Exam 3: Disability, Sexual Function & Intimacy
1/55
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
56 Terms
ability to derive pleasure from the senses
sensuality
desire, sexual preference, and sexual identity and behavior
sexuality
t/f sexuality can symbolize how a person is dealing with the world
true
t/f sexuality is an integral part of the human experience and is important for self esteem and self-concept
true
t/f if a person feels inadequate as a sexual, sensual, and lovable human
being, the motivation to pursue other avenues are not really affected affected.
false
before initiating a conversation about sexuality, the OT practitioner should:
ask the client for permission
these are topics that some may find uncomfortable
t/f sexual hygiene is an ADL
true
an increased dependence on an able-bodied partner can result in
a decrease in the couple's sex life
One possible explanation is that the able-bodied partner is less inclined to be aroused when he or she has just bathed the partner or assisted the partner with toileting.
It is often difficult to transition from caregiver to intimate partner.
emasculation
loss of power and masculinity
The client's sense of masculinity or femininity may be threatened by the disability
For example, lifting weights may no longer be possible,
sports participation may not be possible without adaptations,
One way to approach a discussion of intimate matters is to ask what to female and male clients?
Ask the female client how she will perform breast self-examination with her disability.
Ask the male client if he has noticed any physical changes in his body or how he will perform self-examination of the testicles.
This interaction can set the stage for discussion of other personal matters; it also impresses upon the client the necessity for concern about personal health and reaffirms the client's sexual identity.
Why are clients usually comfortable with talking to OTs about sexual matters?
Clients may feel safe asking the OT about sexual matters related to their disabilities because the therapist deals with other intimate activities, such as bathing, dressing, and toileting
t/f The OT is the most appropriate professional to solve some problems, such as the motor performance needed for sexual activity.
true
For example, discussing positioning to reduce pain or
hypertonicity or to enable the client to more comfortably engage in sexual relations will help the client deal with problems before they occur
The ... of the client, the partner, and the therapist must be examined for the therapist to interact with the client in the most effective and positive manner
sexual values
what is the purpose of a sexual history?
The purpose of a sexual history is to learn how a person thinks and feels about sex and bodily functions and to discover the needs of those concerned
Types of questioning:
1) routine (part of routine OT assessment)
2) generalizing (people frequent experience sexual problems)
3) normalizing (normal given a diagnosis)
4) use of statistics (share characteristics of a stat group)
5) open ended
6) framing (ask about body, terms, sexual engagement)
t/f These conversations may take place while other therapeutic activities are in progress so that billing insurers for time is not a barrier.
true
model that is useful to help determine type and extent of sexuality intervention needed
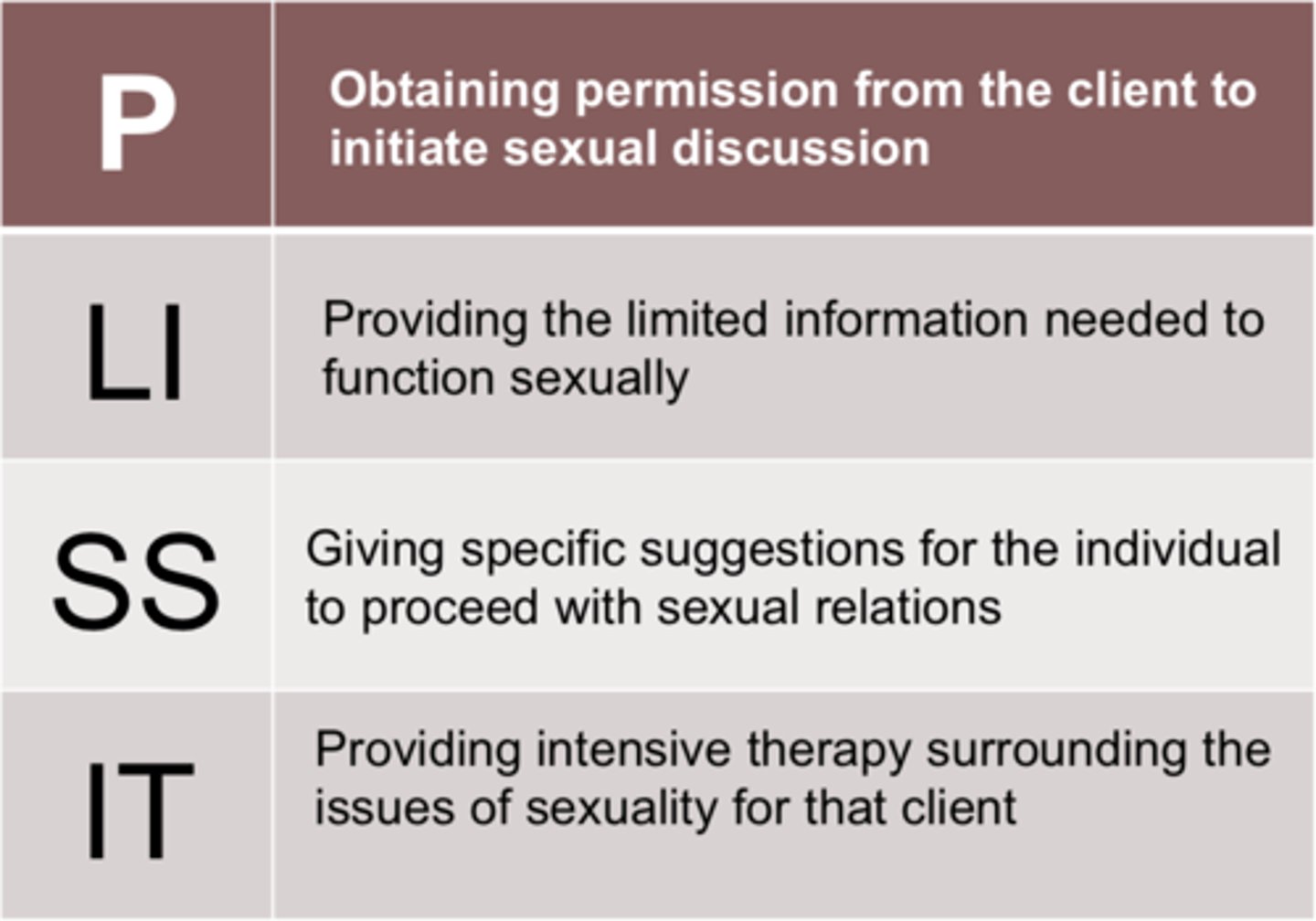
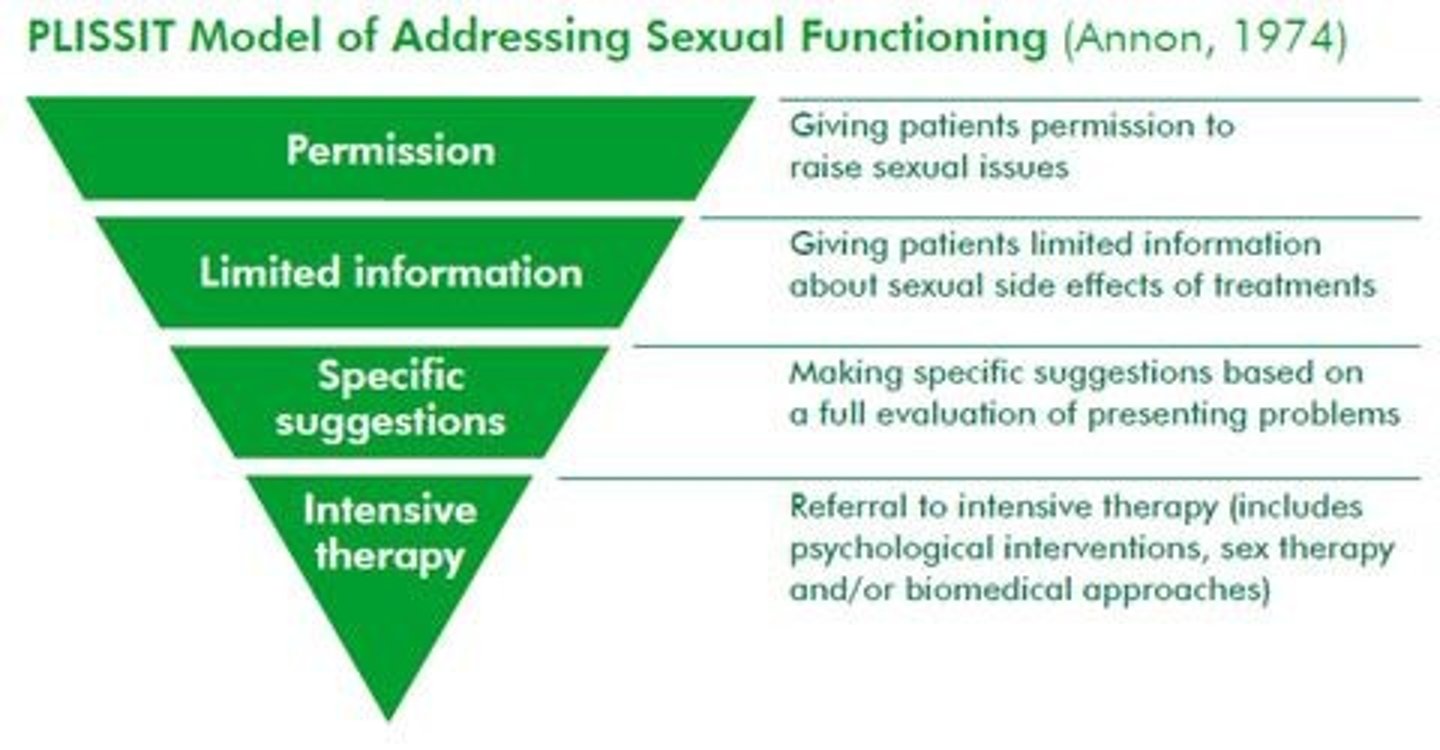
PLISSIT Model
PLISSIT Model
useful to help determine:
- type and extent go sexuality intervention needed
-appropriate clinician skill level
- need for referral to specialist
P - Permission
LI - Limited Information
SS - Specific Suggestions
IT - Intensive Therapy
4 levels of PLISSIT Model
P - Permission
LI - Limited Information
SS - Specific Suggestions
IT - Intensive Therapy
PLISSIT Model - Permission Level
▪Within skill level of all OTs
▪Reassuring patients that actions and feelings are normal and acceptable
▪Proactive approach to discussion of sexuality
▪Include as part of initial evaluation
▪Sexual expression is an ADL
▪ASAP if not included in initial eval
PLISSIT Model - Permission Level OT competencies
▪Acknowledge the sexuality of all persons
▪Comfort with own sexuality
▪Comfortable discussing sexuality or willingness to overcome discomfort
▪Refrain from projecting personal morals and attitudes onto others
PLISSIT Model - Limited Information Level
▪Provision of specific info regarding sexual concerns
▪Dispelling myths or misconceptions
▪Providing facts about effect of disability on sexuality
▪Limit info to patient's specific concern
▪Guide patient in seeking accurate info
PLISSIT Model - Limited Information Level OT competencies
▪Have basic understanding of human sexuality
▪Understand typical sexual physiology
▪Analyze effects of disability on sexual activities
▪Willing to seek and provide accurate info
▪Understand limitations of personal knowledge base
PLISSIT Model - Specific Suggestions Level
▪Suggestions aimed at solving specific sexual difficulty
▪Requires more knowledge, time and skill
▪Obtain detailed sexual history
▪Identify problem areas
▪Collaborate to establish goals
PLISSIT Model - Specific Suggestions Level OT competencies
▪Familiar with various sexual activities
▪Comfortable discussing specific sexual activities
▪Able to compile a sexual problem history
▪Adapt sexual activities to accommodate functional limitations
PLISSIT Model - Intensive Therapy Level OT
▪When sexual problems are beyond scope of goal-oriented suggestions
▪Intervention requires formal training
---Sex therapy
---Sexuality counseling
---Psychotherapy
▪Beyond the scope of most OTs
▪Referral to psychologist or sex therapist
When taking a sexual history, the therapist should create an environment that will allow for:
confidentiality and encourages comfort and self-expression
t/f After taking the sexual history, the therapist can often ascertain whether guilt, fear, or discomfort is connected with the sex act
true
t/f sexual abuse is not problem in adults with disabilities
false!
t/f Caregivers, medical staff members, aides, transportation assistants, or
volunteers of sexual abuse are not typically abusers
false!!
we must always be alert to signs of possible abuse from these sources
How can we help prevent abuse?
The therapy session should help the client develop a sense of personal ownership of her or his body
Teach clients that is okay to say no to being touched!
The therapist should ask permission before touching the client; he or she should touch with respect and maintain the client's sense of dignity. If the therapist does not ask permission to touch a client, the client can:
lose his or her sense of control over being touched by others.
t/f Naming body parts and body processes is a good way of helping clients take charge of their bodies.
true
Once the body parts and processes have been named, using correct terminology rather than slang, the possibility exists for the client to communicate and to relate in an appropriate manner.
The use of the proper terms has the effect of helping the client view the body in a more positive way, whereas slang tends to communicate negative images.
t/f The use of the proper terms has the effect of helping the client view the body in a more positive way, whereas slang tends to communicate negative images.
true
What are some effects of physical dysfunction that can hinder sexual activity?
1) hypertonia
2) hypotonia
3) low endurance
4) loss of mobility and contractures
5) joint degeneration
6) pain
7) loss of sensation
tx strategies for clients with hypertonia:
- slow movements
- use inhibitory techniques (slow rocking, slow stroking)
- avoid cold room temp
- stress can increase tone!! (massage, visualization)
tx strategies for clients with hypotonia:
- need physical support during sexual activity
- pillows, wedges, or bolsters may be used to support body parts, allowing for endurance and protecting the
body from overstretching and fatigue.
- Sexual positions that allow support of the joints involved
should be explored.
tx strategies for clients with low endurance:
- positions that require less E (bottom or sidelying)
- timing
- plan sexual activities -
- de emphasize penetrative intercourse (mutual masturbation, oral sex)
tx strategies for clients with loss of mobility and contractures:
- activity analysis on positions that allow for sexual activity
tx strategies for clients with joint degeneration:
- avoid stress and repetitive motion on affected joints
- take weight off hips and knees
- activity analysis to see what position requires the least amount of strain (ex: sidelying, missionary)
tx strategies for clients with cardio-vascular system challenges:
▪A normal sexual response leads to:
-- increased heart rate
--Increased blood pressure
▪Consult with physician regarding risks
▪Educate patient on ways to monitor
tx strategies for clients with incontinence:
▪Avoid positions that exert pressure on bladder
▪Void before initiating activity
▪Condoms to contain leakage
▪Adhere to timed-voiding schedule
▪Preparation in case of accidents (towels, sheets)
tx strategies for clients with hemiparesis:
▪Side lying on hemiparetic side
-Uninvolved UE is able to touch
-Position provides support
-Permits active movement
-Attention focused on unaffected side
▪Positions for decreased motor control
-Side lying
-Superior or inferior; active or passive
tx strategies for clients with pain:
- schedule for time of day with less pain present
- communicate and educate partner
- explore different positions
- take medication
tx strategies for clients with sexual disinhibition:
▪Sexual "filters" become impaired
▪Address inappropriate behavior immediately
▪Identify special "cue" (Word, Gesture)
▪Explicit statements of appropriate behavior in anticipation of social environment
tx strategies for clients with cognitive/perceptual deficits:
▪Simple positions are recommended (Routine movement = less cognitive demand)
▪Calendar logs for memory impairment
▪Teach partner about unilateral neglect
▪Nonverbal communication for aphasia
▪Changes in sexual initiation role
tx strategies for clients with loss of sensation:
- compensate w/ other input
- be weary of warning signs for pain
- A lack of sensation may be a sign of disruption of the reflex loop responsible for sensation and erections in the male and sensation and lubrication in the female.
- prevention of skin breakdown
Cognitive Impairments and Behavioral Changes that may affect sexual functioning
1) - or + sex drive
2) impulsivity
3) poor initiation
4) attention
5) multitasking
6) memory deficits
7) decreased awareness
8) impaired EF
emotional factors that may affect sexual functioning
1) aging and sexuality
2) isolation
3) medication (side effects)
4) performance anxiety
5) skin care (rubbing + pressure = ulcers)
6) lubrication
7) erection (relfelxogenic erections, injections, other methods)
reflexogenic erection
erection cause by stimulating a reflex loop
Rubbing the penis, the thighs, or the anus can be effective ways to evoke a reflexogenic erection.
t/f If the normal reflex arc is interrupted, it is usually not possible to achieve an erection, and alternative methods must be explored
true
t/f a woman's ability to have children is usually affected once menstruation resumes when having a TBI or spinal cord injury
fale!
but it should be noted that depending on
the disability, women may be subject to certain pregnancy-related complications, and those should be discussed with a physician prior to considering pregnancy.
Because most disabling conditions do not impair fertility (especially
for women), it is important for the client to be aware of
birth control and potential complications of the use of birth control
Catheter care is a concern, especially when hand function is impaired. How should we educate the client to engage in sexual activity with an indwelling catheter?
- no pressure on the bladder (positions)
- void before sexual activity
- do not restrict urine flow for more than 30 minutes
- do not drink fluids for at least 2 hours before
To assess the client's positioning needs, the therapist must:
analyze the demands of the particular activity
This analysis entails looking at the physical, psychological, social, cultural, and cognitive aspects of the client's functioning.
Examples of adaptive aids:
▪Decreased grasp
--Velcro attachment on vibrator
--Masturbation sheath for male
▪Pillows or bolsters for positioning
--Particularly with hypotonia
▪Discuss sexual preferences with patient and partner
▪Use activity analysis to adapt commercially available devices