PTA: 241 stroke test 2 part 1
1/118
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
119 Terms
in hemorrhagic stroke, what is the primary mechanism that causes neurological damage
direct tissue compression and increased intracranial pressure
what is the most common type of stroke
ischemic stroke due to thrombosis or embolism
pt presents with weakness primarily affecting the lower extremity on the right side with some involvement of the right shoulder and proximal arm. mental confusion and difficulty with executive functions are also noted which arterial territory is affected
left anterior cerebral artery
PTA is working with a pt who as anterior cerebral artery syndrome which functional defect would most expected to interfere with gait training
significant lower extremity weakness and spasticity
what set of symptoms would be most indicative of vertebrobasilar artery syndrome
dizziness diplopia dysarthria and bilateral limb ataxia
a PTA notices that a stroke pt consistently ignores objects and people on their left side and only eats food from the right side of their plate what is this a characteristic of
right hemisphere stroke with unilateral neglect
stroke pt exhibits impulsive behavior frequently attempting to stand and walk without assistance despite significant balance deficits they seem unconcerned about falling and become agitated when reminded to use safety precautions. What is this behavior associated with
right hemisphere stroke with impaired judgment
during therapy session a stroke pt becomes extremely frustrated and begins crying when attempting a simple reaching task they previously preformed easily this emotional lability is
Pseudobulbar affect, a common neurological consequences of stroke
in the acute phase immediately following stroke a pt presents with complete flaccidity on the affected side over the following weeks muscle tone gradually increases and spastic patterns begin to emerge this progression is most accurately described as
a typical recovery sequence following upper motor neuron lesions
during therapy a stroke pt demonstrates the ability to perform shoulder flexion to 90 degrees but only when the entire upper extremity flexor synergy is activated according to brunnstrom's stages of recovery this pt is most likely in
stage 3 spasticity increases synergies are strong
during gait training a stroke pt demonstrates automatic finger and wrist extension on the affected side when arm is raised above shoulder height this phenomenon is known as
souques phenomenon
pta observes that when a stroke pt preforms resisted hip abduction on the unaffected side the affected leg also attempts to abduct this represents what
raimiste's phenomenon
during therapy a stroke pts head is turned to the right the right arm extends while the arm flexes creating a fencers position this demonstrates what
asymmetrical tonic neck reflex
stroke pt is supported standing demonstrates rigid extension of the legs with plantar flexion when weight is applied through the balls of the feet this reaction would most interfere with
dynamic weight shifting and stepping activities
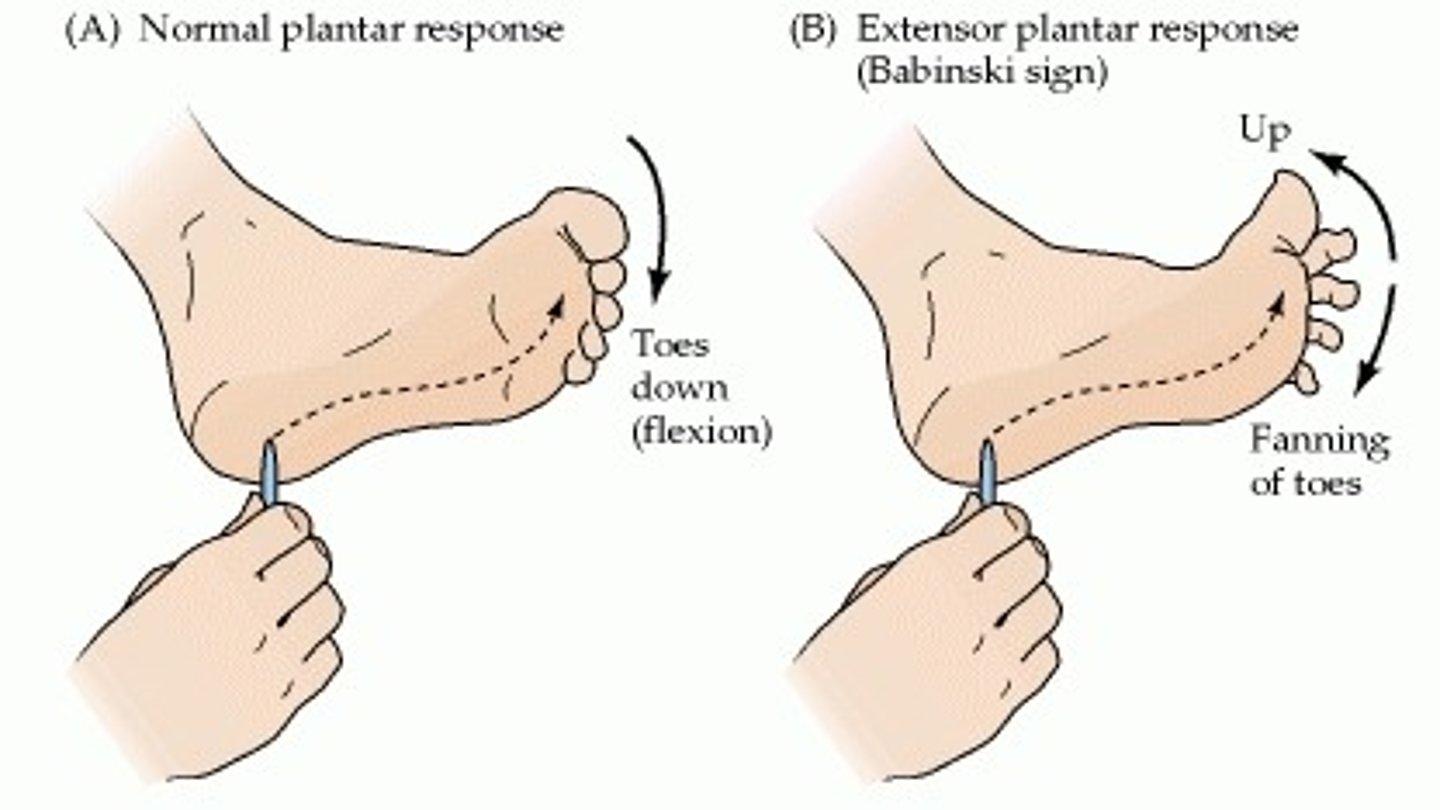
when testing a stroke pts plantar reflex the pta observes dorsiflexion of the great toe with fanning of the other toes upon stroking the lateral sole of the foot this finding indicates
positive babinski reflex indicating upper motor neuron lesions
What is the primary underlying pathological process that leads to most ischemic strokes?
Atherosclerosis of cerebral or carotid arteries
Which combination of clinical signs would be most characteristic of middle cerebral artery (MCA) syndrome?
Contralateral hemiparesis with face and arm > leg, aphasia (if dominant hemisphere)
Which behavioral difference is MOST commonly associated with left hemisphere stroke compared to right hemisphere stroke?
Catastrophic emotional reactions and depression
A patient with right hemisphere stroke demonstrates denial of their left-sided weakness and insists they can walk independently despite clear hemiparesis. This behavior is most consistent with:
Anosognosia (lack of awareness of deficits)
A stroke patient is attempting to flex the hip during gait training and simultaneously demonstrates knee flexion, ankle dorsiflexion, and toe extension on the same side. This movement pattern represents:
Lower extremity flexor synergy pattern
A stroke patient demonstrates involuntary flexion of the affected arm when performing forceful knee flexion on the same affected side. This phenomenon is called:
Homolateral limb synkinesis
A stroke patient is positioned supine and demonstrates increased extensor tone in both arms and legs. When the head is flexed forward, the arms flex and legs extend. This reflex pattern is MOST consistent with:
Symmetrical tonic neck reflex
When testing a stroke patient's plantar reflex, the PTA observes dorsiflexion of the great toe with fanning of the other toes upon stroking the lateral sole of the foot. This finding indicates:
Positive Babinski reflex indicating upper motor neuron lesion
Stroke/ cerebrovascular accident (CVA)
sudden loss of neurological function caused by an interruption of blood flow to the brain
ischemic stroke
most common stroke
result from thrombosis, embolism or hypoperfusion
hemorrhagic stroke
occurs when blood vessels rupture causing leaking of blood around the brain and increasing intracranial pressure
hemiplegia
paralysis of one side of the body
hemiparesis
weakness on one side of the body
what is the major contributory factor in cardiovascular disease that can lead to strokes
atherosclerosis
Atherosclerosis
condition in which fatty deposits called plaque build up on the inner walls of the arteries
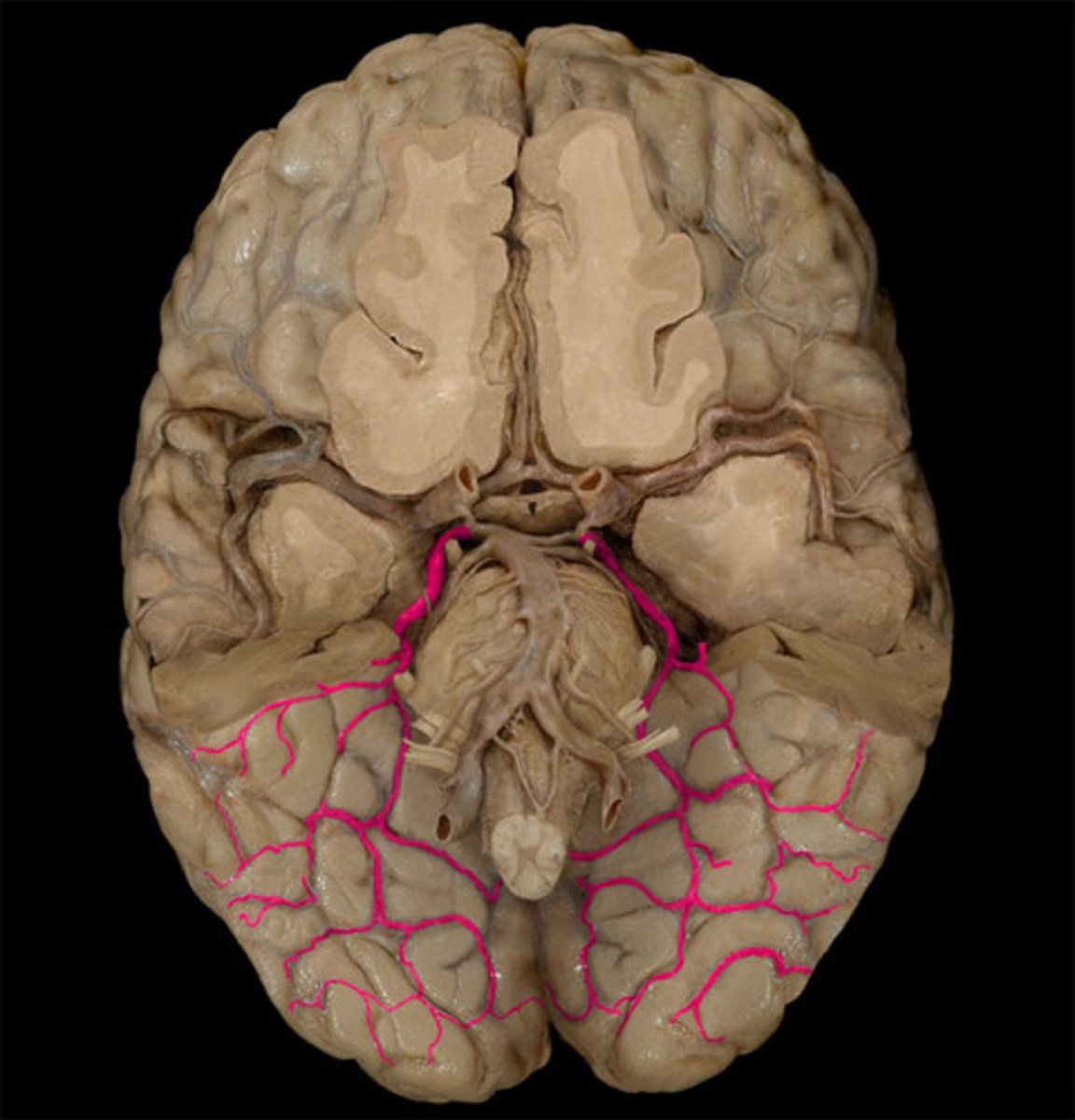
most common sites for lesions to occur
Origin of common carotid artery
Transition into the middle cerebral artery
Main bifurcation of the middle cerebral artery
Junction of the vertebral arteries with the basilar artery
cerebral thrombosis
formation of blood clot within the cerebral arteries or their branches
cerebral embolus
composed of bits of matter that are released into the blood stream and travel and are lodged into the vessel which produces occlusion and infarction
risk factors of stroke
hypertension, DM, disorders of heart, high blood cholesterol, smoking, heart disease
what is FAST in relation to stroke
mnemonic to help improve responsiveness to stroke victims by calling 911 recording to the warning signs
what does FAST stand for
F: face drooping
A: arm weakness
S: speech difficulty
T: time to call 9-1-1
what time of scan is used to differentiate between atherothrombotic stroke and hemorrhagic stroke
CT scan
Transient Ischemic Attack (TIA)
temporary interruption of blood supply to the brain
last less than 24 hrs no permanent defects
anterior cerebral artery
supplies blood to medial cerebral hemispheres
subcortical structures
basal ganglia
anterior fornix
anterior four-fifths of corpus callosum

anterior cerebral artery syndrome
contralateral hemiparesis and sensory loss greater
urinary incontinence
apraxia
contralateral grasp reflex and sucking reflex
what extremities are greater involved with ACA syndrome
lower extremity (LE)
Middle Cerebral Artery (MCA)
supply blood flow to
entire lateral aspect of the cerebral hemisphere
corona radiata
globus pallidus
most of caudate nucleus and putamen

middle cerebral artery syndrome
contralateral spastic hemiparesis and sensory loss of the face
global aphasia
contralateral ataxia
aphasia
what extremities are greater involved with MCA syndrome
upper extremity
posterior cerebral artery
supplies blood to
occipital lobe
medial and inferior temporal lobe
posterior cerebral artery syndrome
contralateral hemiplegia
hemianesthesia
visual agnosia
dyslexia
memory defects
vertebral arteries
supply blood to
cerebellum and medulla

Locked-in syndrome (LIS)
occurs with basilar artery thrombosis and bilateral infarction of the ventral pons
catastrophic event with sudden onset
s/s of LIS
cannot move or speak but remains alert and oriented
communication only by eye movements
aphasia
acquired communication disorder
impairment of language comprehension and formulation
receptive aphasia (Wernicke's aphasia)
pt can not comprehend spoken language and has a hard time following commands
nonfluent aphasia
comprehension is good but speech is slow and hesitant speech production is labored or lost completely
global aphasia
severe aphasia impairments of both language and comprehension.
dysarthria
slurred speech due to lesions in parts of CNS or PNS that mediate speech production
dysphagia
swallowing dysfunction
aspiration
penetration of food liquid saliva or gastric reflux into the airway
nasogastric tube (NG)
Tube inserted through the nose to the stomach.
gastrostomy tube (G-tube)
tube placed through the abdomen directly into the stomach and used to provide nourishment long term use
disorientation
pt being unable to provide information about self, time and location
result of lesions in prefrontal cortex, limbic system and limbic cortex
attention
ability to select and attend to specific stimulus
memory
the ability to store experiences and perceptions for later recall
Confabulation
memory gaps filled with inappropriate words or fabricated stories
perseveration
continued repetition of words thoughts or acts pt gets "stuck" with repeating words "parrot talk"
confusion
result of disruption of the prefrontal cortex
executive functions
abilities that enable a person to engage in purposeful behaviors
impulsiveness lack of abstract thinking impaired organization, impaired planning ability
Pseudobulbar Affect (PBA)
emotional lability
quickly changes in laughing to crying with only slight provocation
left hemisphere lesion results with side effects on what side
right
(right hemiplegia)
right hemisphere lesion results with side effects on what side
left
(left hemiplegia)
side effects of right hemisphere lesion
"tigger"
quick impulse behavior
poor judgment unrealistic
unaware of defects
happy about everything
side effects of left hemisphere lesion
"eeyore"
slow
difficulties in communication
highly distractible
very aware of defects
difficulty expressing positive emotions
unilateral neglect
lack of awareness of part of body or external environment
depression
persistent feelings of sadness accompanied by feelings of hopelessness worthlessness and or helplessness
apathy
do not care attitude
shallow affect and blunted emotional responses
euphoria
increased levels of irritability or frustration and social inappropriateness
Brunnstrom 6 stages of recovery
1: flaccidity
2: min. voluntary movement,spasticity begins to develop
3: voluntary control of synergies, spasticity at peak
4: movements don't follow synergies, spasticity declines
5: learns difficult movements
6: spasticity disappears; return to normal motor function
bobath 3 stages of recovery
1: early-initial flaccid stage 2: middle-stage of spasticity
3: late-stage of relative recovery
upper extremity flexion synergy
Scap retraction/elevation• Shoulder abd, ER
Elbow flexion
Forearm supination
Wrist & finger flexion
upper extremity extension synergy
Scap protraction
Shoulder add, IR
Elbow extension
Forearm pronation
Wrist & finger flexion
lower extremity flexion synergy
Hip flexion, abd, ER
Knee flexion
DF, inversion• Toe dorsiflexion

lower extremity extension synergy
Hip extension, add, IR Knee extension
PF, inversion
Toe plantar flexion

describe ataxia gate
wide base of support
lower center of mass
associated reactions
see in pts with strong synergies and spacity
unintentional motions
souques phenomenon
if UE is affected and UE is elevated fingers will extend
Raimiste's phenomenon
resisted AB or ADduction on unaffected side and affected leg will respond
homolateral limb synkinesis
mutual dependency between affected UE and LE
(if right leg flexes right arm will flex)
basal ganglia CVA
bradykinesia (slow movement)
involuntary movements
cerebellum CVA
cerebellar ataxia
motor weakness
motor praxis
the ability to plan and execute coordinated movement
apraxia
seen with left hemisphere lesion
pt demonstrates difficulty planning and executing purposeful movement
ideational apraxia
inability to formulate an initial motor plan and sequence tasks where the proprioceptive input necessary for movement is impaired
ideomotor apraxia
pt is unable to produce the task you ask them todo but is able to move automatically
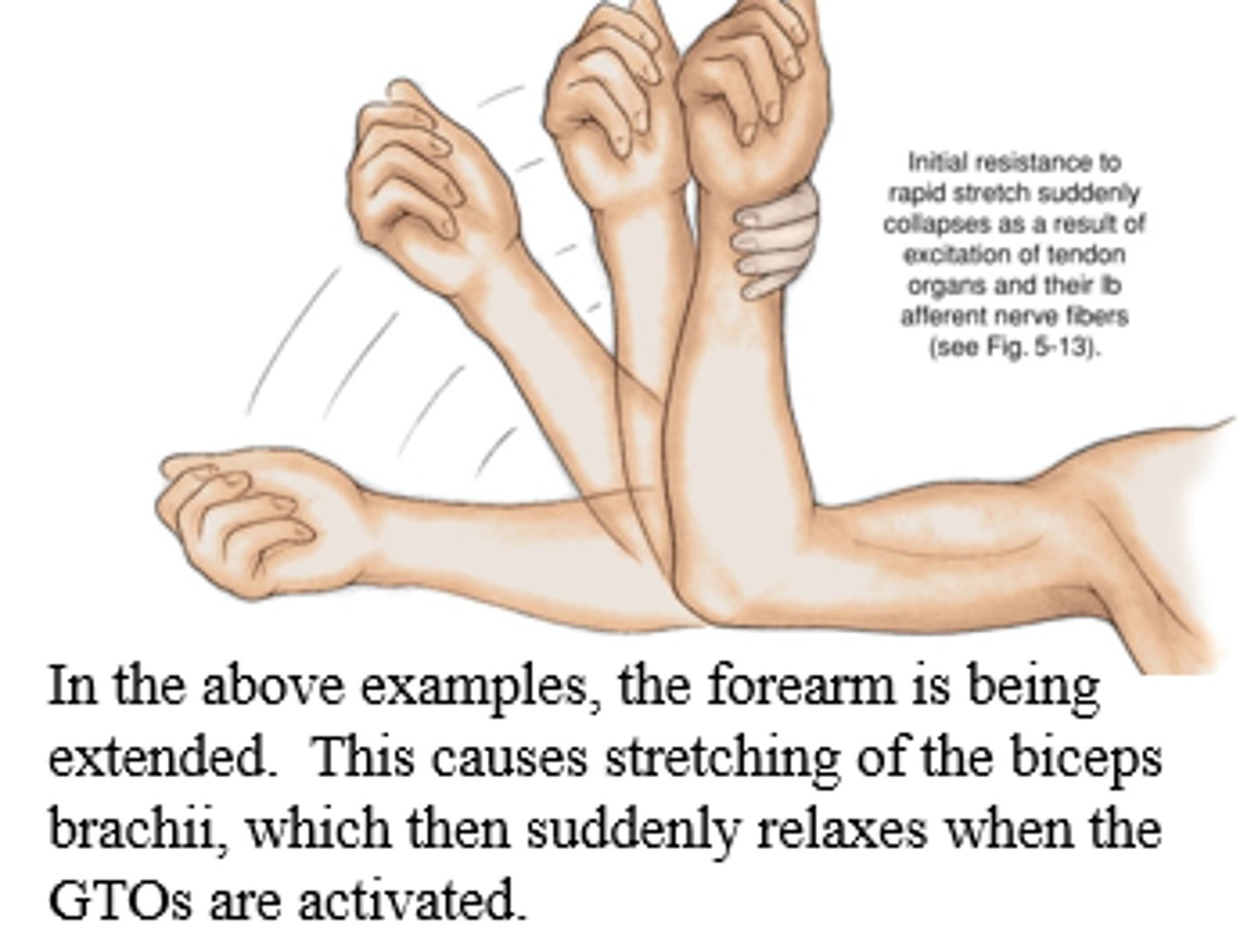
hyperactive stretch reflex
protective mechanism
protects muscle from being stretched too far
ex) knee will bend if SLR is occurring too far

clonus
seen in ankle and foot
foot bounces if rapidly changed position
simplicial reaction to sustained stretch in a muscle
clasp knife reflex
increase muscle resistance gives when passive motion is applied causing limp to close like a pocket knife
positive babinski
stroking lateral side of foot causing great toe to extend and lateral toes to fan out
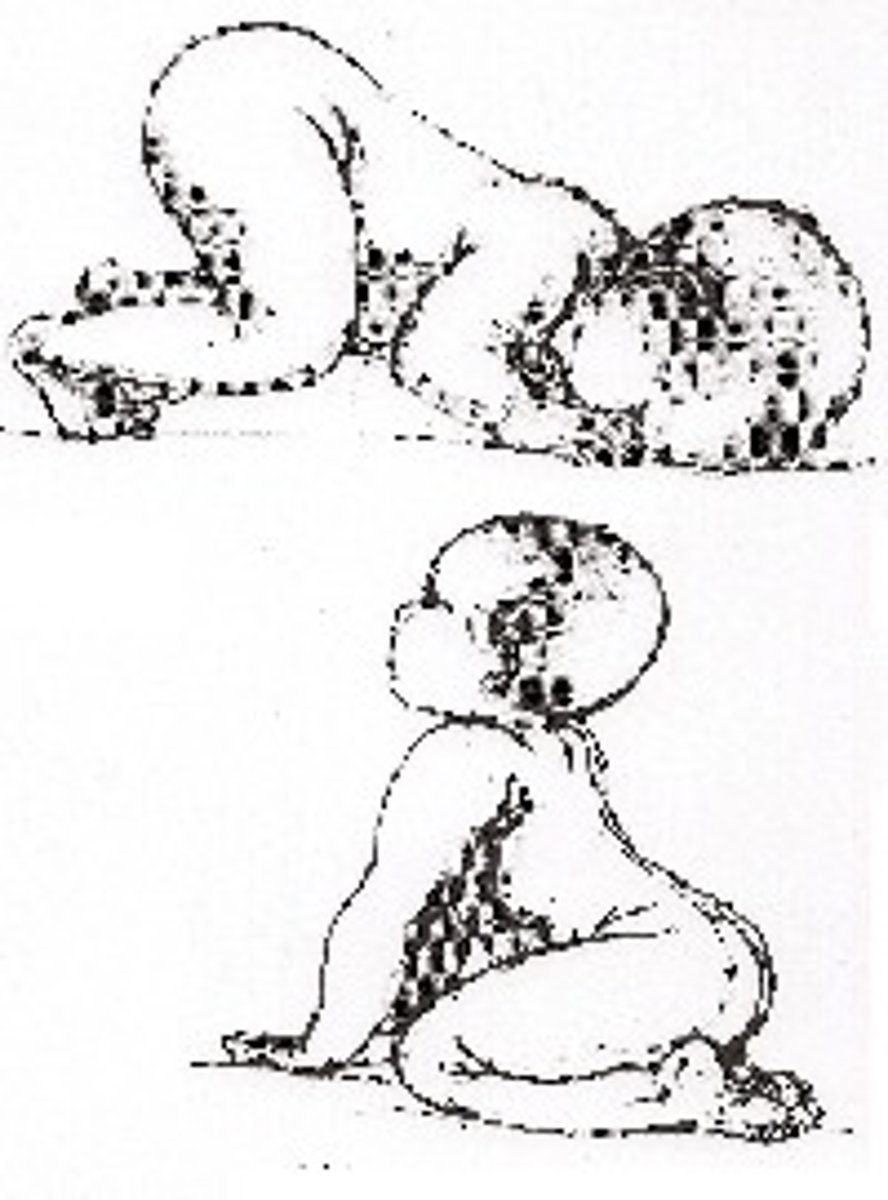
STNR (symmetrical tonic neck reflex)
(dog under fence)
flexion of head creates flexion of UE
extension of head creates extension of UE
opposite motion of head happens with LE
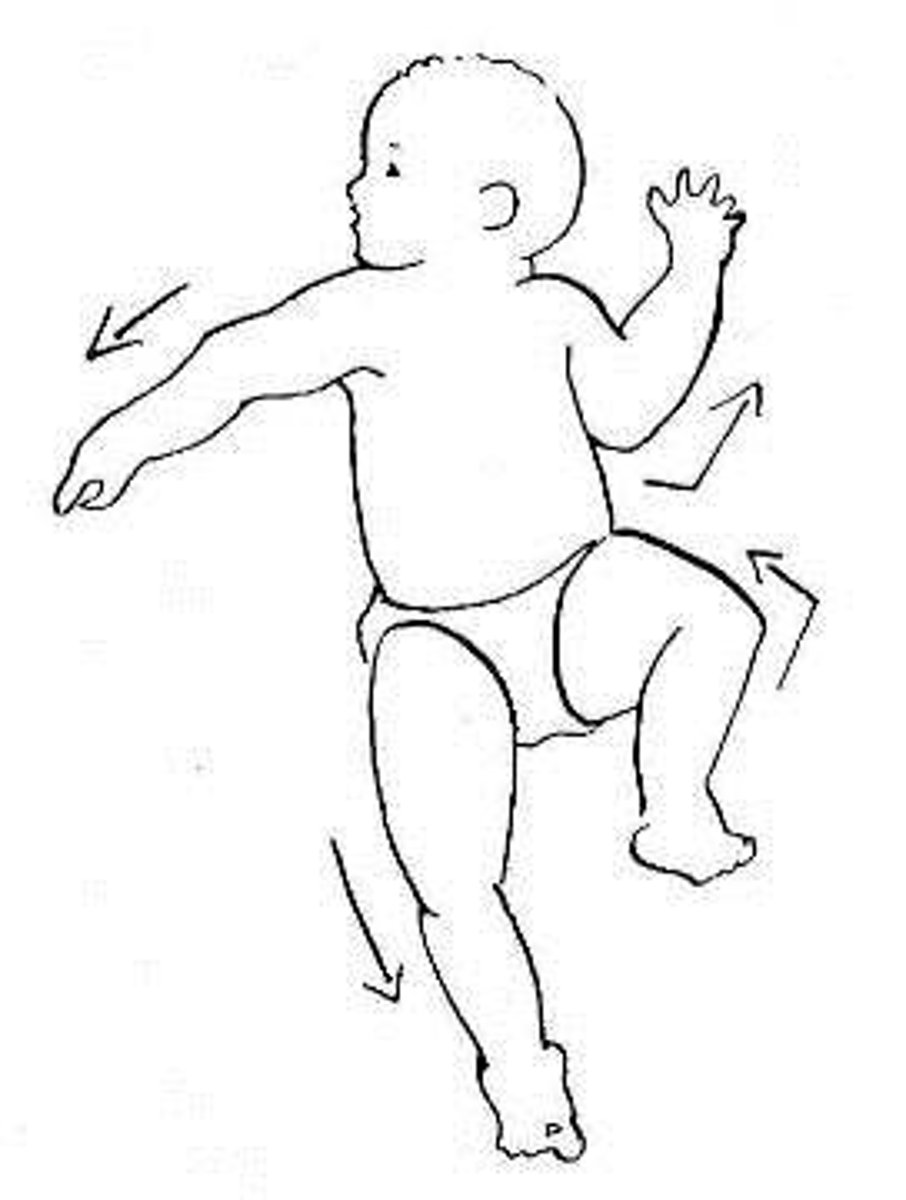
ATNR (asymmetrical tonic neck reflex)
(fencer reflex)
turn of head result sin face side extends skull side flexes
ex) head turns to right, right arm and leg extends left arm and leg flexes
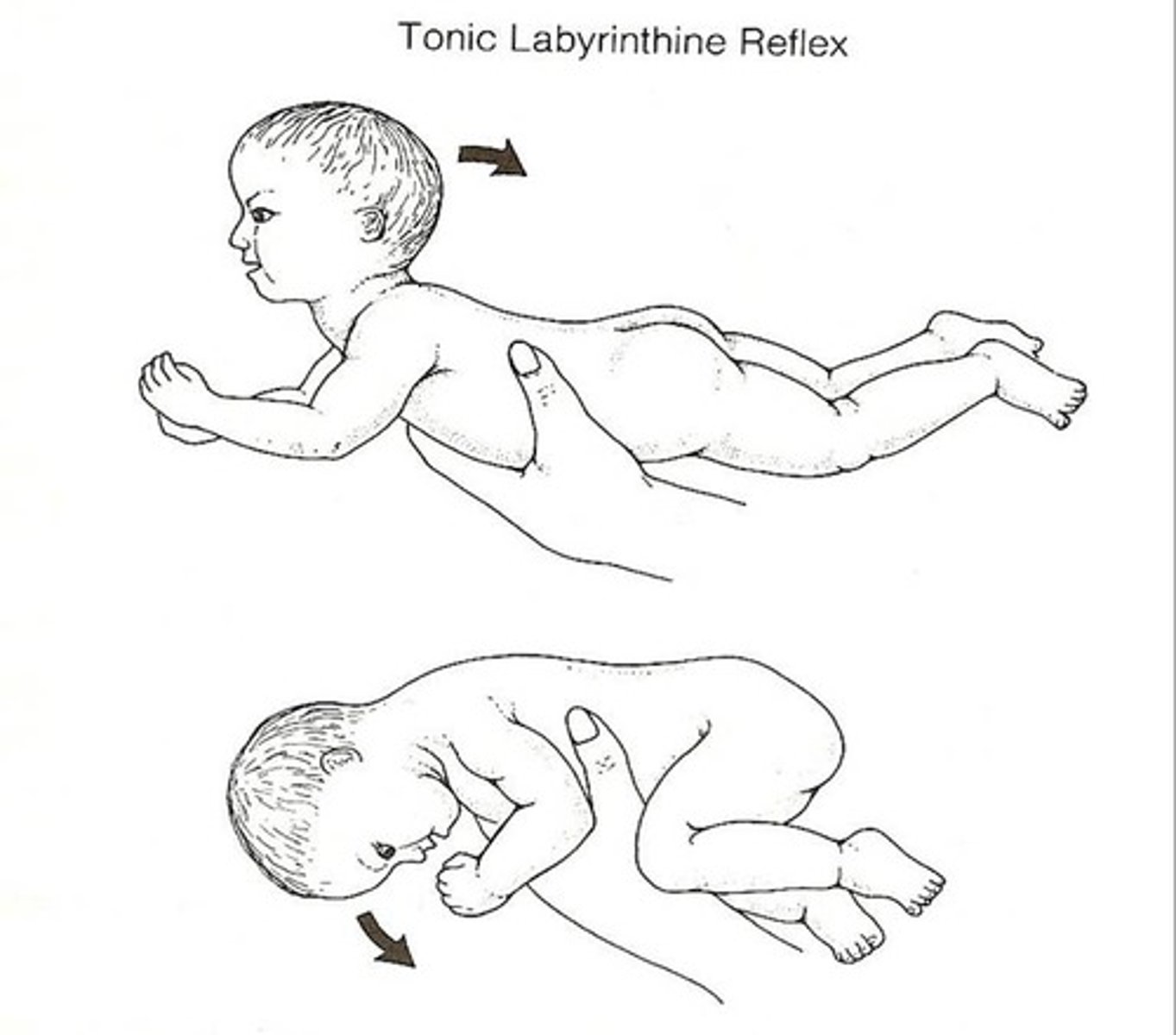
STLR (symmetrical tonic labyrinthine reflex)
prone: everything flexes
supine: everything extends
positive support reaction
pressure of bottom of foot cretes extension of hip and knees

proprioception
sense of body position in space