Hemodialysis AV Fistulas
1/44
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
45 Terms
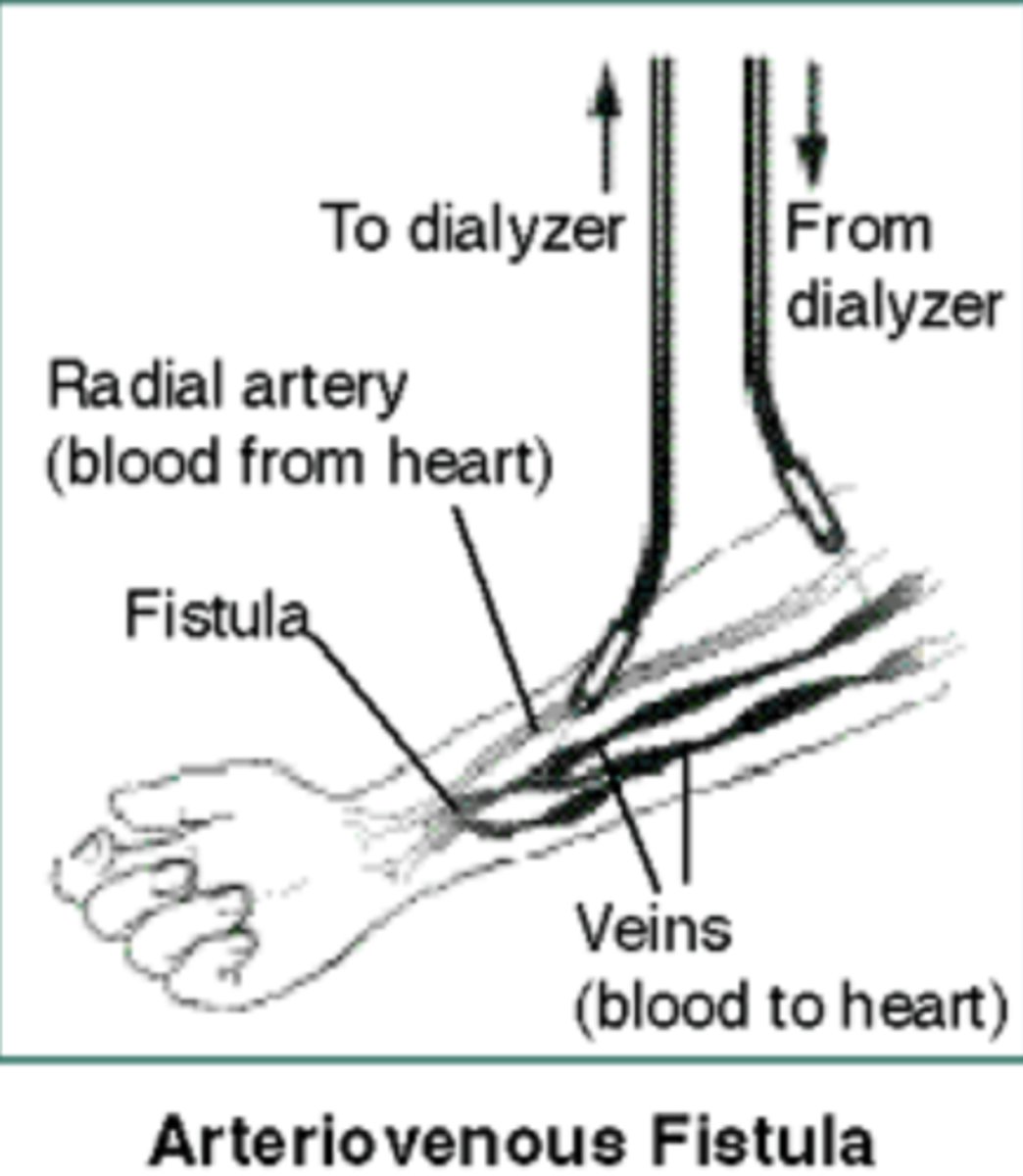
Hemodialysis AV Fistula
Anastomosis of artery & vein
Reliable, repeatable hemodialysis access with minimal complications
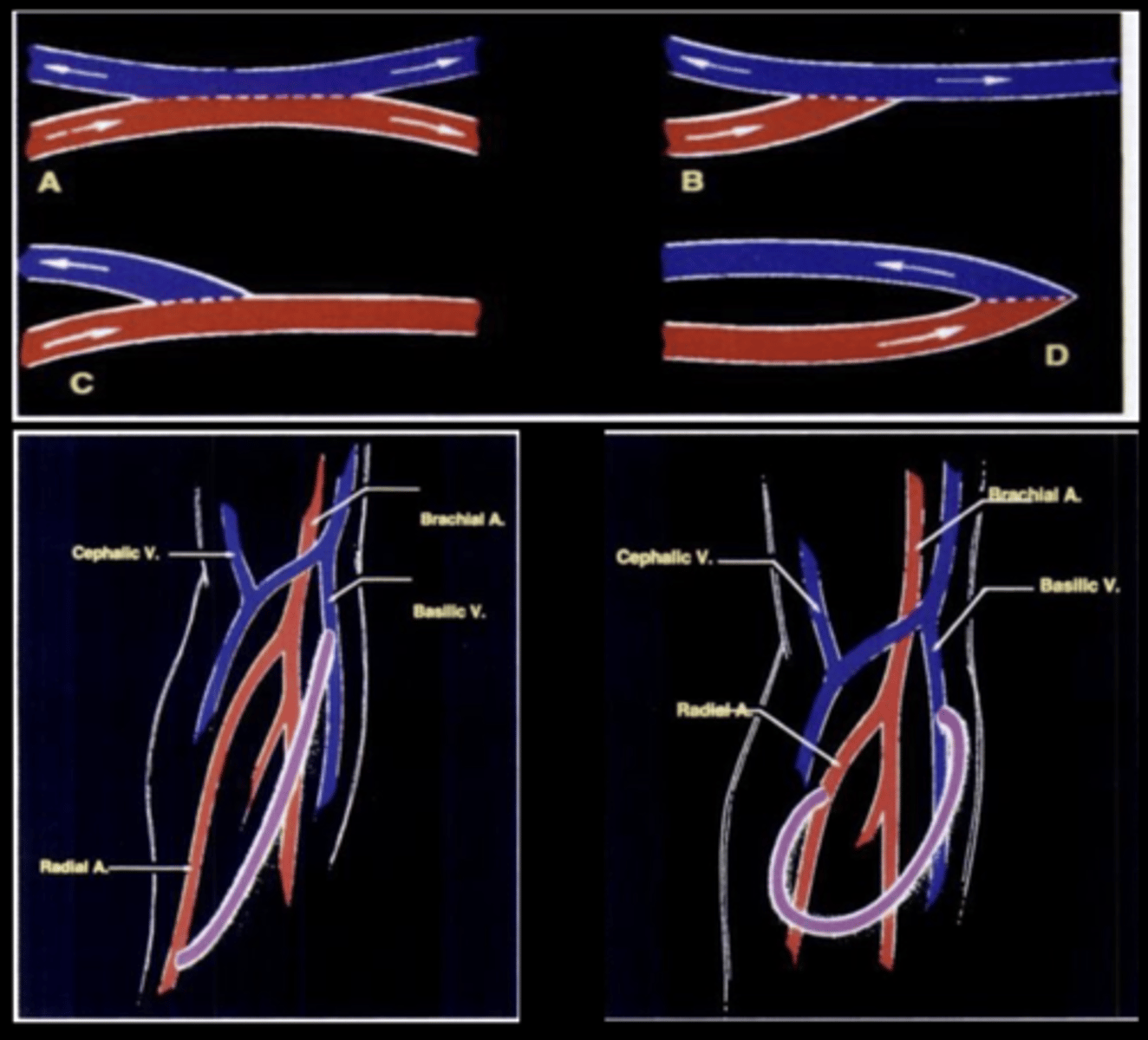
Types of Anastomoses
Site Preferences for AV Fistula
Non dominant forearm
Dominant forearm
Non dominant upper arm
Dominant upper arm
Lower extremity
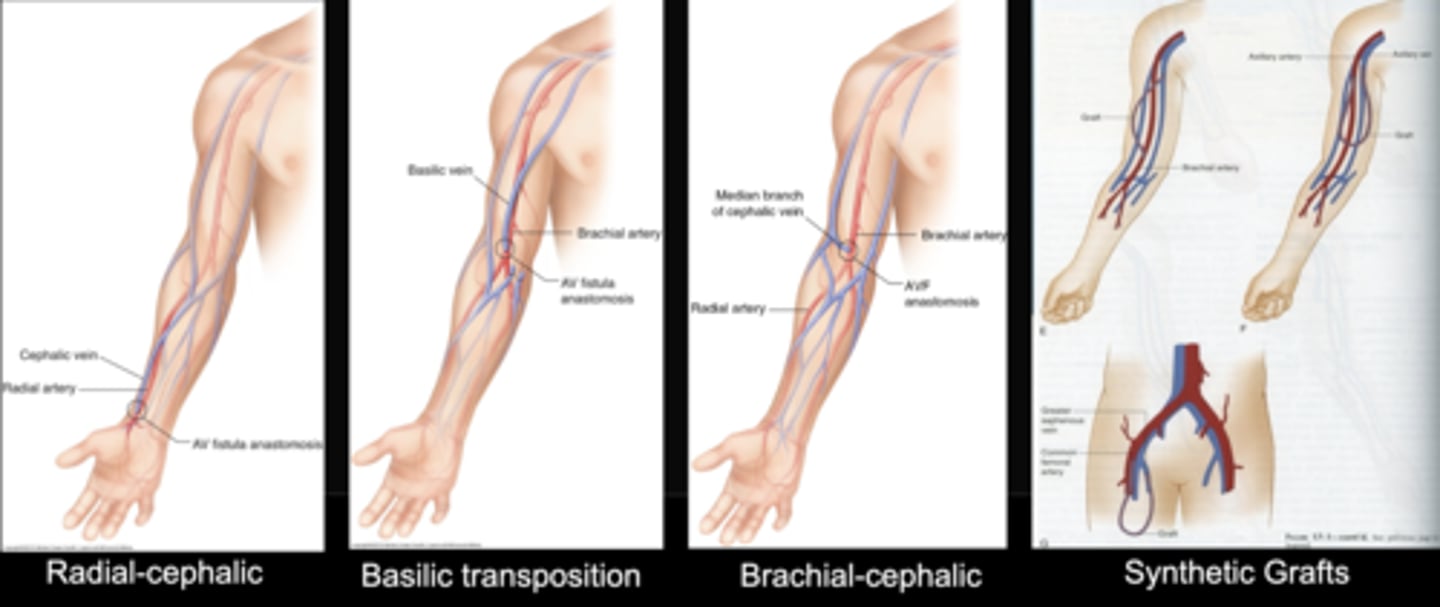
Preferred Site for AV Fistula
As distal as possible in non-dominant arm
Why is the upper extremity preferred for AV fistulas?
Patient comfort & preference
Lower infection rates
Greater longevity
Easier to access
Patient Prep & Assessment
Keep room warm
Patient in supine/sitting position
Take bilateral blood pressures
Take pulses of brachial, radial, and ulnar arteries
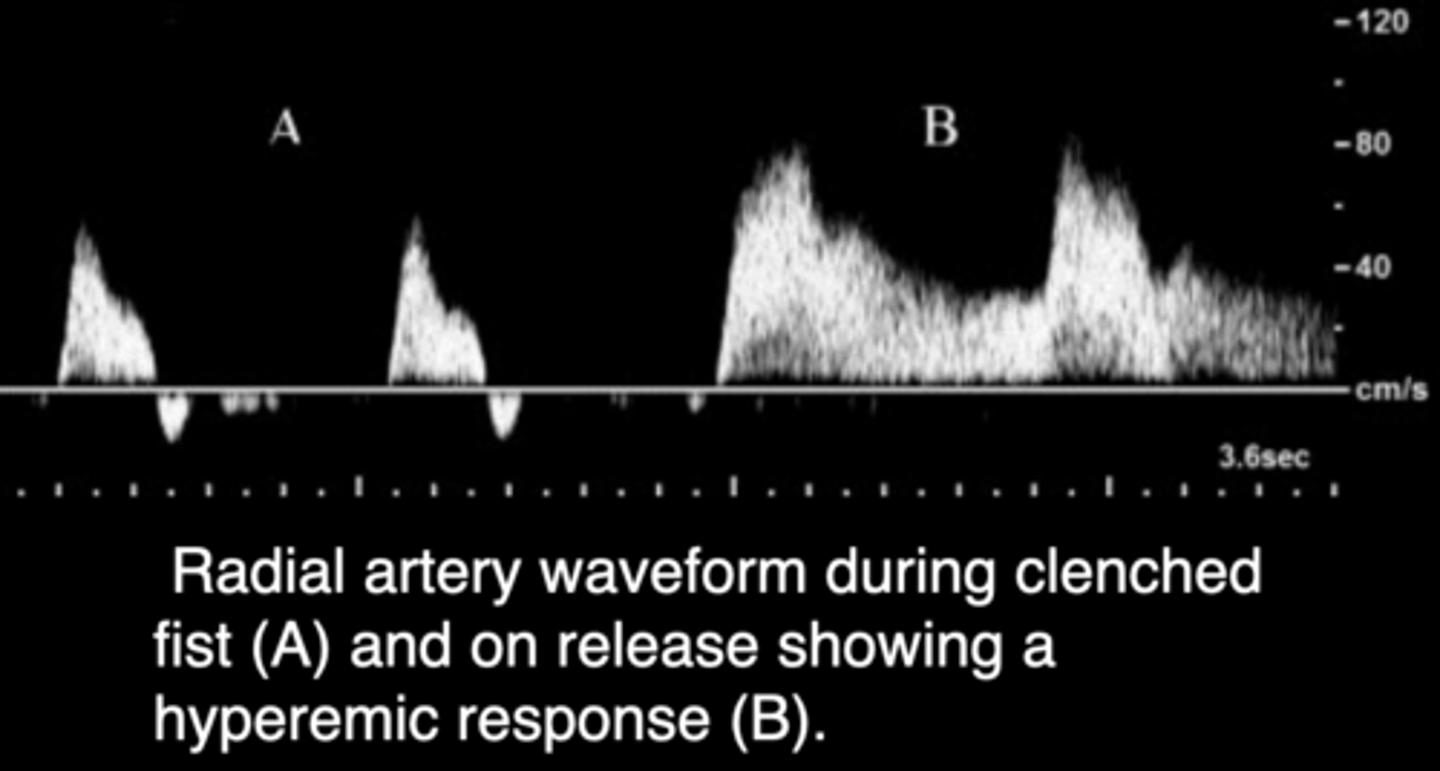
Allen Test: assesses for intact palmar arch - clenched fist - reactive hyperemia after compression indicates patency
Assess superficial veins using tourniquets
Fistula Maturation Failure
Caused by obligatory use of small/suboptimal veins
Quality of Artery
Determines capacity to dilate & accommodate increased flow
Fistula/Graft Mapping
Find suitable artery before moving onto venous system
AV Fistula & Hemodialysis Graft Arterial Mapping
Start with distal forearm of non-dominant arm
Assess for plaque, thickening, stenosis, compliance
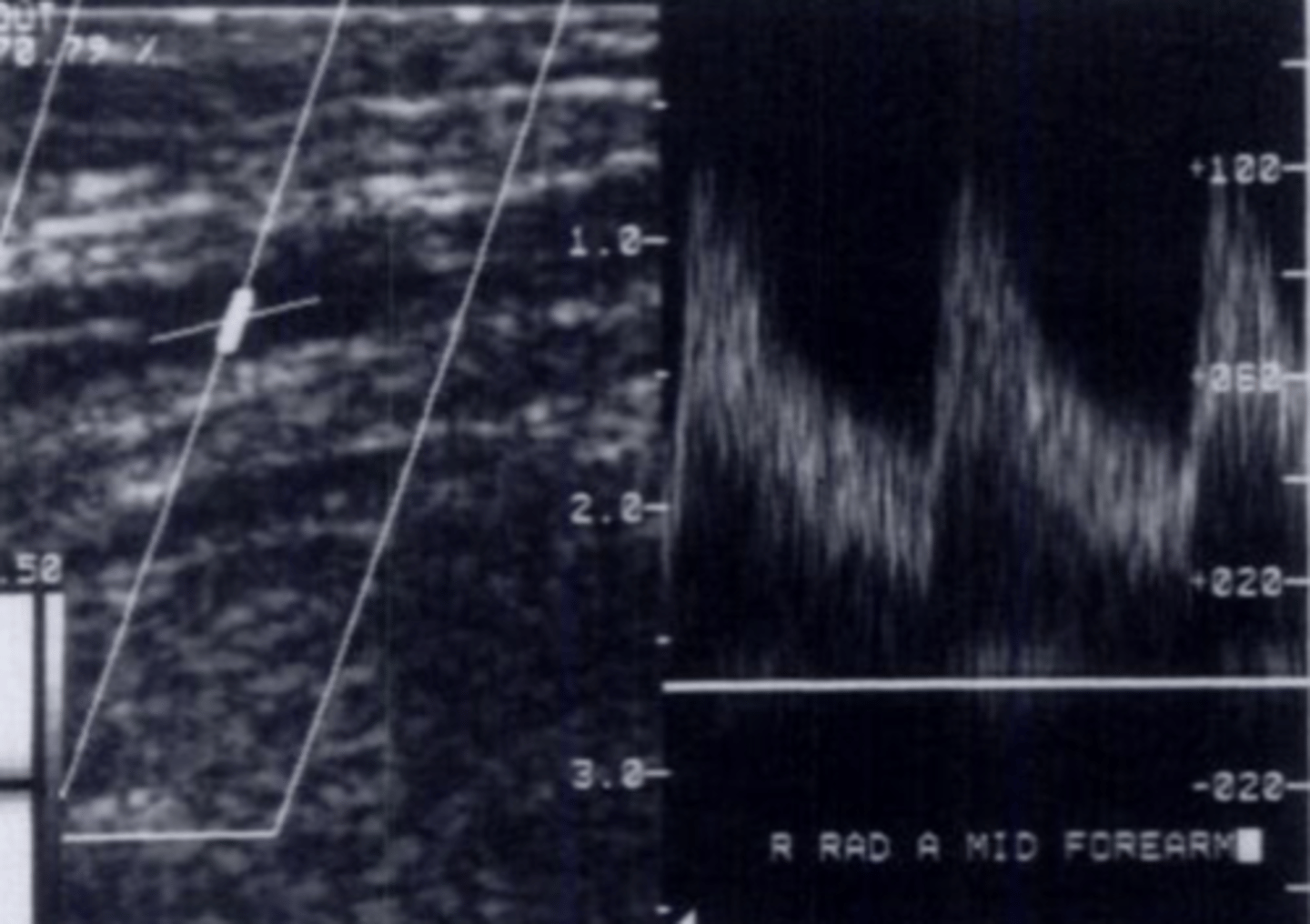
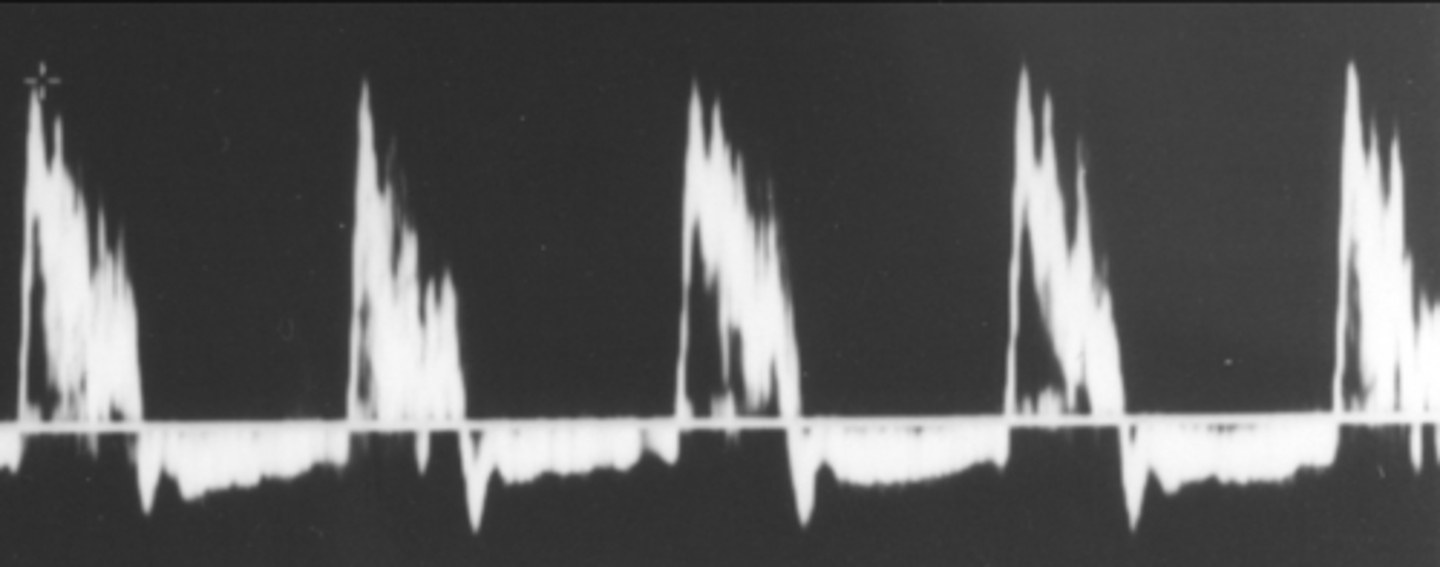
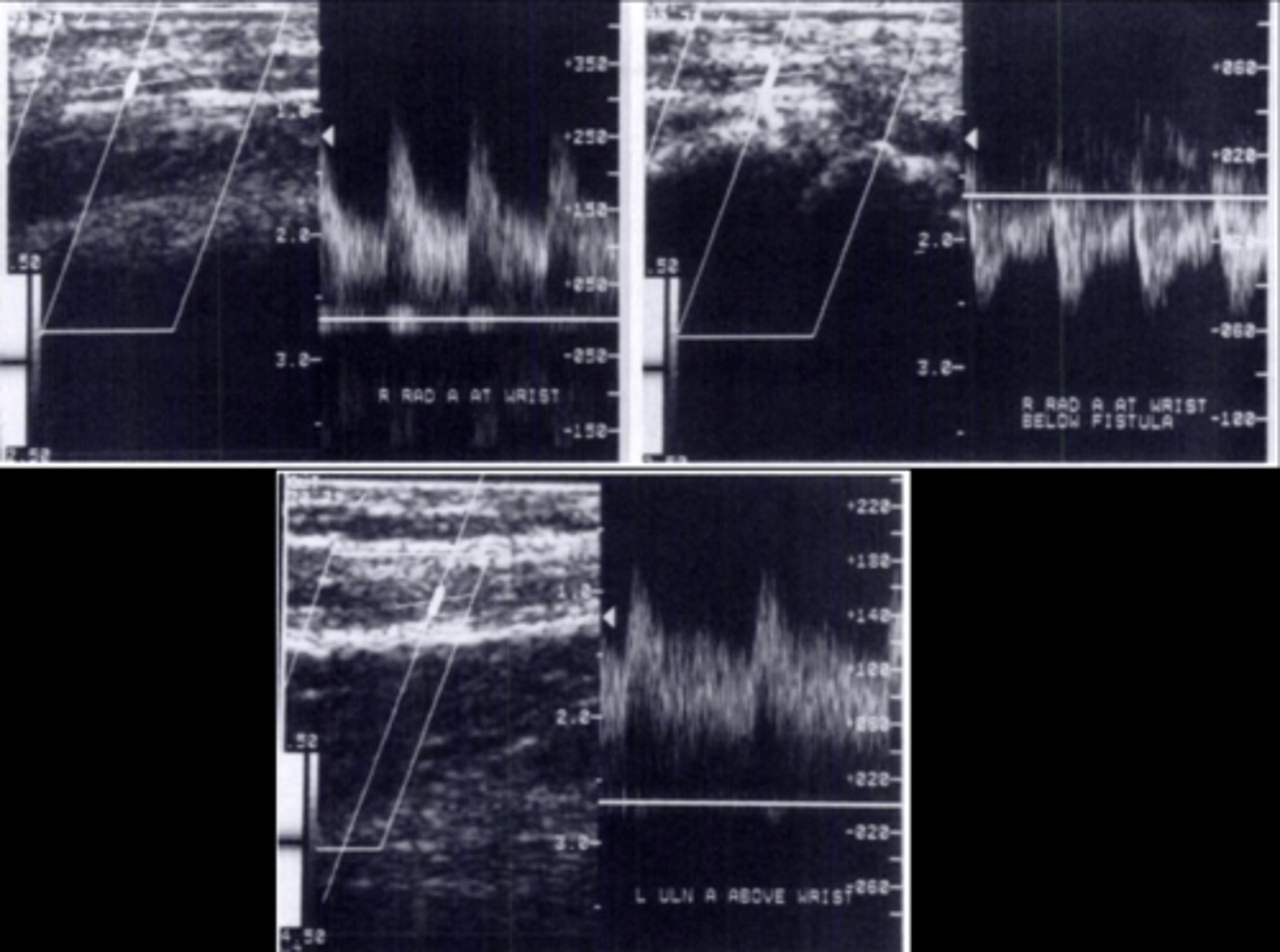
Evaluate waveform & note PSV - high resistant (rapid upstroke, sharp peak, low diastolic flow)
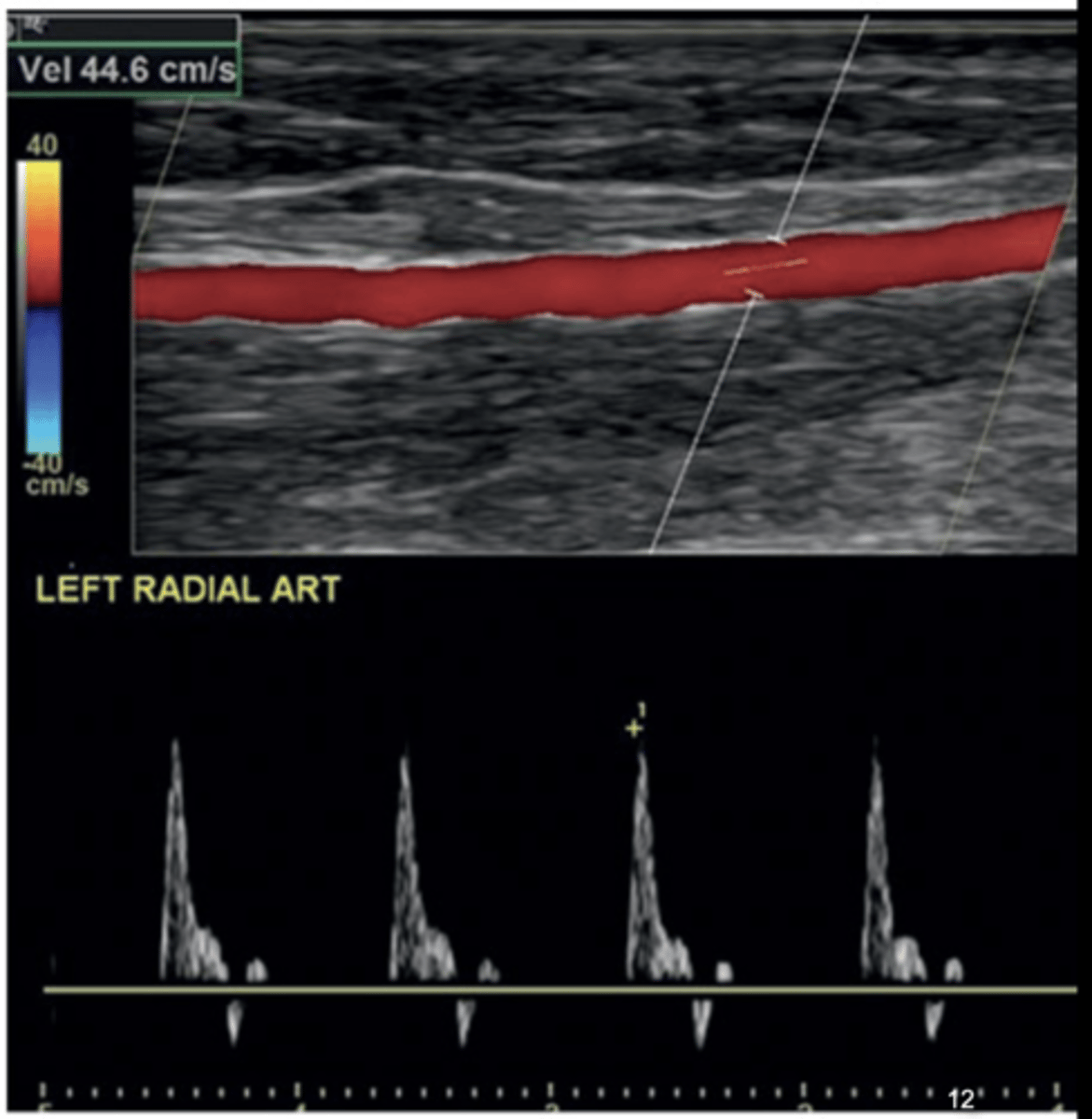
Arterial Diameter for Fistulas/Grafts
> 2.5 mm
AV Fistula & Hemodialysis Graft Venous Mapping
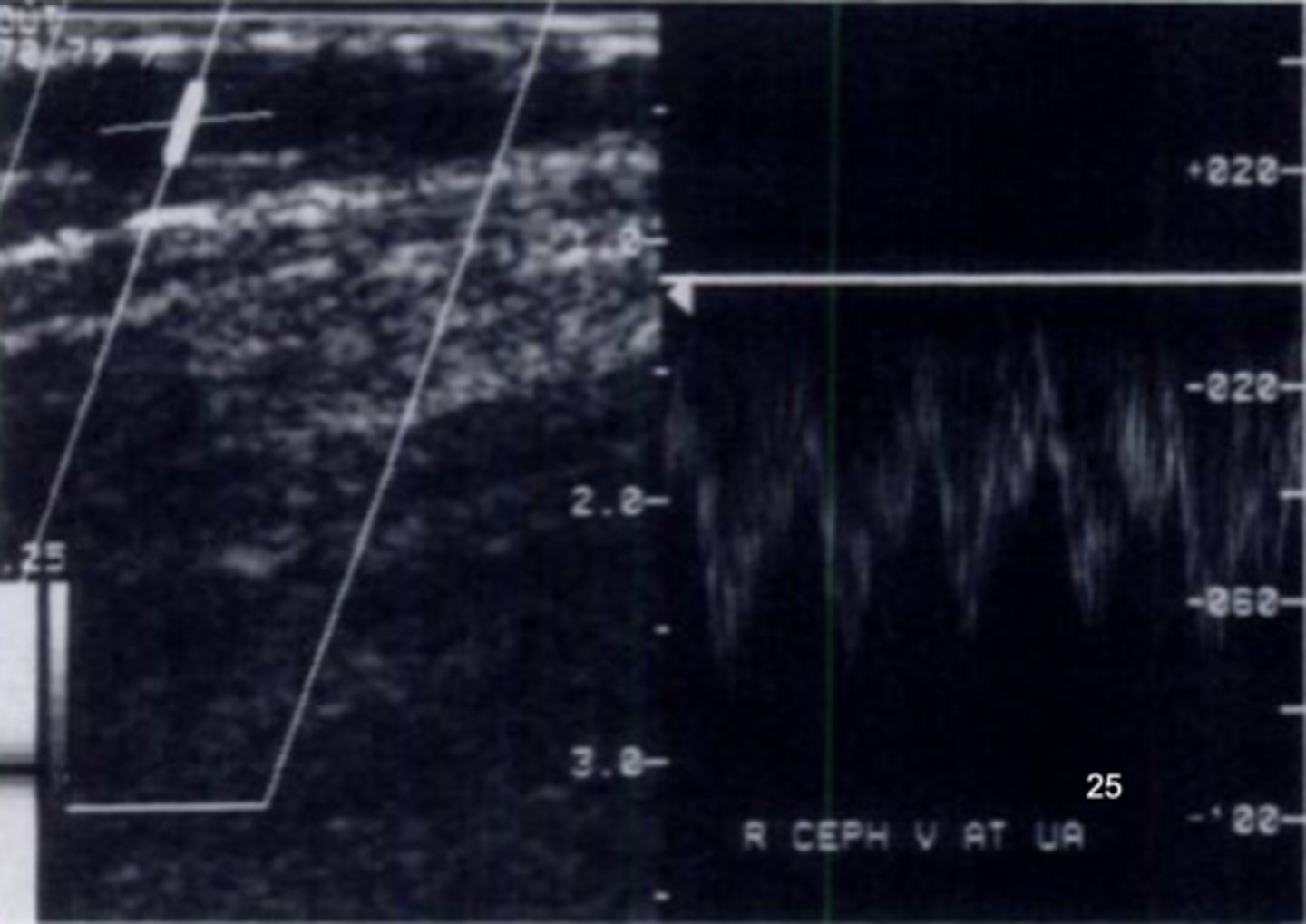
Start with superficial system of non-dominant forearm
Begin with cephalic, basilic, and median cubical veins at wrist and move proximally to axilla
Assess for thrombus, compressibility, narrowing, tributaries , scarring- central veins have respirophasicity & cardiac pulsatility
Compress & record diameter every 2 cm
Doppler with augmentation (include subclavian & IJV)
Measure vein diameter with & without tourniquet (2 tourniquets-at axillary & forearm-for 3 minutes)
Assess depth from skin surface to anterior wall of vein
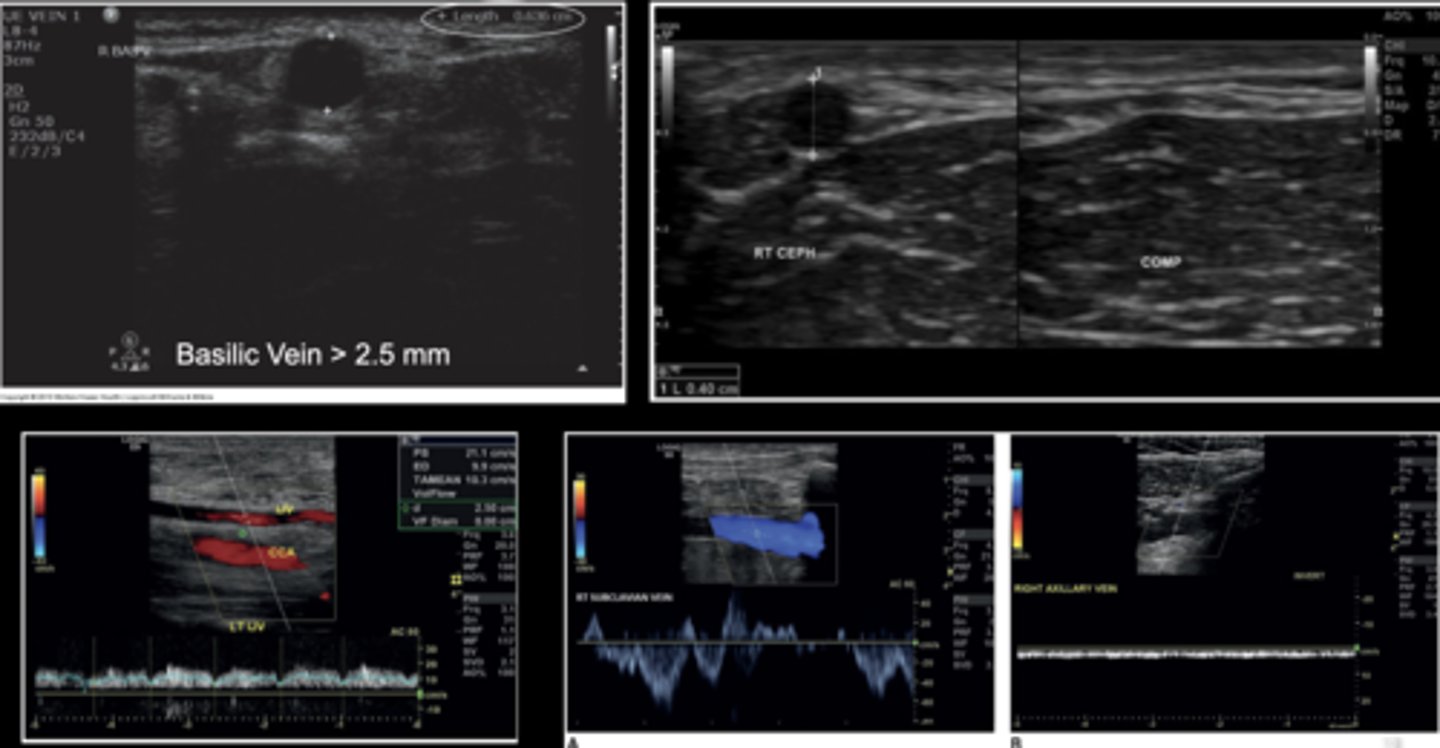
Vein Diameter for Fistulas/Grafts
> 2.5 mm
Vein Diameter for Synthetic Fistulas/Grafts
≥ 4 mm
Basilic Vein Length for Fistulas/Grafts
≥ 10 cm
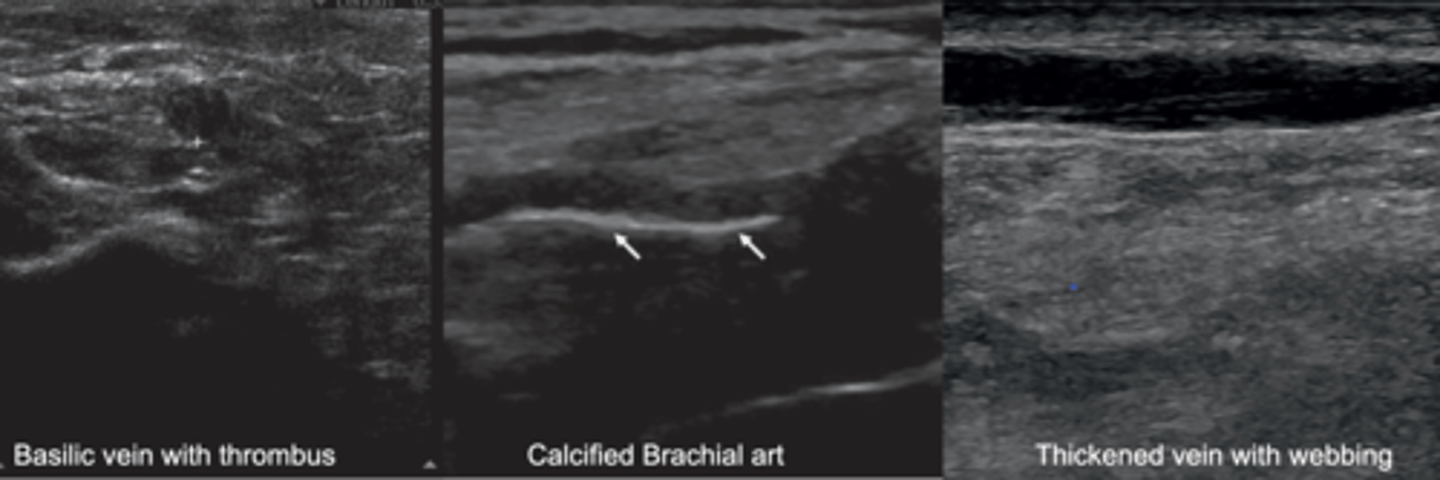
Pre-Mapping Contraindications for AV Fistula Placement
Thrombus
Calcifications
Thickened vessels
Local infection
Dressings that can't be removed
Open wounds
AV Fistula/Graft Maturity
Occurs 6 weeks - 6 months after placement
Assess 10-12 weeks after placement before hemodialysis begins
Mature AV Fistula/Graft
Drop in peripheral resistance
Can handle 6 cycles a month
Audible swishing bruit
Palpable thrill/vibration - turbulent flow at anastomosis
Large enough for two 15-gauge needles
Normal PSV for Fistula
100-400 cm/sec
Normal EDV for Fistula
60-200 cm/sec
Fistula Surveillance
Fistula diameters
Depth from skin surface
PSV's of:
- Native artery prox to anastomosis/arterial inflow
- Arterial anastomosis
- Throughout fistula - walk-through technique
- Venous outflow
Assess patency of all inflow arts/outflow veins
Arterial Side of Fistula
Low-resistant waveform
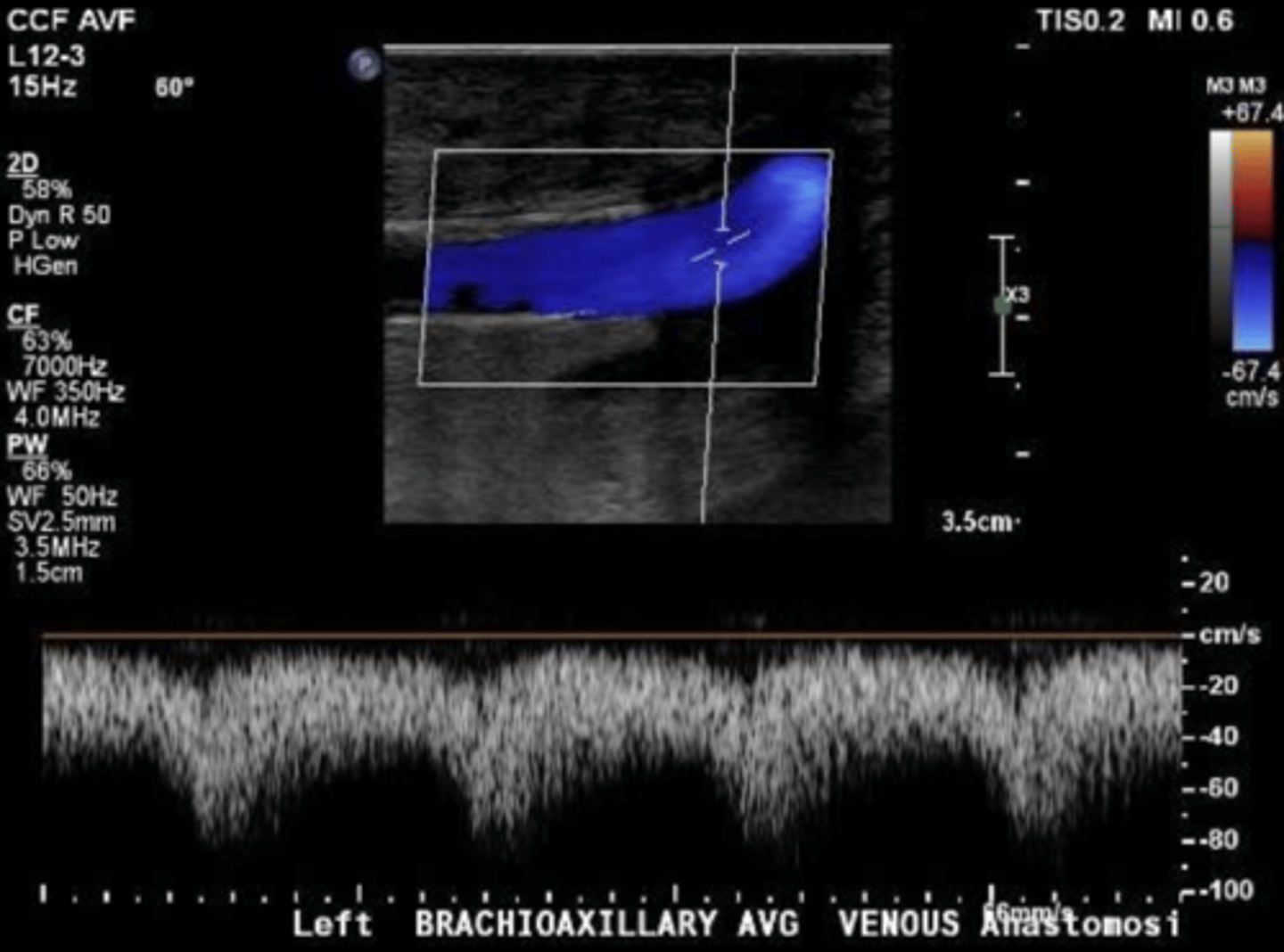
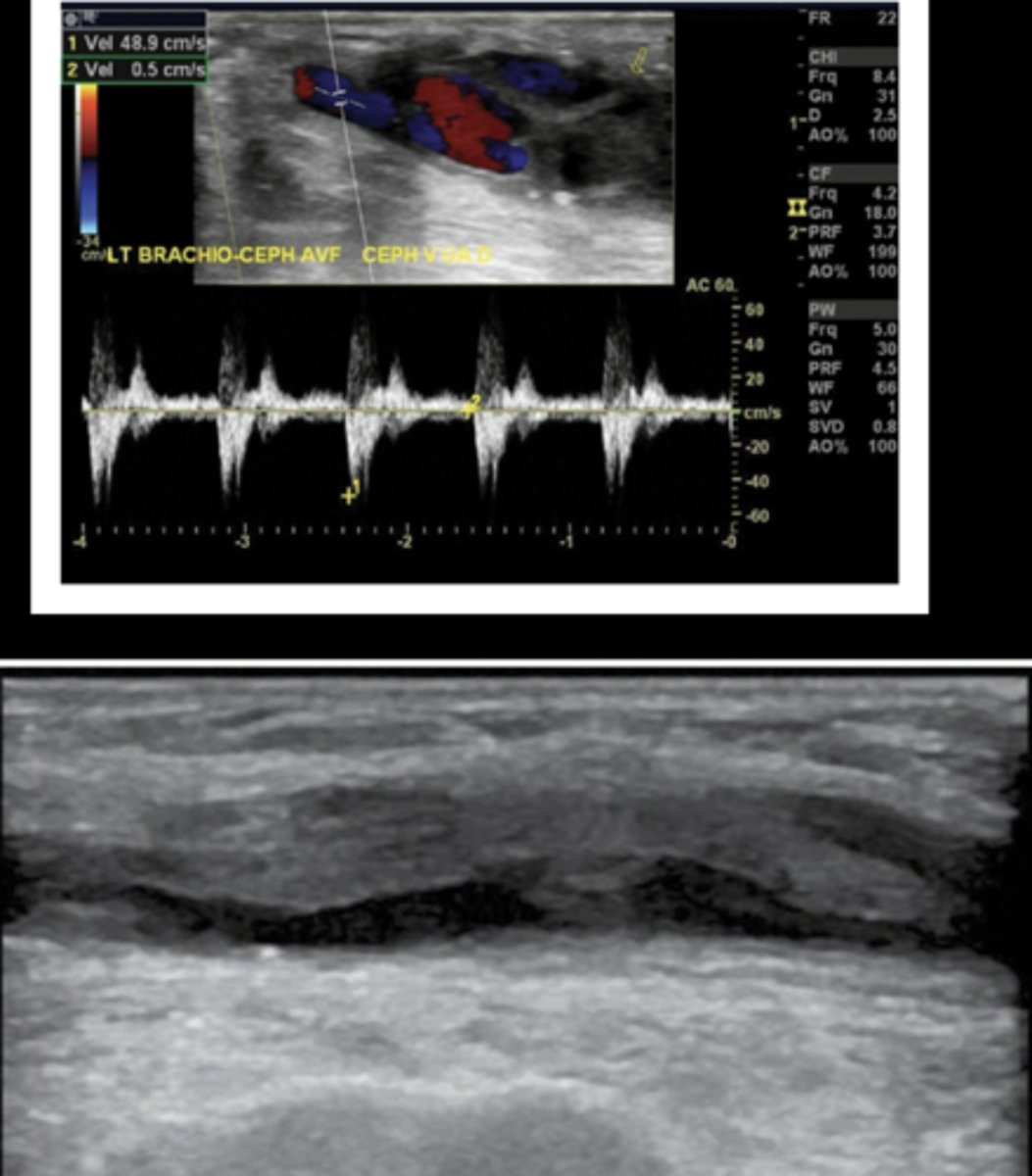
Venous Side of Fistula
High flow volume
Pulsatile prox to anastomosis
Normal Fistula Inflow Artery
Proximal to anastomosis
Low resistant - forward diastolic flow & spectral broadening
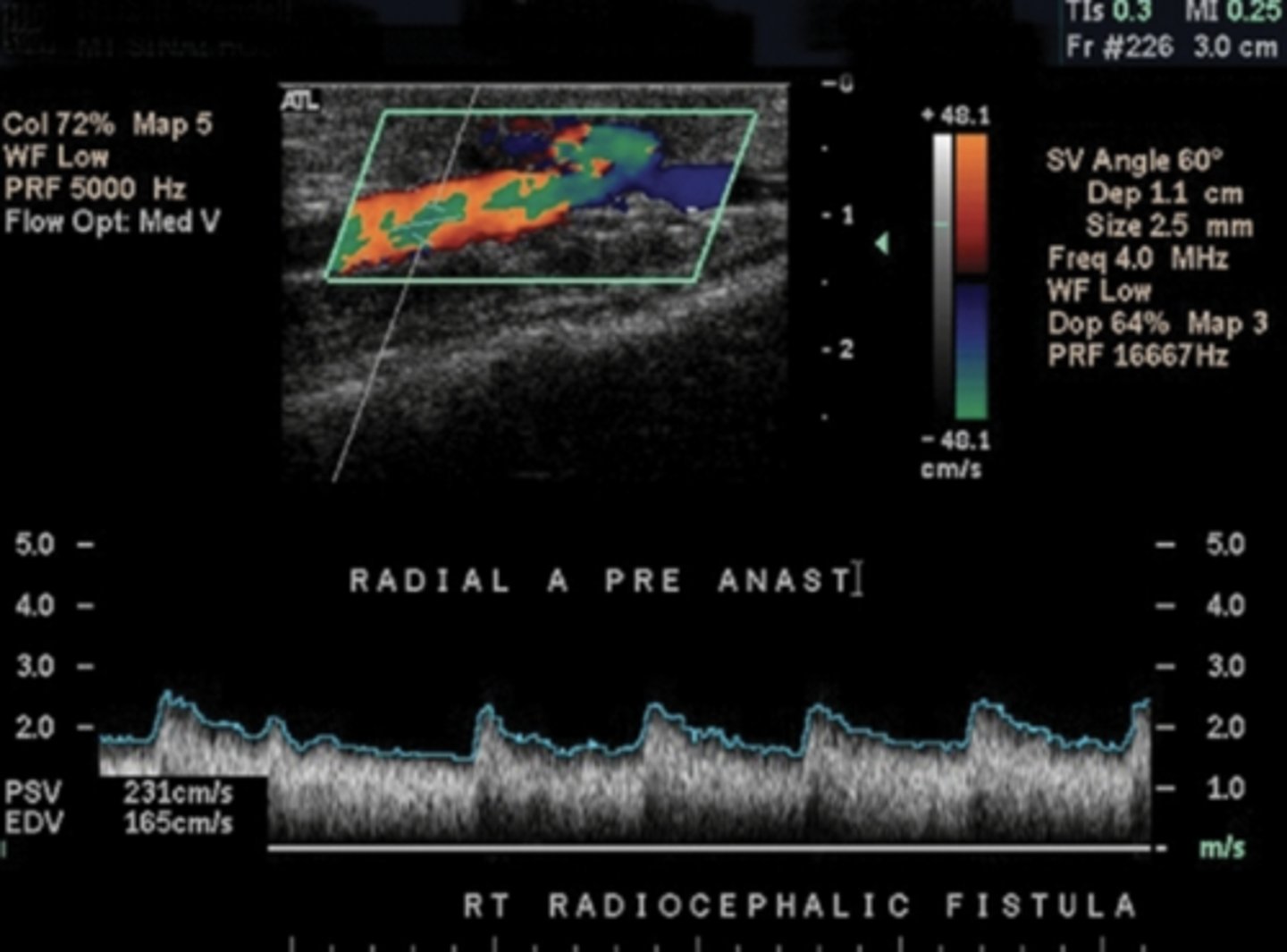
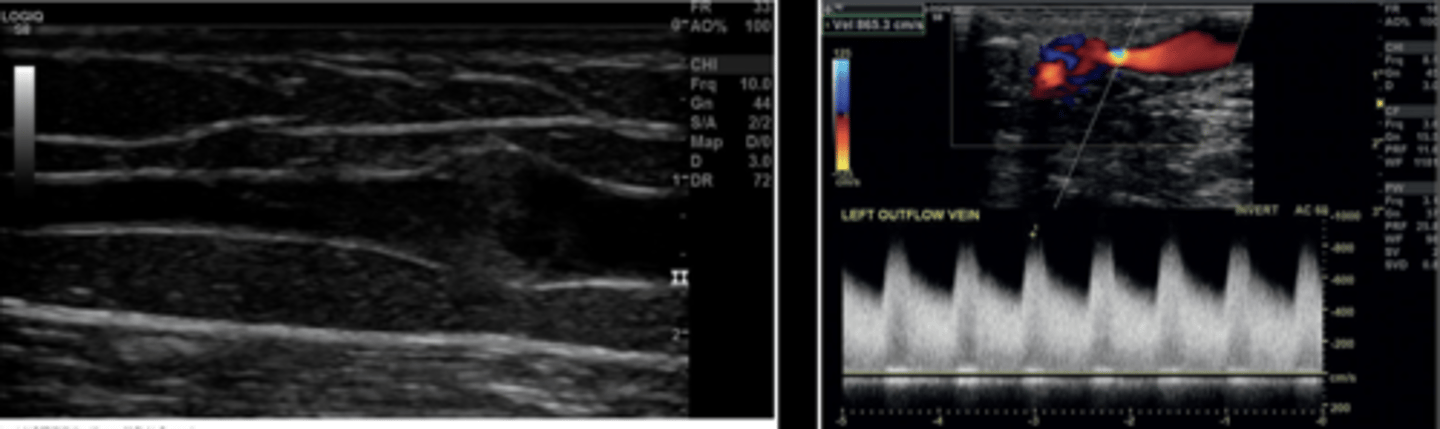
Normal Fistula Flow
1 cm below skin
Low resistant - forward diastolic flow & spectral broadening
Elevated PSV & EDV velocities
Normal Venous Outflow
Pulsatile flow
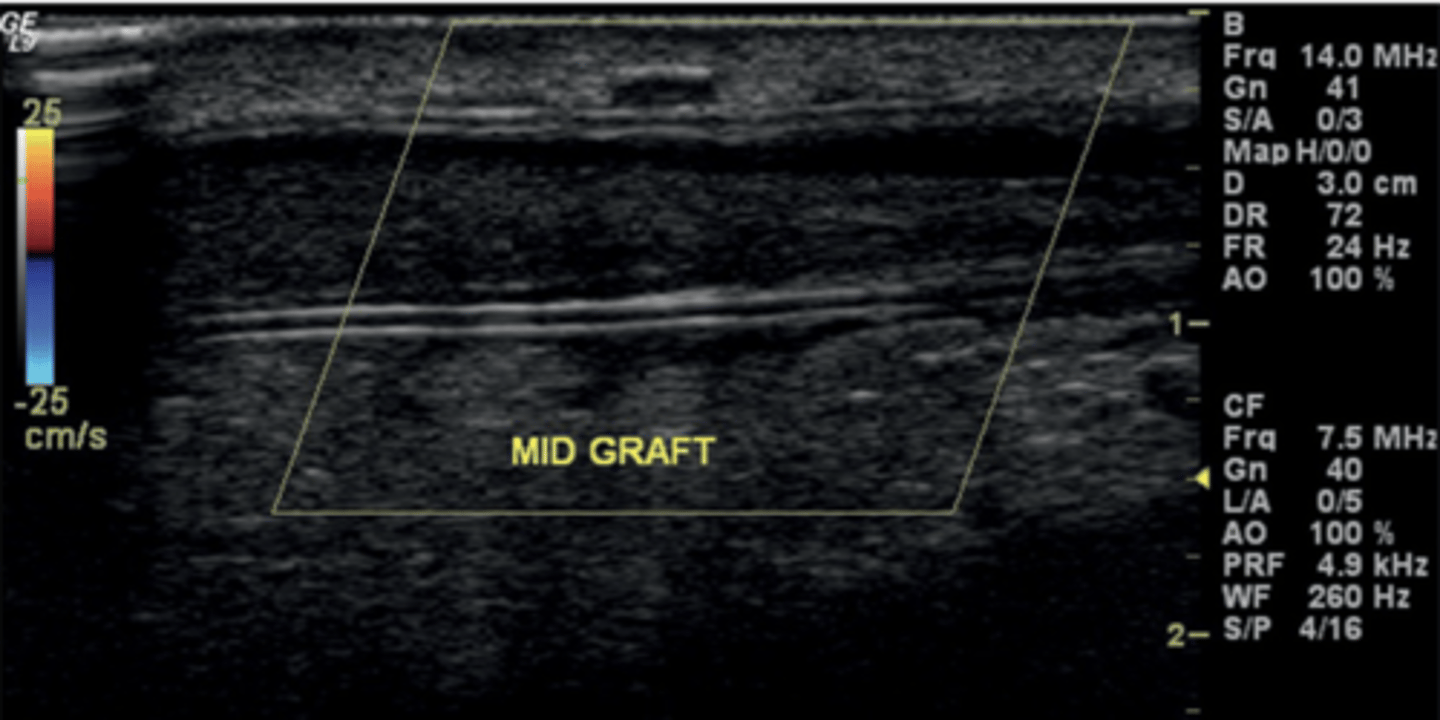
Acquiring Flow Volume of a Mature Fistula
Evaluate function at mid-fistula
Large sample volume (wide as vessel)
Measure diameter on grayscale
Use auto-tracing or trace 3-4 waveforms for mean velocity
Take at least 3 times
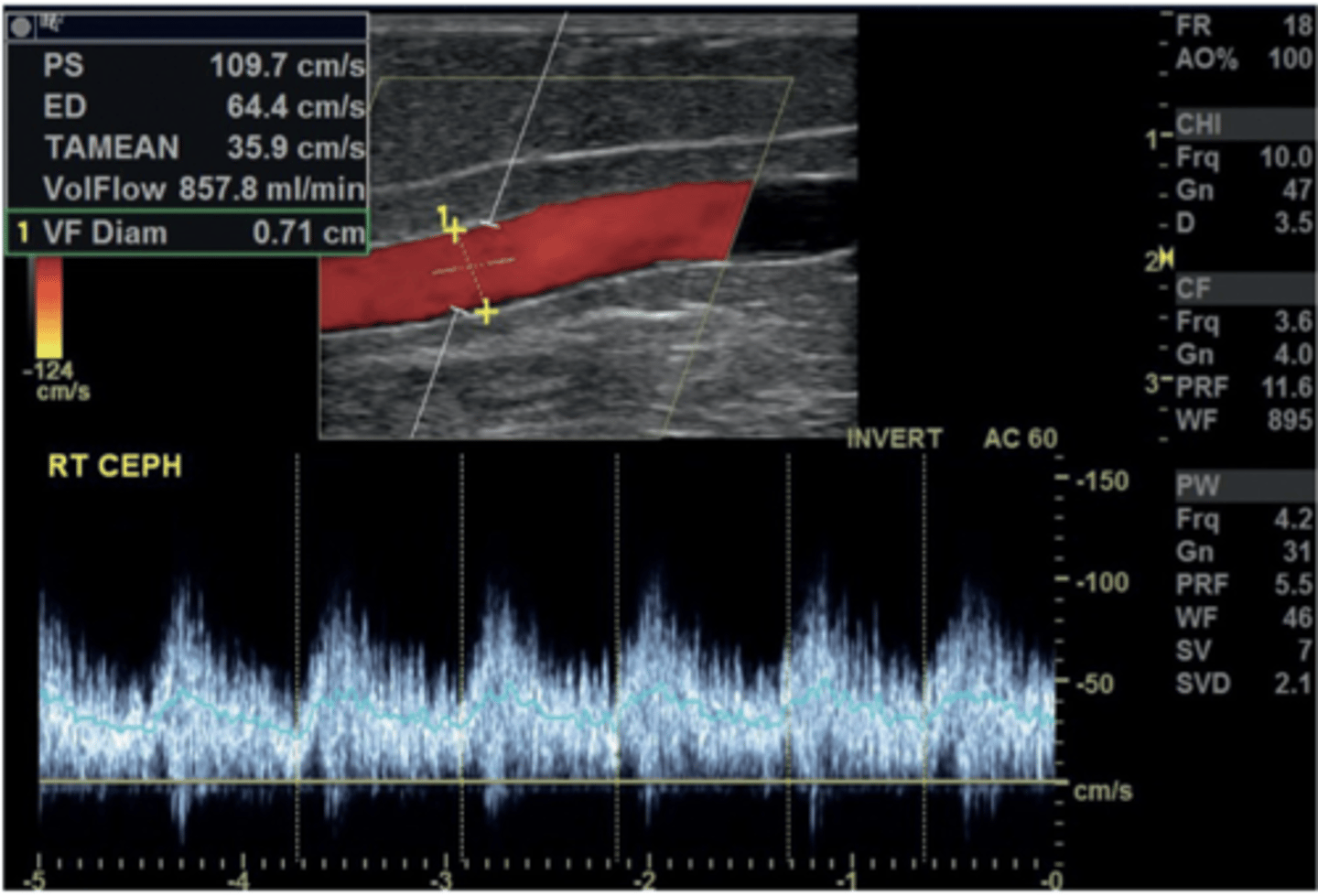
Normal Flow Volume of a Mature Fistula
> 800 ml/min
AV Fistula & Graft Complications
Immaturity
Stenosis
Occlusion
Thrombosis
Aneurysm and Pseudoaneurysm
Fluid collections
CHF
Arterial Steal Syndrome
Immature AV Fistula
Proximal hammer pulse
Minimal thrill
Lack of venous distention
Lack of high-pitched bruit
Signs of stenosis & palpable distal thickening
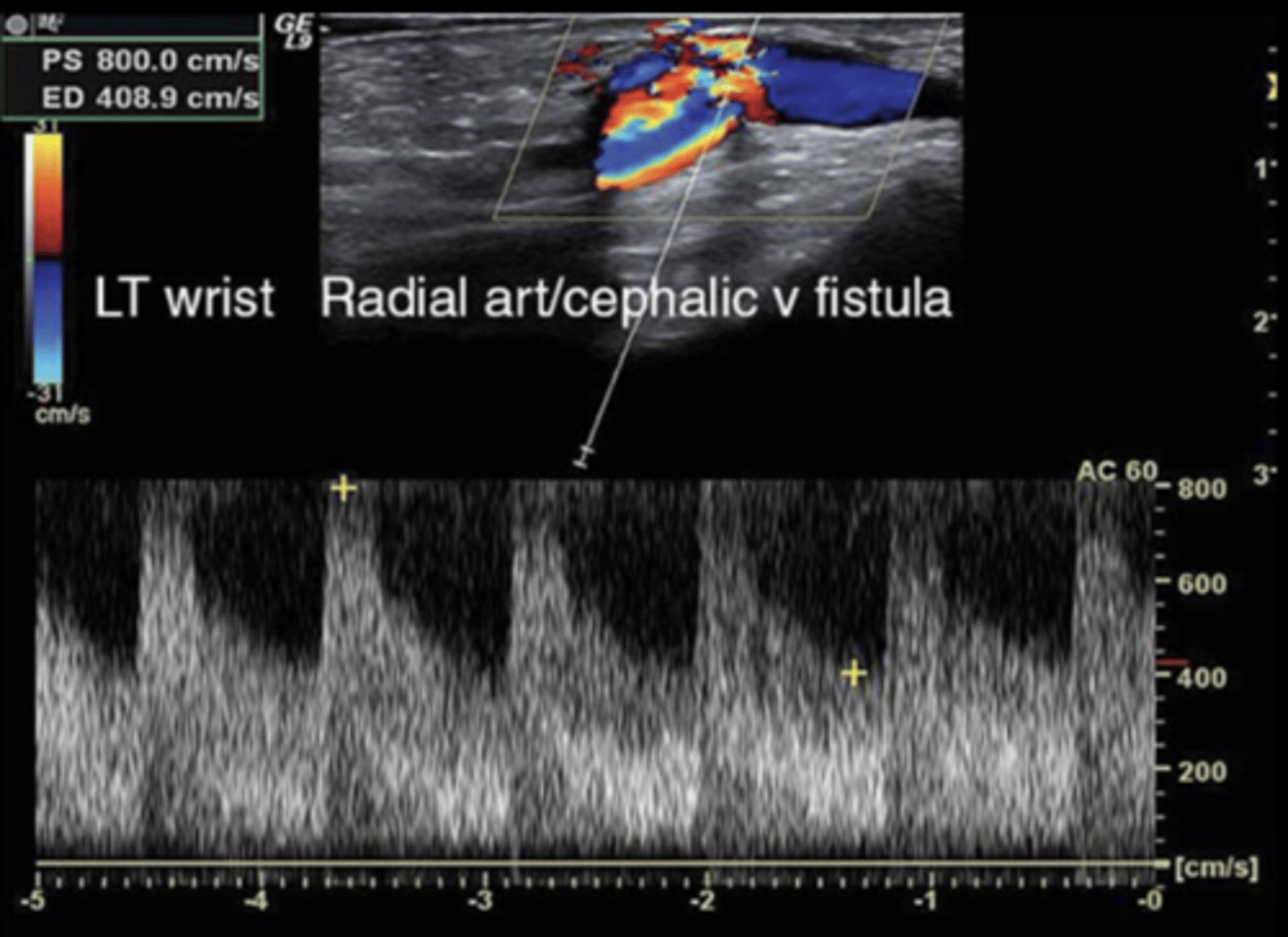
AV Fistula Stenosis
Most common in venous anastomosis & outflow vein
Echogenic intraluminal lesion
Flow reduction
Mild/Moderate Stenosis Flow Volume
500-800 ml/min
Severe Stenosis Flow Volume
< 500 ml/min
PSV of AV Fistula Stenosis
> 375 cm/sec
PSV Ratio for > 50% Stenosis on Arterial Side
> 3:1
PSV Ratio for > 50% Stenosis on Venous Side
> 2:1
AV Fistula Occlusion
Absent flow in lumen
Echogenic thrombus in lumen
Prox high-resistant flow
AV Fistula Thrombosis
To and Fro flow- inflow
Low PSV
Absence of color flow & no outflow
Echogenic material
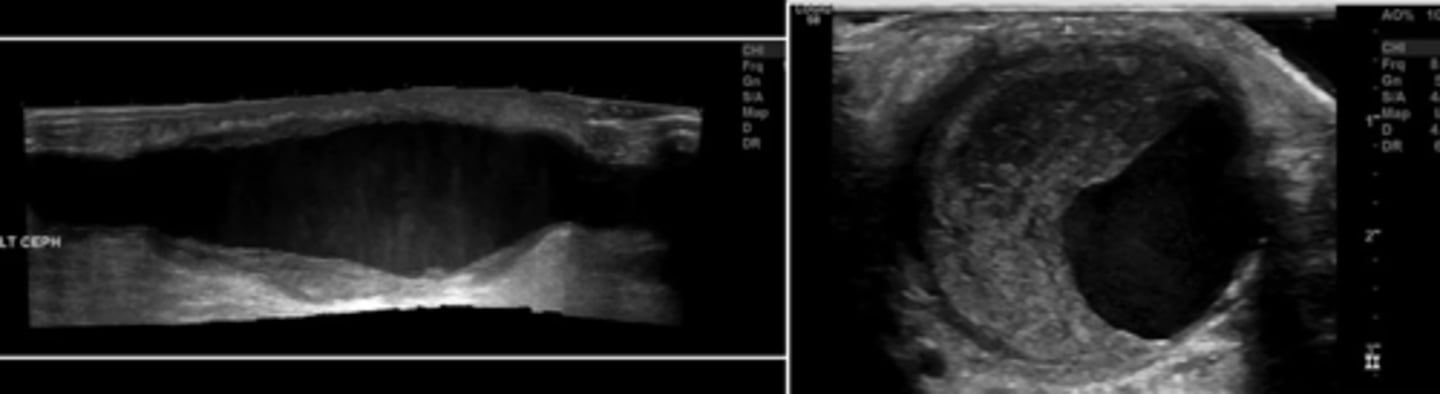
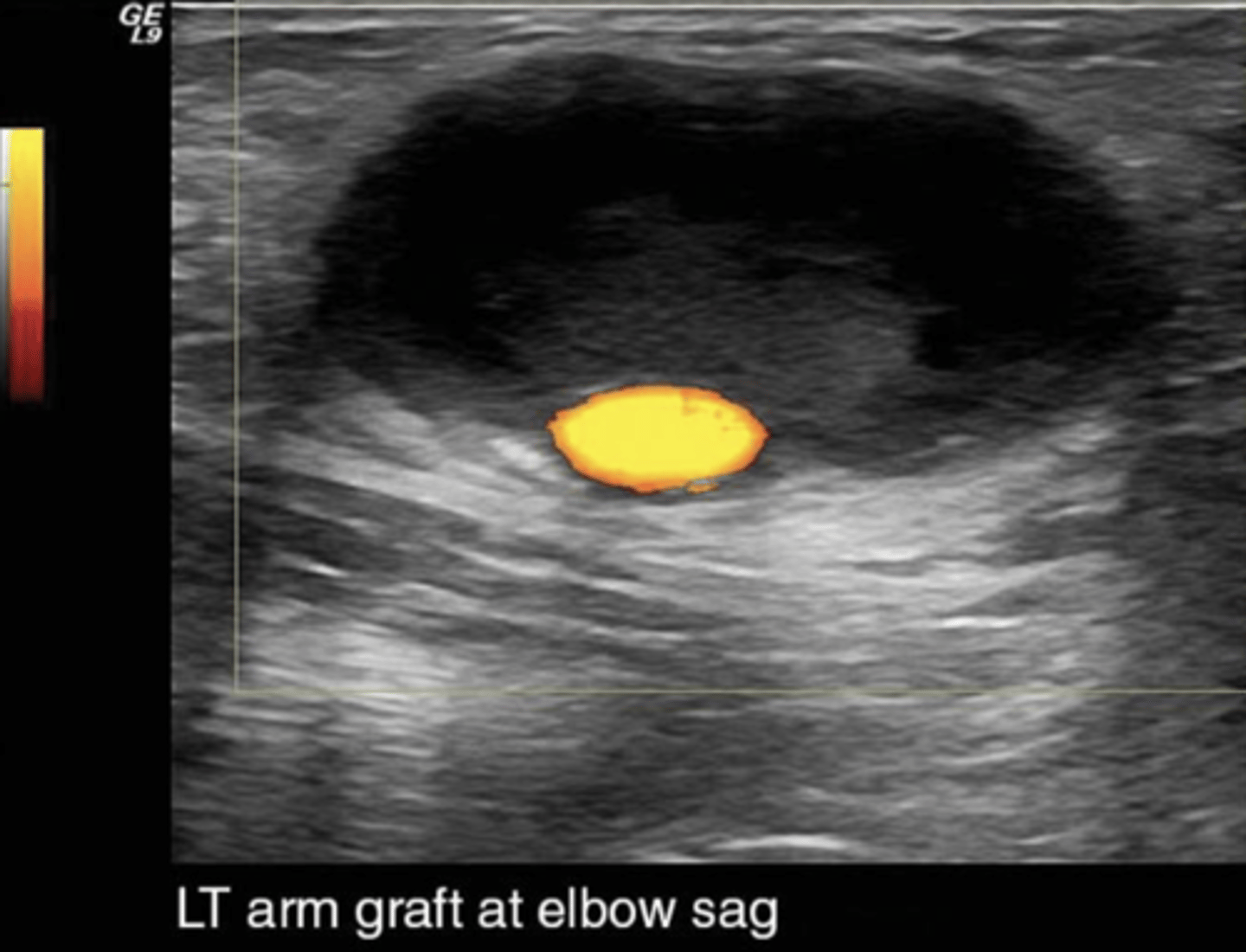
AV Fistula Aneurysm
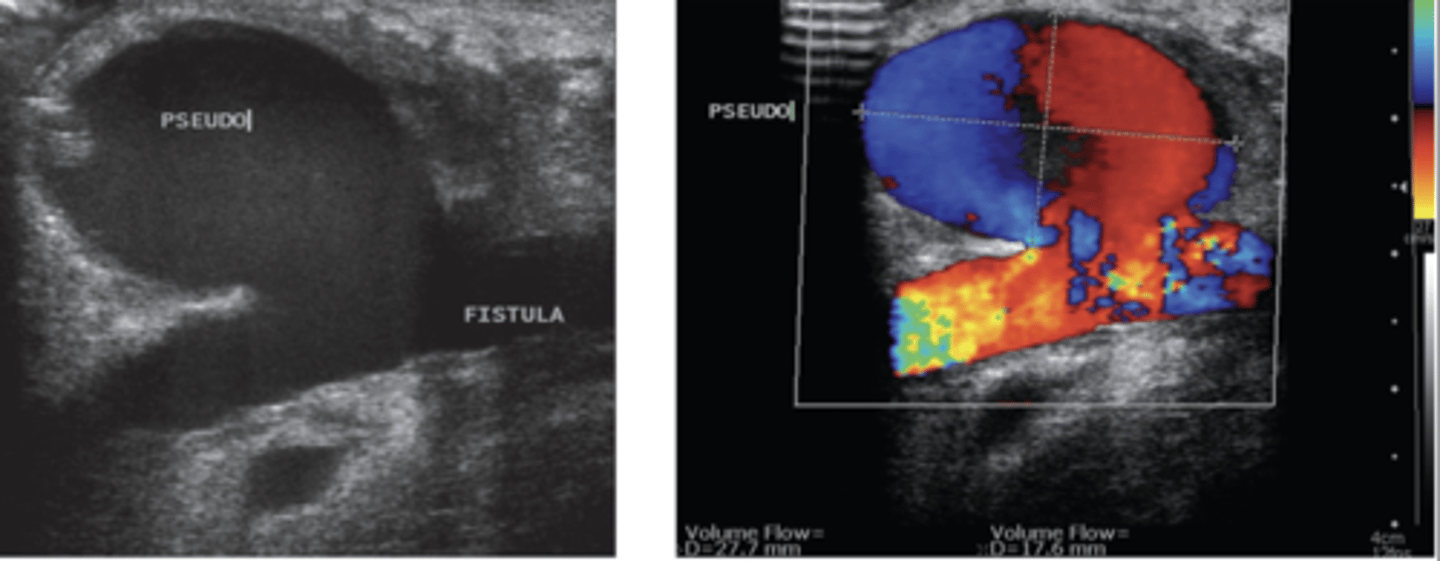
AV Fistula Pseudoaneurysm
AV Fistula Fluid collections
Arterial Steal Syndrome
Occurs in 75-90% of patients
Most patients are asymptomatic
Due to poor distal collateral circulation & high flow through fistula
Low-resistant outflow vein draws antegrade flow from inflow artery & steals retrograde flow from distal artery
Failing AV Fistula/Graft Interventions
Percutaneous transluminal angioplasty
Percutaneous recanalization
Interoperative branch ligation
Interoperative revision and vein interposition
DRIL procedure
DRIL Procedure
Ligation of native artery distal to dialysis access
Bypass from native artery to artery distal to ligation

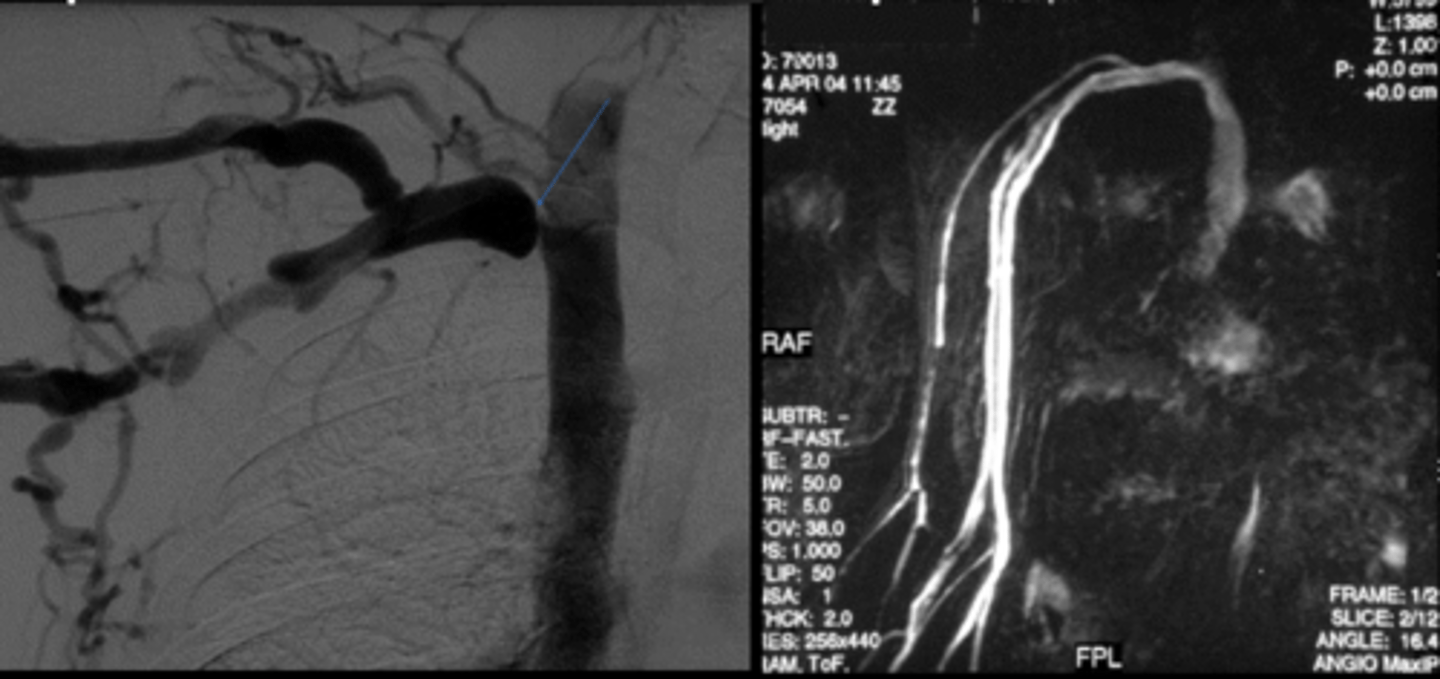
Complimentary Imaging for AV Fistula Mapping/Monitoring
Venography
Enhanced MR Venogram