Lecture 2- Chest Xray pt 1
1/38
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
39 Terms
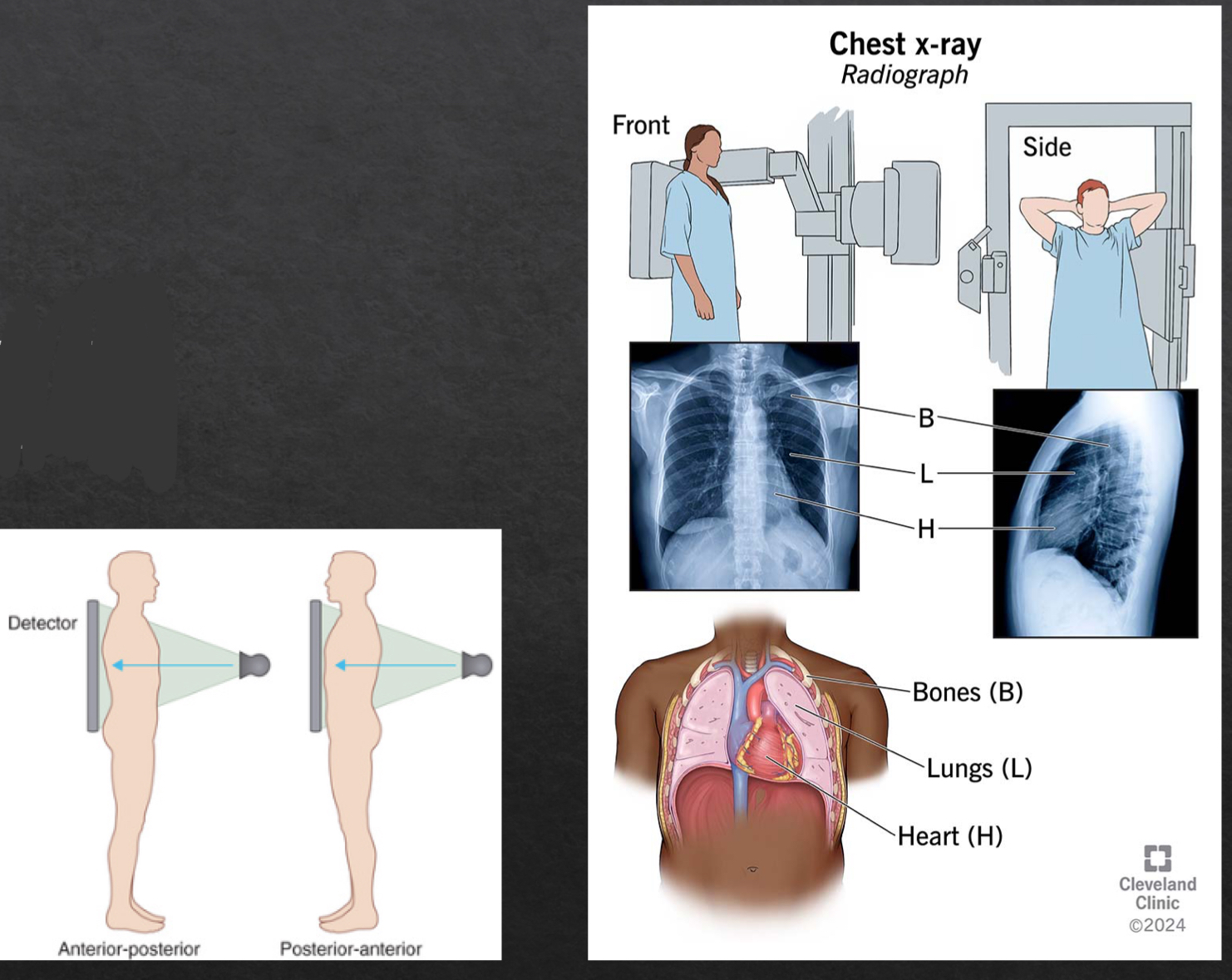
views of a chest X-ray
frontal
posteroanterior (PA)
anteroposterior (AP)
lateral
left lateral
why order lateral chest xray
determine location of disease seen on frontal view
confirm presence of disease suspected on frontal view
demonstrate disease not visible on frontal view
what to look for on lateral view xray
retrosternal space
hilar region
fissures
thoracic spine
diaphragm and posterior costophrenic sulci
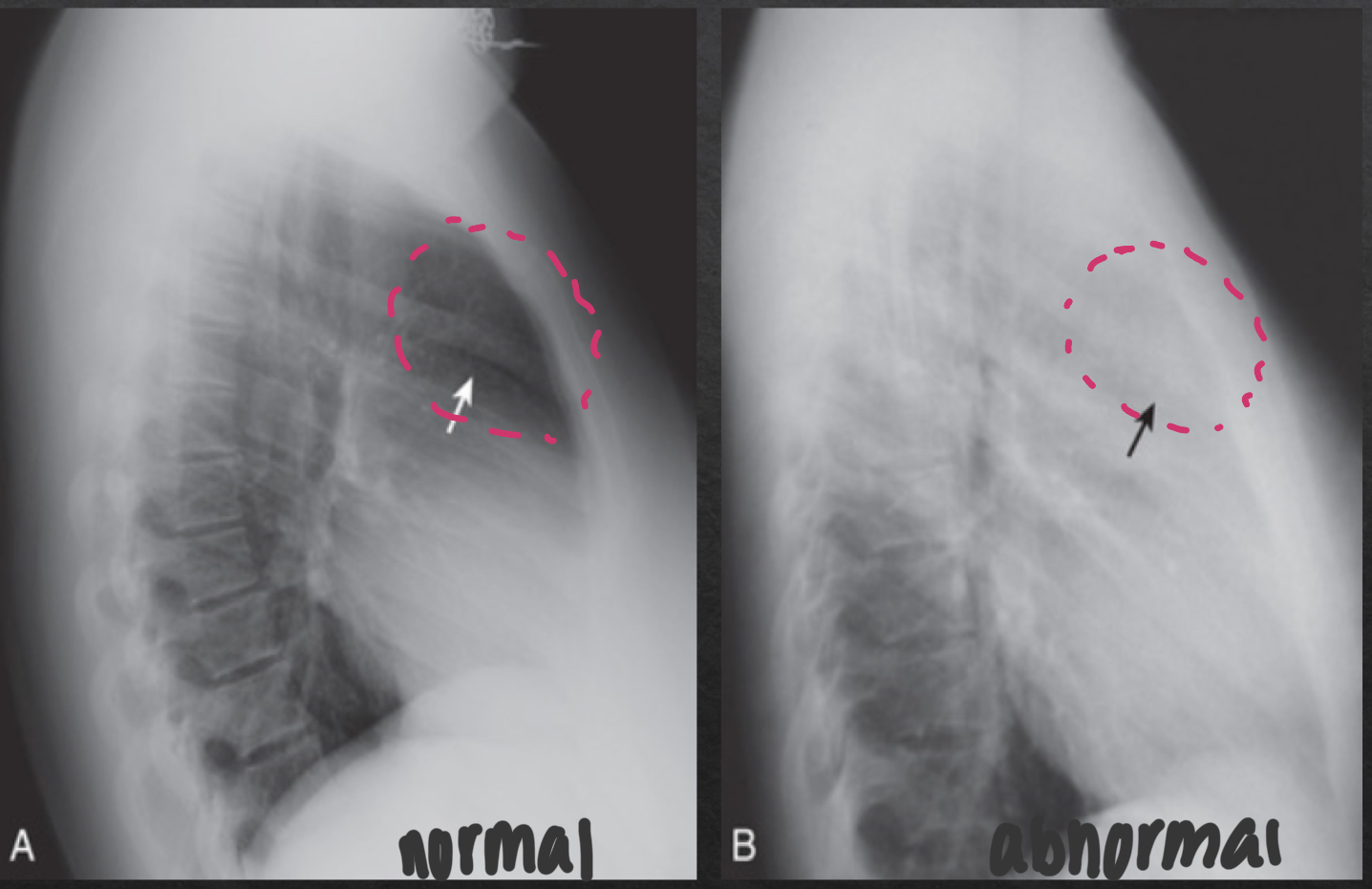
retrosternal space
NORMAL
lucent crescent btwn sternum and ascending aorta/anterior heart
ABNORMAL
soft tissue density filling normal space behind the sternum
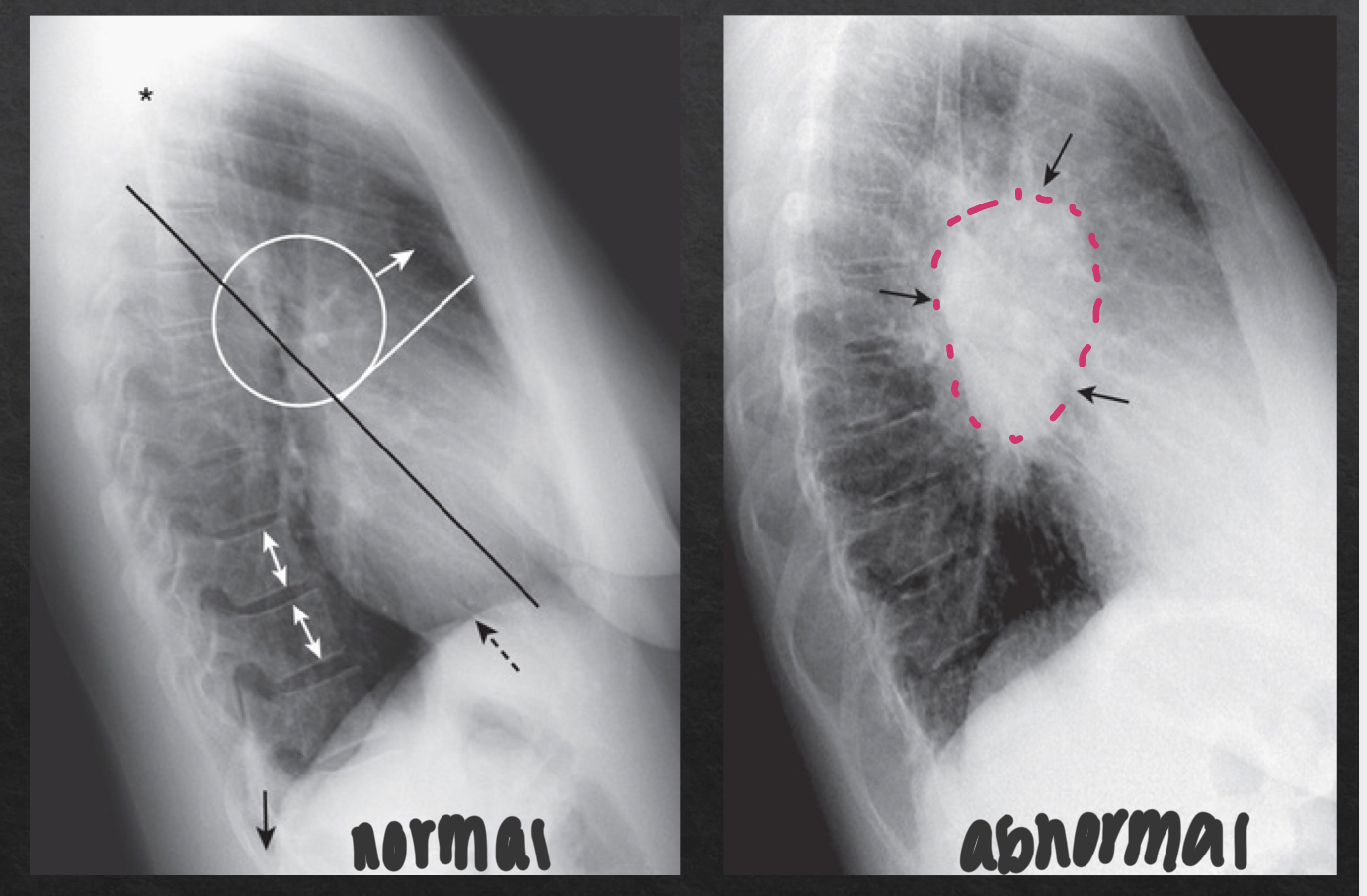
hilar region: lateral view
consists of pulmonary vasculature, pymph nodes, aft, and major bronchi
NORMAL
no discrete mass present
ABNORMAL
distinct, opaque hilar mass
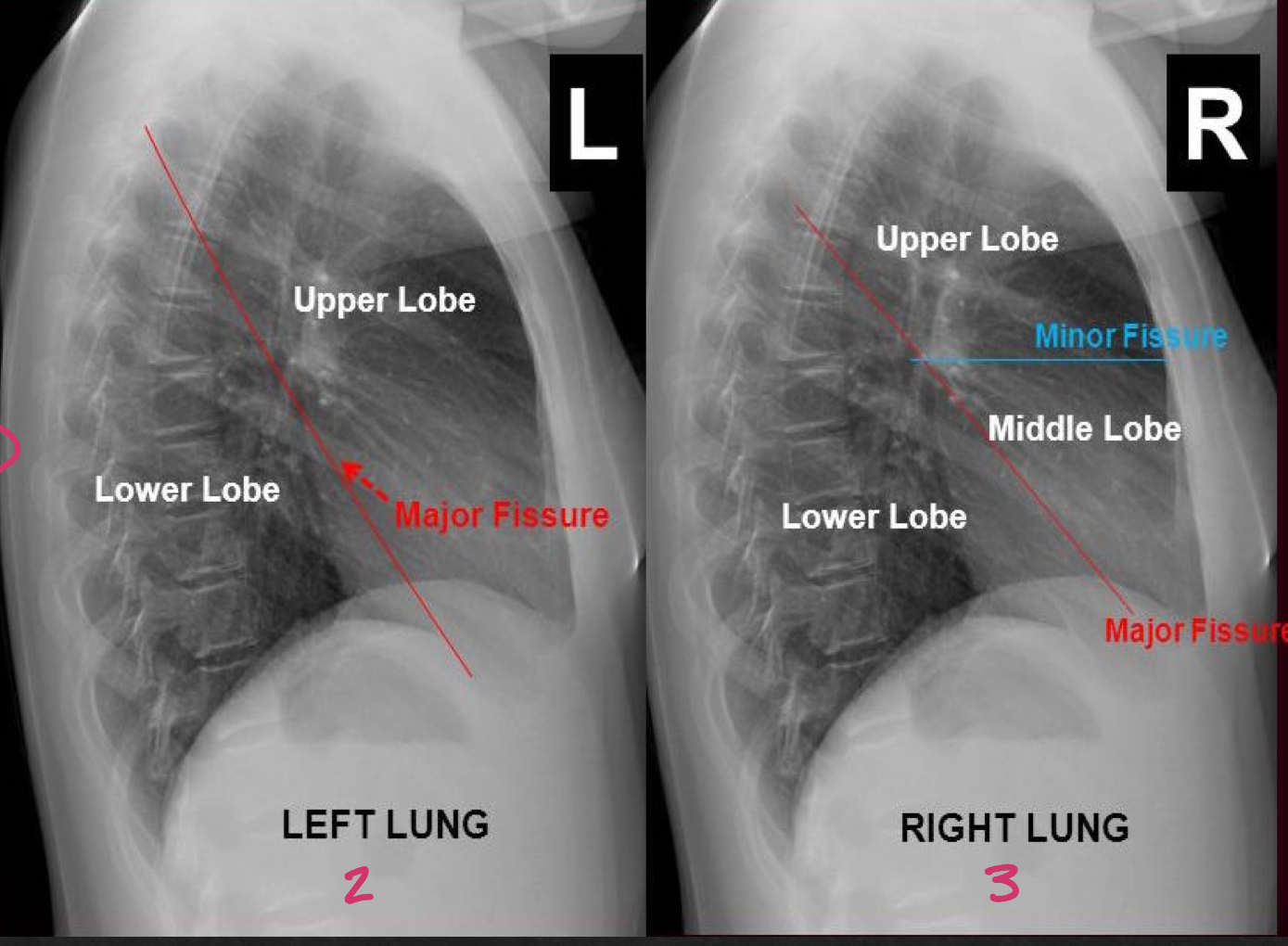
fissures and lung fields; lateral view
major (oblique) and minor (horizontal) fissures should be pencil thin or not visible
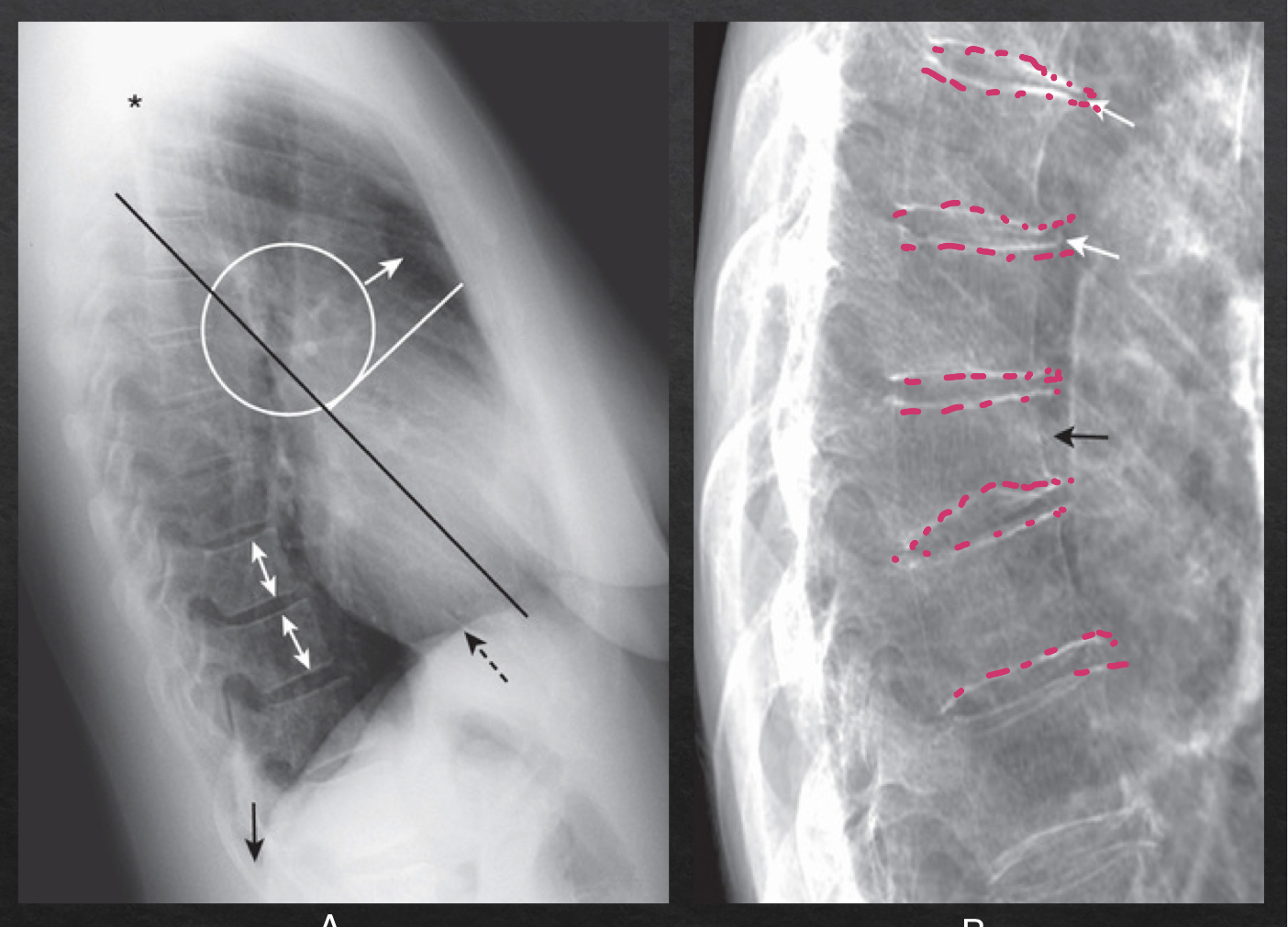
thoracic spine: lateral view
NORMAL
rectangular vertebra; bodies with parallel endplates
disk spaces maintain height from top to bottom of thoracic spine
ABNORMAL
narrowing of disc space
vertebral body loses height (compression fracture)
bony spurring
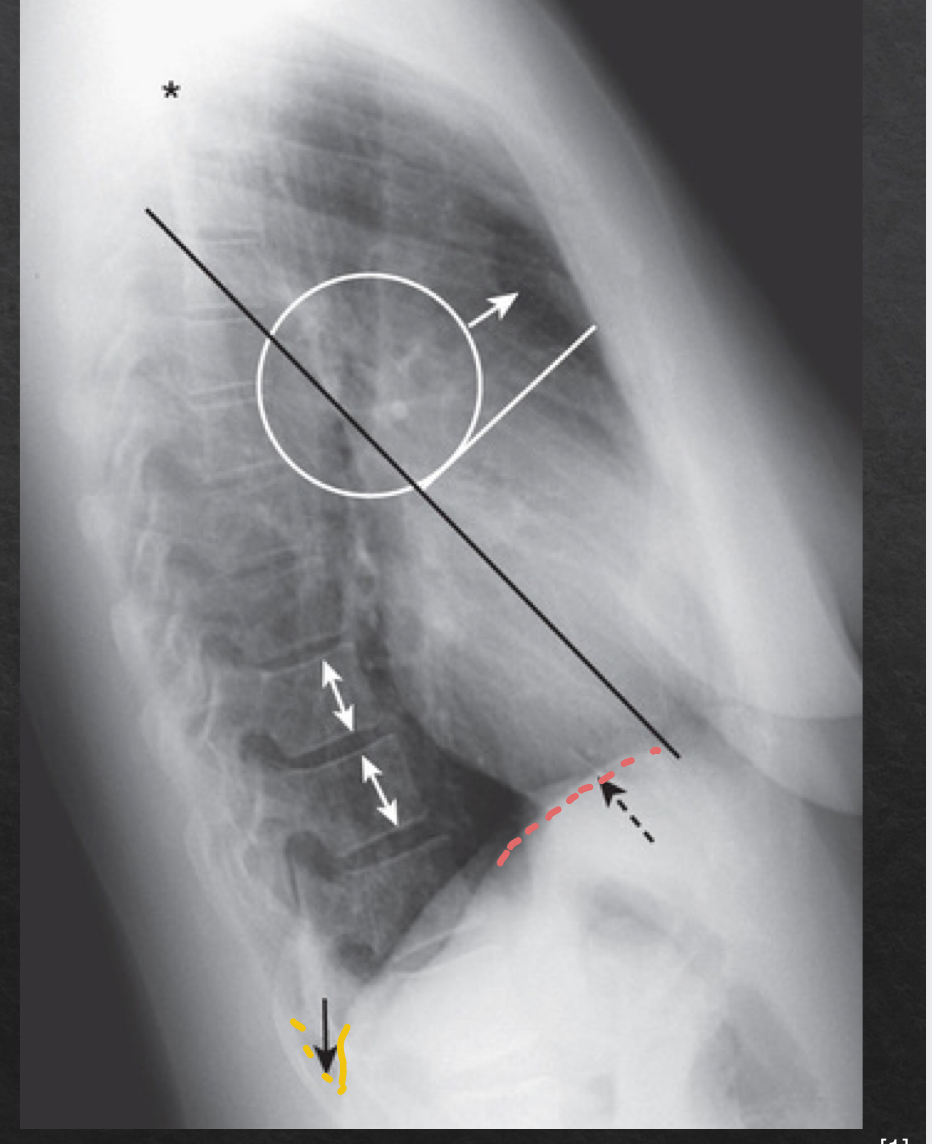
diaphragm and posterior costophrenic sulci: lateral view
NORMAL
sharp posterior costophrenic sulci
R and L hemidiaphragm
R hemi is usually slightly higher and visible for its entire length front to back
L hemi anterior edge usually not visible (silhoueted by heart anteriorly) and posterior edge seen sharply
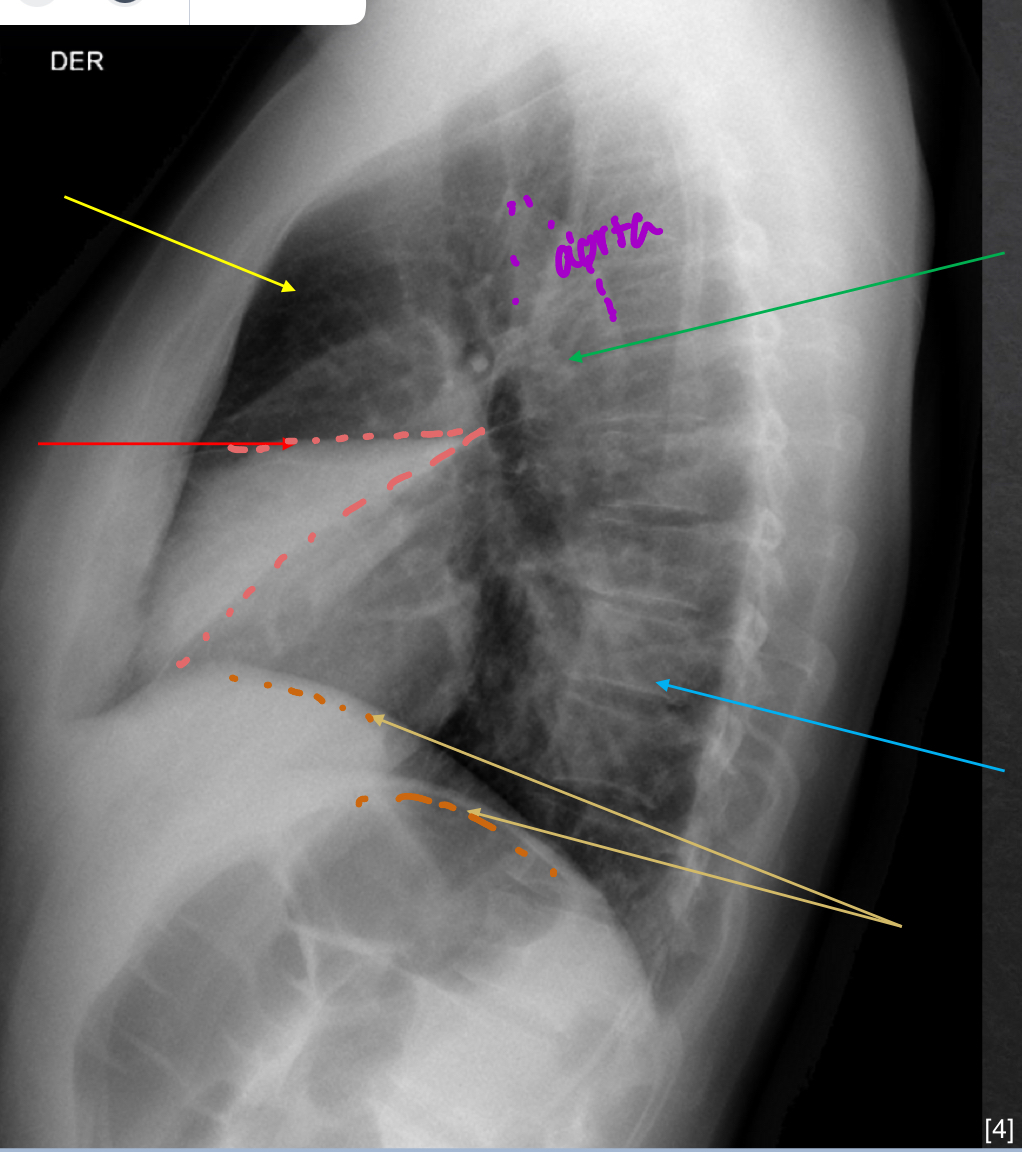
yellow: retrosternal spcae-clear
green: hilar region- no mass
red: fissures- VISIBLE
blue: thoracic spine- good
orange: diaphram and post costo sulci- slightly elevated
technical adequacy of chest xray
PRIMA
Penetration
Rotation
Inspiration
Magnification
Angulation
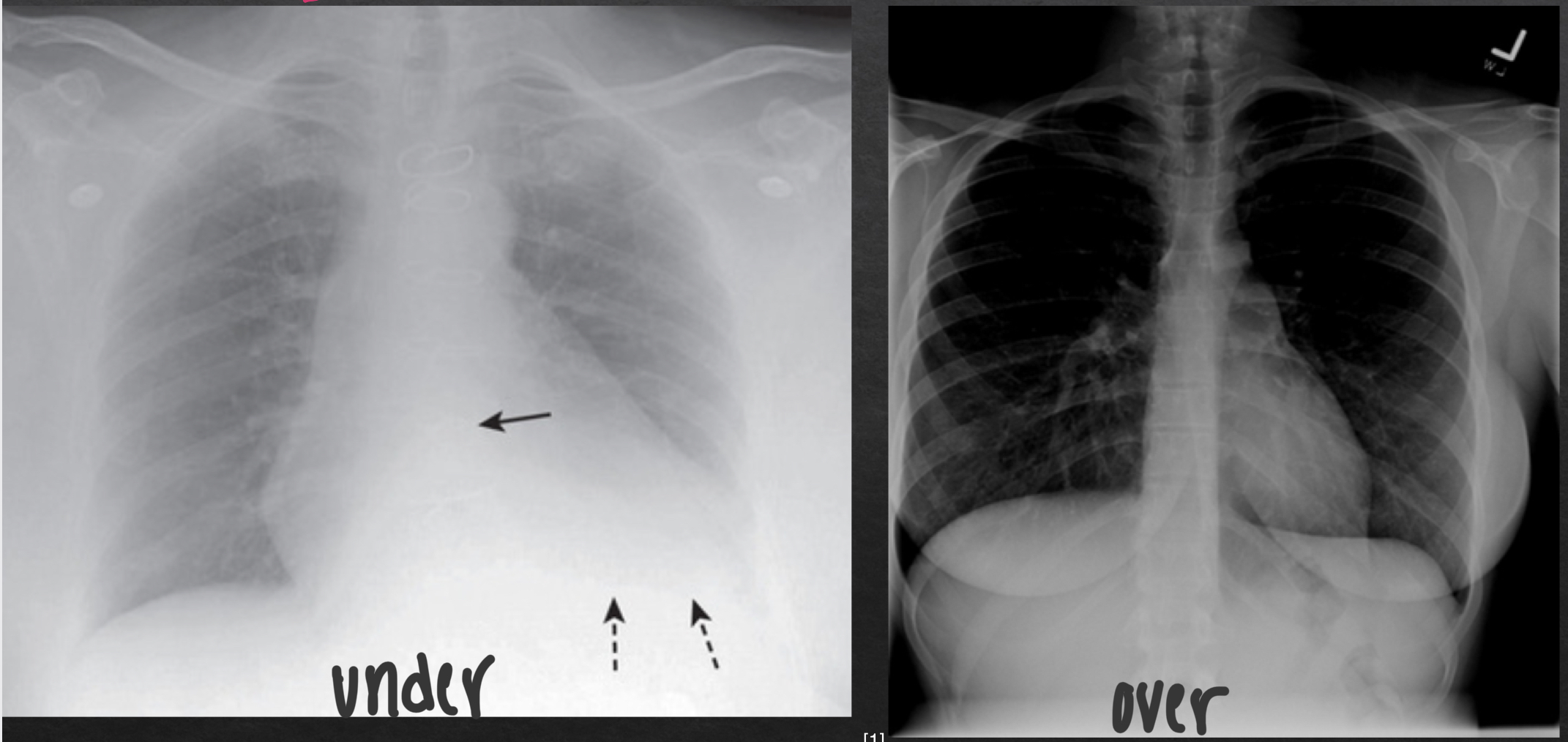
penetration of chest xray
degree to which xrays have passed through the body
adequate penetration:
outline of the thoracic spine visible through heart
inadequate penetration
can mimic or hide disease
underpenetrated vs overpenetrated CXR
inspiration
fills lungs adn contracts diaphragm
10 posterior ribs are visible above diaphragm
8-9 in hospitalized pts
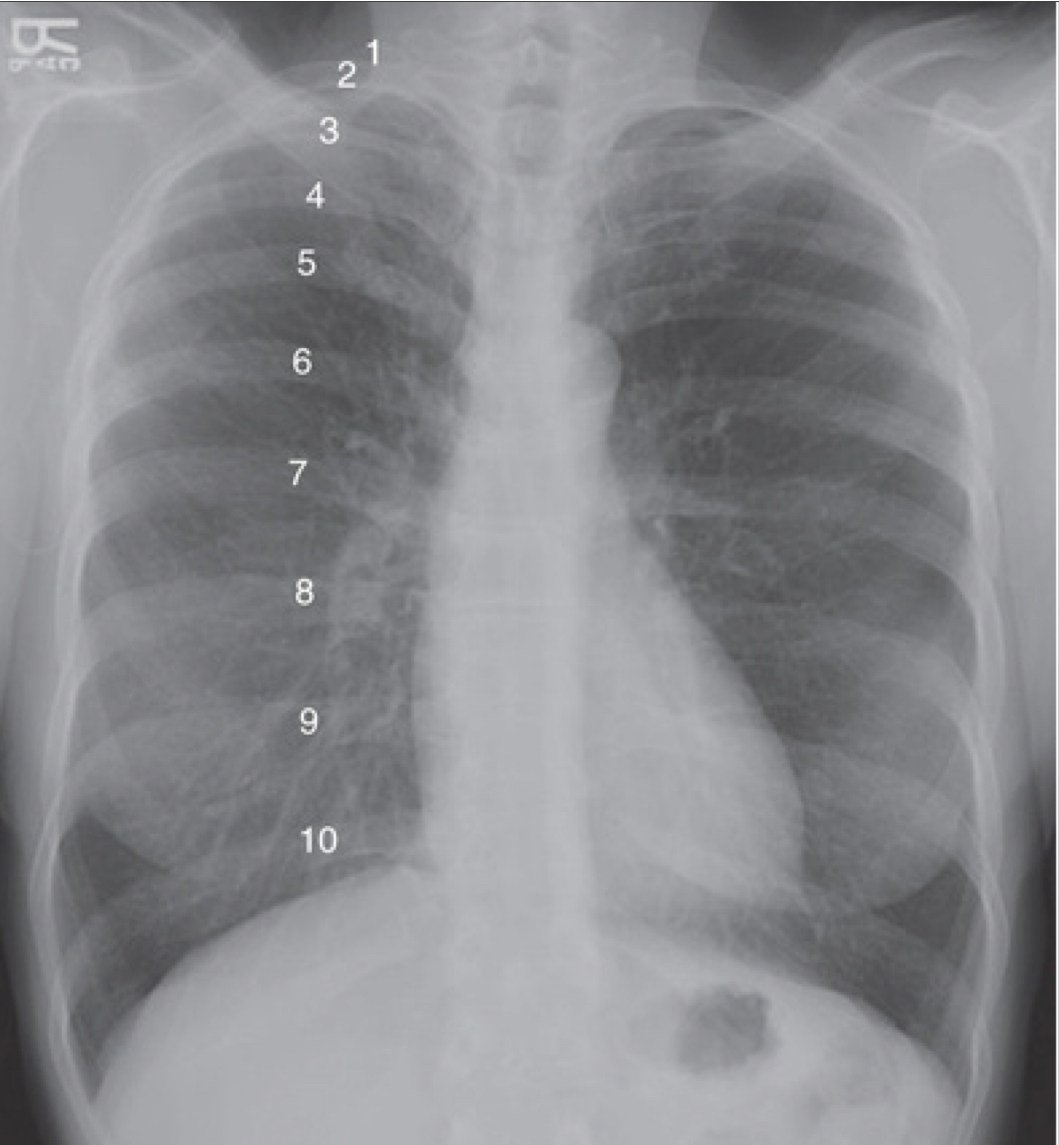
suboptimal inspiration
compress and crowd the lung markings at the llung bases adn diaphram
could be misleading of pneumonia or cardiomegaly
only 7 posterior ribs visible

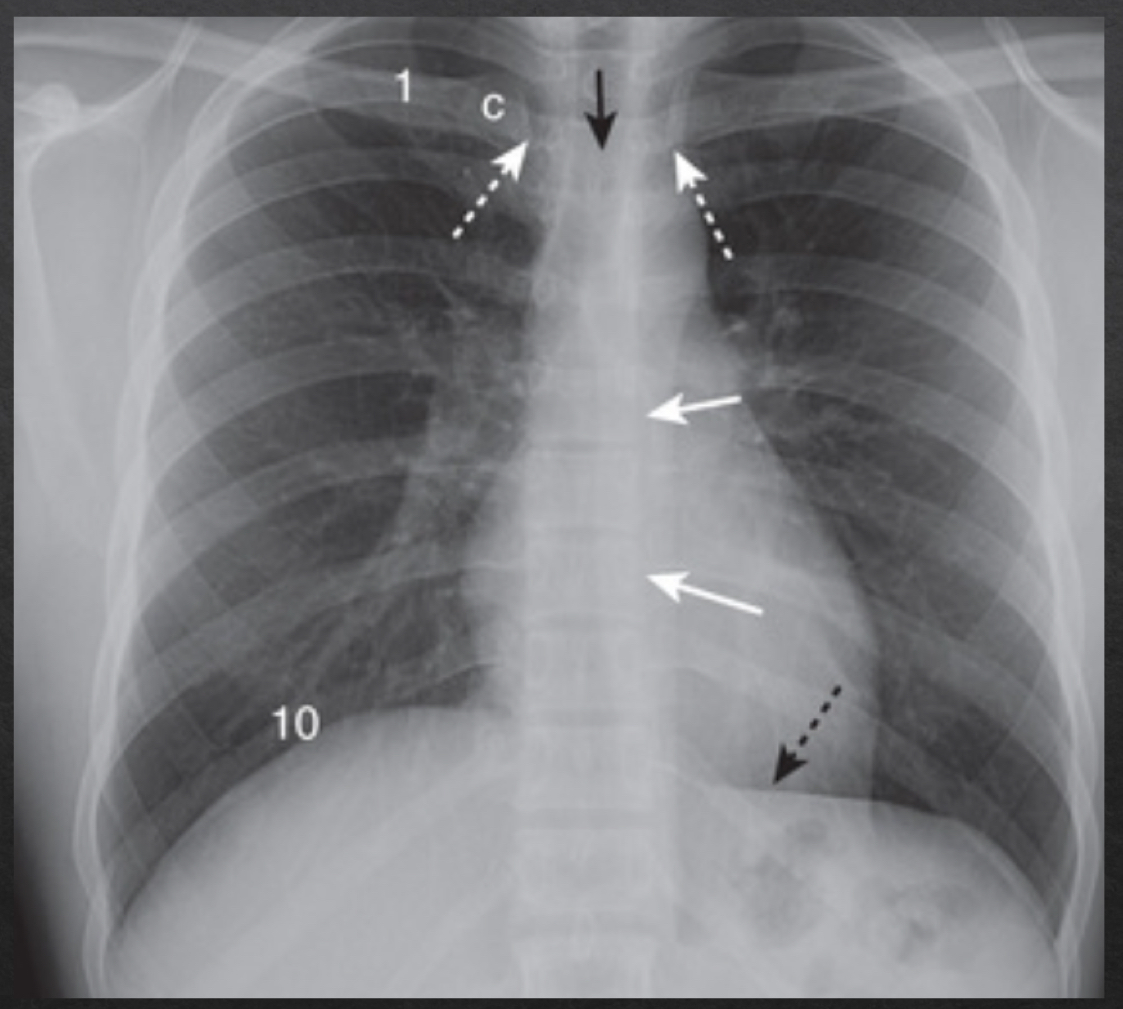
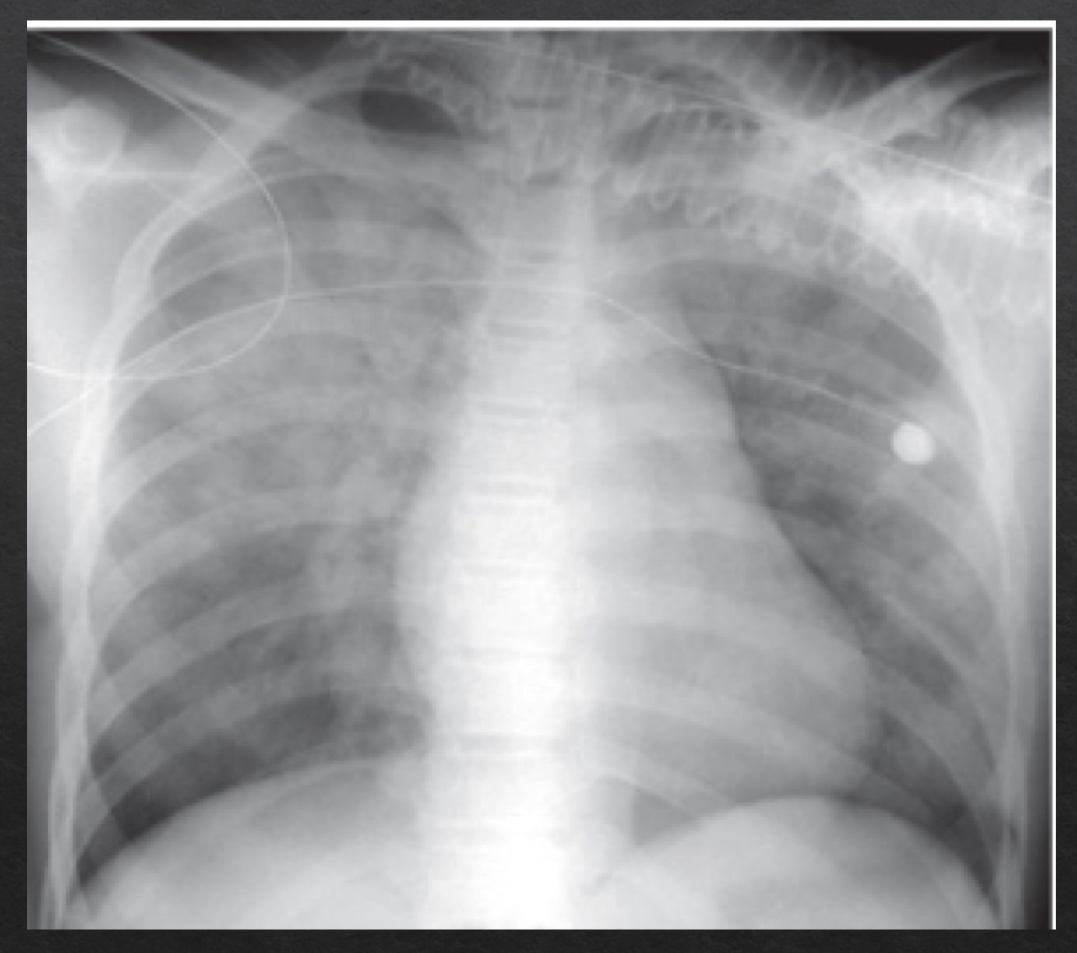
rotation
adequate rotation: spinous processes are equidistant btwn the medial ends of the clavicle
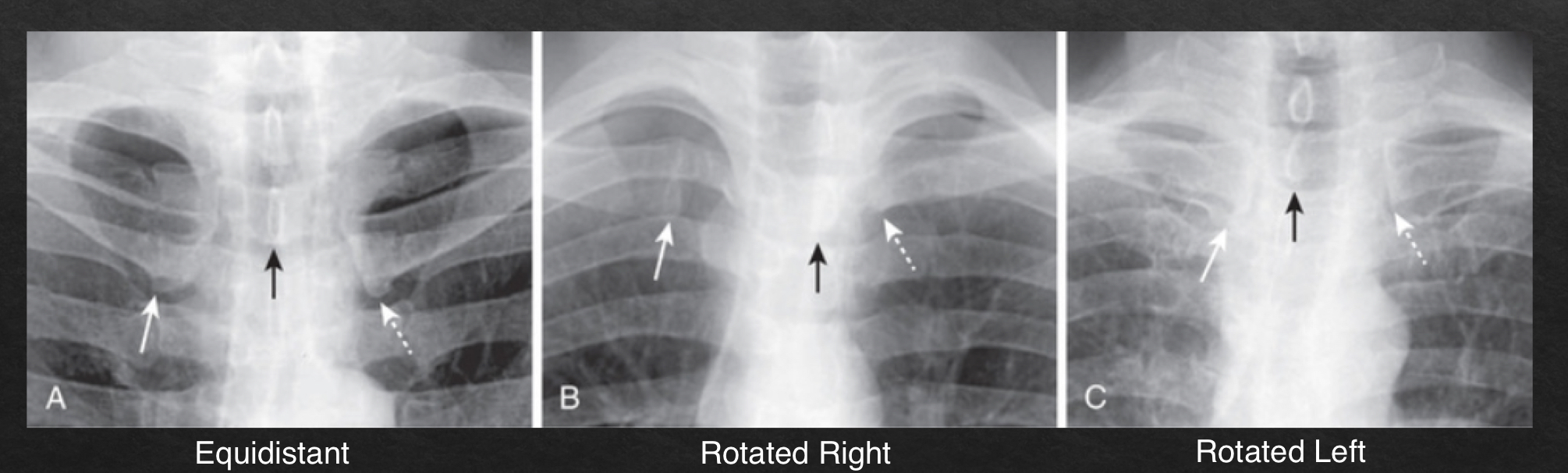
severe rotation findings
trachea appears shifted from midline (black arrow)
left lung appears much larger, right lung appears smaller
heart contour appears changed
left hemidiaphragm appears raised (white arrow)
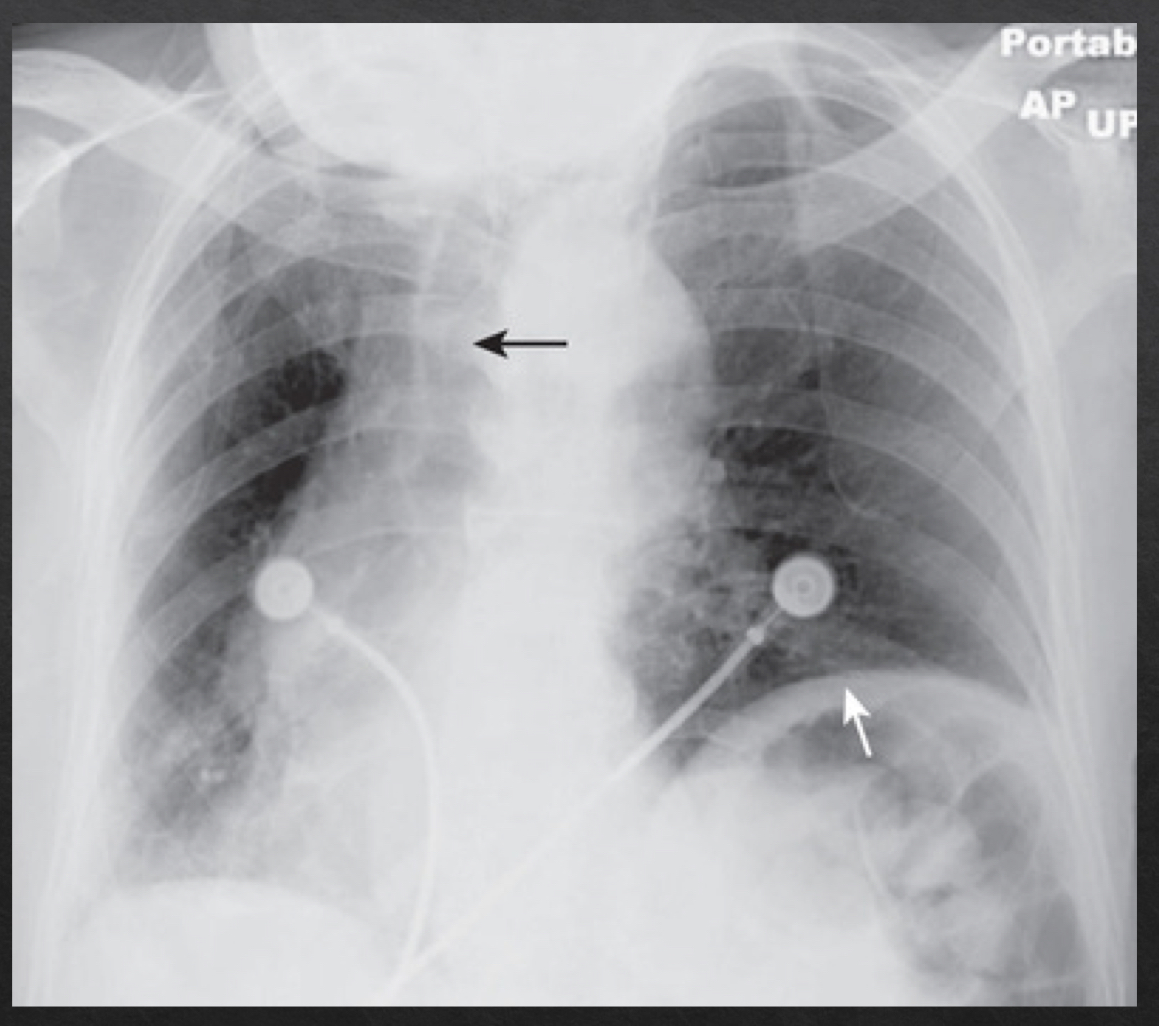
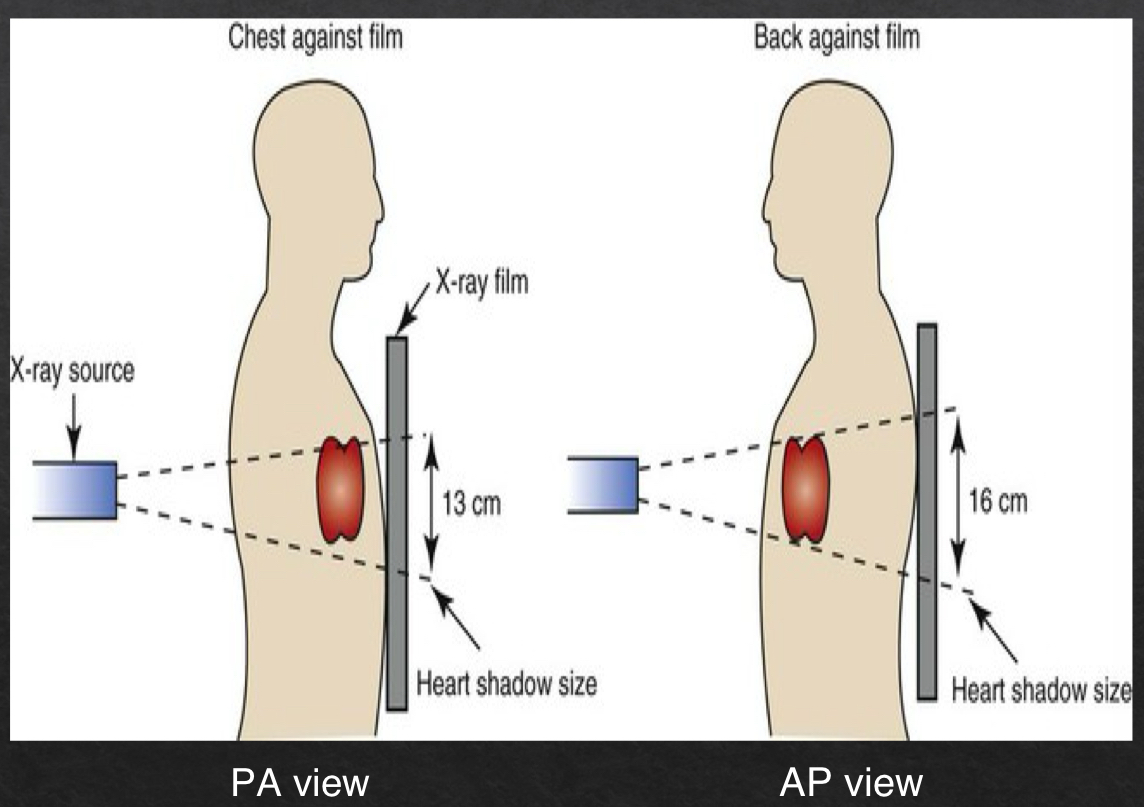
magnification
plays a role in assessing heart size
closer an object is to the surface on which it is being imaged, the more true to actual size the resultant object will be
PA view is more true to size
farther away → more magnified
AP view
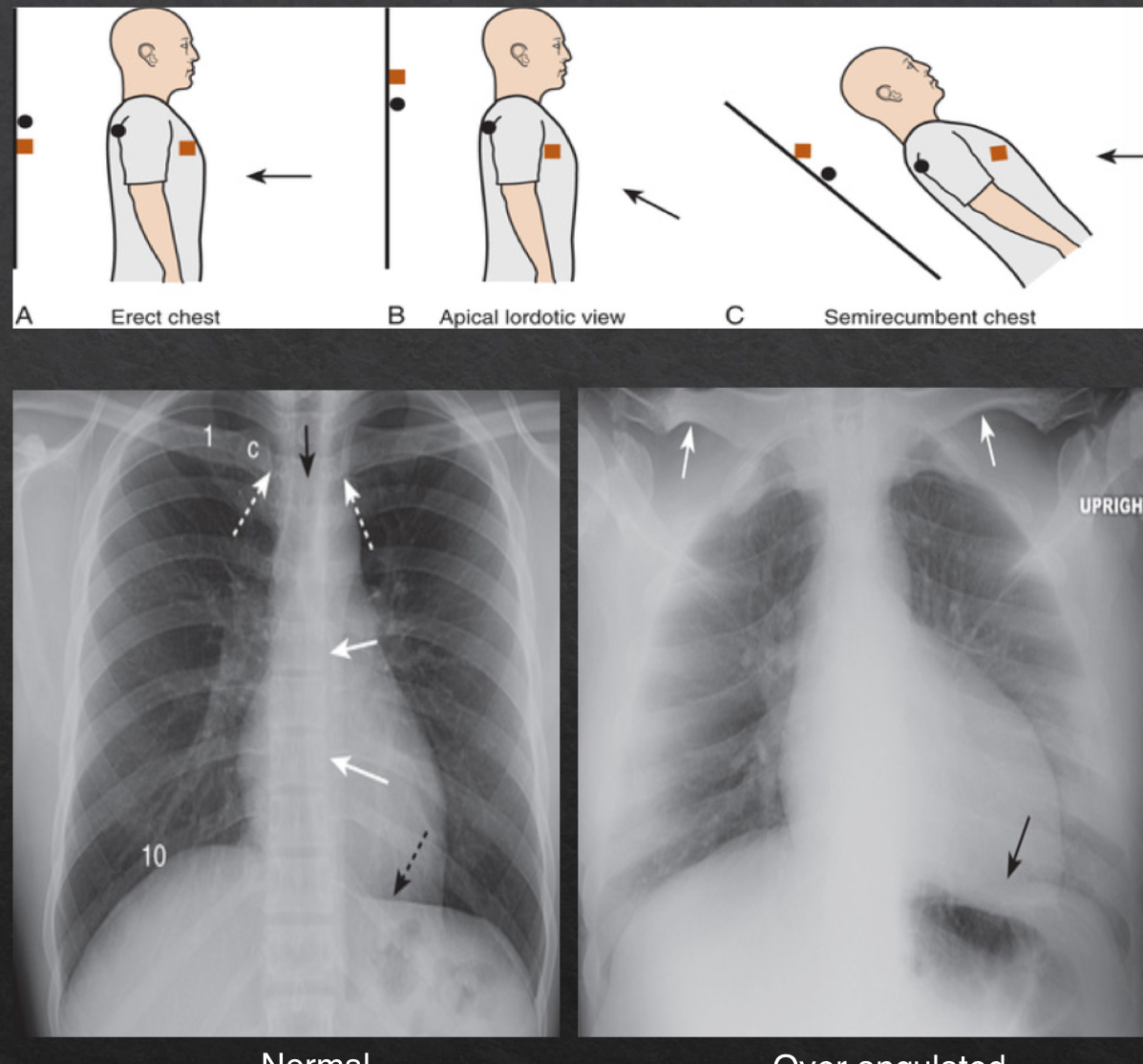
angulation
orientation of xray beam passing through object
views:
horizontal- normal
parallel to floor
medial end of the clavicle superimposes on 3rd or 4th rib
over angulated
bedridden pts that cannto fully sit up
clavicles are projected above first rib
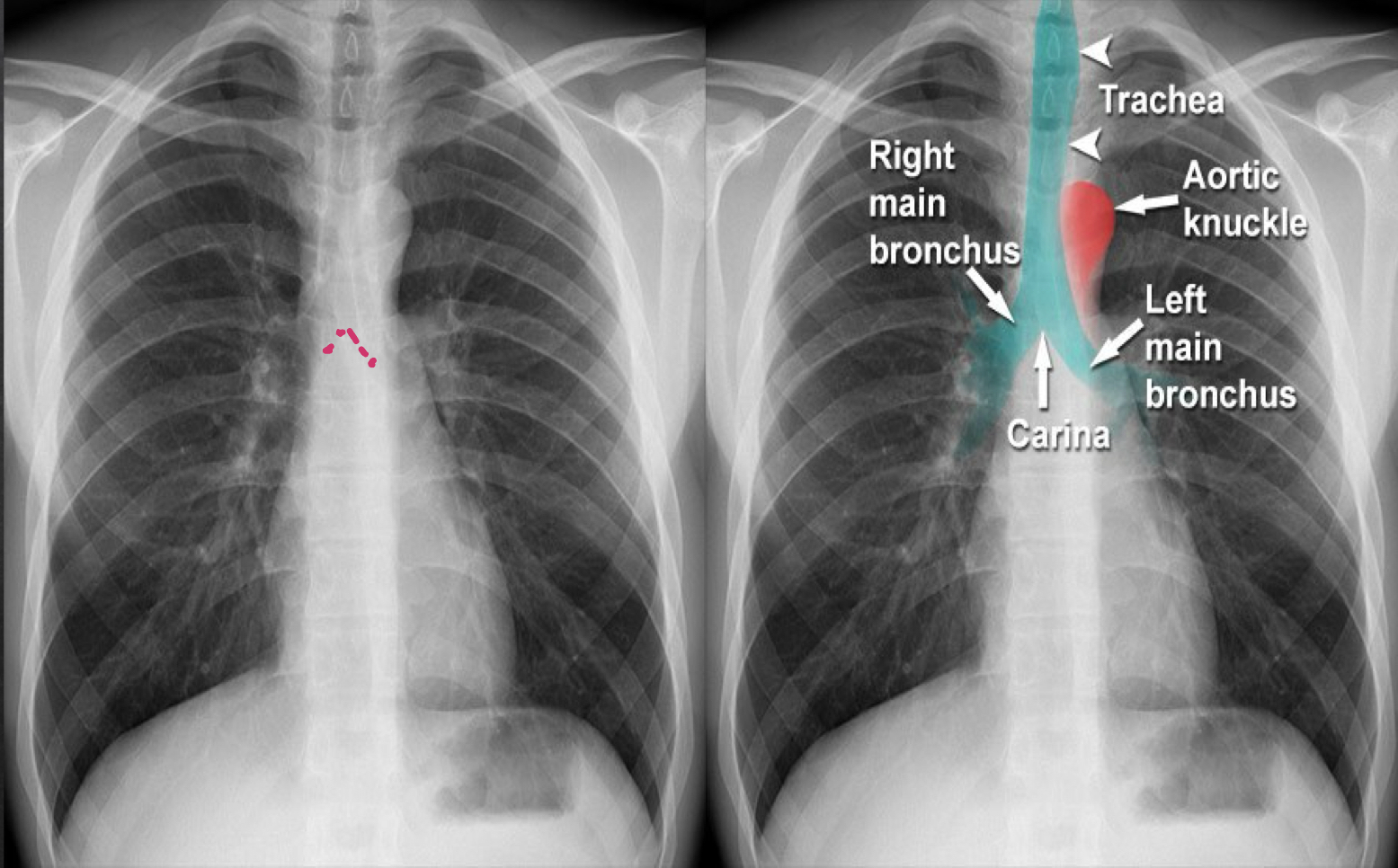
airway (frontal)
trachea: look for deviation other than aortic knob
bronchi: should be visible
carina: should be visible
breathing (frontal view)
lungs
clear lungs fields
appropriate lung markings
fissures/pleura
major and minor fissures should be pencil point thin or not visible
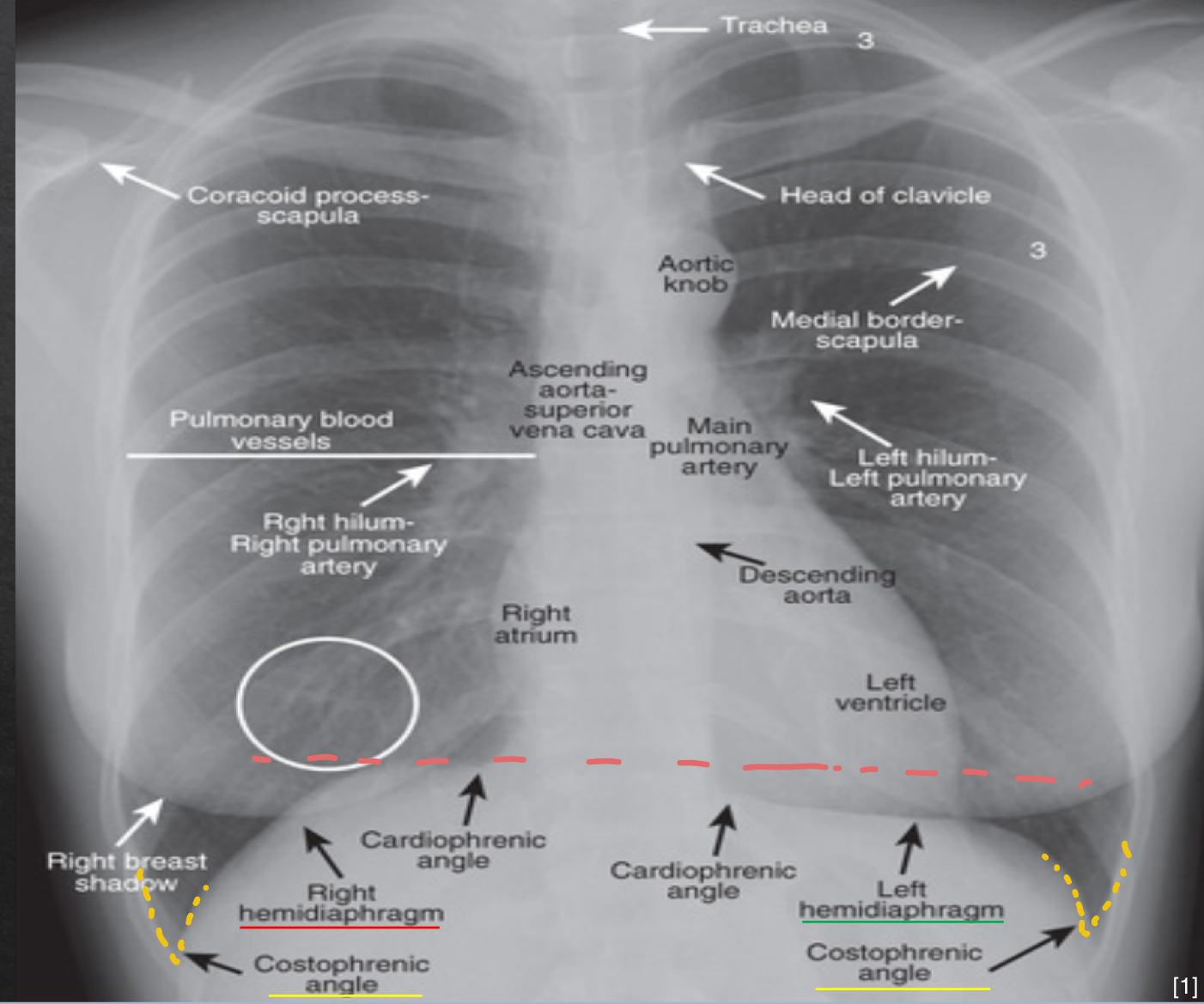
cardio anatomy: frontal view
ascending aorta: shoudl not project more lateral than the RA
aortic knob: will normally push trachea slightly to right
right atria: should project more lateral than ascending aorta
left atria: doe snot contribute to border of heart unless pt is rotated
left ventricle: should not show significant enlargement
descending aorta: parallels spine and barely visible
cardiac: heart size- frontal view
normal: cardiothoracic <50% of internal diameter of thoracic rib cage
AP view → slightly larger than 50% due to magnification
diaphragm: frontal view
right hemi
slightly more elevated
left hemi
no significant elevation
costophrenic angles
sharp
lucency
darker area on the image; more xrays reaching detector
opacity
bright/whiter area on the image; more xrays absorbed, therefore less reaching detector
consolidation
complete filling of alveolar air spaces with fluid, pus, blood, cells, or other material
infiltrate
nonspecific radiologic term describing any abnormal opacity
air bronchogram
visibility of air in bronchus due to surrounding airspace disease
silhouette sign
loss of visible edge that occurs when two objects of the same radiographic density (water and soft tissue) touch each other
airspace disease vs interstitial disease
airspace: disease in the thin walled alveoli
fills alveolar space
interstitial (infiltrative) disease: interstitium
btwm alveoli and blood vessel
contains lymphatic vessels, fibroblasts, adn ECM proteins
thickens walls btwn air spaces
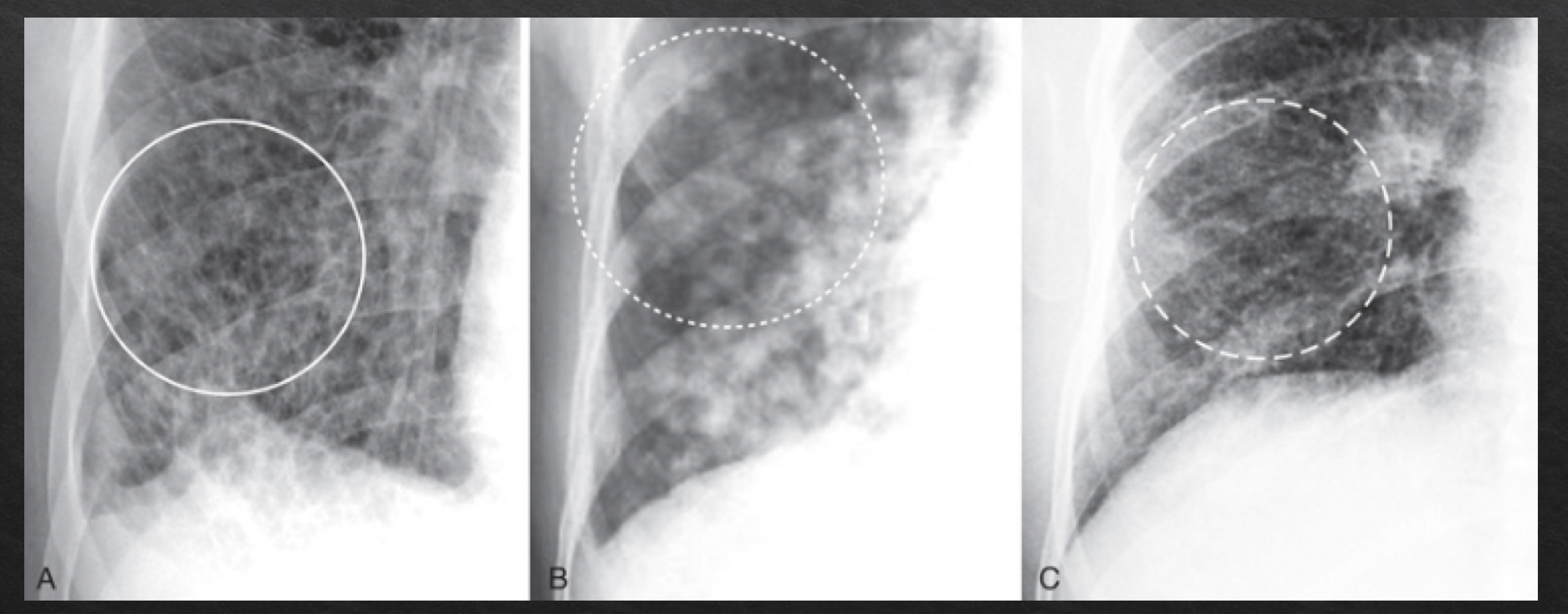
airspace disease
fluffy, cloud-like, hazy opacities
indistinct margins that blend together
may contain air bronchograms
fluid has replaced the air normally surrounding the bronchus, trapping air inside and givngit contrast to be visible
may demonstrate silhouette sign
interstitial disease
criss cross pattern
reticular- lines
nodular- dots
reticulonodular- lines and dots
margins- sharper and discrete
radiographic characteristics: pneumonia
opacities
alveoli (airspace disease)
interstitial pneumonia- walls btwn air spaces become opaque
air bronchograms may be present- air trappe din bronchi that cant escape
clearing/resolution: typically occurs in <10days
pneumoccocal pneumonia may clea within 48 hrs