En of sem 2026 MID2102
1/100
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
101 Terms
Hepatic changes in pregnancy
Decreased tone and mobility
tendency to retain bile salts
increased glycogen storage
altered production of liver enzymes
enlarging uterus that places pressure on gall bladder
Lupus and pregnancy
Infertility can result from SLE's regimen
Women with serious SLE should be counseled against pregnancy (decreased platelets and WBCs increase risks)
risks - stillbirth, IUGR, PTB, neonatal lupus, PET, thormbosis
Multidisciplinary team rheumatologist
Recommendation for postdates
IOL at 41 weeks
OR
Monitoring: CTG, amniotic fluid, Biophysical profile (NST, US assessment of FM, tone, breathing and quantification of amniotic fluid)
Diagnosis of hypertension in pregnancy
Systolic BP ≥ 140 and or diastolic BP ≥90
Severe - Systolic BP ≥160 and/or diastolic BP ≥110
≥170 sBP with or without 110 dBP is a medical emergency
Diagnosis of Chronic hypertension
Preconception or prior to 20 weeks
either with no cause (primary) or associated with an underlying condition
Diagnosis of white coat hypertension
elevated BP in a clinical setting & a normal BP at other times
earlier than 20 weeks
Diagnosis of masked hypertension
Normal BP in a clinical setting and an elevated BP at other times
Diagnosis of gestational hypertension
New onset after 20 weeks without features of pre-eclampsia
Diagnosis of preeclampsia
Hypertension and involvement of one or more other organ systems and/or the fetus
Diagnosis of transient gestational hypertension
Hypertension that is detected in the clinical setting but settles after repeated readings
Diagnosis of superimposed preeclampsia
features of preeclampsia superimposed on either pre-existing hypertension or renal disease
Hypertension risks
Postpartum hemorrhage
Cerebral injury
placental abruption
heart attack or stroke
low birth weight
fetal death
preterm birth
Respiratory distress
Management of hypertension in pregnancy
Control BP - antihypertensives (Labetalol, nifedipine)
Urinalysis
more USS
Delivery - mode determined by obstetric indications
Postpartum - BP may be unstable & require additional therapy
Monitor for the development of PET
organ involvement and symptom in Preeclampsia
Renal - proteinuria
Liver - NV
Neurological - Blurred visoin headaches
Haematological - low platelets
Pulmonary oedema
features of placental dysfunction- IUGR
maternal complications of preeclampsia
placenta abruption
organ damage
haemostatic disorder & major haemorrhage
Stroke or cerebral bleeding
seizures
death
CVD later in life
Fetal complications of preeclampsia
low birth weight
preterm birth
death
CVD later in life
Cause of preeclampsia - Stage 1
Abnormal placentation & trophoblast invasion into maternal vessels
Abnormal spiral artery remodelling (they are either too small or blocked which caused placental hypoxia and oxidative stress)
Cause of preeclampsia - Stage 2 Hypertension
Increased response to vasoactive substances (Angiotensin Il )
Reduced production of endothelial vasodilators eg prostacyclin, NO,
EDRF production
Release of procoagulants, mitogens, vasoconstrictors
Increased levels of markers of endothelial cell injury
Fibronectin, Factor Vlll antigen, thrombomodulin
Cause of preeclampsia - Stage 2 systemic inflammatory response
Activation of neutrophiles, monocytes, lymphocytes
Increase TN\- a, 116, IL8
Metabolic adaptations associated with systemic inflammatory response include acute phase response, oxidative stress, hyperlipidaemia, insulin resistance
Asprin for preeclampsia
150mg, prior to 16 weeks, preventative for preeclampsia
Drugs to avoid in preeclampsia
Diuretics
NSAIDS
ACEI/ARB
HELLP syndrome
hemolysis, elevated liver enzymes, low platelets
VARIANT OF SEVERE PRE-ECLAMPSIA
Magnesium sulfate may be indicated
risk factors for preeclampsia
First pregnancy
Previous PE
>10 years since last baby
Maternal age >40 years old
Body mass index >35 kg/m2
Family sister of PE (mother or sister)
Multiple pregnancy
Underlying medical conditions: pre-existing hypertension, renal disease or diabetes
Presence of antiphospholipid antibodies
Renal system
Includes the kidneys, bladder, ureters and urethras
Responsible for blood filtration and reabsorption of required substances and elimination of wastes through urine. BP regulation
renal changes in pregnancy
Kidney size increases.
GFR, renal plasma flow, Cr clearance increase. Ureters elongated, displaced, and compressed by uterus.
Decreased bladder capacity. (INcreased urination)
Increased UTI susceptibility
UTI in pregnancy
Can be asymptomatic or symptomatic
Can become more serious pyelonephritis
Increased risk for preterm birth
Chronic kidney disease in pregnancy
Can worsen Kidney damage/ reduced renal function
Risks of preterm birth, IUGR, preeclampsia, deteriorating renal function
multidisciplinary care
Monitor fetal growth, hypertensions, regular kidney function tests
GI changes in pregnancy
Gums appear red/swollen and bleed easier caused by elevated estrogen levels,
nausea/vomiting, constipation, reflux, diarrhea common in pregnancy
Hormones cause smooth muscle relaxtion, reducing motility and gatsic emptying
increases appetite
more absorption of essiential nutrients
Reflux GERD in pregnancy
stomach acid or bile irritates the food pipe lining
very common especially later in gestation
heartburn caused by reduced tone of esophageal sphincter caused by progesterone
Nausea and vomiting in pregnancy
•80-85% experience nausea and vomiting in first 12 weeks
stomach has decreased tone and motility
delayed gastric emptying
Advice for NVP
•Eat frequent small meals a day that include carbohydrate
•Avoid fatty and spicy foods
•Drink plenty of fluids
•Ginger can offer some relief
Metoclopramide, ondansetron, doxylamine etc if needed
hyperemesis gravidarum
severe nausea and vomiting in pregnancy that can cause severe dehydration in the mother and fetus
Can cause dehydration and malnutrition
IV treatment of fluids may be needed
•1% experience severe nausea
Continues past 20 weeks
Intrahepatic cholestasis of pregnancy
Most common liver disease of pregnancy
marked pruritis
elevated total bile acids and or LFTs
Stasis of bile acids in teh gall bladder,
Treatment for ICP
Ursodeoxycholic acid (UDCA) Provides cytoprotection against the hepatotoxic effects of the hydrophobic bile acids and improves hepatobiliary bile acid transport
ICP birth outcomes
associated with increased rates of preterm birth, meconium-stained amniotic fluid, RDS, prolonged admission to the neonatal unit, and stillbirth
Treatment for GERD
-Lifestyle changes → small frequent meals, eat upright, eat slowly, avoid spicy/v acidic foods Antacids -Acid lowering drugs → H2 blockers, PPI, antacids Further investigations
Haematological changes in pregnancy
Increased blood volume, Red cell mass, white blood cells
Physiological anemia (Dilution affect)
increased iron and folate requirements
hypercoagulable state
Anemia
a deficiency of red blood cells
causes for anemia
-blood loss
-decreased production of RBCs or haemoglobin
-destruction of RBCs
Iron deficiency
Thrombocytopenia
low platelet count
can be gestational
just keep a close eye on levels before birth
Autoimmune disorders in pregnancy
Might decrease symptoms in pregnancy due to anti-inflammatory state
Monitor symptoms, continue usual treatment
systemic lupus erythematosus
chronic autoimmune inflammatory disease of collagen in skin, joints, and internal organs
term pregnancy
pregnancy from 37 weeks to 42 weeks
prolonged pregnancy
over 42 weeks
Prolonged Pregnancy Risks
-Placenta ages - delivering oxygen and nutrients to the fetus less efficiently
-The fetus may lose weight
-stillbirth
-Meconium may be expelled and aspirated
-Low blood glucose levels in the fetus
- >4000g birth weight
PPH
Normal gestation of birth multips
50% by 40+3
75% by 41
Ways to stimulate labor
•upright position (gravity helps)
•Intercourse
•nipple stimulation
walking
how does spontaneous labour start
Prostaglandins and oxytocin increase at term - more gap junctions too. Ca crosses gap junctions causing coordinated uterine contraction
CRH increases estrogen and cortisol causing more receptors in teh uterus for P and O
Increase in estrogen in relation to progesterone also helps initiate labour
Induction of labour
Is the planned initiation of labor prior to the onset of spontaneous labor
induction of labor indications
Fetal compromise (intrauterine growth restriction, Rh incompatibility)
PROM
Post term pregnancy
Infection
GDM, preelcmapsia
Hypertension associated with pregnancy
Maternal medical conditions
Fetal death
risks of induction of labour
- Operative birth
- Tachysystole
- Chorioamnionitis
- Cord prolapse
- PPH
- Failed induction
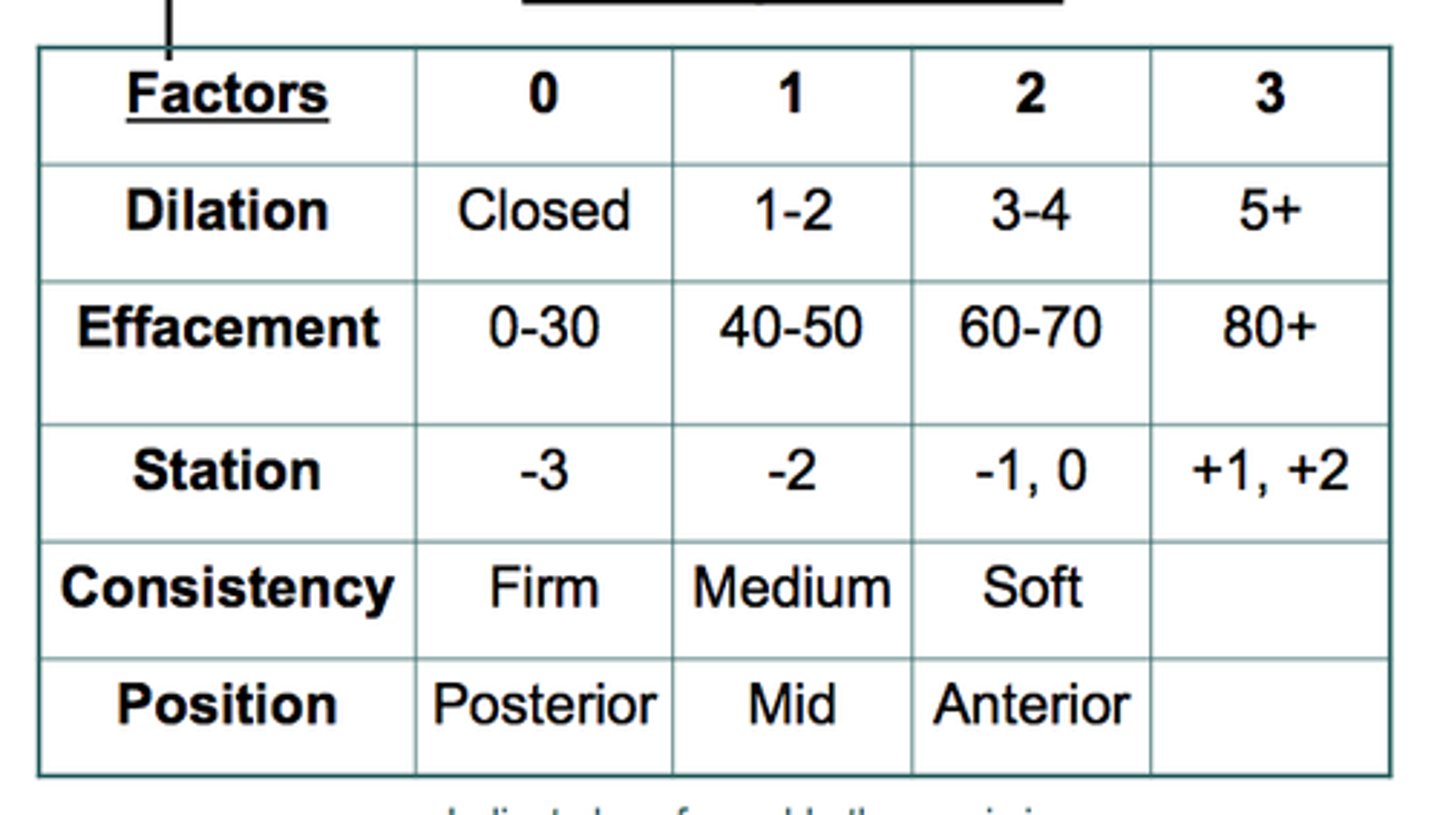
Bishop score
Determines maternal readiness for labor by evaluating whether the cervix is favorable by rating cervical dilation, effacement, consistency, position, and station
cervical ripening methods
- chemical agents (prostaglandins)
- mechanical and physical methods (Balloon)
Prostaglandin Gel
softens the cervix when applied before labor induction; woman is placed on bed rest for 1-2 hours and monitored for uterine contractions
Midwives Role in CVD in pregnancy
Primary clinician across the continuum of pregnancy care
Discuss symptoms
Facilitate risk assessment, detection, referral and consultation
Collaborate with multidisciplinary colleagues caring for high-risk women in pregnancy
Normal Cardiorespiratory Changes in Pregnancy
BP falls 10 mmHg by 20/40 and then returns to baseline T3
Pulse rate increases by 10-20 BPM and can be bounding or collapsing — average HR 91 BPM at 34 weeks ( Range 68-115)
Peripheral oedema
Cardiac output increases 50%
Blood volume increases by 50%, plamsa 100ml, 500 RBC
ECG changes: 15-20 degree left axis deviation, Transient ST segment and T wave changes, Q wave (small) and inverted T wave lead Ill
attenuated Q wave in AVF, Inverted T wave in VI, V2 and occasionally V3 and SVT and ventricular extrasystoles are common.
Haemodynamic changes related to labour and delivery
Cardiac output increases
BP increases during each contraction
Uterine blood flow 700mls/min at term
How much does CO increase in labour and then postpartum
15% early labour; 25% active phase; 50% pushing
Immediately postpartum CO increases up to 80% - due to auto transfusion 500ml blood from uterine involution and Release of IVC compression from uterus
By how much does BP increase in labour
Systolic 10-15% Diastolic 10-15%
how does supine body position influence the cardiovascular system in pregnancy
2nd & 3rd trimester uterus compresses the Inferior Vena Cava(lVC) & reduces venous return
Results in decreased CO and increased HR compared to lateral position
Can cause maternal hypotension
Associated increased HR, decreased pulse pressure & symptoms of autonomic
activation
May result in reduced placental perfusion with no reassuring CTG
Signs and symptoms of normal pregnancy mimic cardiorespiratory disease
Shortness of Breath
Palpitations
Peripheral oedema
Dizziness
Easy fatigability, decreased exercise capacity
Increased heart rate
Why does looking an amniotic fluid help monitor health of baby
With diminished placental function selective perfusion of the brain and heart and reduced perfusion of other systems including the kidneys takes place
Reducing fetal urine
Dating pregnancies
Naegle's Rule
USS dating scan 10-13 weeks
Have a margin of error and can be a few days off
Naegele's Rule
add 7 days to LMP, subtract 3 months, add 1 year
Normal gestation of birth Primparous
50% by 40+5
75% by 41+2
balloon catheter
silicone double-balloon catheter used for mechanical dilation of the cervical canal prior to labor induction
artificial rupture of membranes ARM
Bag of waters is broken using a hooked instrument in an attempt to induce or speed up labor. This is often carried out in conjunction with a drip of a synthetic hormone (SYNTOCININ) into the arm to stimulate contractions.
Syntocinon infusion for induction
Synthetic oxytocin that causes uterine contractions
Start at 1ml/h, 2, 4, 8, 12ml/hr
CTG monitoring needed
30 unites in 500ml
Trauma
emotional or physical response to a life-threatening or harmful event or circumstances, with lasting adverse affects
Birth trauma
ANY FORM OF TRAUMA THAT HAS OCCURED AS A RESULT OF A BIRTH EXPERIENCE
Believes her baby or herself is in danger
Depends on how a woman perceives her birth
Feel helpless, out of control, abandoned, disrespected
How does birth trauma PTSD manifest
Nightmares
sleep disturbances
dwelling on experience
avoidance
irritability, hyperarousal
interrupted baby bonding
How to interact with a woman with birth trauma
Listen
no judgement
acknowledge feelings
take seriously
Importance of self-care
referral potentially
focus on informed choice and shared decision making
Consent is key
Explaining what recommend care is and what you are doing
"What do you want from me?"
"Thank you for trusting me"
Trauma informed care
an approach to treatment that acknowledges the role that trauma can have on the mental health of individuals
Flexible and focuses on safety, trust, choice, collaboration and empowerment
Edinburgh Postnatal Depression Scale (EPDS)
Screening test used to identify depression during pregnancy or in the postpartum period
Above 13 means referral
EPDS Q10
Harm/suicide
I see you have ticked yes for Q10 Can you tell me more about this?
Importance of documentation
Documented treatment and safety plan and thoughts about required care
anxiety
The condition of feeling stressed or worried about what may happen more than the average person
Stress
the body's reaction to any type of perceived threat
Stress biochemical
Triggers SNS and adrenal line and cortisol release
this increases HR, RR, muscle contract and mind sharpens
stress and anxiety effect on unborn baby
SGA
PTB
LBW
negative birth experiences (Birth trauma)
exacerbate placental issues
affect babys brain devlopment
Identify risks of mental health decline
Warning signs
Psychosocial stressors
Mental state exam
See how changes over pregnancy
baby blues
Mild depressive symptoms, anxiety irritability, mood swings, tearfulness, increased sensitivity, fatigue
Usually peak at days 4 and 5 and resolve by day 10
80% of mother experience
Postpartum Depression
a mood disorder characterized by feelings of sadness and the loss of pleasure in normal activities that can occur within a year after giving birth. lasts longer than 2 weeks
Postpartum Depression symptoms
Fatigue
Irritability
Loss of appetite
Sleep disturbances
Low mood
withdrawal
Concern about inability to care for infant
Bipolar
A mood disorder in which the person alternates between the hopelessness and lethargy of depression and the overexcited state of mania.
Can get worse in pregnancy and postpartum
medications might be changed
Schizophrenia
a psychological disorder characterized by delusions, hallucinations, disorganized speech, and/or diminished, inappropriate emotional expression.
Increased risk of postpartum psychosis
What third stage uteronic for those with hypertension
syntocinin
not syntometrine or ergometrine
Magnesium sulfate for preelcmapsia
anticonvulsant 4g loading, 1g maintenance
What are predisposing factors to Post Traumatic Stress Disorder (PTSD) following Birth Trauma?
Having prior trauma
prior PTSD
fear of birth
history of psychiatric disorders
Anxiety
What are precipitating factors to Post Traumatic Stress Disorder (PTSD) following Birth Trauma?
Instrumental/ operative birth
long labour
out of control
extensive blood loss
Negative neonatal outcomes
Subjective
Four sub themes to the perfect storm of trauma
Bring the baggage to birth - preexisting health
trauma by 1000 cuts - accumulation of negative experiences
Thrown in the pressure cooker - lack of sleep, parenting, trauma, recovery
trying to work it out - healing, seeking support, reflection, validation
Midwives role
debriefing
infomed choice
building trusting relationships
supportive
idneity risk factors
recognise trauma coming - hey this is whats heppening, lets focus on this thing right ot
taking symptoms seriouly
sleep, excersie
BF - help with bonding
Antiphospholipid syndrome
Blood becomes sticky
Low does aspirin, multidisciplinary team, clexane
risks
miscarriage, pre-eclampsia, placental abruption, IUGR, PTB
Asymptomatic UTI
Increases low birthweight
Mid stream urine sample recommended in ecah trimester
Increased risk if you have Hx of recurrent UTI, diabetes or an abnormal urinary tract
5 day antibiotic course
Symptomatic UTI
ant biotic, discoloured, cloudy urine, temperature
oral antibiotic therapy
severe cases - IVABS
Diagnosed by MSU
Acute pyelonephritis
INfection of ranal pelvis that can spred into kidney tissue
Symptoms - UTI, backache, tenderness, fatigue, fever, malise, rigors, NV, dehydration,
Complications of Acute pyelonephritis
Endotoxic shock
chronic renal infection
renal failure
IUGR
Preterm birth
Managemenet of Acute pyelonephritis
MSU
blood specimen
IV fluids'
IVABS
real function tests
OBS
Management of preelcmpsia
Urinalysis regularly
USS and CTG twice weekly
early delivery
Fluid management in birth - Catheter
MgSO4 if signs of eclampsia (Central nervous dysfunction)
Eclampsia