SIADH, DI, Cerebral Salt Wasting
1/18
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
19 Terms
SIADH:
Syndrome of Inappropriate ADH Secretion
Definition: levels of ADH are inappropriately elevated compared to body's low osmolality, and ADH levels are not suppressed by further decreases in blood osmolality.
SIADH: causes
Irritation of CNS: meningitis, encephalitis, brain tumors, brain hemorrhage, hypoxic insult, trauma, brain abscess, Guillain Barre, hydrocephalus
Pulmonary disorders: pneumonia, asthma, positive end expiratory pressure ventilation, CF, TB, pneumothorax
SIADH: causes continued
Drugs: vincristine, vinblastine, opiates, carbamazepime, cyclophosphamide
Unregulated tumor production of ADH-like peptides: oat cell lung carcinoma for example, Ewings sarcoma, carcinoma of duodenum, pancreas, thymus
SIADH: function of ADH
antidiuretic hormone = vasopressin
ADH is made in the supra-optic nuclei in the
hypothalamus, stored in the posterior pituitary
Normally released into the bloodstream when
osmo-receptors detect high plasma osmolality
At the kidney, attaches to receptors in the collecting ducts, opens up water channels
Water is passively reabsorbed along the kidney's medullary concentration gradient
SIADH: signs and symptoms
Decreased/low urine output
Signs of hyponatremia: lethargy, apathy, disorientation, muscle cramps, anorexia, agitation
Signs of water toxicity: nausea, vomiting, personality changes, confused, combative
If Na < 110 mEq/L, seizures, bulbar palsies, hypothermia, stupor, coma
SIADH: lab values
Serum Na < 135 (Na is diluted by excessive free water re-absorption)
Serum osmolality low, normal is ~ 270
Urine Na is inappropriately high, >20 mmol/L, actually losing Na in urine instead of retaining it
Urine osmolality is inappropriately high, can range b/t 300-1400 mosm/L
CVP is high from free water retention
SIADH: treatment
Fluid restriction, ¾ maintenance
If symptomatic, may actually need to replace NaCl, can use hypertonic saline for example: 300cc/m2 of 1 ½ % NS
Diuretics such as lasix
Treat underlying disorder, for example usually resolves after removal of lung carcinomas
SIADH: treatment cont...
Demeclochlorotetracycline, blocks ADH receptors in the renal collecting ducts
In severe cases, hemodialysis
Warning, if increase Na too fast, at risk for pontine
myelinolysis
Max correction of 15mEq in 24 hours
DI = Diabetes Insipidus
Definition: inability to effectively conserve urinary water
Central: ADH not made or not released in the
hypothalamic-pituitary axis
Nephrogenic: ADH is released but not detected by the receptors in the kidney collecting ducts, often a sex-linked recessive condition, also due to renal pathology, electrolyte disorders, drugs
Central DI: causes
Head trauma
Brain neoplasms
Congenital CNS defects
CNS infections
CNS hypoxia
ADH secretion also decreased by certain drugs: EtOh, demerol, MSO4, dilantin, barbiturates, glucocorticoids
DI:
Make sure distinguish DI from conditions in which the presence of non-absorbable, osmotically active solutes in the renal tubules prevent water re absorption.
Example: glucose loss in the urine of diabetics will decrease the tubule- medullary concentration gradient and even though ADH is there, water won't get passively reabsorbed
Central DI: signs/symptoms
Polyuria
Dehydration, may not be readily apparent b/c of hyper- osmolarity, fluid shifts from cells to intravascular spaces and maintains blood pressure, CVP
Weight loss is a better measure of fluid status
Central DI: Lab values
Hypernatremia, Na >150-160
High serum osmolality (normal 270)
Urine Na < 20 mmol/L
Low urine osmolality (very dilute urine)
Central DI: treatment
Increase po or IV free H20 consumption, use hypotonic saline
Volume replacement cc for cc
Vasopressin/ ADH administration (bolus or drip 1.5-2.5 mU/kg/hr)
Of course, treat underlying cause
Cerebral Salt Wasting Causes:
CNS damage
Closed head injury
CNS surgery
CNS tumors
CNS infections, meningitis
Cerebral Salt Wasting s/s
Polyuria
Wt loss
Dehydration/hypovolemia
Hypotension
Low CVP
Cerebral Salt Wasting labs
Hyponatremia due to excessive renal Na loss
High urine Na, > 20 mmol/L
Increased plasma ANP, atrial natriuretic peptide, b/c of low volume status
Inappropriately normal or low aldosterone and ADH levels despite high ANP
Cerebral Salt Wasting treatment
Volume for volume replacement of urine Na losses
When dc'd from hospital, most will still need oral Na supplementation for a period of time
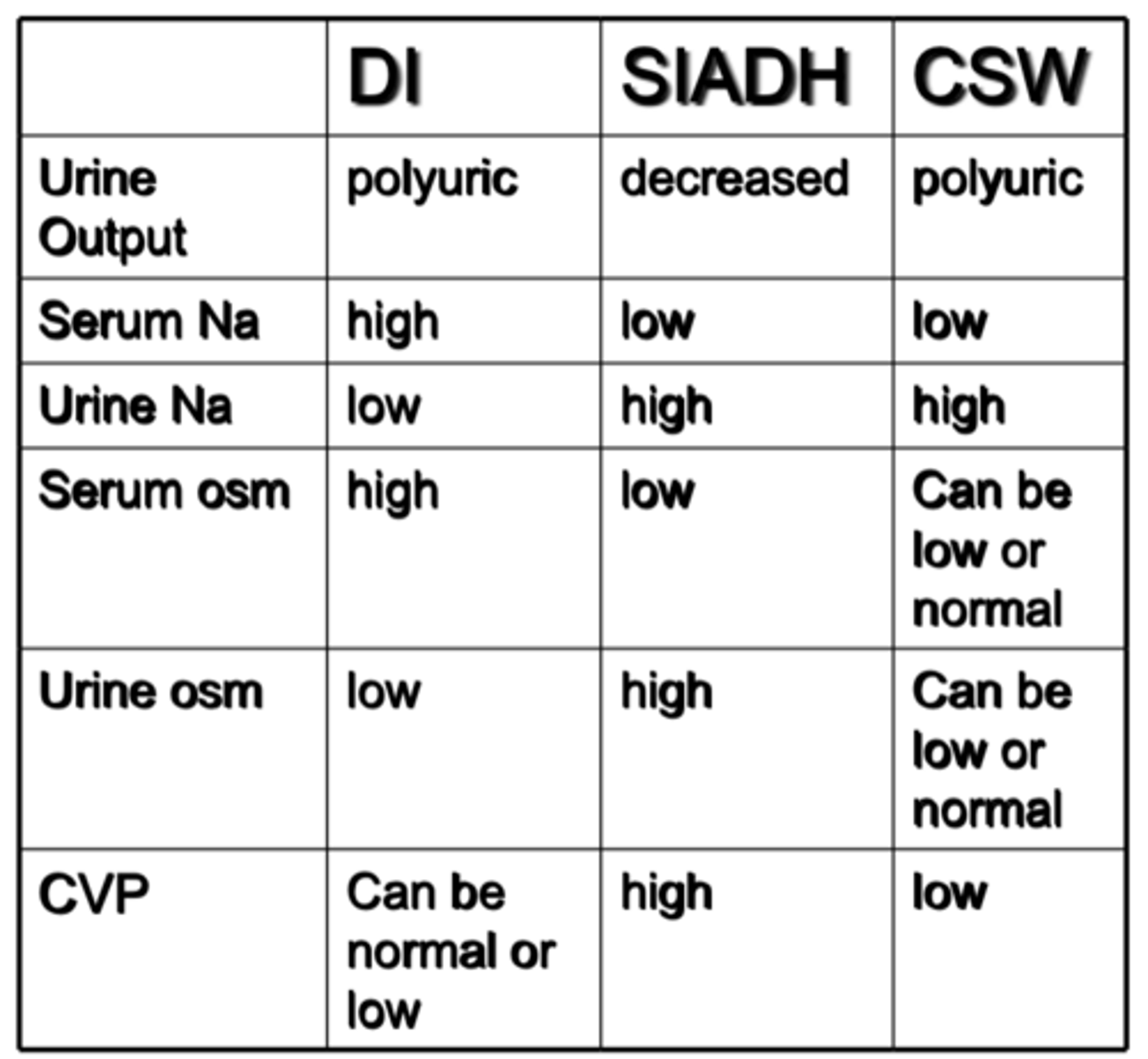
chart
pic