NR507 Chamberlain: Advanced Patho Final With 100% correct answers + rationales 2026
1/87
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
88 Terms
Acute Renal Failure
- Sudden loss of kidney function.
- Reversible.
What is the best indicator of a good prognosis for recovery from acute renal failure?
Kidneys respond well to Furosemide
Acute Pyelonephritis- Pathophysiology
"Upper UTI"
- Bacteria enter & colonize in urethra and bladder
- Inflammation and immune response
- Bacteria multiply and ascend to kidneys and colonize
- If still untreated: bacteria can spread into circulation via renal veins causing bacteremia & septic shock
Acute Pyelonephritis- Assessment
- Diagnosing by clinical symptoms alone can be difficult (similar to cystitis- lower tract).
- S/S: flank pain, abdominal tenderness, fever.
- Severe infection: systemic signs: high fever, chills, tachycardia.
Acute Pyelonephritis- Diagnosis
- Urinalysis: positive urine culture with significant bacteriuria and the presence of pyuria. WBC casts indicates pyelonephritis, but may not always be present.
- CBC: can show an elevated WBC, indicating infection.
- Imaging studies: renal ultrasound or CT scan, can help identify structural abnormalities and complications like abscess formation or obstruction.
Acute Pyelonephritis- Treatment
- Antibiotics
- Supportive care: adequate hydration and analgesics (NSAIDs)
- Hospitalization: severe cases, pregnant women, individuals w/underlying comorbidities, or those unable to tolerate oral intake may require hospitalization for IV antibiotic therapy and close monitoring.
- Follow-up: crucial to monitor treatment response, complete full course of antibiotics, and ensure resolution of infection through follow-up visits and repeat urine cultures.
Renal Calculi (kidney stones)- Pathophysiology
- Supersaturation: urine becomes oversaturated with certain substances like calcium.
- Nucleation: crystals act as nucleation sites, where further crystal deposition can occur.
- Crystal retention: urinary stasis or inadequate urine flow allows crystals to remain in the urinary tract.
- Stone growth and composition: overtime, crystals accumulate and grow into stones.
Renal Calculi- Assessment
- Medical hx: identify risk.
- Physical exam: flank or abdominal pain, costovertebral angle (CVA) tenderness, hematuria
- Imaging studies: crucial for assessing the presence, size, location, and composition of stones: CT scan, renal ultrasound, or X-ray.
- Lab tests: urinalysis (blood, crystals, or infection), blood tests evaluate renal function and identify metabolic abnormalities.
Renal Calculi- Treatment
- Conservative treatment for stones <5mm that are asymptomatic or causing mild symptoms.
- Medical management: thiazide diuretics (calcium stones) or allopurinol (uric acid stones).
- Stone removal (lithotripsy) for larger stones (>5mm) or stones causing severe symptoms.
Renal Calculi: Goals of Treatment
- Manage acute pain
- Promote passage of stone
- Reduce the size of stone already formed
- Prevent new stone formation
Chronic Kidney Disease (CKD)
- Progressive, irreversible loss of kidney function.
- Associated with systemic diseases such as hypertension, diabetes mellitus (most significant risk factor), systemic lupus erythematosus, or intrinsic kidney disease.
- Once stage IV is reached, progression to stage V is inevitable (plus dialysis or kidney transplant).
CKD- Candidates for Dialysis
- Based on symptoms, kidney function, overall health status, and individual circumstances.
- Symptomatic uremia.
- Fluid overload and hypertension.
- Hyperkalemia.
- Acid/base imbalances.
- Progressive loss of kidney function.
5 Stages of CKD
- Determined by estimates of GFR and albuminuria.
- Stage 1: kidney damage with normal or increased GFR (eGFR 90-100 mL/min).
- Stage 2: kidney damage with mild decrease in GFR (60-89 mL/min).
- Stage 3: moderate decrease in GFR (30-59 mL/min).
- Stage 4: severe decrease in GFR (15-29 mL/min).
- Stage 5: kidney failure, end stage (<15)
Gastroesophageal Reflux Disease (GERD): Pathophysiology
- Lower esophageal sphincter (LES) dysfunction: reduced pressure or improper relaxation allows gastric acid to flow back into the esophagus.
- Hiatal hernia: contributes to GERD by disrupting the normal barrier between the esophagus and stomach.
- Esophageal motility disorders: impaired esophageal peristalsis and reduced esophageal clearance can lead to pooling of gastric acid in the esophagus.
- Acidic gastric contents.
GERD- Assessment
- Subjective: heartburn (burning sensation in chest), regurgitation (acidic taste in mouth), dysphagia (difficulty swallowing), chest pain (may mimic cardiac chest pain).
- Objective: usually normal in uncomplicated cases, may be signs of esophagitis or other complications in severe cases.
Warning signs of GERD
- Symptoms over the age of 50
- Dysphagia (difficulty swallowing food)
- Odynophagia (pain with swallowing)
- Nausea and vomiting
- Weight loss
- Melena (dark, tarry stools)
- Early satiety
GERD- Diagnosis
- Clinical symptoms
- Response to empiric therapy
- Diagnostic tests: if symptoms are severe or persistent: upper GI endoscopy, esophageal pH monitoring, and esophageal manometry
GERD- Treatment
- Lifestyle modification: weight loss, elevate HOB, avoid food 2-3 hr before bedtime, avoid trigger foods (caffeine, chocolate, alcohol, spicy/acidic).
- Medications: antacids, H2 receptor antagonists, proton pump inhibitors, prokinetic agents (improve esophageal motility).
- Surgery.
Hiatal Hernia
- Diaphragmatic hernia with protrusion of the upper part of the stomach through the diaphragm and into the thorax d/t dilation of the gastroesophageal junction (GJ).
Sliding Hiatal Hernia
- Type of hiatal hernia where the stomach and the top of the esophagus slide up into the chest through the diaphragm.
Hiatal Hernia- Assessment
- Diaphragmatic weakness
- Symptoms: often asymptomatic. S/S can develop later in life and are associated with GI disorders like GERD (heartburn, regurgitation, dysphagia, epigastric pain).
- Contributing factors: aging, obesity, pregnancy, increased intra-abdominal pressure (chronic coughing or valsalva maneuver), structural abnormalities of the diaphragm.
Hiatal Hernia- Diagnosis
- Upper GI barium swallow or EGD
Hiatal Hernia- Treatment
- Lifestyle modification (similar to GERD: small meals, no food 2-3 hr before bed, chew thoroughly, avoid trigger foods, lose weight).
- Medications: antacids, prokinetic agents.
- Surgery
Duodenal Ulcer
- An ulcer, or erosion, in the wall of the duodenum of the small intestine (uppermost part, just after the stomach).
- Patho: H. Pylori (most common), gastric acid hypersecretion (NSAIDs & smoking), impaired mucosal defense mechanisms, disruption of the balance between aggressive and defensive factors.
Duodenal Ulcer- Assessment
- Medical history
- Symptoms: characteristic manifestation: chronic intermittent pain in the epigastric area, worse on empty stomach/decreases after eating. Not unusual for pain to occur in the middle of the night and disappear by morning.
- Physical exam
Duodenal Ulcer- Diagnosis
- Upper GI endoscopy
- H. Pylori testing
- Imaging studies
Duodenal Ulcer- Treatment
- Medications: PPIs, H2 receptor blockers, antibiotics, antacids, cytoprotective agents.
- Lifestyle modifications (NSAIDs, smoking)
- Follow-up and monitoring
Peptic Ulcer Disease
- A break or ulceration in the protective mucosal lining of the lower esophagus, stomach, or duodenum.
- Least likely to occur in the large intestine.
Peptic Ulcer Disease- Aggressive vs Protective Factors
- Aggressive factors: H. Pylori, gastric acid secretion, NSAIDs, lifestyle factors.
- Protective mechanisms: mucus and bicarbonate secretion, prostaglandins, mucosal blood flow, epithelial cell renewal.
Peptic Ulcer Disease- Assessment and Diagnosis
- Medical history: NSAID use, age >65, genetic predisposition, alcohol ingestion.
- Symptoms: gastric (pain increases after meal) or duodenal (pain decreases after meal).
- Physical exam
Peptic Ulcer Disease- Diagnostic Testing
- Endoscopy
- H. Pylori testing
- Imaging studies
Peptic Ulcer Disease- Treatment
- Medications: PPIs, antibiotics, H2-receptor antagonists, cytoprotective agents.
- Lifestyle modifications: avoidance of NSAIDs, smoking cessation, dietary changes.
- Follow-up and maintenance therapy.
Major Depressive Disorder- Pathophysiology
- Neurotransmitter imbalance: serotonin, norepinephrine, dopamine.
- Neuroendocrine deregulation: abnormalities in the hypothalamic-pituitary-adrenal axis: elevated cortisol levels.
- Inflammatory processes: chronic inflammation.
- Neuroplasticity and structural changes.
Major Depressive Disorder- Treatment
- SSRIs are the standard first-line treatment.
- Initial selection of an antidepressant includes: assessment of symptoms, age, side effects, safety, cost.
Social Anxiety Disorder- Key Features
- Fear and avoidance of social situations to the point that it affects their ability to perform daily activities.
- Ex: Anxious person may feel very uncomfortable having a conversation or interacting with others and very conscious of being scrutinized and humiliated or rejected by others.
Generalized Anxiety Disorder (GAD)
- Excessive, persistent, unreasonable anxiety about everyday situations including work, money, family, and relationships.
- Thought of getting through day can cause anxiety.
Panic Disorder
- Consists of multiple disabling panic attacks and is characterized by intense autonomic arousal: lightheadedness, tachycardia, difficulty breathing, chest discomfort, sweating, weakness, trembling, GI distress, and chills or hot flashes.
Schizophrenia- Symptoms
- Positive: hallucinations, delusions, formal thought disorder, disorganized speech, bizarre behavior.
- Negative: flat affect, alogia (lack of content in speech), anhedonia (lack of pleasure), attention deficits, apathy, avolition (decreased motivation).
- Cognitive: inability to perform daily tasks requiring attention and planning.
Schizophrenia- Diagnosis
- Advanced neuroimaging techniques have revealed structural brain abnormalities.
- A consistent finding is the enlargement of the lateral and third ventricles and the widening of frontocortical fissures and sulci.
Hypothyroidism
- Most common disorder of thyroid function.
- More common in women and elderly.
- Affects 0.1-2% of US population.
Hormone replacement therapy with ___________ is the treatment of choice for hypothyroidism.
Levothyroxine
Thyroid Stimulating Hormone (TSH)
- Signaled by thyroid-releasing hormone via the hypothalamus.
- Released from the anterior pituitary gland; causes stimulation of the thyroid, resulting in release of T3 and T4.
- Small changes are early indicators of disease & can be seen before a patient is symptomatic.
- High TSH w/ hypothyroidism & low TSH w/ hyperthyroidism.
Grave's Disease/Hyperthyroidism- Ophthalmopathy
Two categories:
1) Functional abnormalities resulting from hyperactivity of the sympathetic division of the autonomic nervous system (lag of the globe on upward gaze or lag of the upper lid on downward gaze).
2) Infiltrative changes involving the orbital contents with enlargement of the ocular muscles. Affect >50% of Grave's patients. Increased secretion of hyaluronic acid, adipogenesis, inflammation, and edema of the orbital contents result in exophthalmus, periorbital edema, and extraocular muscle weakness leading to strabismus and diplopia (double vision).
The two most distinguishing factors of Grave's disease is:
- Pretibial myxedema: thick, scaly plaques and swelling in the lower legs; skin can take on a waxy, discolored appearance.
- Exophthalmos: protrusion of the eyeballs.
Grave's Disease/Hyperthyroidism- Treatment
- Directed at controlling excessive thyroid hormone production, secretion, or action.
- Includes antithyroid drug therapy (methimazole, propylthiouracil), radioactive iodine therapy, and surgery.
- Goal of radioactive iodine ablation is to destroy overactive thyroid tissue.
Type 1 Diabetes Mellitus
- Autoimmune process
- Environmental and genetic factors trigger cell-mediated responses that destroy pancreatic beta cells.
- Environmental factors: viral infections (enteroviruses, coxsackievirus), H. pylori, exposure to cow's milk proteins, lack of vitamin D.
The diagnostic criteria for Diabetes Mellitus according to the American Diabetes Association is:
Hemoglobin A1C greater than or equal to 6.5%
Actions of Insulin
- Promotes glucose uptake mostly in the liver, muscle and adipose tissue.
Complication of Diabetes: Autonomic Neuropathy: GI Symptoms
- decreased esophageal motility
- gastroparesis
- delayed gastric emptying
Hypoglycemia- Symptoms
- Tachycardia
- Palpitations
- Diaphoresis
- Tremors
- Pallor
- Anxiety
Hyperparathyroidism
- High parathyroid hormone (PTH).
- Primary: usually caused by parathyroid gland tumor. Labs: high calcium, low/normal phosphate.
- Secondary: in response to hypocalcemia, usually caused by chronic kidney disease. Labs: low/normal calcium, high phosphate.
(As PTH increases, it can lead to hypercalcemia)
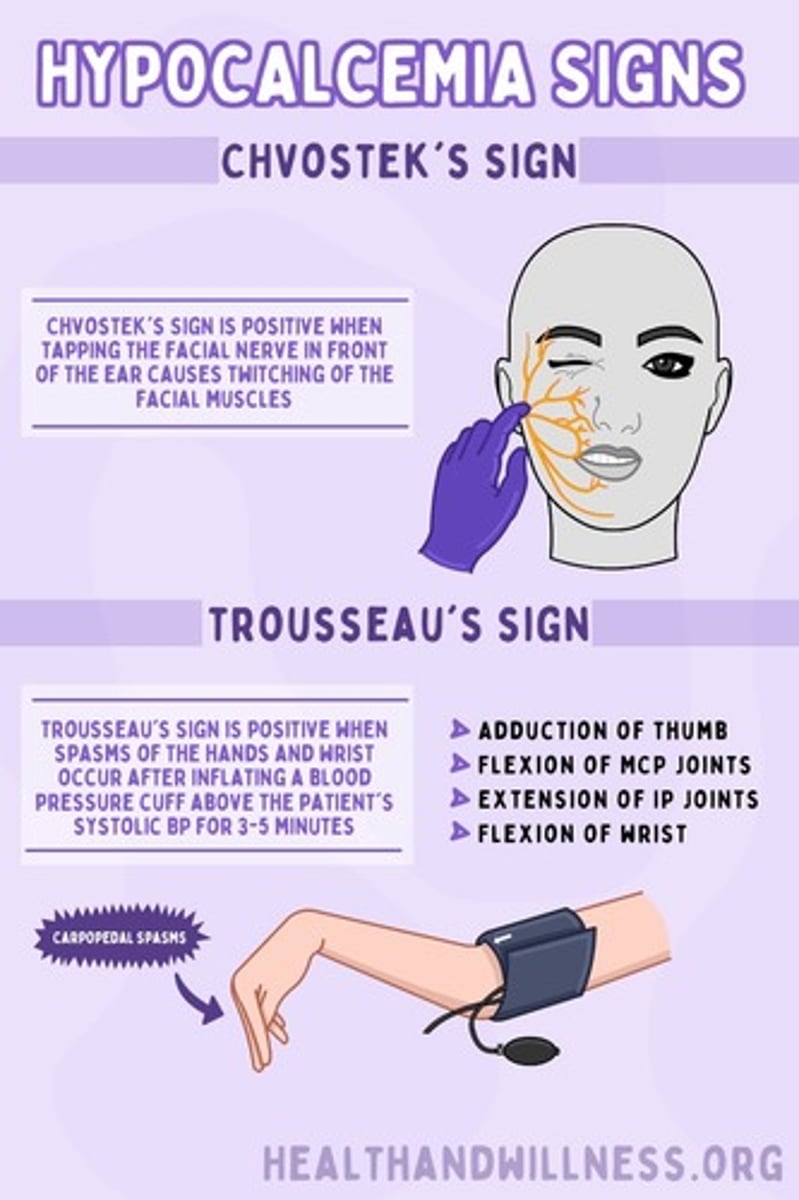
Hypercalcemia
- Hypercalcemia (and hypophosphatemia) may be asymptomatic or affected individuals may present with symptoms related to the neuromuscular changes that include paresthesia and muscle cramps.
- Can have low bone density (osteoporosis) that is most noted in the distal one-third of the radius.
- Other issues: kidney stones, pathological fractures, ventricular hypertrophy, depression, gastric issues.
Hypoparathyroidism
- Low magnesium inhibits parathyroid hormone (PTH) secretion.
- Hypomagnesemia may be related to: chronic alcoholism, malnutrition, malabsorption, increased renal clearance of magnesium caused by the use of amino-glycoside antibiotics or certain chemotherapeutic agents, or prolonged magnesium-deficient parenteral nutritional therapy.
Hypocalcemia- Symptoms
- Dry skin
- Loss of body and scalp hair
- Hypoplasia of developing teeth
- Horizontal ridges on the nails
- Cataracts
- Basal ganglia calcifications
- Bone deformities
- Bowing of the long bones
Hypercortisolism- Pathophysiology
Adrenal Tumors-
- produces cortisol independent of the normal regulatory mechanisms of the HPA axis.
- suppression of ACTH: due to high cortisol levels that exert negative feedback on the pituitary gland and hypothalamus which inhibits secretion of ACTH.
Pituitary tumors (Cushing's disease)-
- hypercortisolism caused by a pituitary tumor that secretes excess ACTH.
Glucose & Hypercortisolism
- Glucose intolerance is associated with hypercortisolism.
- Glucose intolerance occurs because of cortisol-induced insulin resistance and increased gluconeogenesis and glycogen storage by the liver.
Cushing's syndrome is characterized by:
- Patterns of fat deposition described as "truncal [central] obesity", "moon face", and "buffalo hump".
Hypocortisolism- Adrenal Crisis
- Insufficient cortisol production.
- Lack of aldosterone.
- Stress response failure.
- Fluid and electrolyte imbalances: hyponatremia, hypoglycemia, hyperkalemia, hypovolemia.
- Adrenal crisis triggers: infection, surgery, trauma, sudden discontinuation of corticosteroid therapy.
The onset of adrenal crisis is signified by-
- Hypotension
- Can progress to complete vascular collapse and shock.
Adrenal Crisis develops due to-
- undiagnosed disease, acute withdrawal of glucocorticoid therapy, or the occurrence of infection or other comorbid stressful events.
Lab work that indicates primary hypocortisolism (Addison's disease)
- Serum and urine levels of cortisol are depressed, and adrenocorticotropic hormone (ACTH) levels are increased.
When prescribing cortisol, the NP should keep in mind-
- With acute stressors (infection, surgery, or trauma), additional cortisol must be administered to approximate the amount of cortisol that might be expected to be secreted if normal adrenal function were present.
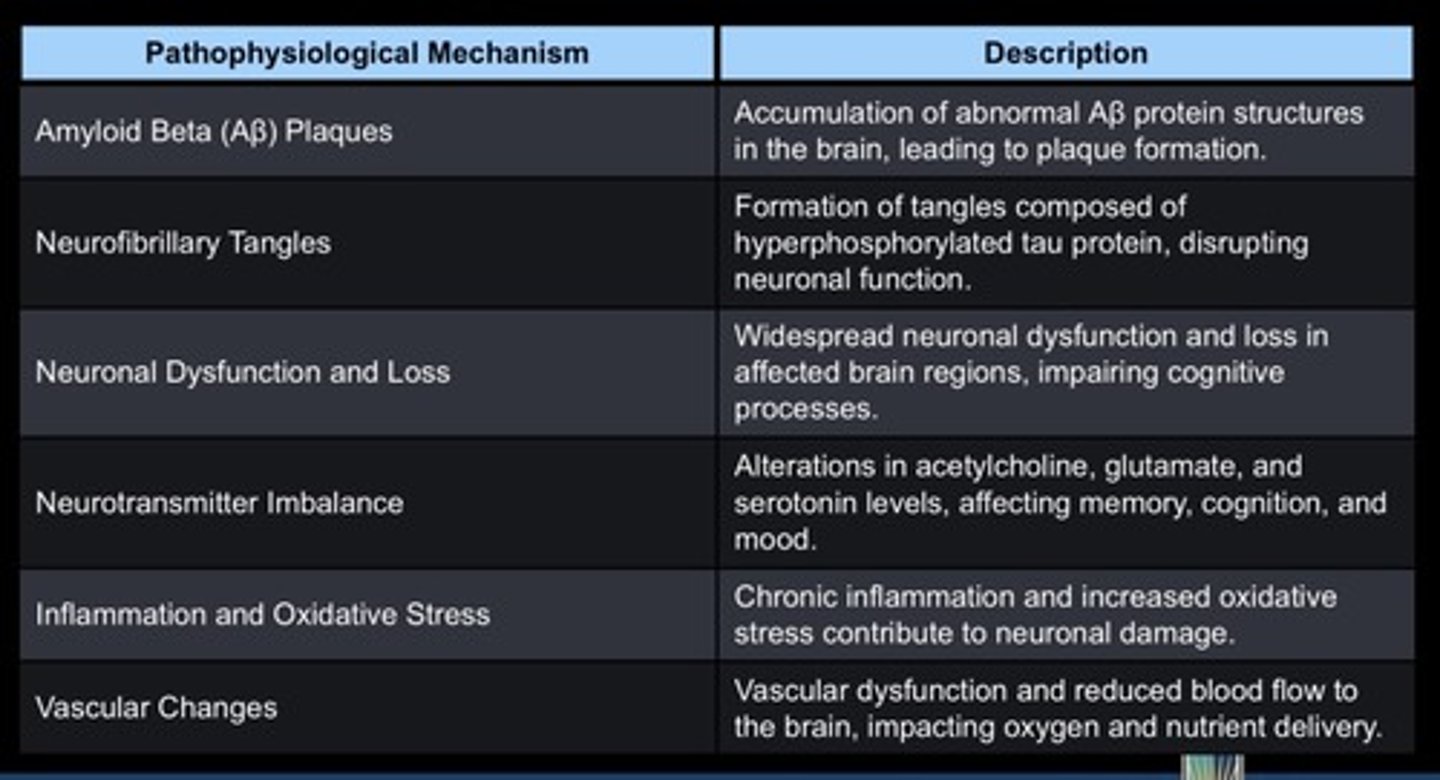
Alzheimer's Disease
- Neurodegenerative disease.
- Progressive disorder associated with impaired cognitive function and cortical skills.
- Decreased short term memory (hippocampus shrinkage). Once atrophy reaches cortical regions, long-term memory can become altered.
Alzheimer's Disease- Pathophysiology
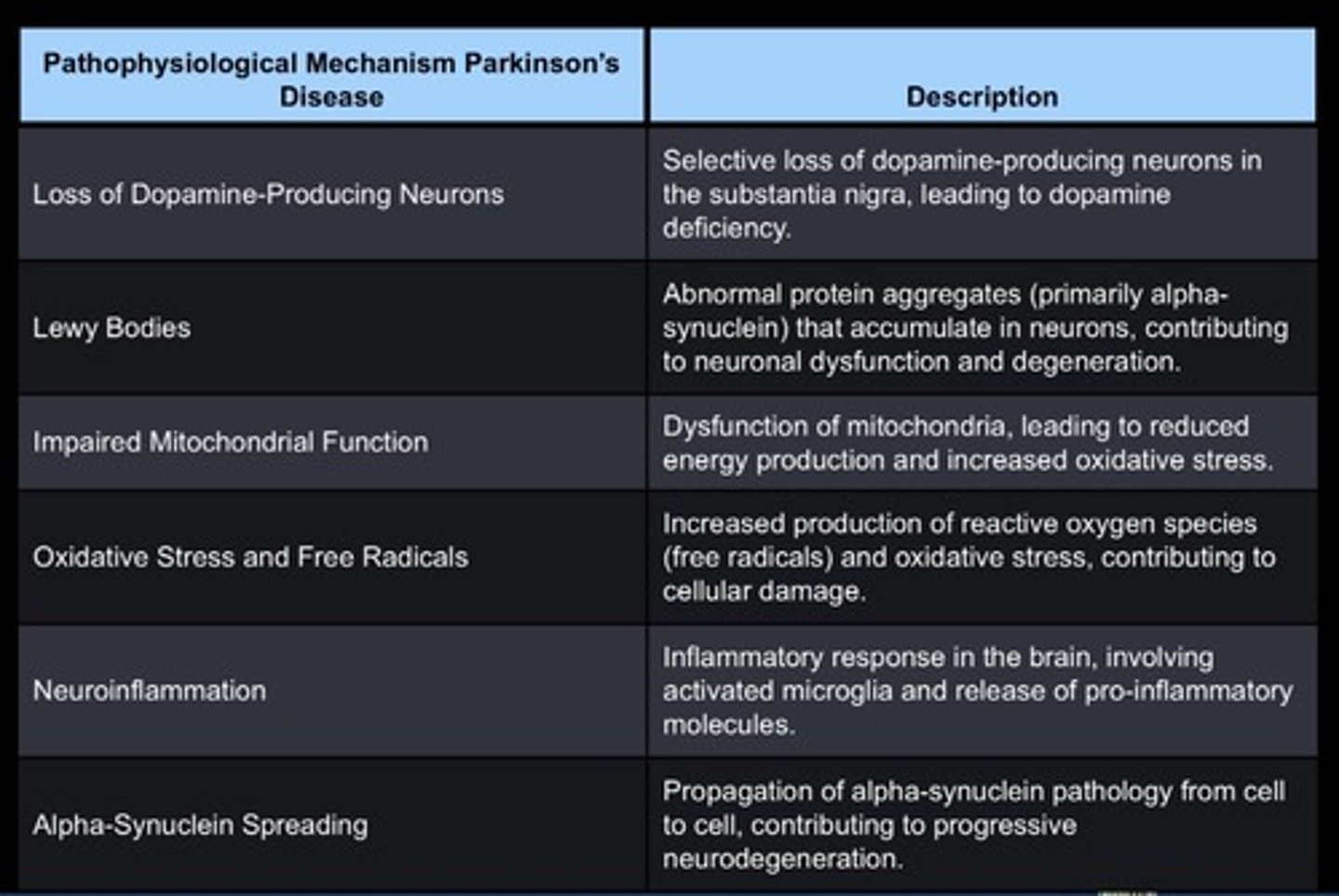
Parkinson's Disease
- Progressive movement disorder where dopamine-producing areas of the brain undergo neuron degeneration.
Parkinson's Disease- Pathophysiology
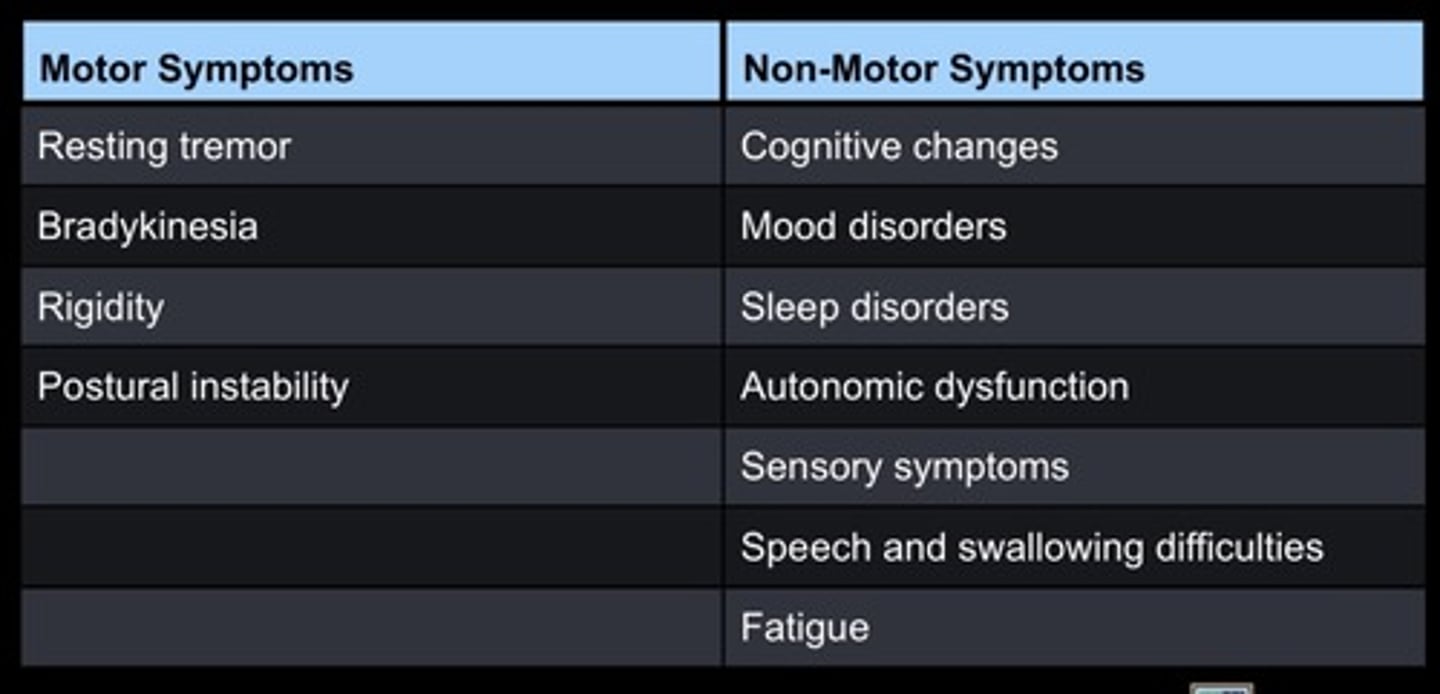
Parkinson's Disease- Signs and Symptoms
- Bradykinesia-> shuffling gait.
- Speech (dysarthria) and swallowing (dysphagia) difficulties.
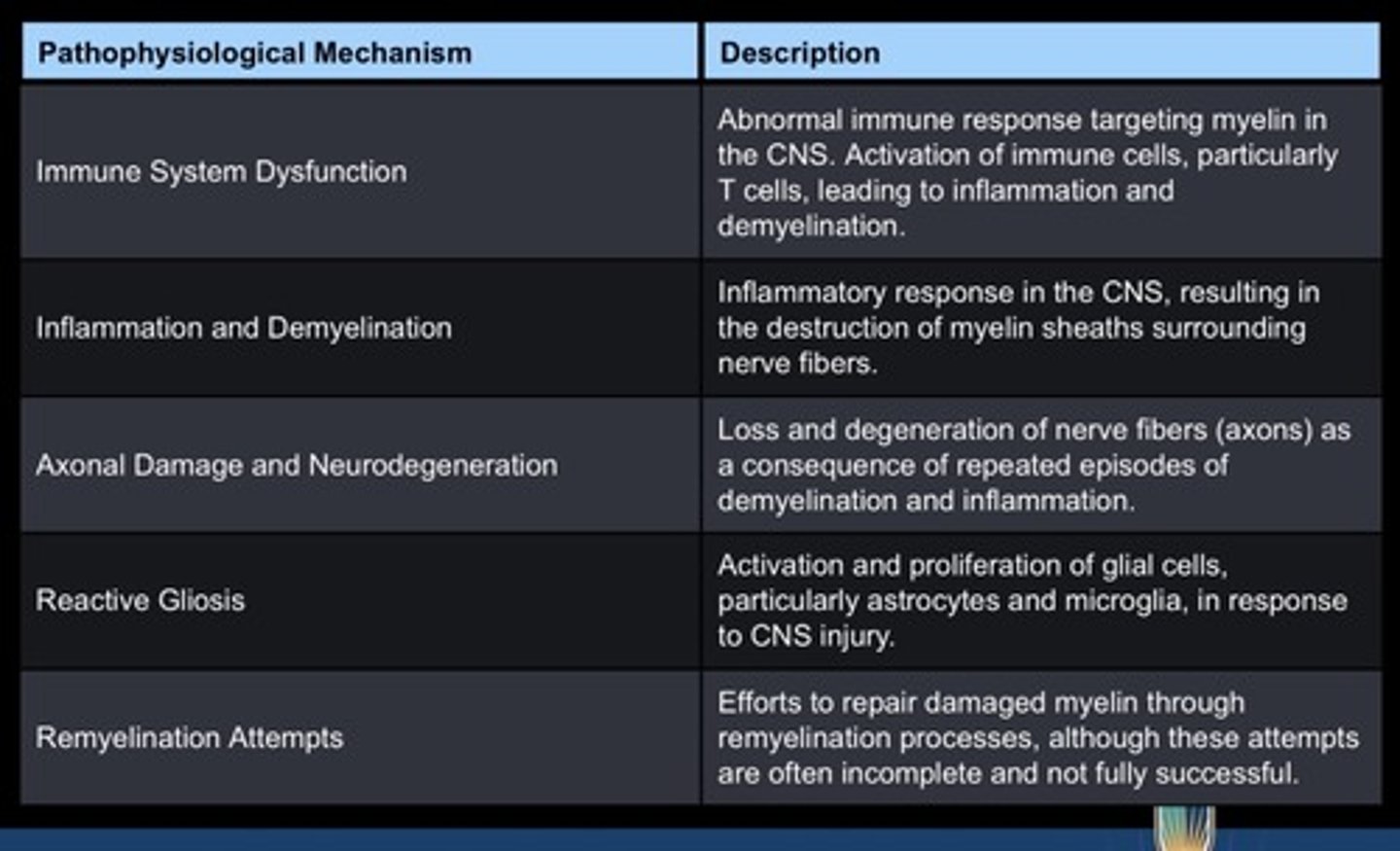
Multiple Sclerosis
- Demyelinating disease of the CNS (brain and spinal cord).
- Risk factors: smoking, vitamin D deficiency, and EBV.
Multiple Sclerosis- Pathophysiology
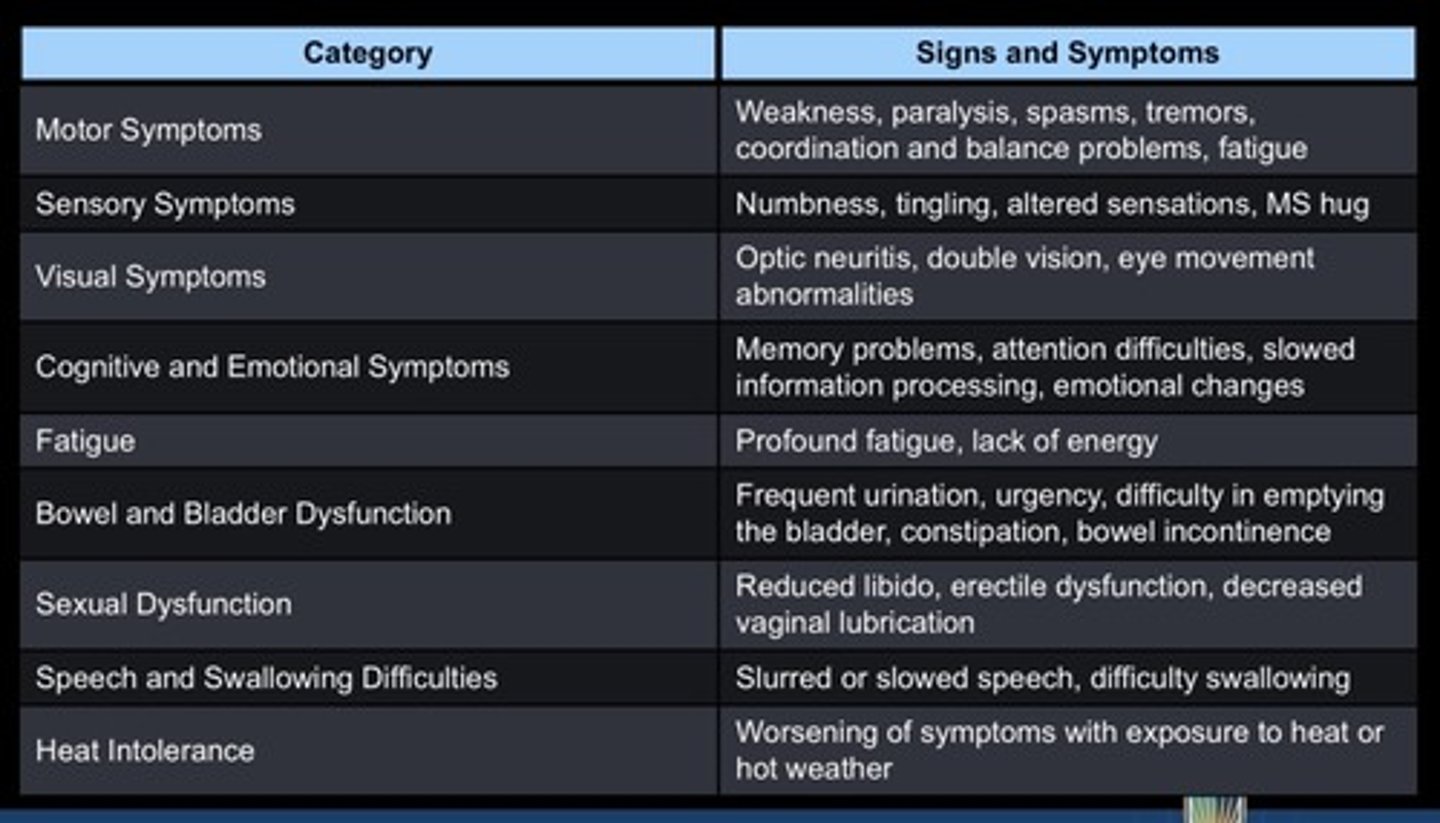
Multiple Sclerosis- Signs and Symptoms
MS hug = a feeling of tightness or pressure around the chest or stomach
One possibility for the development of febrile seizures is that-
- neurons are excited by decreased carbon dioxide (CO2) levels caused by hyperventilation during a febrile state.
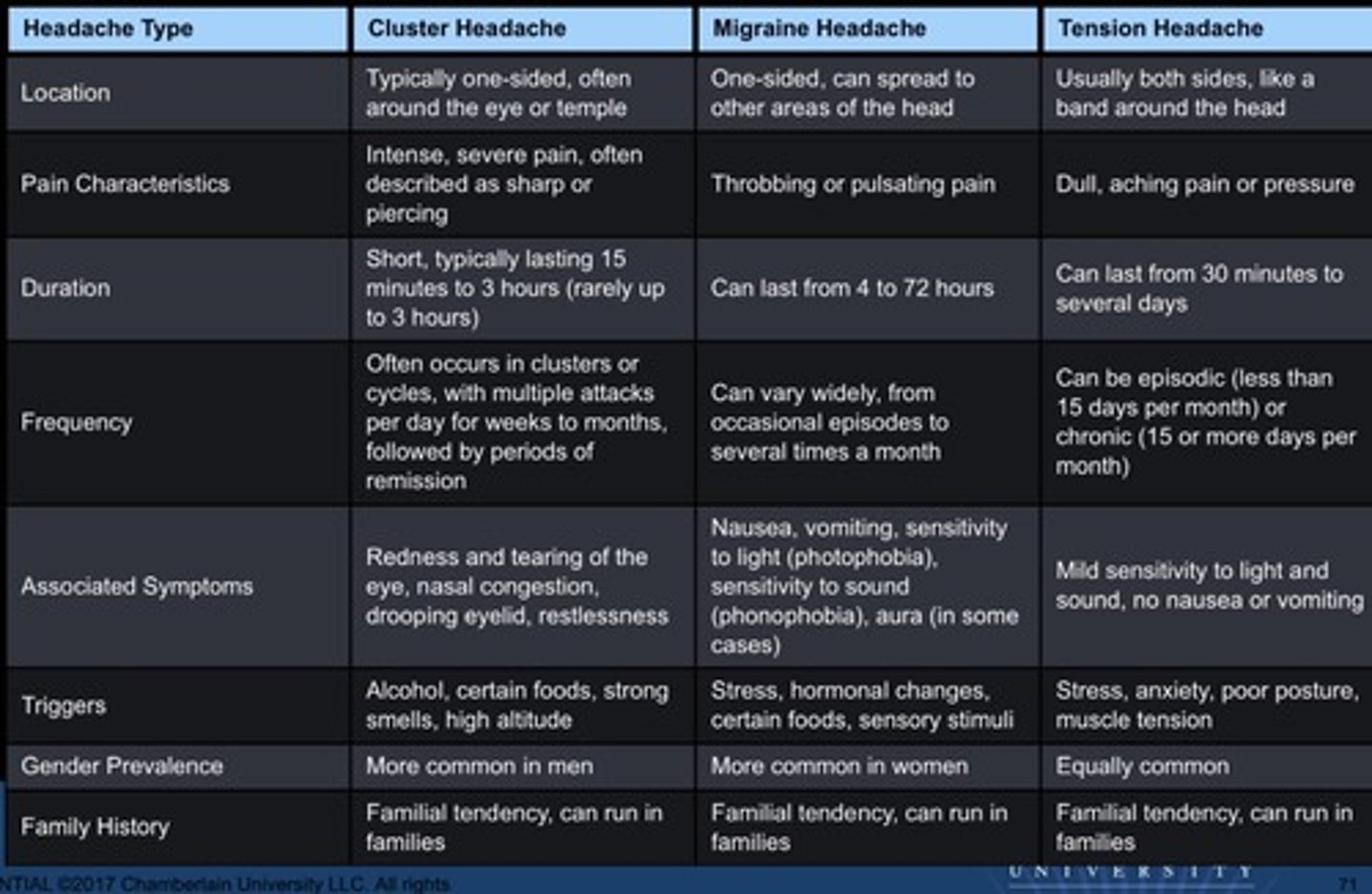
Cluster Headache
- Characterized by unilateral trigeminal distribution of severe pain with ipsilateral autonomic manifestations, including tearing and ptosis (upper eyelid drooping) on the affected side, and congestion of the nasal mucosa.
- Primarily in men between 20-50 years of age.
- Pain may alternate sides with each headache episode and is severe, stabbing, and throbbing.
- Pain is often referred to the midface and teeth.
Migraine Headache
- An episodic neurologic disorder whose marker is headache lasting 4-72 hours.
- Diagnosed when any two of the following features occur: unilateral head pain, throbbing pain, pain worsens with activity, moderate or severe pain intensity. And at least one of the following: nausea, vomiting, photophobia, phonophobia.
- Types: 1) migraine without aura (most common), 2) migraine with aura with visual, sensory, or motor symptoms, 3) chronic migraine.
Tension Headache
- Mild to moderate bilateral headache with a sensation of a tight band or pressure around the head.
- Most prevalent type of recurrent headache.
- Not vascular or migrainous.
- Average age of onset is during the second decade of life.
Comparison of Headaches
Bell's Palsy
- Associated with cranial nerve VII (facial nerve) paralysis.
- Results in facial asymmetry and inability to close eye, smile, or frown on affected side.
Trigeminal Neuralgia
- Associated with compression of cranial nerve V (trigeminal nerve).
- Results in severe and sharp stabbing pain that can worsen with chewing.
Bacterial Meningitis
- Inflammation of the meninges (layers that surround and protect the brain) caused by a bacteria.
- Characterized by s/s of systemic infection: fever, tachycardia, and chills.
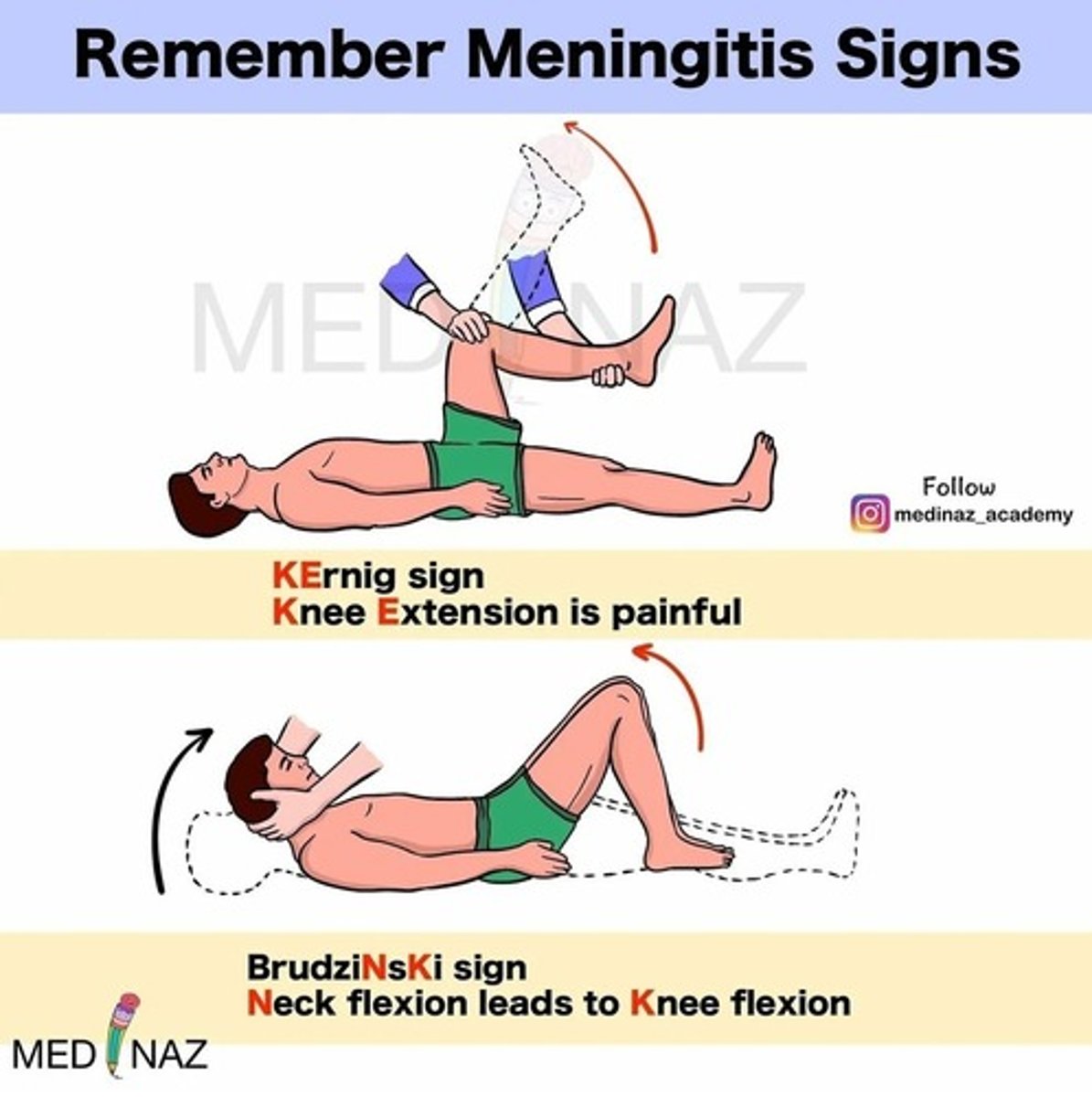
- S/S of meningeal irritation: severe throbbing headache, severe photophobia, nuchal rigidity, positive Kernig sign (resistance to extension of the leg while hip is flexed), and positive Brudzinski sign (flexion of the hips and knees when the neck is flexed).
Meningitis: Kernig's and Brudzinski's signs
Anterior Cerebral Artery (ACA) Infarct Symptoms
- Motor and sensory deficit (lower extremities: leg & foot, slight upper extremity involvement, contralateral).
- Urinary incontinence.
- Abulia (lack of will).
Middle Cerebral Artery Infarct Symptoms
- Motor and sensory deficit (upper extremities and face, contralateral, decreased conjugate gaze-inability to move both eyes together, homonymous hemianopia- decreased vision on one half of both sides).
- Dominant side symptoms (aphasia).
- Non-dominant side symptoms (neglect, anosognosia- patient is unaware of their neurological deficit)
Lateral Medullary Syndrome (Wallenberg)
- Involves posterior-inferior cerebellar artery.
- Face symptoms will be ipsilateral to the lesion (same side), body symptoms will be contralateral (opposite side).
- Symptoms: face (pain, numbness, nystagmus, diplopia), body (decreased pain & temp sensation in lower extremities), vertigo, n/v, dysphagia, hoarseness, decreased gag reflex.
Medial Medullary Syndrome
- Involves anterior spinal artery
- Face symptoms will be ipsilateral to the lesion (same side), body symptoms will be contralateral (opposite side).
- Symptoms: face (tongue paralysis), body (paralysis of the entire body on the affected side and decreased proprioception).
Basilar Artery Syndrome
-"Locked in syndrome": patient cannot move or talk, but their sensory functions are intact. Only motor movement is eye movement.
- Contralateral loss of vibratory sense, sense of position with dysmetria (lack of coordination of movement), loss of two-point discrimination, impaired rapid alternating movements.
Rosacea
- Chronic skin disorder of the face with red inflamed areas appearing mostly on the nose and cheeks.
- Familial tendency; several genes have been identified.
- Neurovascular dysregulation, infection, and factors that trigger altered innate and adaptive immune response are involved. Ex- chronic sun exposure and damage, heat, drinking alcohol or hot beverages, hormone fluctuation, mites colonization, mental stress, anxiety.
The most aggressive skin cancer is-
- Melanoma
What impacts melanoma prognosis?
Thickness of the lesion
The typical lesion of plaque psoriasis is-
- a well-demarcated, thick, silvery, scaly, erythematous plaque surrounded by normal skin that can appear anywhere on the body.