Shoulder Special Test
1/29
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
30 Terms
Yergason test
PURPOSE- Integrity of transverse ligament
DESCRIPTION- Patient sitting with elbow flexed to 90° and stabilized against the thorax and with the forearm pronated. Resist the supination of forearm and external rotation of shoulder
RESULT- Tendon of long head of biceps will pop out of the groove. Tenderness in the bicipital groove alone without the dislocation may indicate bicipital paratenonitis/tendinosis
Speeds Test
PURPOSE- Identify bicipital tendinosis/ tendinopathy
DESCRIPTION- Upper limb in full extension and forearm supinated, resist shoulder flexion. Alternate – place shoulder in 90 degree flexion and push upper limb into extension
RESULT- Pain in long head of biceps tendon/ increased tenderness in the bicipital groove

Neers Impingement Test
PURPOSE- For impingement of supraspinatus and biceps tendon
DESCRIPTION- The patient’s arm is passively and forcibly fully elevated in the scapular plane with the arm medially rotated by the examiner. This passive stress causes the greater tuberosity to jam against the anteroinferior border of the acromio
RESULT- Reproduces symptoms of pain in the shoulder region

Empty Can/Jobe Test
PURPOSE- Identify tear/ impingement of supraspinatus tendon or suprascapular nerve neuropathy
DESCRIPTION- The patient’s arm is abducted to 90° with neutral (no) rotation, and the examiner provides resistance to abduction. The shoulder is then medially rotated and angled forward 30° (“empty can” position) so that the patient’s thumbs point toward the floor in the plane of the scapula. Differentiate if pain is present between two positions
RESULT- Reproduces pain in supraspinatus tendon or weakness in empty can position

Drop Arm Test
PURPOSE- Also known as Codman’s test. Identify tear/ full rupture of rotator cuff
DESCRIPTION- The examiner abducts the patient’s shoulder to 90° and then asks the patient to slowly lower the arm to the side in the same arc of movement
RESULT- A positive test is indicated if the patient is unable to return the arm to the side slowly or has severe pain when attempting to do so
Posterior Internal Impingement Test
PURPOSE- To identify impingement between rotator
cuff and greater tuberosity or posterior glenoid and labrumDESCRIPTION- The patient is placed in the supine lying position. The examiner passively abducts the shoulder to 90° to 110°, with 15° to 20° extension and maximum lateral rotation
RESULT- Reproduction of pain in posterior shoulder during test

Hawkin-Kennedy Impingement Test
PURPOSE: Identify sub-acromial impingement
DESCRIPTION: The arm of the patient is passively flexed up to 90 degrees in the
plane of the scapula. The arm is stabilized and the forearm is forced into IR
RESULT: Pain indicates a positive test for supraspinatus paratenonitis/tendinosis or secondary impingement

Yocum
test is a modification of this test in which the patient’s hand is placed on the opposite shoulder and the examiner elevates the elbow. Pain indicates a positive test

Horn Blower Sign (Patte test)
PURPOSE: To detect Rotator cuff tears involving the teres minor
DESCRIPTION: The test is performed with the patient in the sitting or standing position. The patient’s arm is supported at 90 degrees of abduction in the scapular plane, with the elbow flexed to 90 degrees. The patient is then asked to rotate the forearm externally against the resistance of the clinician’s hand.
RESULT: . If the patient is unable to externally rotate the shoulder in this position, the horn-blower’s sign is said to be present

Active Compression Test of O’Brien
PURPOSE: To detect SLAP (Type II) or superior labral lesions
DESCRIPTION: Two-part test. The patient stands with his or her involved shoulder at 90 degrees of flexion, 10 degrees of horizontal adduction, and maximum IR with the elbow in extension. In this position, the patient then resists a downward force applied by the clinician to the distal arm. The test is then repeated in the same manner except that the arm is positioned in maximum ER.
RESULT: If pain on the joint line or painful clicking is produced inside the shoulder (not over the acromioclavicular joint) in the first part of the test and eliminated or decreased in the second part, the test is considered positive for labral abnormalities.

Bicep Load Test
PURPOSE: To check the integrity of the superior labrum.
DESCRIPTION: The patient is supine or seated with the shoulder abducted to 120° and laterally rotated with the elbow flexed to 90° and the forearm supinated. The examiner performs an apprehension test on the patient by taking the arm into full lateral rotation. If apprehension appears, the examiner stops lateral rotation and holds the position. The patient is then asked to flex the elbow against the examiner’s resistance at the wrist.
RESULT: If apprehension decreases or the patient feels more comfortable, the test is negative for a SLAP lesion. If the apprehension remains the same or the shoulder becomes more painful, the test is considered positive for SLAP lesions

Clunk Test
PURPOSE- Identifies glenoid labrum tear
DESCRIPTION- Patient is supine, with shoulder in full abduction. Push humeral head anteriorly, while rotating humerus externally
RESULT- Audible clunk is heard while performing test

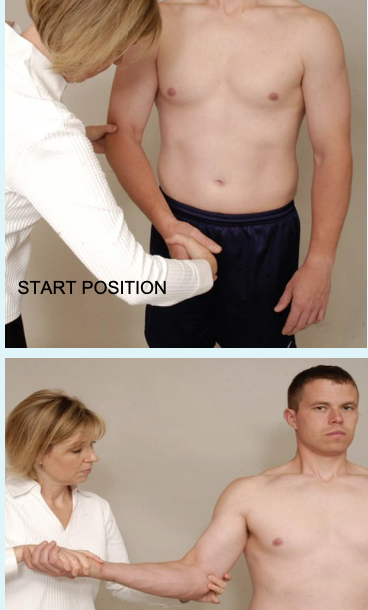
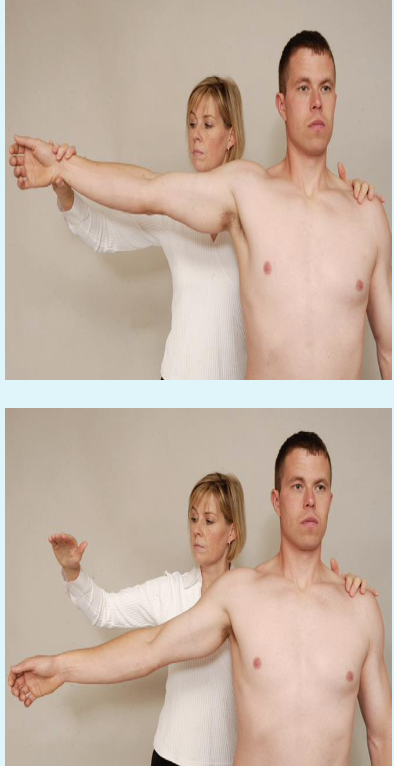
Lateral Rotation Lag Sign
PURPOSE: To test the teres minor and infraspinatus. Also known as Infraspinatus “Spring Back” Test.
DESCRIPTION: The patient is seated or in standing position with the arm by the side and the elbow flexed to 90°. The examiner passively abducts the arm to 90° in the scapular plane, laterally rotates the shoulder to end range and asks the patient to hold it
RESULT: For a positive test, the patient cannot hold the position and the hand springs back anteriorly toward midline, indicating infraspinatus and teres minor cannot hold the position due to weakness or
pain

Abdominal Compression Test
PURPOSE: Checks the subscapularis muscle. Also k/a Belly-Press or Napoleon Test
DESCRIPTION: The patient is standing, examiner places a hand on the abdomen below the xiphoid process so that the examiner can feel how much pressure the patient is applying to the abdomen. The patient places his hand of the shoulder being tested on the examiner’s hand and pushes the hand as hard as he can into the stomach (medial shoulder rotation). While pushing the hand into the abdomen, the patient attempts to bring the elbow forward to the scapular plane, causing greater medial shoulder rotation.
RESULT: If the patient is unable to maintain the pressure on the examiner’s hand while moving the elbow forward, or posteriorly flexes the wrist or extends the shoulder, the test is positive for a tear of the subscapularis muscle

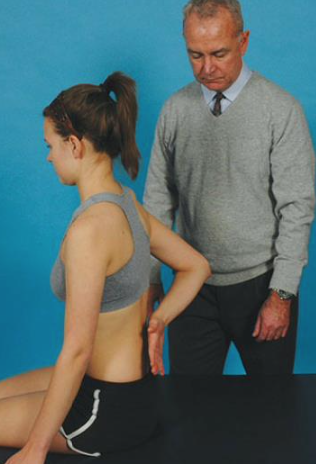
Lift Off Sign (Gerber Test)
PURPOSE- To detect a lesion of the subscapularis muscle
DESCRIPTION- The patient places the dorsum of the hand on his back pocket or against the mid-lumbar spine. (Great subscapularis activity is shown with the second position). The patient then lifts the hand away from the back.
RESULT- An inability to do so indicates a lesion of the subscapularis muscle.
Pectoralis Major Contracture Test
PURPOSE: To identify tightness of pectoralis major muscle
DESCRIPTION: The patient lies supine and clasps the hands together behind the
head. The arms are then lowered until the elbows touch the examining table
RESULT: A positive test occurs if the elbows do not reach the table and indicates a tight pectoralis major muscle.

Jerk Test
PURPOSE: To test recurrent posterior instability
DESCRIPTION: The patient sits with the arm medially rotated and forward flexed to 90°. The examiner grasps the patient’s elbow and axially loads the humerus in a proximal direction. While maintaining the axial loading, the examiner moves the arm horizontally across the body
RESULT: A positive test is the production of a sudden jerk or clunk as the humeral head slides off (subluxes) the back of the glenoid. When
the arm is returned to the original 90° abduction position a second jerk may be felt as the head reduces.

Sulcus Sign
PURPOSE: To test for inferior shoulder instability
DESCRIPTION: The patient stands with the arm by the side and shoulder muscles relaxed. The examiner grasps the patient’s forearm below the elbow and pulls the arm distally
RESULT: The presence of a sulcus sign may indicate inferior instability or glenohumeral laxity but should only be considered positive for instability if the patient is symptomatic

Anterior Apprehension/Crank Test
PURPOSE- Identify past anterior dislocation of shoulder
DESCRIPTION- Patient supine, the examiner abducts the arm to 90° and laterally rotates the patient’s shoulder slowly. By placing a hand under the glenohumeral joint to act as a fulcrum, the apprehension test becomes the fulcrum test
RESULT- Patient does not allow or does not like to move shoulder into that direction to simulate anterior dislocation

Posterior Apprehension Sign
PURPOSE- To identify past history of posterior shoulder dislocation
DESCRIPTION- Patient supine/ sitting. The examiner elevates the patient’s shoulder in the plane of the scapula to 90° while stabilizing the scapula with the
other hand, then applies a posterior force on the patient’s elbow. While applying the axial load, the examiner horizontally adducts and medially rotates the arm.RESULT- RESULT- Patient does not allow or does not like to move shoulder into that direction to simulate posterior dislocation
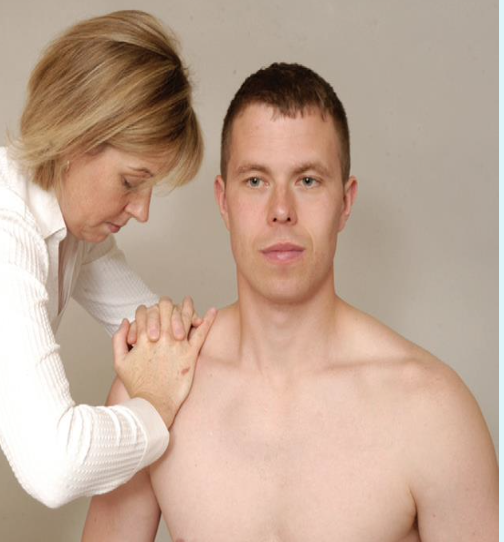
Acromioclavicular Shear Test
PURPOSE- Identifies dysfunction of AC joint such as arthritis, separation
DESCRIPTION- With the patient in the sitting position, the examiner cups his or her hands over the deltoid muscle with one hand on the clavicle and one hand on the spine of the scapula. The examiner then squeezes the heels of the hands together
RESULT- Reproduces pain in AC joint
Halstead Maneuver
PURPOSE: Identify pathology of structures that pass through thoracic inlet
DESCRIPTION: The examiner finds the radial pulse and applies a downward traction on the test extremity while the patient’s neck is hyperextended and the head is rotated to the opposite side
RESULT: Absence or disappearance of a pulse indicates a positive test for thoracic outlet syndrome.

Adson Test
PURPOSE- Identify pathology of structures that pass through thoracic inlet
DESCRIPTION-The examiner locates the radial pulse. The patient’s head is rotated to face the test shoulder. The patient then extends the head while the examiner laterally rotates and extends the patient’s shoulder. The patient is instructed to take a deep breath and hold it.
RESULT- A disappearance of the pulse indicates a positive test.

Costoclavicular Syndrome (Military Brace Test)
PURPOSE- Identify pathology of structures that pass through thoracic inlet
DESCRIPTION-The examiner palpates the radial pulse and then draws the patient’s shoulder down and back
RESULT- A positive test is indicated by an absence of the pulse and implies possible thoracic outlet syndrome (costoclavicular syndrome). This test is particularly effective in patients who complain of symptoms while wearing a backpack or heavy coat.

Wright (hyperabduction) test
PURPOSE- Identify pathology of structures that pass through thoracic inlet
DESCRIPTION- Patient sitting, locate radial pulse of the extremity being tested. Move shoulder into maximum abduction and external rotation.
Taking deep breath and rotating head opposite to test site may accentuate symptoms.RESULT- Neurological/ vascular symptoms (disappearance of pulse) will be reproduced
Roos Test
PURPOSE- Identify pathology of structures that pass through thoracic inlet
DESCRIPTION- The patient stands and abducts the arms to 90°, laterally rotates the shoulder, and flexes the elbows to 90° so that the elbows are slightly behind the frontal plane. The patient then opens and closes the hands slowly for 3 minutes
RESULT- If the patient is unable to keep the arms
in the starting position for 3 minutes or suffers ischemic pain, heaviness or profound weakness of the arm, or numbness and tingling of the hand during the minutes, the test is considered positive for thoracic outlet syndrome on the affected side.

Median Nerve, anterior interosseous N (C5, 6, 7)
shoulder: depression and abduction (110)
elbow: extension
forearm: supination
Wrist: extension
finger: extension

Median N, musculocutaneous N, axillary N
shoulder: depression and abduction (10), ER
elbow: extension
forearm: supination
Wrist: extension
finger: extension

Radial N
shoulder: depression, IR, Abd (40), ext (25)
elbow: extension
forearm: pronation
Wrist: flexion and ulnar deviation
finger: flexion

ulnar nerve (C8-T1 N root)
shoulder: depression and abduction (10-90), ER
elbow: flexion
forearm: supination or pronation
Wrist: extension and radial deviation
finger: extension
