Lecture 5/6: Sx of the Intestines
1/104
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
105 Terms
What is an incision into the intestine?
enterotomy
What is removal of a segment of the intestines?
enterostomy
What intestinal resection and anstomosis?
an enterostomy with reestablishment of continuity between the divided ends
What is surgical fixation of one intestinal segment to another?
intestinal plication (aka an enteroenteropexy)
What is an enteropexy?
fixation of an intestinal segment to the body wall or another loop of intestine
surgical fixation of the colon
colopexy
partial or complete resection of the colon
colectomy
typhlectomy
resection of the cecum
colostomy
surgical creation of an opening between the colon and the surface of the body
tenesmus
straining to defecate
dyschezia
pain or discomfort on defecation
hematochezia
passage of stools that contain red blood
melena
passage of tarry stools (digested blood)
What are the common indications for sx of the small intestines?
GI obstruction: tumors, intussusception, FBs, masses
Trauma: perforation, ischemia
malpositioning
trauma
diagnostic/supportive procedures: biopsy, culture, cytology, feeding tubes
What are the common indications for sx of the large intestines?
obstruction: tumors, intussusception, granulomatous masses
perforation
colonic inertia
chronic inflammation
What can information about small intestines can visual examination provide?
mental status
temperament
nutritional state
comfort
What can information about small intestines can visual abdominal palpation provide?
pain
thickened intestine
abdominal masses
mispositioned organs
What portions of the large intestines are normally palpable?
colon (dorsocaudal abdomen)
feces or masses
sublumbar LN enlargement may be palpable
What are you evaluating for during a SA rectal exam?
• Shape & symmetry of pelvis
• Mucosal thickness
• Pelvic canal masses
• Intraluminal masses
• Distal strictures
What pre-op steps should be taken before intestinal surgery?
minimum database BW
localize lesions with diagnostics
correct abnormalities
transfuse if necessary
withhold food
administer prophylactic antibiotics if necessary
What systemic diseases need to be identified before small intestinal surgery?
• Renal Disease
• Hepatic Disease
• Hypoadrenocorticism
• Hypercalcemia
• Diabetes Mellitus
• Pancreatitis
True or false: most animals with large bowel disease have no laboratory abnormalities.
true
What can contrast studies show in the SI?
• Foreign bodies
• Obstructions
• Abnormal displacements
• Abnormal bowel wall thickness
• Irregular mucosal pattern
• Distortion of the bowel wall
Why is abdominal ultrasound typically done before contrast studies?
it often provides the diagnosis and allows the contrast study to be circumvented
What type of masses may be identified if colon contains gas?
luminal
What does a coiled spring appearance (with gas or barium) indicated in LI?
cecal inversion or intussusception
What have been replaced by colonoscopies?
barium enemas
What is the preferred intestinal imaging modality?
ultrasonography
What allows visualization and biopsy of the duodenum?
gastroduodenoscopy
What allows visualization and biopsy of the ileum?
colonoileoscopy
Visualization of intestinal mucosa may detect ______ that is not detected with radiographs or ultrasound.
ulcers, erosions, infiltrated mucosa and/or lymphangiectasia
What is endoscopy and colonoscopy more sensitive for than radiology?
masses
ulcers
infiltrates
intussusceptions
The benefits of stabilizing the animal’s condition before surgery must be weighed against:
risk of ischemic necrosis
risk/presence of septic abdomen
What contians more bacteria than the rest of the GI tract?
colon
What pre-op management step is unique to the colon?
emptying and cleansing indicated to reduce bacterial load, unless perforation or obstruction suspected
What is an elemental diet?
a diet that proposes the ingestion, or in more severe cases use of a gastric feeding tube or intravenous feeding, of liquid nutrients in an easily assimilated form. It is usually composed of amino acids, fats, sugars, vitamins, and minerals
What is given 24 hours prior to LI surgery?
laxatives
cathartics
warm water enemas
An electrolyte solution + enema is the best for cleansing the colon. When are electrolyte solutions contraindicated?
with obstruction
What negative effect can enemas have if given any closer to surgery than 3 hours pre-op?
may liquefy intestinal content and add to the dissemination of contaminated material during surgery
What type of enema should never be given to small or constipated patients?
hypertonic phosphate
What are the negatives of pre-op enemas?
enemas can further deteriorate debilitated, anorectic patients
may cause colonic perforation
may be ineffective in cats with megacolon
What are operative wounds in which the respiratory, gastrointestinal, or genitourinary tract is entered under controlled conditions without unusual contamination or without significant spillage of contents?
clean-contaminated wounds
What are open, fresh, accidental wounds; procedures in which gastrointestinal contents or infected urine is spilled or a major break in aseptic technique occurs?
contaminated wounds
When are SI prophylactic antibiotics indicated?
• In animals with intestinal obstruction because there is an increased risk of contamination associated with bacterial overgrowth
• When devascularized and traumatized tissue is present
• When surgery is expected to last longer than 2 to 3 hours
True or false: the risk of infection after colorectal surgery is low.
false
What type of antibiotics should be given for LI surgery?
systemic perioperative abx effective against anaerobes and gram (-) aerobes
What type of suture should be used for intestinal surgery?
monofilament, synthetic absorbable suture such as polydioxanone (PDS), polyglyconate, poliglecaprone (monocryl)
What type of needle should be used for intestinal surgery?
swaged-on taper or taper-cut point needle
What does optimal healing after intestinal surgery require?
good blood supply
accurate mucosal apposition
minimal surgical trauma
What intestinal layer provides mechanical strength?
submucosa
What approximating suture patterns are used in intestinal surgery?
simple interrupted
gambee
simple continuous
stapling techniques feasible
What should intestinal surgical sites be covered with?
omentum or serosal patch
What should be done before closing the abdomen during intestinal surgery?
replace contaminated instruments and gloves
What are the measurements for an approximating suture closure of the intestine?
place simple interrupted sutures 2 mm from the edge and 2-3 mm apart - engage slightly more serosa than mucosa to force everted mucosa back into the lumen
What suture pattern is this?
gambee
What are the advantages to enterotomy for biopsies?
• Allows access to the entire GI tract
• Provides full-thickness biopsies
• Can examine and sample the rest of the abdomen at the same time
What are the disadvantages to enterotomy for biopsies?
• Most expensive and most invasive technique
• Does not allow one to detect mucosal lesions
• Does not allow one to obtain as many mucosal samples as flexible endoscopy
• It is possible to take nondiagnostic tissue samples if proper technique is not followed
How is an intestinal biopsy performed?
occlude lumen, make stab incision into lumen with No. 11 blade
remove 2-3 mm ellipse of tissue with metzenbaum scissors
make second incision approx parallel to the first with a scalpel
clos incision with simple interrupted sutures
How is an enterotomy closed?
may be closed transversely if the intestinal lumen is small
join extremes of longitudinal incision with simple interrupted suture to transpose the incision to a transverse orientation
place remaining sutures 2 to 3 mm apart
How can you leak test enterotomy site?
syringe with sterile fluid
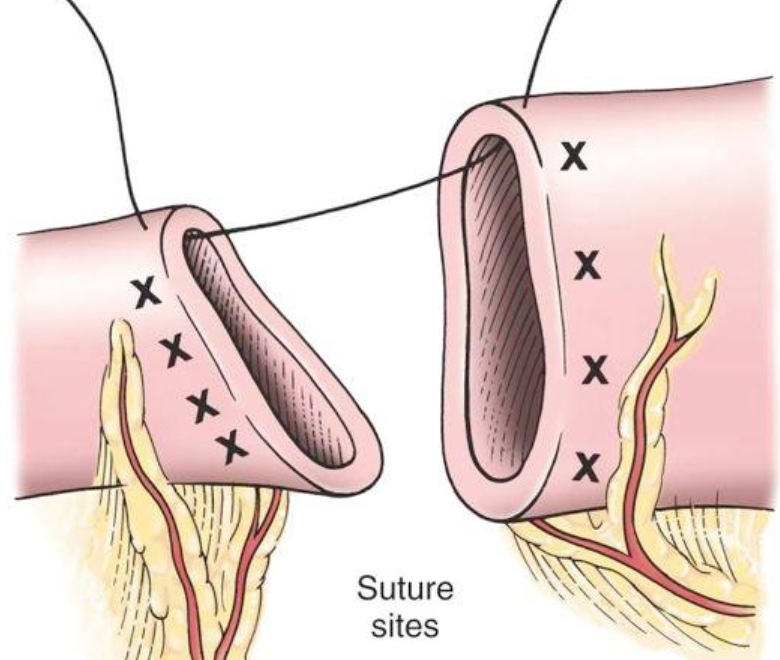
How is SI resection and anastomosis performed?
place forceps transversely across dilated proximal intestine and obliquely across the distal intestine
ligate vessels as indicated
transect intestine and mesentery where dashed lines indicate
place first suture at mesenteric border and second at anti-mesenteric border
place additional simple interrupted sutures to complete the anastomosis - appose mesentery in simple continuous pattern
How is an end-to-end anastomosis using a modified simple continuous pattern performed?
place and tie appositional sutures at mesenteric and anti-mesenteric borders, leaving the needles attached
using suture tags as stay sutures to maintain tension, place continuous suture pattern between anti-mesenteric and mesenteric sutures
reposition intestine and begin a second continuous suture line on the opposite side
What are the benefits of stapled anastomosis techniques?
• Less tissue reaction
• More mature fibrous connective tissue
• Greater tensile strength
• Fewer mucoceles
• Fewer necrotic areas
• Less luminal stenosis
What are the four stapled anastomosis techniques?
1. Triangulating End-to-End Anastomosis
2. Inverting End-to-End Anastomosis
3. Side-to-side or Functional End-to-End
4. End-to-side Anastomosis
How is a triangulating end-to-end anastomosis performed?
place 3 stay sutures that appose the ends of the intestine, and divide the circumference into 3 equal parts
apply tension between 2 of the sutures, fire the stapler, leaving a double staggered row of sutures
apply tension between next 2 sutures and position stapler to it overlies the end of the first row of staples and fire again
steps repeated a third time to complete anastomosis
How is an inverting end-to-end anastomosis performed?
Use an end-to-end anastomosis stapler and a transverse stapler.
Insert the stapler cartridge into the intestinal lumen through an enterotomy 3 to 4 cm from the transection site.
Insert the anvil into the other intestinal end.
Tie purse-string sutures securely around the shaft of the stapler.
After completing the anastomosis, close the enterotomy with sutures or a transverse stapler

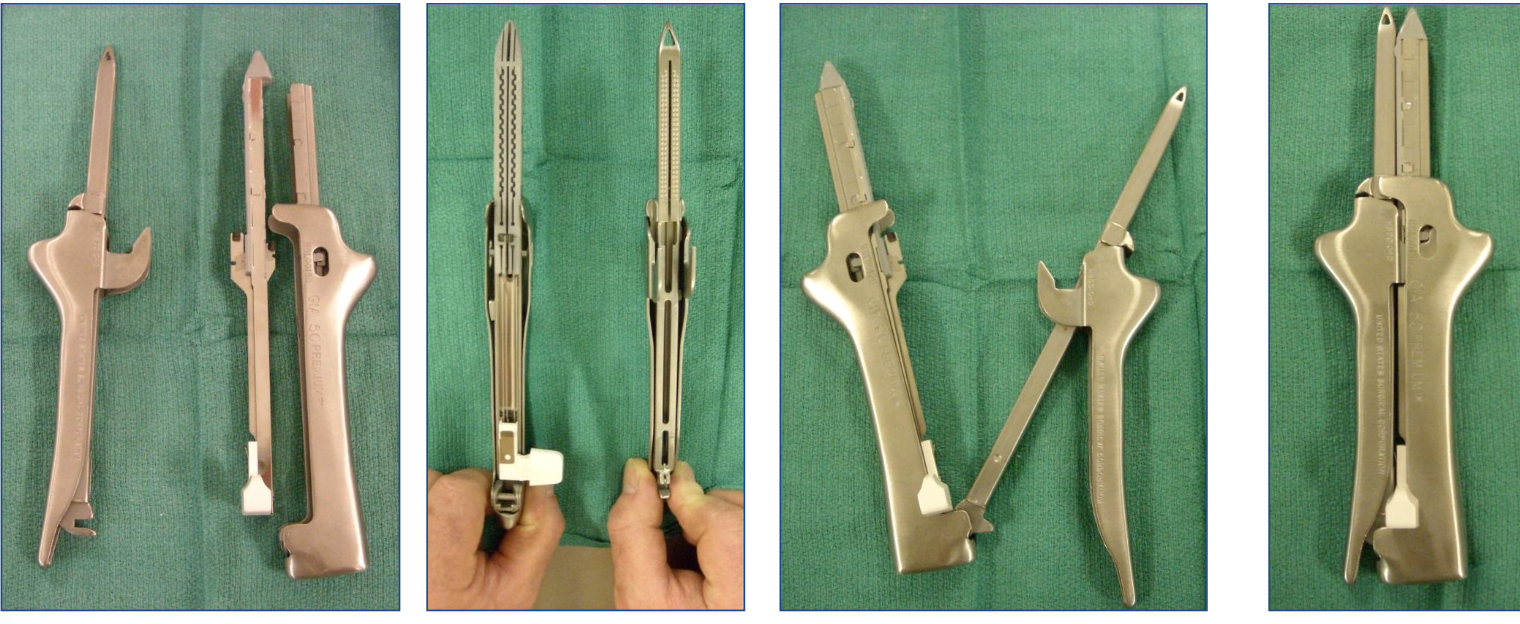
What is this stapler?
reloadable GIA 60 stapling device
side-to-side or functional end-to-end
(putting on the pants, putting on the belt)
What is the telescoping or invagination of one intestinal segment (intussusceptum) into the lumen of an adjacent segment (intussuscipiens)?
intussusception
What are the most common areas of intussusceptions?
ileocolic and jejunojejunal
True or false: the cause of most intussusceptions is unknown.
true
What is the presence of an intussusception in a cat more likely associated with than in dogs?
neoplasia
What are the major causes of protein-losing enteropathies in young dogs?
intussusception and parasites
How do intussusceptions appear on ultrasound?
target or bull’s eye pattern (concentric intestinal alyers)
What prevents recurrence of intussusception?
enteroenteropexy
How is an intussusception reduced?
place traction on neck as you milk the apex out of the intussuscipiens
What is the major concern when performing colonic surgery?
blood supply
How do you reduce colonic bacterial numbers?
by eliminating oral intake preparing the colon, and giving antibiotics
True or false: dehiscence is more likely with large bowel sx than small bowel.
true
Why is a colopexy typically performed
to create permanent adhesions between serosal surface of colon and abdominal wall
to prevent causal movement of the colon and rectum
to treat chronic recurring rectal prolapse
What is the typical complication of a colopexy?
infection resulting from suture penetration of the colonic lumen
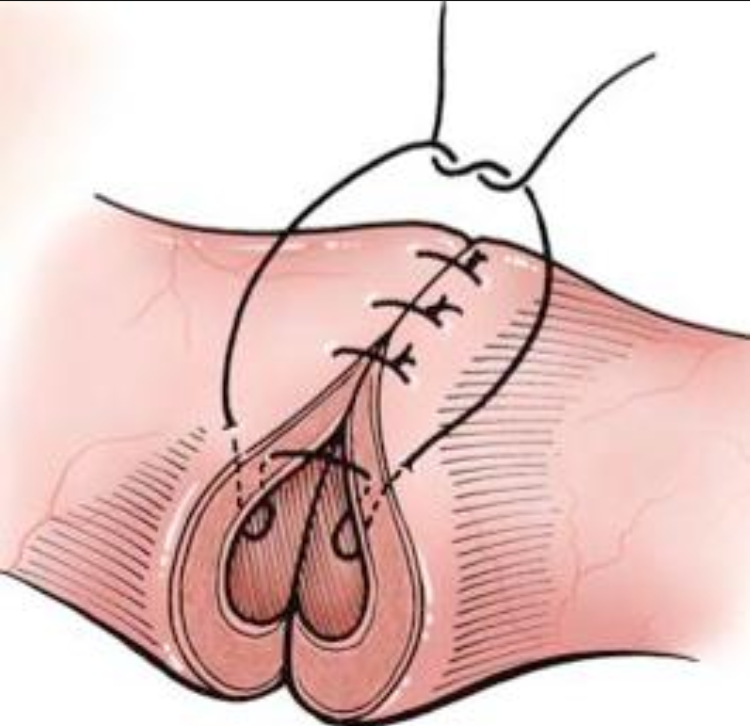
What is the technique for a colopexy?
locate and isolate descending colon
pull colon cranially to reduce prolapse
verify reduction by nonsterile assistant
make 3-5 cm longitudinal incision through only serosal and muscular layers along the antimesenteric border of descending colon
make similar incision in left abdominal wall several cm lateral to linea alba through peritoneum and underlying muscle
complete pexy with simple continuous pattern of 2-0 or 3-0 monofilament absorbable suture
lavage surgical site
wrap with omentum before closing
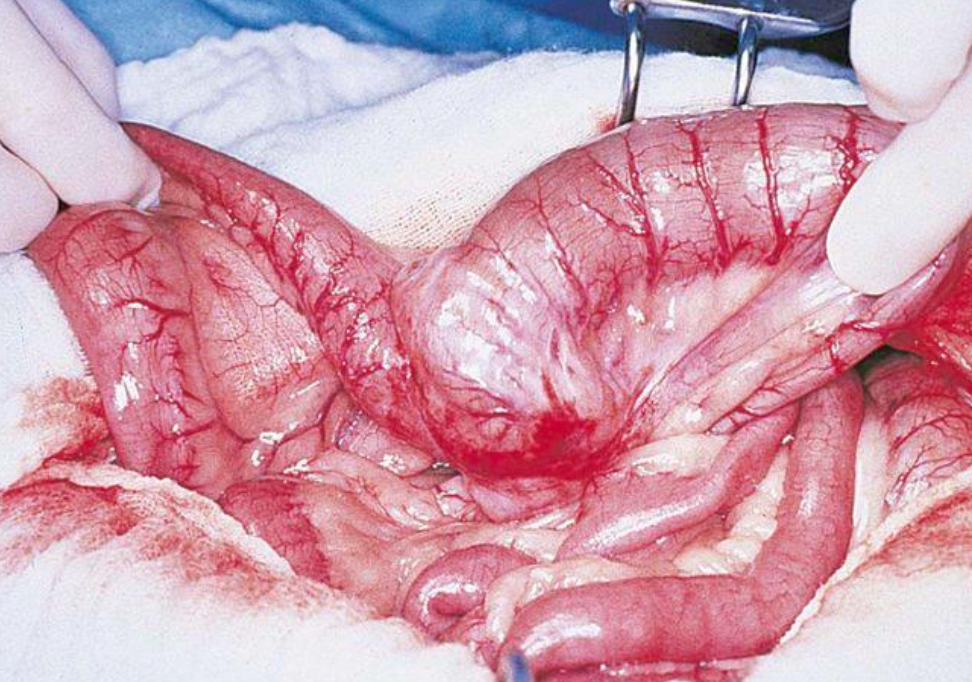
What procedure is being performed here?
colopexy
What are colectomy and resection primarily used for?
colonic mass removal and megacolon
What percent of the colon can be resected in animals without adverse side effects?
70%
True or false: dogs tolerate colonic resection better than cats.
false
What should the owners be warned about after a subtotal colectomy in a cat?
the cat will probably defecate frequently and have soft stools
Why should the colonic lumen be occluded at both ends?
to minimize fecal contamination
During a colonic anastomosis, why should a needle be angled so that slightly more serosa than mucosa is engaged?
to prevent mucosa from protruding between sutures
What should be done if there are minor disparities between lumen sizes?
space sutures around the larger lumen slightly further apart than the sutures in the segment with the smaller lumen
When should a two-layered anastomosis be performed?
if there is tension at he anastomotic site
What are the two layers of a two-layered anastomosis?
first layer of simple interrupted sutures is placed to appose the mucosa and submucosa, and the knots are tied within the lumen
the second layer of interrupted sutures apposes the muscularis and serosa, and the knots are positioned extraluminally
The distal colon may be anastomosed to:
ileum or jejunum
What are the indications for a typhlectomy (cecal resection)?
impacted cecum
inverted cecum
perforated cecum
neoplastic cecum
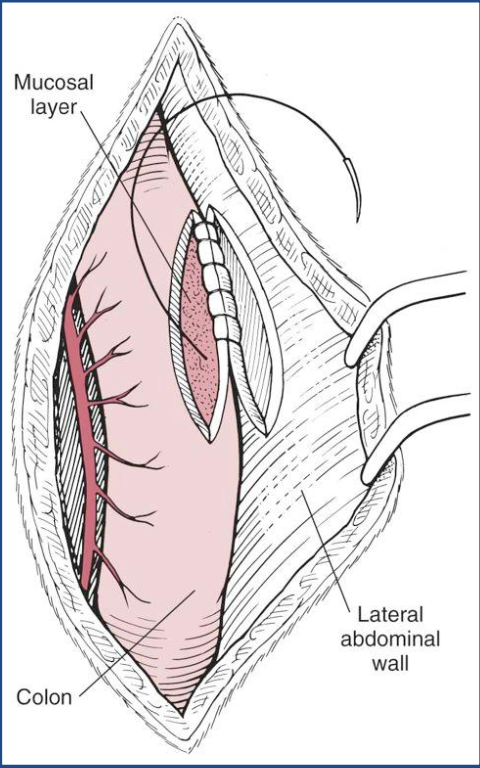
How is a typhlectomy performed?
double ligate cecal branches of ileocolic vessels
dissect the ileocecal fold of mesentery
place clamp across base of cecum near the cecocolic orifice and transect
close colonic defect with simple interrupted sutures
Why is a typhlectomy indicated for this animal?
cecum inverted into colonic lumen
What is megacolon?
persistent increased large intestinal diameter and hypomotility associated with severe constipation
What is the difference between constipation and obstipation?
• Constipation – difficult or infrequent defecation with passage of unduly hard, dry fecal material
• Obstipation – extreme constipation (no feces may be passed)
What species is megacolon most common in?
cats
What measurement determines megacolon in cats?
diameter of colon is greater than 1.5 x length of L7