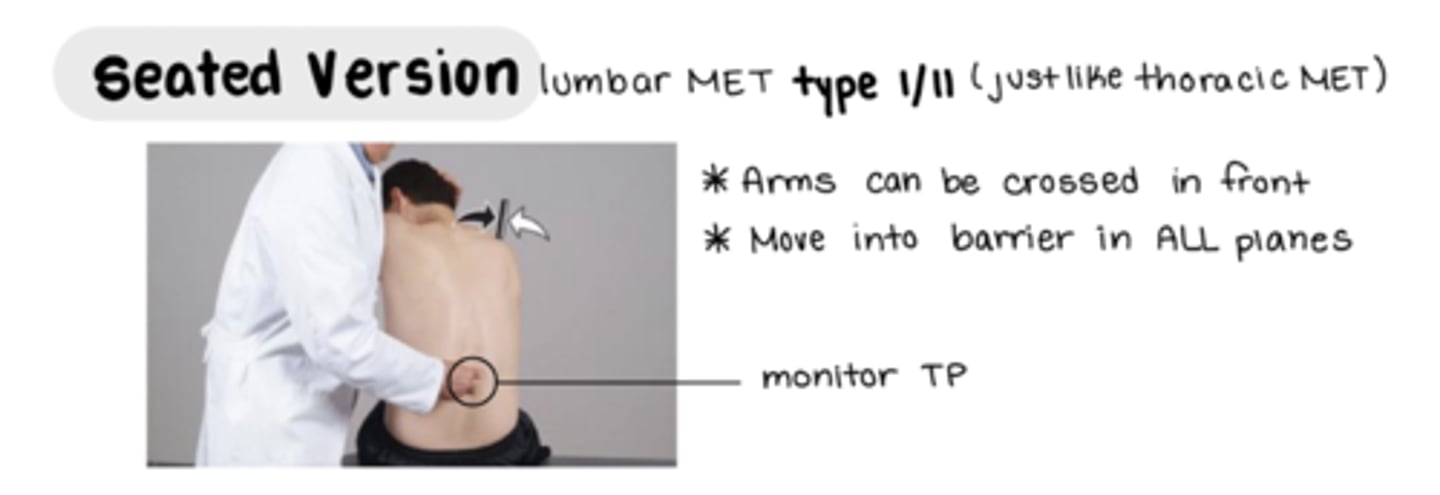
Lumbar MET Type 1/2 (sitting)
osteopathic hug or pt arm on neck
monitor TP
(same as thoracic sitting MET)
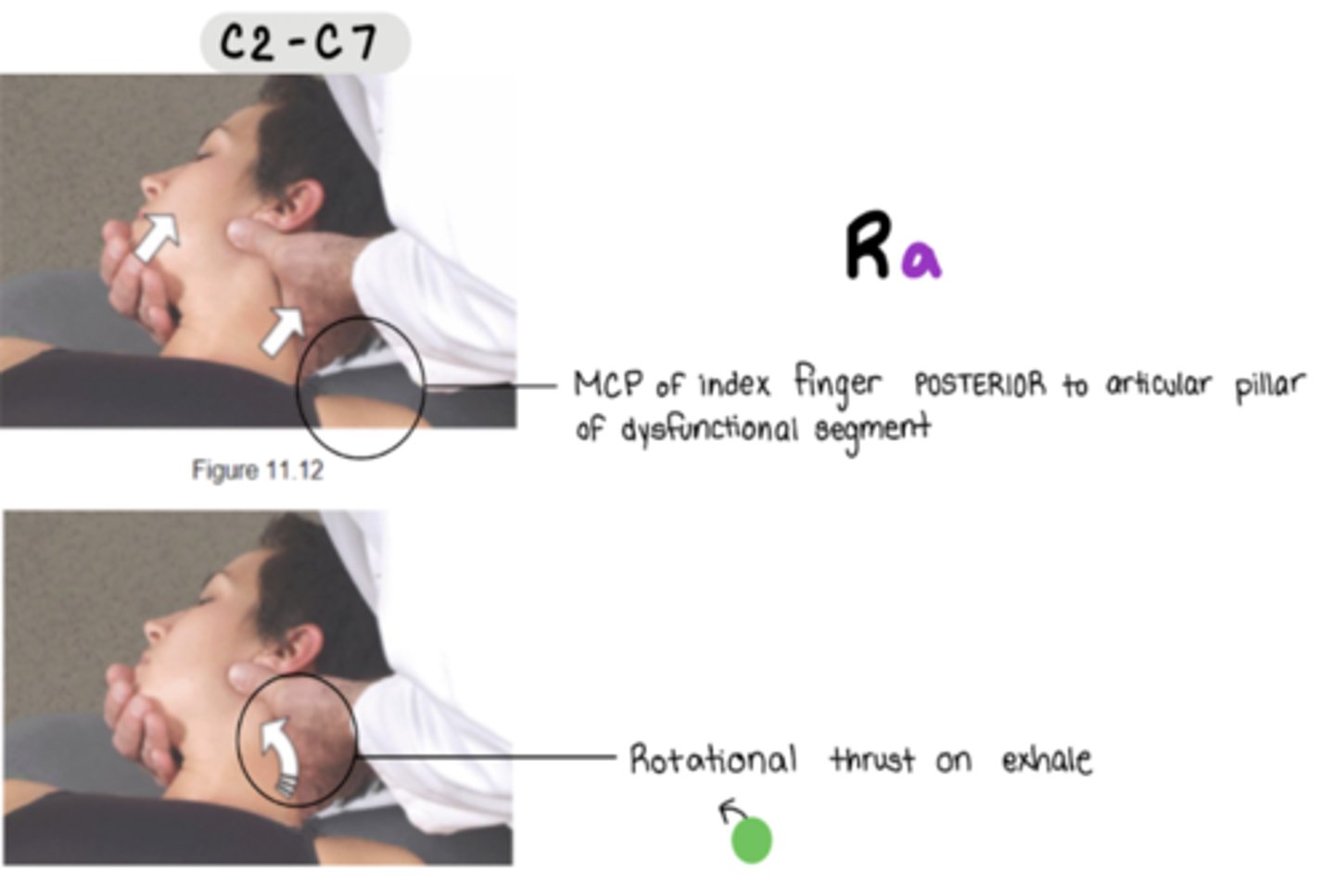
Cervical HVLA C2-C7
stand on SAME side of dysfunctional rotation component
MCP of index finger POSTERIOR to articular pillar of dysfunctional segment
**must lock out
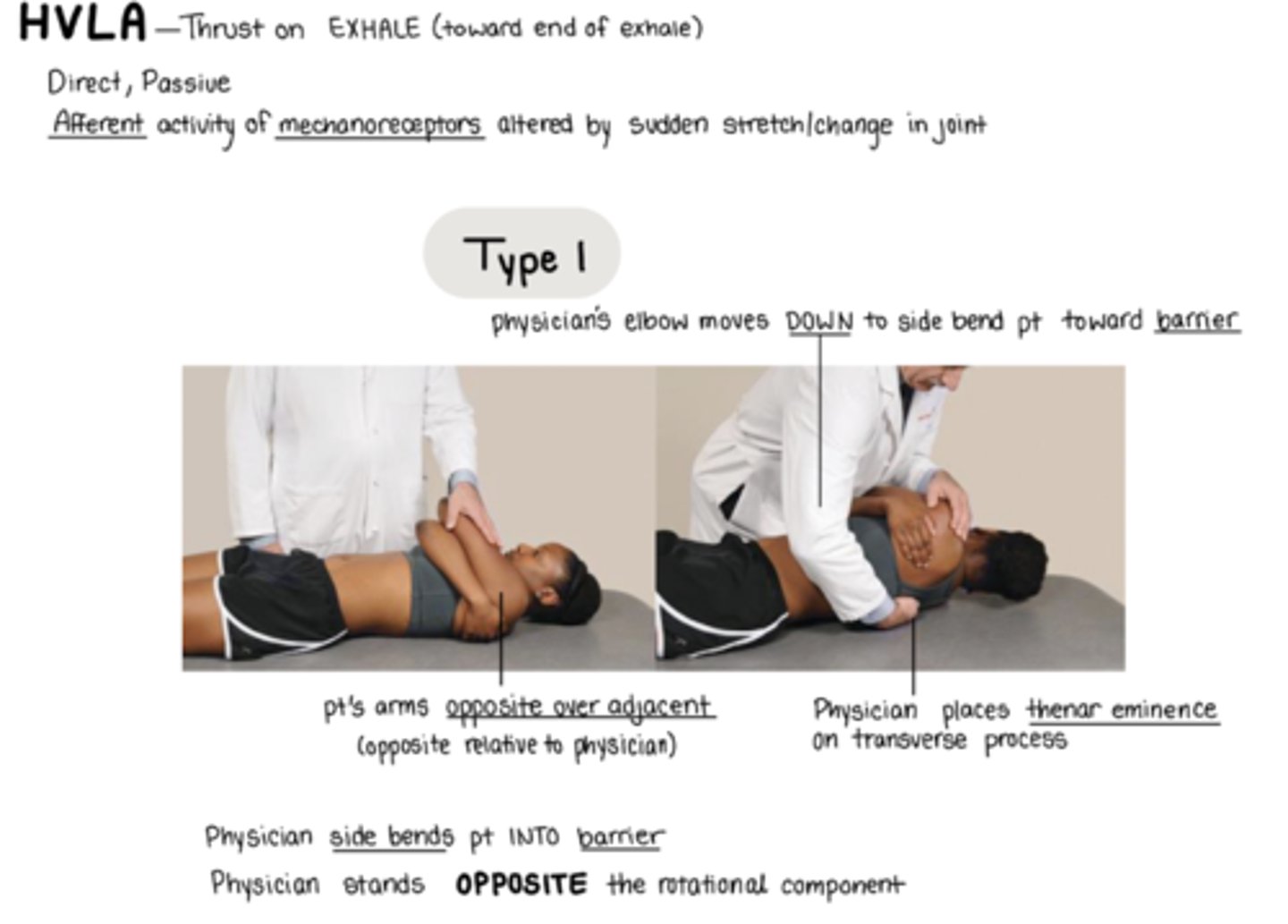
Thoracic HVLA Type 1 SD
pt supine, arms FAR/NEAR
physician stands on OPPOSITE side of the rotation component, pt faces toward you
place THENAR EMINENCE posterior to the rotated TP
Sidebend pt INTO barrier by moving elbow down
thrust @ end of pt exhale
*ensure thrust vector localizes to target spinal level
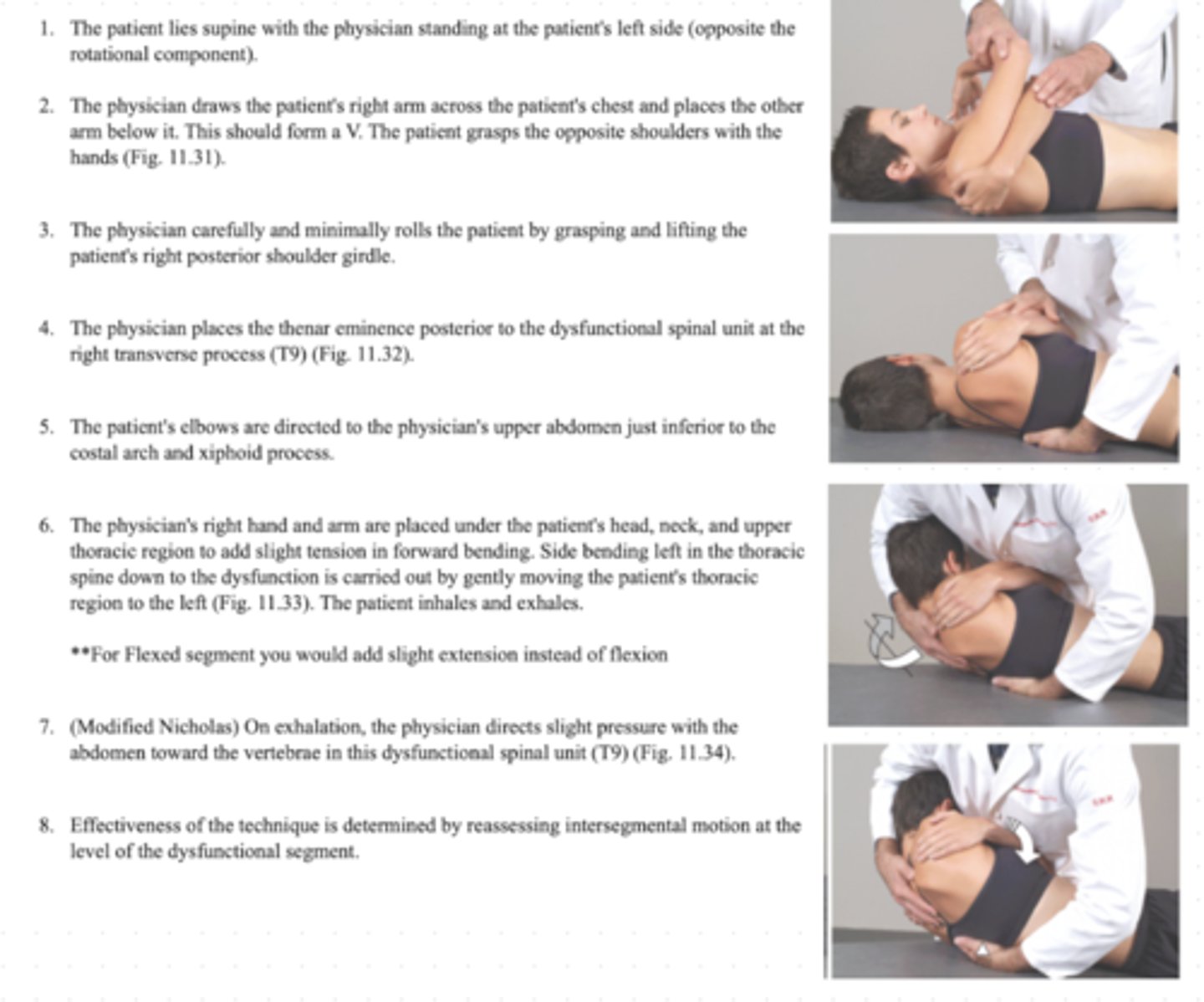
Thoracic HVLA Type 2 SD
pt supine, arms FAR/NEAR
stand on OPPOSITE side of rotational component
place THENAR EMINENCE posterior to the rotated TP
Sidebend pt INTO barrier by moving elbow UP
slight F/E
thrust @ end of pt exhale
*ensure thrust vector localizes to target spinal level
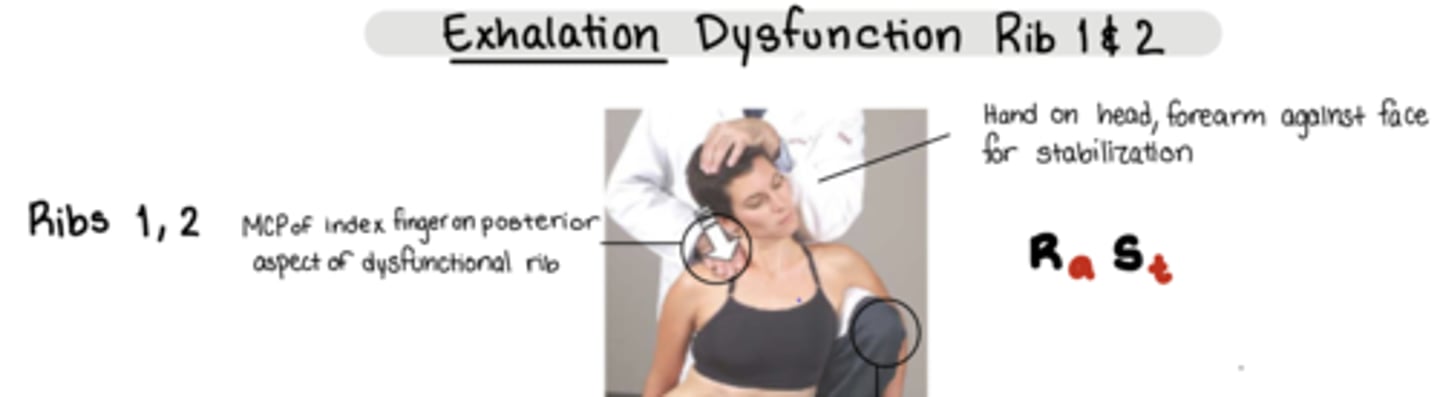
Rib 1,2 HVLA Exhalation SD
Ra St
Pt is SEATED
Physicians leg OPPOSITE of the SD on table to stabilize
one hand on pt head, forearm against head for stabilization
Thrust:
MCP of index finger on POSTERIOR aspect of dysfunctional rib - thrust @ end of exhalation
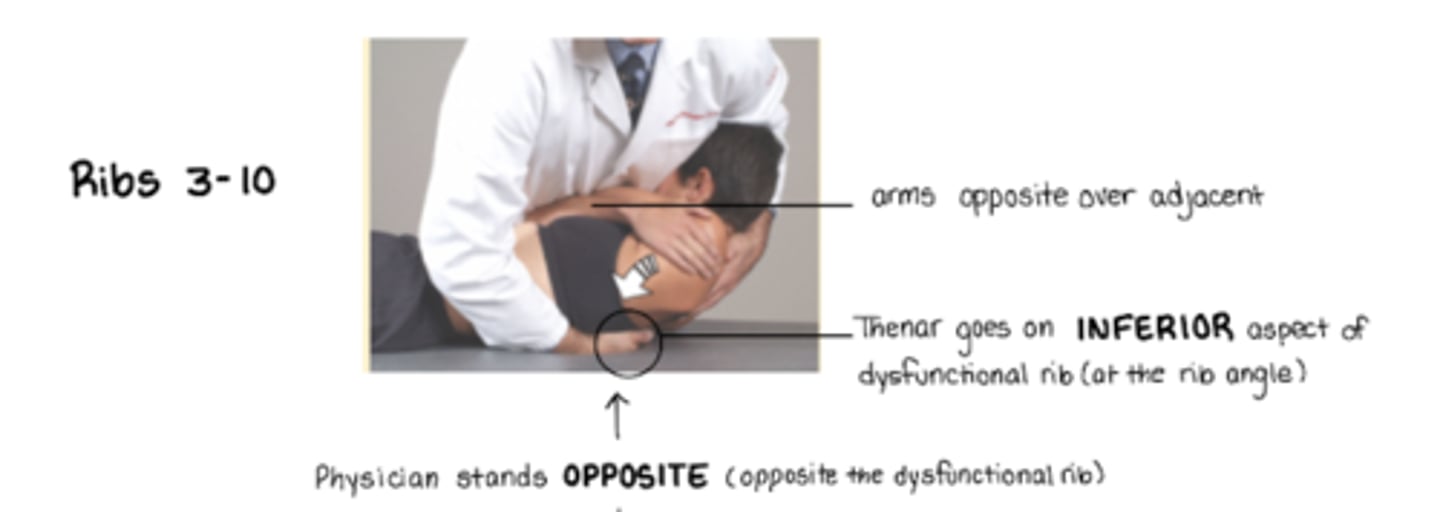
Ribs 3-10 HVLA Exhalation SD
pt supine, arms FAR/NEAR
stand on OPPOSITE side of dysfunctional rib
thenar eminence on inferior angle of rib angle to push rib back UP
ribs stuck DOWN
(basically thoracic HVLA other than hand placement)
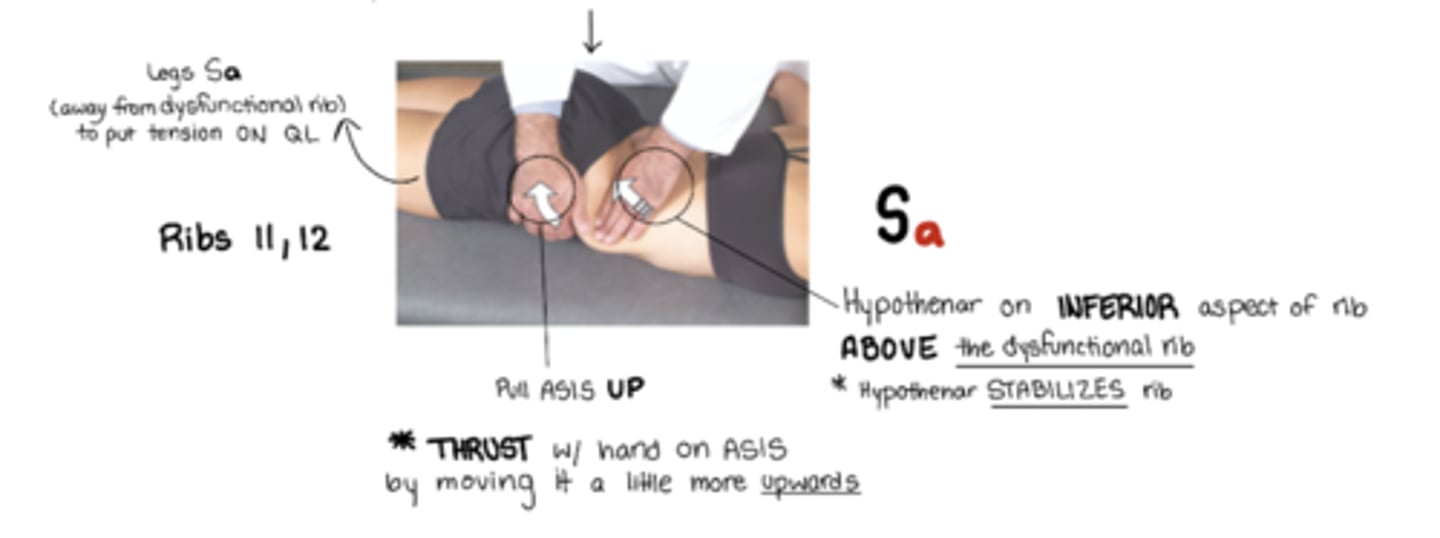
Ribs 11,12 HVLA Exhalation SD
Sa = legs away from dysfunctional rib
stand OPPOSITE of dysfunctional rib
active hand: hand pulls UP on ASIS to push rib back down
other hand: hypothenar eminence on inferior aspect of rib ABOVE dysfunctional rib to stabilize rib
ribs stuck UP
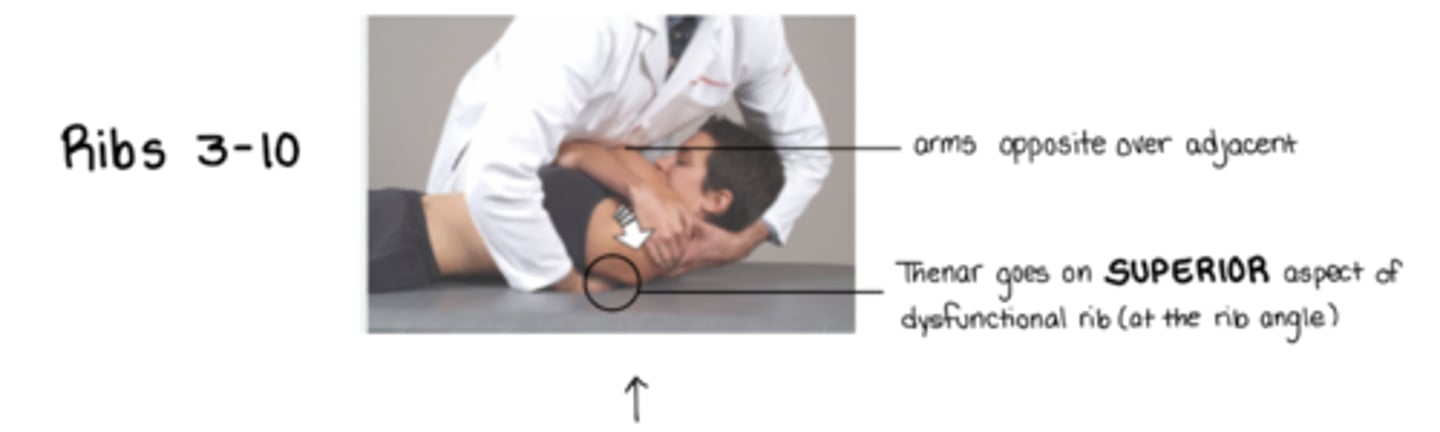
Ribs 3-10 HVLA Inhalation SD
pt arms FAR/NEAR
stand on OPPOSITE side of dysfunctional rib
thenar eminence on superior angle of dysfunctional rib at the rib angle
ribs stuck UP
(basically thoracic HVLA other than hand placement)
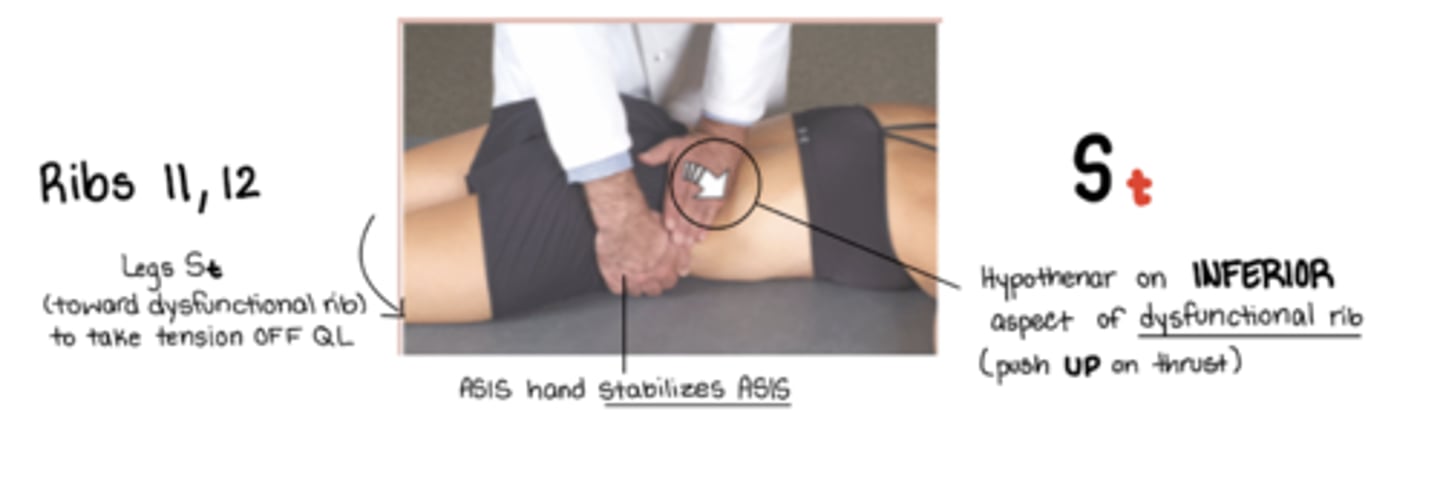
Ribs 11,12 HVLA Inhalation SD
St = legs away from me
standing OPPOSITE side of dysfunctional rib
hypothenar eminence on inferior aspect of dysfunctional rib - to push rib back UP
(other hand stabilizes on ASIS)
ribs stuck DOWN
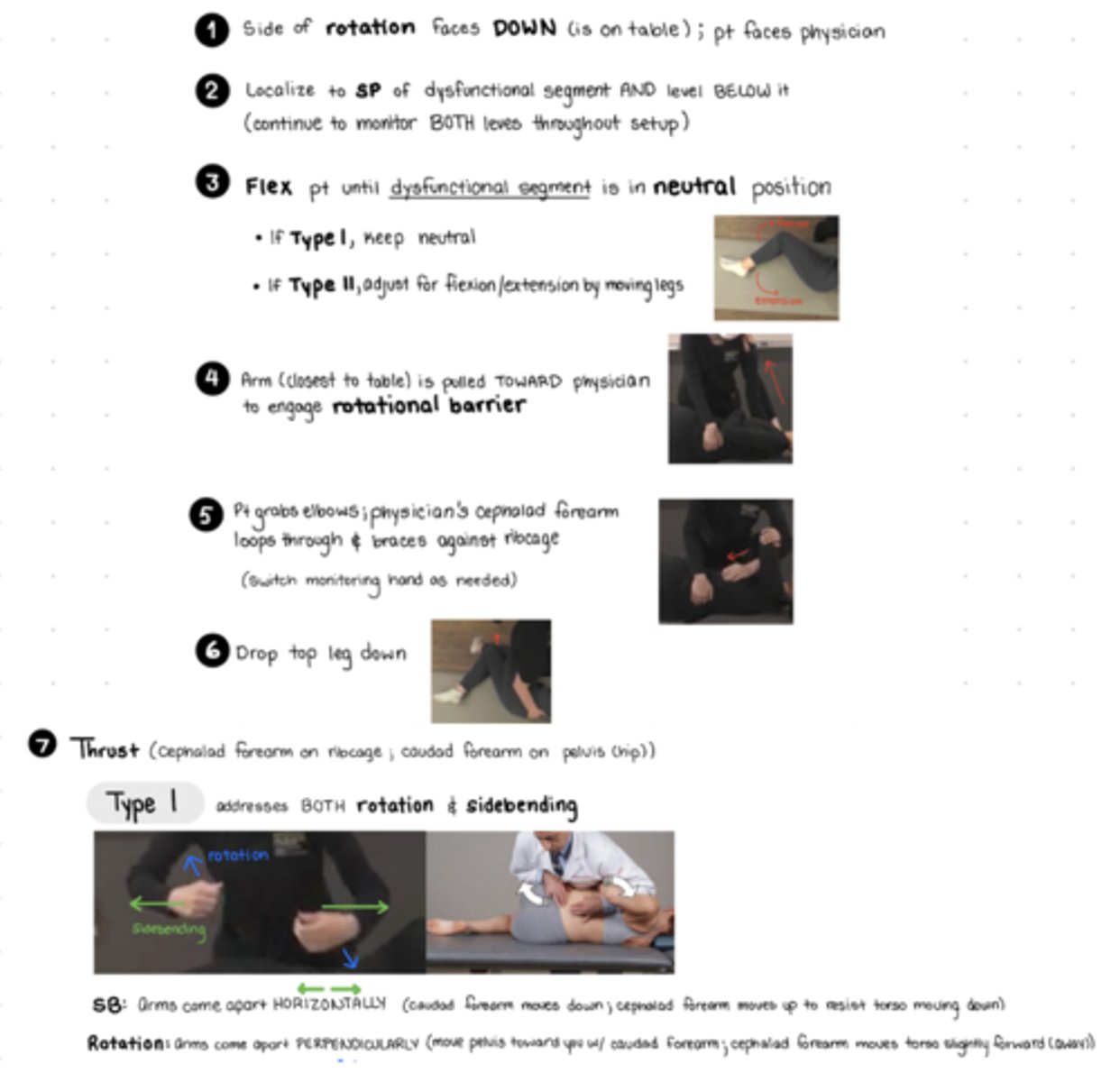
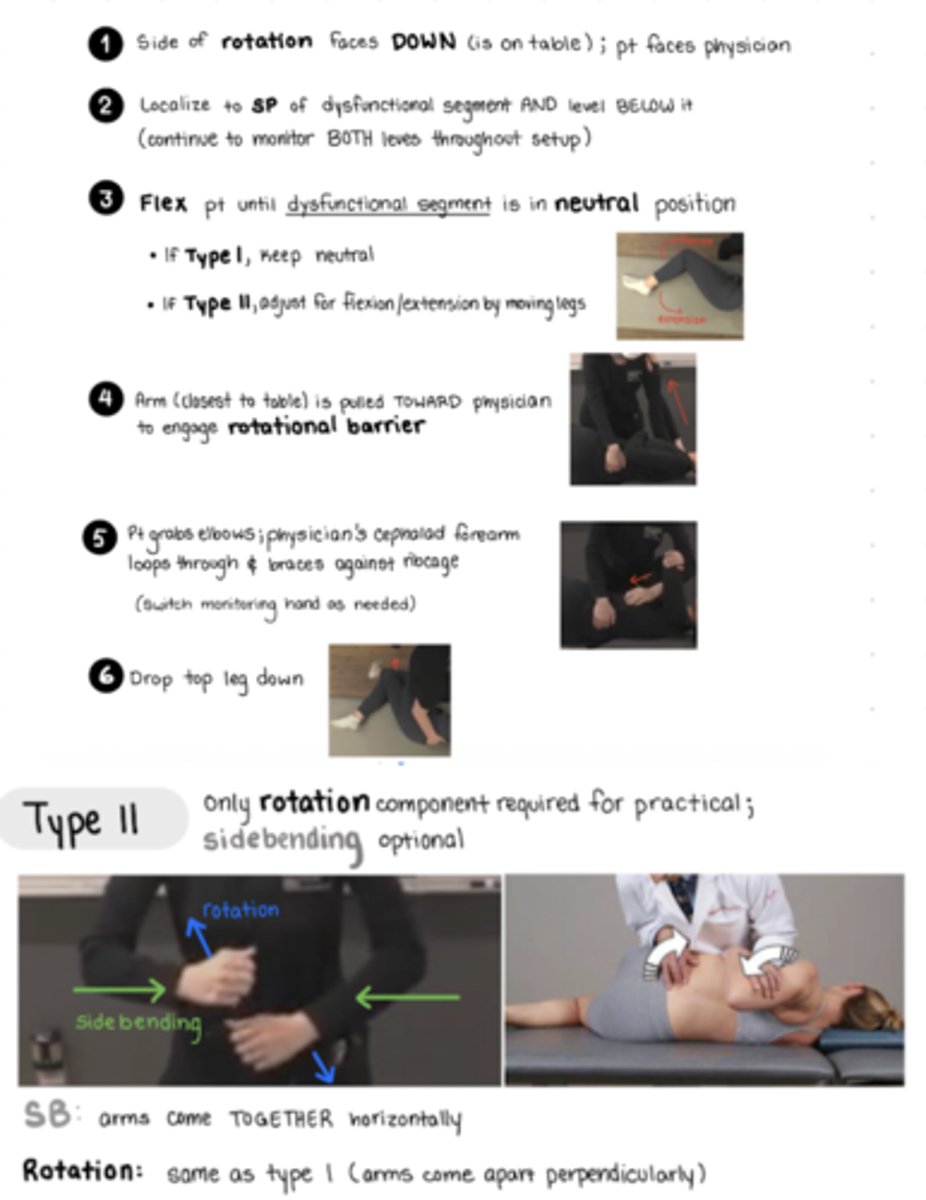
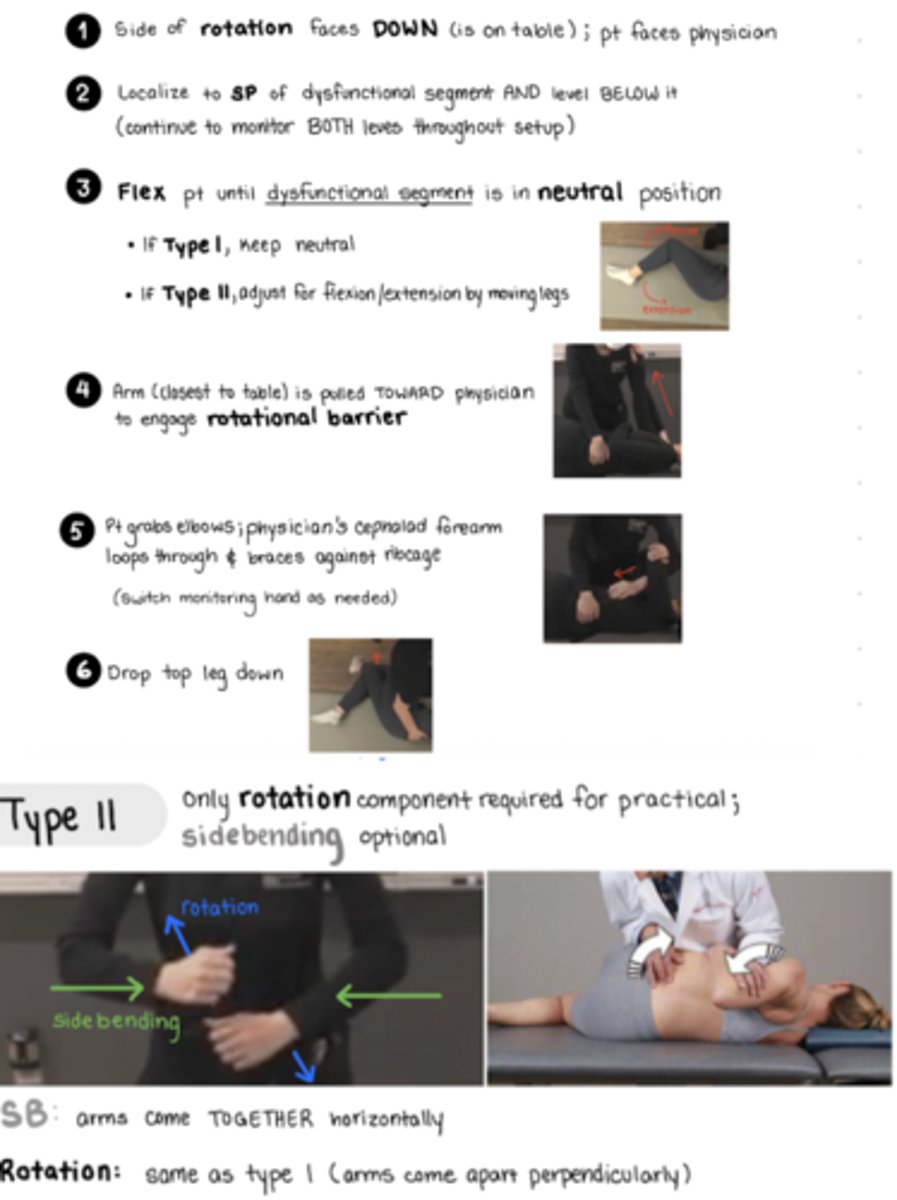
Lumbar HVLA Type 1 SD
Pt lays on SAME side as rotational component of dysfunction
pt lying facing physician
flex to localize to SP of dysfunctional segment AND level below it - monitor both levels throughout set up
*flex just enough so that the dysfunctional segment is in the neutral position
arm closest to table is pulled TOWARD physician to engage ROTATIONAL BARRIER (have pt hold your shoulder to pull them)
pt grabs their elbows, physician loops cephalad arm through (this is the arm monitoring @ SP), brace forearm against ribcage
caudad forearm placed over greater trochanter
top leg drops down off table, cepahald to the bottom leg now
THRUST: OUT and rotate
SB: arms come apart horizontally - caudad forearm moves DOWN, cephalad forearm moves UP to resist torso from moving down
ROTATION: arms come apart PERPENDICULARLY - moving pelvis toward physician with caudad arm, cephalad forearm moves torso slightly forward (AWAY)
Lumbar HVLA Type 2 Flexion SD
Pt lays on SAME side as rotational component of dysfunction
pt lying facing physician
flex to localize to SP of dysfunctional segment AND level below it - monitor both levels throughout set up
*flex just enough so that the dysfunctional segment is in the neutral position -
arm closest to table is pulled TOWARD physician to engage ROTATIONAL BARRIER (have pt hold your shoulder to pull them
pt grabs their elbows, physician loops cephalad arm through (this is the arm monitoring @ SP), brace forearm against ribcage
caudad forearm placed over greater trochanter
have pt straighten bottom leg to induce EXTENSION, top leg drops down off table, cepahald to the bottom leg now
THRUST: IN and rotate
SB: arms come TOGETHER horizontally
Rotation: ROTATION: arms come apart PERPENDICULARLY - moving pelvis toward physician with caudad arm, cephalad forearm moves torso slightly forward (AWAY)
Lumbar HVLA Type 2 Extension SD
Pt lays on SAME side as rotational component of dysfunction
pt lying facing physician
flex to localize to SP of dysfunctional segment AND level below it - monitor both levels throughout set up
*flex just enough so that the dysfunctional segment is in the neutral position -
arm closest to table is pulled TOWARD physician to engage ROTATIONAL BARRIER (have pt hold your shoulder to pull them
pt grabs their elbows, physician loops cephalad arm through (this is the arm monitoring @ SP), brace forearm against ribcage
caudad forearm placed over greater trochanter
flex by pulling legs in until flexion at the level of the dysfunction, bottom leg will stay flexed, top leg drops down off table, cepahald to the bottom leg now
THRUST: IN and rotate
SB: arms come TOGETHER horizontally
Rotation: ROTATION: arms come apart PERPENDICULARLY - moving pelvis toward physician with caudad arm, cephalad forearm moves torso slightly forward (AWAY)
Diagnosis of the OA
OA = opposite always (type 1 mechanics) d/t position of the lateral AO ligament
for examination: translate head from left - right and right to left with head in neutral position
dx: determine translation (gives S/R) check with slight flexion/extension
ex: if motion is greater from L to R, freedom is side-bent L and rotated right (restriction in right side-bending), if restriction of lateral translation is MORE signficant in flexion, but goes away in extension, then the segment is extended
Diagnosis of AA
AA = rotation ONLY
you must be standing
1. ensure pt nods head forward to lock out OA joint
2. flex pt next to approx 45 degrees until locking occurs below the AA joint in the rest of the cervical spine
3. slowly rotate head from midline to left and then midline to right
if head rotates more freely to the right the diagnosis is AA Rr
Diagnosis of the typical cervical spine (C2-C7).
C2-C7 follow type 2 mechanics
1. palpate spinous process of segment being evaluated
2. move fingers laterally about 1/2 an inch and anteriorly to palpate articular pillars
3. feel which side appears more posterior to the table
OR push articular pillar gently from left to right and right to left - identify loss of translation
4. check segments in F/E
first branch of left and right subclavian artery enters @ C5-C6 level into the transverse foramen of vertebra
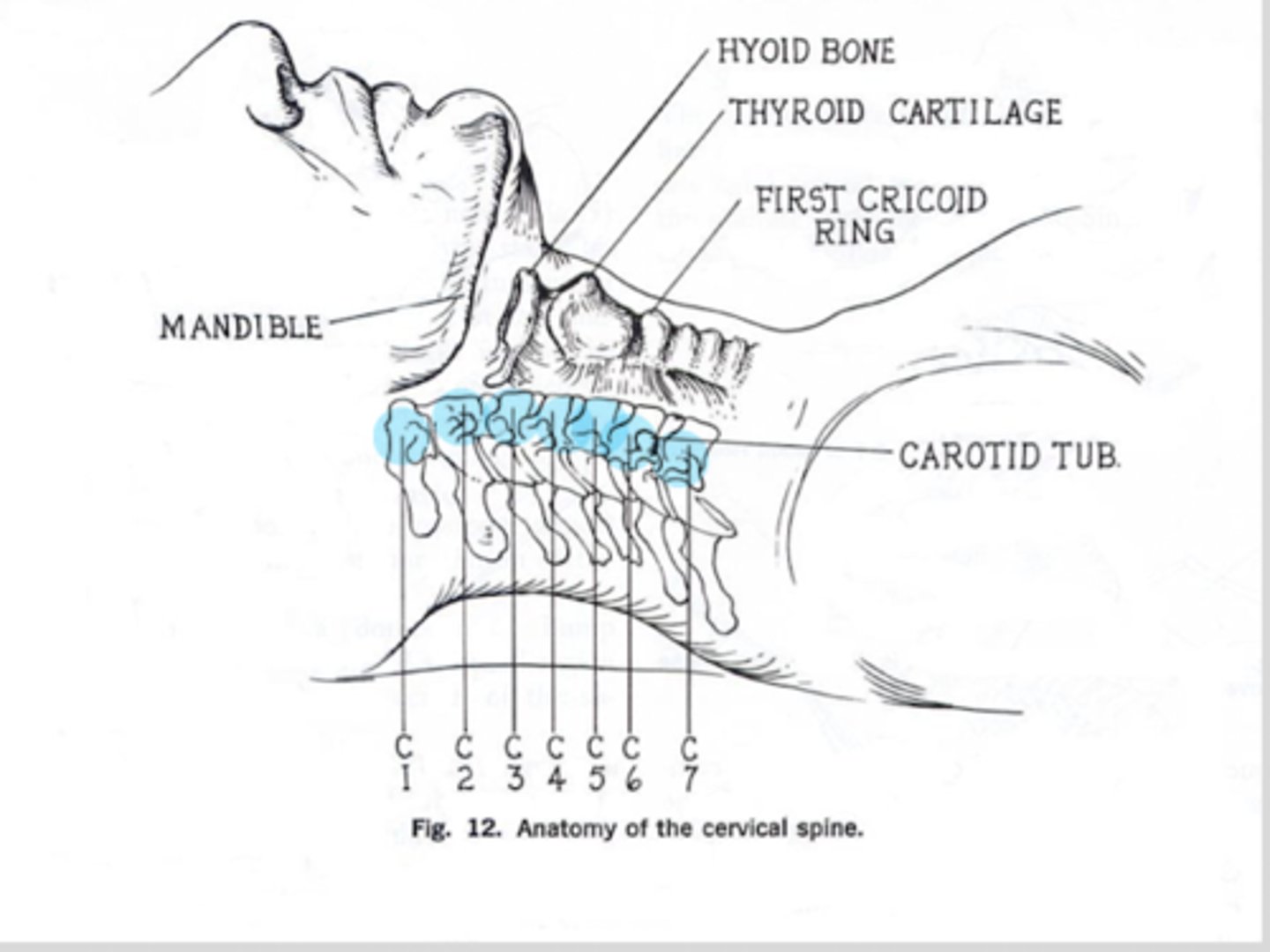
LANDMARKS:
C1: TP located behind ascending ramus of jaw
C2: level of the angle of the mandible
C3: level of hyoid bone
C4: @ superior aspect of thyroid cartilage
C5: @ thyroid cartilage body
C6: @ first cricoid ring or carotid tubercle
C7: vertebral prominens
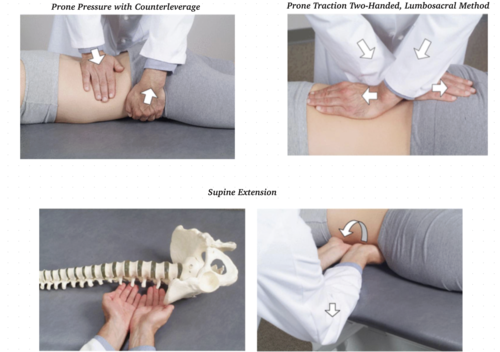
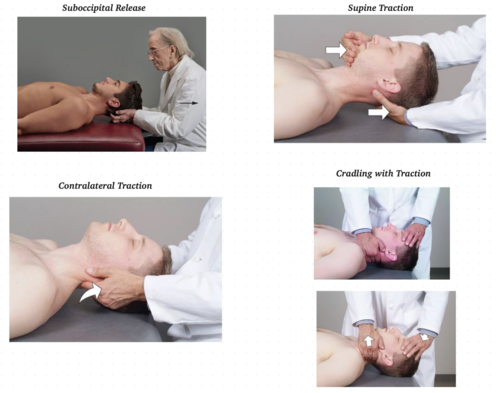
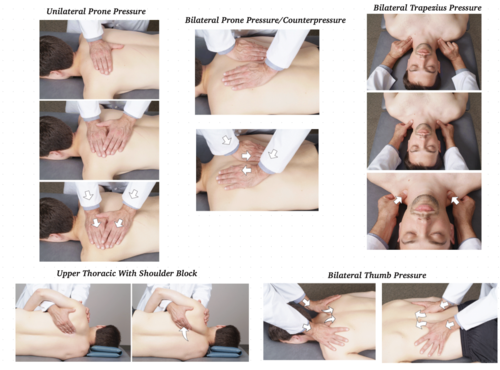
Cervical Soft Tissue
Thoracic Soft Tissue
Lumbar Soft Tissue